

Page 1
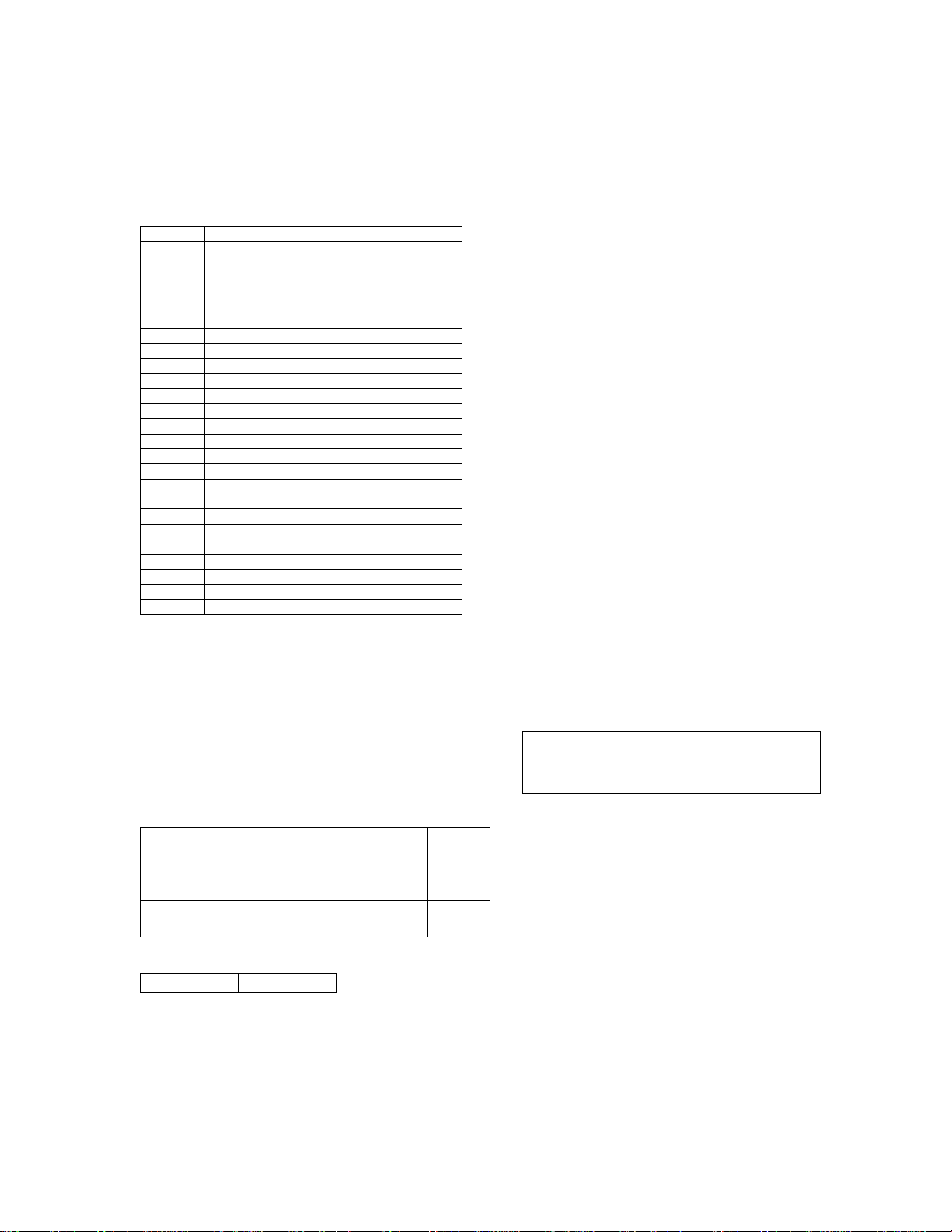
Icy® Catheter
Quantity
English
1
Icy® Catheter 3-Lumen
Applause™ Coated
2
Guidewires (.032” x 75cm)
1
Vessel Dilator
1
Detachable Suture Tab & Clip
1
18ga x 2 ½" (6.3cm) Radiopaque OTN Catheter
1
000 Silk Suture
1
Chloraprep® Triple Swabstick Prep Pack
6
4" x 4" Gauze Sponges
1
3cc Syringe
2
5cc Syringes
1
Fenestrated Drape
1
Povidone Ointment
2
22ga x 1 ½" (3.8 cm) Needles
1
18ga x 2 ¾" (7.0 cm) Needle
1
5cc Ampule Lidocaine HCL 1%
1
Needle Disposal Cup
1
SilvaSorb® Site Antimicrobial Dressing
Flow rate
Priming
Guidewire
Medial Port
(white)
Proximal
IC-3893
9.3F
6,126,684
6,299,599
6,409,747
6,416,533
6,585,692
6,645,234
6,652,565
6,656,209
6,719,724
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
Caution: Federal law restricts this device to sale by or on
the order of a physician.
Model IC-3893A/8700-0657-01 (Also referred
to as IC-3893)
Includes:
Storage:
Store between 20-25°C. Avoid f reezing and exces sive
heat above 40°C.
United States Patent Nos.:
9.3 French x 38cm
Triple Infusion Lumen
Extension Line Clamps
Radiopaque Polyurethane
1 25ga x 1" (2.5 cm ) Needle
1 No. 11 Surgical Blade w/ long handle
1 SureSite Transparent Film Dressing
Device Description:
The Icy® Heat Exchange Heat Catheter is a sterile, single use
flexible catheter designed for placement in the inferior vena
cava from an insertion site in the femoral vein. The Icy
Catheter is to be connected to a ZOLL single use disposable
CoolGard 3000
separately) and the CoolGard 3000
System. A dilator and guidewire are required for the
percutaneous insertion of the
lumens are available for infusion and sampling.
Port (brown)
®
/Thermogard XP® Start-Up Kit (supplied
®
/Thermogard XP®
Icy® Catheter. Three (3)
ml/hr
IC-3893 1700 ml/hr 0.5 cc
®
IC-3893 900 ml/hr 0.4 cc
Port (blue)
IC-3893 1200 ml/hr 0.4 cc
Insertion Size
®
Catheter blood contact surfaces are
The Icy
Applause™treated. Applause is a trademark of SurModics,
Inc., registered in the U.S. Patent and trademark off ice.
Sterility
Ethylene oxide sterilized. The Icy® Catheter is supplied
sterile for single use only and should not be resterilized. The
package should be inspected prior to use to ensure that the
sterility barrier has not been compromised.
1 of 11 106085-001 Rev.2
Volume
6,749,585
Other U.S. and foreign patents pending.
Indications for Use:
The ZOLL Icy® Catheter Model IC-3893A, connected
to the ZOLL Th e rmal Regulation System, is indicated
for use:
• in cardiac surgery adult patients to achieve and/or
maintain normothermia during surgery and
recovery/i ntensive care, and
• to induce, maintain and reverse mild hypothermia
in neurosurg ery adult patients in surgery and
recovery/i ntensive care.
Safety and Efficacy Considerations:
Central venous catheterization should only be
performed by well-trained personnel well versed in
anatomical landmarks and safe technique. Personnel
should also have knowledge of potential complications.
Product designed for single use only. Do not r esterilize
or reuse. Do n o t reinsert, onc e removed from patient.
Do not alter the catheter in any way.
Potential risks with re-use of a single use device include
but are not limited to:
• Potentially life threatening infection
• Toxic shock due to degrad ation of materials
• Increased risk of thrombosis
• Reduced heat exchange power
• Device failures
Warning: Do not allow catheter to be placed into right
atrium or right ventricle. Placement in right atrium or
right vent ricle can resul t i n severe patient injury or
death.
Contraindications:
1. The risks of t he catheter are essentially those of a
central line. The catheter should not be used in
patients for whom central line placement is not
indicated.
2. Bleeding diathesis.
3. Active sepsis.
4. Infection o r active bleeding at the site of catheter
insertion.
5. Patients with no vascular access, or vascular
system will not accom m odate catheter including
patients with vena cava filters or other implanted
impediments t o passage of the catheter.
6. Patients for whom the required temperature
monitoring cannot be established.
7. Hypothermia is contraindicated in patients who
have hemato lo g ical diseases that will be made
worse with hypothermia e.g. any disease that
produces cryoglobulinemia, any
hemoglobinopathy in which hemolytic anaemia
Page 2

Icy® Catheter
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
can be precipitated by cold including Sickle Cell
Disease or Thalassemia.
Warnings and Precautio ns:
1. SINGLE USE ONLY. Product designed for single use
only. Do not resterilize or reuse. Do not reinsert, once
removed from patient. Do not alter the catheter in any
way. Maximum use period: 4 da ys.
2. Do not allow catheter to be placed into right atrium or
right ventricle. Catheter should be positioned so that
the distal tip of catheter is in the inferior vena cava
below its junction with the right atrium and parallel to
the vessel wall. X-ray examination should b e us ed to
ensure that the catheter is not in the right atrium or
ventricle.
3. Cardiac Tamponade: Placement of indwelling catheters
in the right atrium is a practice that may lead to cardiac
perforation and tampon a de . Pr actitioner s pla c i ng
central venous catheters must be aware of this
potentially fatal complication before advancing the
catheter too far relative to patient size. The actua l
position of the tip of the indwelling catheter should be
confirmed by x-ray after insertion. Central venous
catheters should not be placed in the right atrium unless
specific ally required f o r special relativ ely short term
procedures, such as aspiration of air emboli during
neurosurg ery. Such procedures are nevertheless risk
prone and should be closely monitored and controlled.
4. Alcohol and acetone can weaken the structure of the
polyureth ane material. Care should therefore be taken
when infusing drugs containing alcohol or when using
alcohol or acetone when performing routine catheter
care and maintenance. Alcohol should not be used to
declot the catheter.
5. Use of a syringe smaller than 10 ml to irrigate or declot
an occluded catheter may cause intraluminal leakage or
catheter rupture.
6. Caution: If blood is observed within the circuit
circulating the sterile saline, stop the procedure.
7. The catheter is coated with Heparin. This may induce
or aggravate pre-existing Heparin induced
thrombocytopenia (HIT).
8. Central venous catheterization should only be
performed by well-trained personnel well versed in
anatomical landmarks and safe technique. Personnel
should also have knowledge of potential complications.
9. Catheter shoul d be placed via a femoral vein approach
only.
10. Possible complications with central venous catheters
include: atrial or ventricular perforation, cardiac
tamponad e, air embolism, catheter embolism, thoracic
duct laceration, bacte r e m ia, sept icemia, thrombosis,
inadvertent ar te r ia l pu ncture, hematoma formation,
hemorrhage, nerve damage and dysrhythmias.
11. All Luer-Lock connections and covers must be securely
tightened to prevent air embolism or fluid or blood loss.
12. Never use exces sive force in moving the catheter or
guidewire. If resistance is encountered, an x-ray should
be performed to identify the r eason for the resistance.
13. Passage of t he guidewire into the right heart can cause
dysrhythmias, right bundle branch block, vessel wall,
atrial or ventricular perforation.
14. Use only sterile normal saline for catheter priming
and as the ci r culating fluid in the catheter.
15. Catheter should be routinely inspected for flow
rate, security of dressing, correct catheter position
and for secure Luer-Lock connection. Use
centimeter markings to identify if the catheter
position has c ha n g ed.
16. Only x-ray examination can ensure that the
catheter tip has not entered the heart or no longer
lies parallel to the vessel wall. If catheter position
has change d, p e r form an x-ray examination to
confirm catheter tip position.
17. For blood sampling, temporarily shut off
remaining infusion ports through which solutions
are being inf us ed.
18. Use only a 30cc or smaller s yringe for blood
sampling.
19. Use only ZOLL suture tab and clip provided in kit
to prevent catheter damage.
20. Do not infuse into the teal-green Luer-Lock
connections.
21. Use care when infusing drugs that may be
affected by cool temperat ures (as low as 4ºC).
Mannitol containing solutions are temperature
sensitive and must not be delivered through the
®
Icy
Catheter except for rapid push of up to a
concentration of 20% mannitol solution followed
by saline flush. Higher than a 20% concentration
of mannitol or drip or in fusion pump delivery of
mannitol must be done via a separate line.
22. WARNING: When connecting infusion
sets/injection systems to ZOLL Catheters do not
exceed 100 psi/689 k Pa.
23. Not intend ed for pediatri c o r neonatal use.
24. For patients being made hypothermic, the
hypothermia itself may exacerbate some disease
states. Care should be taken to properly monitor
patient homeostasis during hypothermia.
• Cardiac rhythm disturbances – both
bradycardia and ventricular
tachyarrhythmia.
• Clotting and coagulations function. Patients
at risk for disturbances of their clotting or
coagulation function s ho uld be close ly
monitored during hypothermia.
• Blood gas and pH analysis. Hypothermia
modifies resting pH and PaC O
should be aware that of the eff ect of
temperatur e up on the result.
• Prolonged hypothermia depresses the
immune response and lung function.
WARNING: INTRALUMINAL LEAKAGE
Intraluminal leakage between the saline lumen and
infusion lumens is an unc om mon but potential catheter
failure. In the event of such a failure, sterile saline
from the cooling circuit will be introduced into the
patient. Intral uminal leakage will usually be associated
with a fluid loss alarm which will stop the system.
ALWAYS INVESTIGATE FLUID LEVEL ALARMS.
The cooling circuit is a closed loop system – usually
fluid loss alarms indicate a breach somewhere in this
. Physicians
2
2 of 11 106085-001 Rev.2
Page 3

Icy® Catheter
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
closed loop. With any fluid loss alarm, check both the
integrity of the catheter and the Start-Up Kit (see belo w).
To check the integrity of the catheter:
1. Stop operation of the C oolGard 3000
®
XP
2. Disconnect the Start-Up Kit from the catheter and
3. Fill a sterile 10 ml syringe with sterile saline.
4. Connected to the INFLOW lumen of the catheter and
5. Now cap the OUTFLOW lumen and pull 5 cc of
6. Ease the vacuum and recap the INFLOW lumen.
To check the integrity of the tubing set:
1. Look for obvious leaka ge.
2. Remove the tubing from the pump raceway and inspect
3. Check along the tubing from the pump to the patient for
4. Similarly, check the tubing that returns to the pump
5. Trace the tubing from the saline bag back to the pump.
More warnings and preca utions are located in following
instructions.
System.
properly cap both the catheter and Start-Up Kit using an
aseptic technique.
disconnect the outflow cap. Infuse the 10 ml of saline –
it should flow out the outflow lumen.
vacuum and sustain this for at least 10 seconds.
Approximately 4 ml of saline, but not blood, should
enter the syringe and you should be able to maintain the
vacuum.
for damage (return it to position if not damaged).
sources of fluid loss.
Look for damage to the tubing and/or the presence of
air within the tubing.
• Inspect, and tighten as nece ssar y, each Luer fitting
(do not use instruments to tighten Luer fittings).
from the patient. Examine the saline bag to ensure that
it has not been accidentally compromised (for example,
the spike may have damaged the bag wall).
Materials Required:
Quantity Description
®
1 Icy
1 Bag of Normal Saline
1 Start-Up Kit
1 CoolGard 3000
Kit for percutaneous introduction
®
Catheter Preparation and Insertion:
Use sterile technique.
1. Caution: Use f e moral vein app r oach only.
2. Place patient in a supine position.
3. Prep and dra pe puncture site as required.
4. Caution: Always prime catheter before it is inserted
into patient.
5. Carefully rem ove catheter from package, leaving on
catheter membrane cover.
Catheter Preparation Procedure:
3 of 11 106085-001 Rev.2
®
/Thermogard
/Thermogard XP® System
1. Remove caps from the inflow and outflow luer
hubs. With the catheter cover in place, fill syringe
(5cc or larger) with steril e saline and attach
syringe to female inflow luer hub.
2. Warning: Never inject positive pressure into
the inflow hub with the outflow luer cap in
place.
3. Gently inject saline through cathet er u ntil it
begins to exit from outf low luer.
4. Using 5 cc or larger syringe, flush the distal
infusion lumen with sterile saline. Leave the
distal luer uncapped for guidewire passage.
5. Remove catheter membrane cover. If there is
resistance in removing the m embrane cover from
the catheter, flush the membrane cover with
sterile saline. Inspect catheter to assur e that air
has been pu rged from the heat ex change
membrane. Inspect the catheter for leaks .
6. Warning: Do not cut the catheter to alter
length.
Catheter Insertion:
1. Obtain femoral venous access using standard
percutaneous techniques. Access should be
maintained with a .032” guidewir e. See special
instructions for Guidewires.
2. Warning: Do not attempt to re-insert a partially
or completely withdrawn OTN (over the needle)
introducer needle from its catheter.
3. Caution: Do not use a guidewire larger than
.032” with the Icy
4. Holding spring guidewire in place, remove
introducer catheter. Precaution: Maintain a firm
grip on the guidewire at all times.
5. Enlarge the cutaneous puncture site with cutting
edge of scalpel positioned away from the
guidewire. Warning: Do not cut guidewire. Use
vessel dilator to enlarge site as required. Do not
leave vessel dilator in place as an indwelling
catheter to minimize risk of possible vessel wall
perforation
6. Thread tip of Icy
Maintain a sufficiently firm grip on the guidewire
during catheter insertion. Grasping near skin,
advance ca t heter into vein with a slight twisting
motion.
7. Using c en timeter marks on the catheter as
positioning reference points, advance catheter to
final indwe ll ing position.
8. Hold catheter at desired depth and remove
guidewire. If resistance is encountered when
attempting to remove the guidewire after catheter
placement, the guidewire may be kinked about the
tip of the cat heter. If resistance is encountered,
withdraw the catheter relative to the guidewire
about 2-3 cm and attempt to remove the
guidewire. If resistance is again encount ered
remove the guidewire and ca t heter
simultaneously.
9. Caution: Do not apply undue force to the
guidewire.
10. Verify that the guidewire is intact upon removal.
®
Catheter.
®
Catheter over guidewire.
Page 4

Icy® Catheter
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
11. Check lumen placement by attaching a syringe to the
distal infusion luer hub and aspirate until a free flow of
venous blood is observed . Connect infusion luer to
appropriate Luer-Lock line as required. Unused
infusion port may be "locked" through injection cap
using standard hospital protocol. A slide clamp is
provided on the tubing to occlude flow through the
infusion lum en during line a n d injection ca p changes.
Precaution: To minimize risk of dam age to the tubing
from excessive pressure, the clamp must be opened
prior to infusing through the lumen.
12. Caution: Do not clamp or occlude inflow or outflow
lines. This can cause line blockage and possible
failure.
13. Secure and dress insertio n site and catheter temporari l y.
14 Verify catheter tip position by chest x-ray immediately
after placement. X-ray exam must show the catheter
located in the IVC with the distal end of the catheter
parallel to the vena cava wall. If the catheter tip is
malpositioned, reposition and reverify.
15. Proximal radiopaque marker indicates proximal end of
balloons to ensure that balloons reside com pletely in
vessel. If catheter is malpositioned, reposition and
reverify.
16. Secure ca theter to patient. Use juncture h u b side wings
as primary suture site to minimize the risk of catheter
migration.
17. The ZOLL suture tab and clip can also be used as an
additional attachment point. Assure that catheter bod y
is secure and does not slide.
18. Caution: Use on l y the ZOLL suture tab and clip
provided in the kit. Catheter damage may result if
other tabs or clips are used.
19. Caution: Do not suture directly to the outside
diameter of the catheter to minimize the risk of
cutting or damaging the catheter or impeding
catheter flow.
20. Dress puncture site per hospital protocol. Maintain the
insertion site with regular meticulous redressing using
aseptic technique.
21. Record on the patient's chart the indwelling catheter
length using the centimeter marks on the catheter shaft
as reference. Frequent visual reassessmen t should be
made to ensure that the cath eter has not moved .
22. Attach a primed Start-Up Kit to Icy
Catheter by connecting the male luer of the Start-Up
Kit to the female inflow luer of the Icy
the female luer of the Start-Up Kit to the male outflow
luer of the Icy
loosely to the INFLOW and O UTFL OW extension
tubes to help identify them. Assure that a sufficient
amount of sterile saline i s present at the ends of the
hubs to make an air free connection. Refer to
CoolGard 3000
details on C oo lGard 3000
operation.
23. Warning: Failure to connect the Start-Up Kit
correctly to the catheter could result in catheter
failure. Do not attach Start-Up Kit to the brown
luer.
24. Caution: Do not attach Start-Up Kit to distal port.
®
Catheter. White "ZOLL" tags are fitted
®
/Thermogard XP® manual for
4 of 11 106085-001 Rev.2
®
Heat Exchange
®
Catheter an d
®
/Thermogard XP®®
25. Caution: Do not place any stopcocks in line
that may be inadvertently shut off. This can
cause line blockage and possible failure.
26. Pump saline through Start-Up Kit and catheter to
assure that all connections are secure and that
there is no leaking. Allow any remaining air in
system to be purged out.
Disconnecting Catheter from CoolGard
®
/Thermogard XP® System:
3000
1. Stop circulation of saline through catheter.
2. Disconnect Start-Up Kit from catheter.
3. To maintain sterile connections, immediately cap
off luer connectors of both catheter and Start-Up
Kit using sterile luer caps or connect inflow and
outflow luers together.
Reconnecting Catheter to CoolGard
®
/Thermogard XP® System:
3000
1. Remove luer caps from luer connectors of catheter
and Start-Up Kit and discard or disconnect inflow
and outflow luers from each other.
2. Attach Start-Up K it to Icy
Catheter by connecting the male luer of the StartUp Kit to the female inflow luer of the Icy
Catheter and the female luer of the Start-Up Kit to
the male outflow luer o f the Icy
Assure that a sufficient amount of sterile saline is
present at t he ends of the hubs make an air free
connection.
3. Warning: Failure to connect the Start-Up Kit
correctly to the catheter could result in
catheter failure.
4. Warning: DO NOT confuse the INFLOW and
OUTFLOW Luer fittings for standard cent ral line
infusion ports. They are for connection to the
CoolGard 3000
ONLY.
5. Caution: Do not place any extra stopcocks in
line that may be inadvertently shut off. This
can cause line blockage and possible failure.
®
®
Heat Exchange
®
Catheter.
/Thermogard XP® System
®
Catheter Removal:
1. Stop all pumping of saline through the catheter.
2. Disconnect Start-Up Kit from ca theter. Uncap or
leave uncapped the inflow and outflow lumens
of the cooling circuit (coo ling circuit ONLY).
This will allow residual saline within the circuit to
be expressed . As catheter is withdrawn, the
balloons are compressed. Saline within the
balloons must be free to pass out of the balloon or
the balloon will not deflate making the catheter
difficult to r em ov e.
3. Place patient in supine po sition. Remove
dressing . Remove sutures fro m suture site.
4. Slowly remove catheter from patient. As catheter
exits the site apply pressur e with a dressing
impermeable to air, e.g. vaseline gauze.
5. Warning: Do not move catheter if resistance is
felt. Check to ensure that the inflow and
outflow lumens of the cooling circuit are NOT
capped. If they are capped, uncap them and
try removing the catheter again. If resistance
is still encountered, an x-ray should be
Page 5

Icy® Catheter
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
performed to identify the reason for the resistance.
ZOLL Circulation, Inc.
Sunnyvale, CA 94085
USA
+1-408-541-2140
Special Instructions for Guidewires
Note: This information applies only to the use of guidewires
in the Seldinger technique of catheter placement in the
vasculature.
Note: This procedure should be performed only after a
thorough review of technical references, wh ich emphasize
precautions, contr aindications, and risks in much greater
detail.
This spring guidewire was designed for single patient –
one time use only.
It is recommended that guidewires be discarded after one
use. No cleaning agents or techniques will complet el y
remove residual material from the guidewire after use.
INSPECTION
Guidewires should be routinely inspected prior to use and
discarded should any deformities be present in the guidewire.
Guidewire placement should be routinely monitored by x-ray
or fluoroscopic procedure.
CAUTIONS
Because of the delicate and fragile nature of guidewires,
extra care in handling must be taken. Avoid bending or
kinking.
During storage or procedures avoid coiling guidewires in less
than 8-inch diameters as smaller diameters place unnecessary
stress on the guidewires. The provided dispenser is the best
means of storage and handling of the guidewire.
Should resistance occur during insertion, DO NOT advance
guidewire.
Avoid withdrawing guidewire through me ta l needles;
guidewires may shear or PTFE coating may scrape off
against th e needle bevel.
Movable core of guidewire should not be advanced while
guidewire is in patient as this could cause damage to the
guidewire and possible injury to the vessel.
Sufficient guidewire length must remain exposed to maintain
firm grip on guidewire at all times.
PTFE coated guidewires must never be subject to ultra-sonic
cleaning or irradiation sterilization.
TECHNIQUE
1. PUNCTURE VESSEL
Needle Cannula in Vessel
2. Pass the guidewire thro ug h t he needle and
advance 5-10cm of the guidewire into the
punctured v essel. It may be necessary to
manipulate the guidewire in order to successfully
advance it. Usually a gentle, rotating motion is
sufficient to traverse an obstruction. Avoid rough
or overly vigorous manipulation of the guidewire
to prevent d amage to the guidewire or the vessel.
If “J” wire is used, prepare “J” guidewire by
sliding the plastic insertion sleeve over “J” tip to
straighten it. Insert the “J” guidewire into the
needle hub and gently advance it.
Guidewire in V essel
3. REMOVE
Needle Remov ed from Guidewire
4. DILATE TISSUE AND VESSEL WITH THE
DILATOR USING A SLIGHT ROTARY
MOTION.
5. REMOVE DILATOR. (Vessel dilator intend ed
for vascular dilation only.)
5 of 11 106085-001 Rev.2
Page 6

Icy® Catheter
FIG. 2
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
6. INTRODUCE CATHETER BY SLIDING IT OVER
THE GUIDEWIRE.
7. REMOVE GUIDEWIRE.
DISPENSER
Every guidewire is provided i n a un i que dispenser package.
It is recommended that the dispenser be filled with
heparinized solutions. (e.g. saline or dex trose) to bat he the
guidewire during insertion (Figure 2).
Preformed “J” guidewire will resume shape when removed
from product dispenser.
FIG.1
6 of 11 106085-001 Rev.2
Page 7

Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
ICY ® IC-3893
Icy® Catheter
Instructions for Use
7 of 11 106085-001 Rev.2
Page 8

Icy® Catheter
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
MRI Information .
The following models of th e ZOLL Heat Exchange Catheters have been determined to be MR-Conditional (formerly classified as
MRI-safe) according to the terminology specified in the American Society for Testing and Materials (ASTM) International,
Designation: F2503-05. Standa rd Practice for Marking Medical Devices and Other Items for Safet y i n the Magnetic R esonance
Environment. ASTM International, 100 Barr Harbor Drive, PO Box C700, West Conshohocken, Pennsylvania, 2005.
1. Cool Line
2. Icy
3. Quattro
Non-clinical testing demonstrated that these catheters ar e MR Conditional. A patient with this implant can be scanned safely immediately after placement under the following con ditions:
Magnetic Field Interactions
For magnetic field interactions,
-Static magnetic field of 1.5-Tesla or less
-Maximum spatial gradient magnetic field of 2.4 Tesla/meter or less
MRI-Related Heating
In non-clinical testing, these catheters produced the following temperature rises during MRI performed for 20-min in 1.5-Tesla
(1.5-Tesla/64-MHz, General electric Medical Systems, Milwaukee, WI) MR systems, as follows:
Highest temperature change MRI Condition
+0.6˚C 1.5-T/64-MHz
Therefore, the MRI-related heating experiments for these catheters at 1.5-Tesla using a transmit/receive RF body coil at MR system
reported whole body averaged SARs of 2.0-W/kg, indicated that the greatest amount of heating that occurred in association with these
specific conditions was equal to or less than 0.6˚C at 1.5-Tesla.
Artifact Information
MR image quality may be compromised if the area of interest is in the same area or relatively close to the position of these catheters.
The artifact size information is, as follows:
Pulse sequence T1-SE T1-SE GRE GRE
Signal Void Size <1,106-mm
®
®
®
2
<25-mm2 <1,857-mm2 <60-mm
2
Imaging Plane parallel perpendicular parallel perpendicular
Therefore, optimiza tion of MR imaging parameters to compensate for the presence of thes e catheters ma y be necessary.
8 of 11 106085-001 Rev.2
Page 9

Icy® Catheter
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
9 of 11 106085-001 Rev.2
Page 10

Icy® Catheter
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
10 of 11 106085-001 Rev.2
Page 11

Icy® Catheter
ICY
Instructions for Use
Model IC-3893A/8700-0657-01 (Also referre d to as IC-3893)
Silva Sorb Site Dressing
11 of 11 106085-001 Rev.2
 Loading...
Loading...