

3B Scientific Position of the Child before Birth Chart User Manual [en, ru, de, es, fr, it]
Page 1
V2068
(1001226/4006562)
Page 2

2
Page 3

®
English Presentations of the child prior
to the delivery
The developmental period of the child including individual deviations amounts to approximately 270 days.
As the date of the fertilization of the ovocyte is normally unknown, the first day of the last monthly period
is chosen as the basis for calculations. Therefore, the duration of pregnancy amounts to approximately 280
days, i.e. 10 (lunar) months with 28 days each (40 weeks). The embryo repeatedly turns during the progress
of the pregnancy and repeatedly assumes alternating positions in its extra-embryonic membranes. A certain section of the child (mostly the head) acquires closer relations to the parturient canal of the maternal
pelvis during the final 3 - 4 weeks of pregnancy and maintains this position as well. Not until now, the term
“presentation“ is correct.
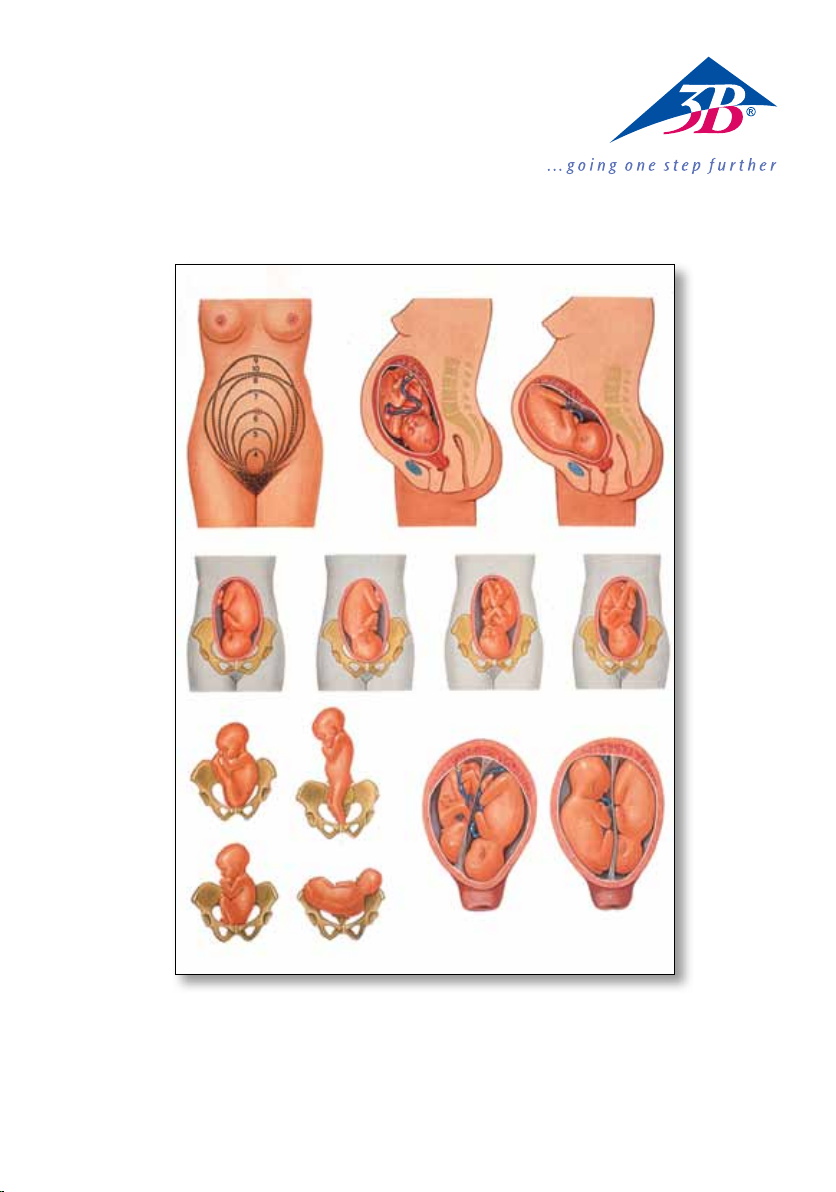
Enlargement of the uterus during the indi-vidual months of pregnancy (fig. 1 to 3)
Fig. 1 displays the enlargement of the uterus which can be determined by external examination from the
4th to the 10th month of pregnancy. The recorded numbers correspond with the end of the
respective month. The uterus is externally (through the abdominal wall) not tactual until the beginning of
the 4th month. From the middle of the 4th month on, the upper part of the uterus (fundus uteri) ascends
from the “small pelvis“ over the pubic symphysis, reaches both costal arches at the end of the 9th month
and then descends again during the 10th month of pregnancy.
At the end of the respective month of pregnancy, the fundus is located at the following position:
4th month: closely below the pubic symphysis
5th month: below the umbilicus
6th month: exactly at the level of the umbilicus
7th month: above the umbilicus
8th month: in the middle between the umbilicus and the ensiform appendix of the xiphoid bone
9th month: fundus reaches the costal arch (highest position)
10th month: fundus descends to the position of the 8th month
The descending of the fundus - which takes place in primiparous women 4 weeks and in multiparous
women 3 weeks prior to the delivery - conditions an alteration of the shape of the abdomen of the expectant mother: the abdomen descends and protrudes more intensely (fig. 3 compared with fig. 2), the uterus
becomes wider (refer to fig. 1: condition at the end of the 10th month). The umbilicus lapses and often
protrudes.
Fig. 2 and 3 display the profile of the abdomen of an expectant mother, the position of the uterus and the
position of the infantile head at the end of the 9th month (fig. 2) and during the 10th month (fig. 3). The
highest position of the uterus respectively corresponds with the peak of the outlines displayed in fig. 1. At
the end of the 9th month (fig. 2), the uterus is upright and it touches the costal arch. The head is loosely
positioned above the superior
pelvic aperture.
During the 10th month of pregnancy (fig. 3), the fundus descends, the abdomen “slides“ lower, the uterus
becomes wider (refer to fig. 1, 10th month). The lower section of the uterus is shortened due to the integration of the lower uterine segment and the infantile head has entered the pelvis.
Presentations (fig. 4 to 13)
The figures serve for the illustration of some essential presentations and positions. The following distinctions are made:
Presentations: Proportion of the infantile to the maternal longitudinal axis
Positions: Direction of the infantile back in proportion to the maternal sides (left, right, front etc.)
3
Page 4

®
Presentations of the child prior
English
to the delivery
Postures: Angle of inclination of the infantile head in proportion to the longitudinal axis of the
Engagements: Anterior part of the child during the appearance through the parturient canal (sinciput, occi-
Presentation and position are determined as follows:
infantile body (flexion, extension)
put, forehead, feet, breech etc.)
1st (first) presentation: the back (in longitudinal presentations) or the head (in transverse
2nd (second) presentation: opposed to the 1st presentation
In addition to the exact direction of the infantile back to the left or the right, there are intermediate positions in which the back in longitudinal presentations can point more to the front (dorso-anterior), to the
back (dorso-posterior) or in transverse presentations to the front (dorso-anterior), to the back (dorso-posterior), upwards (dorso-superior) or downwards (dorso-inferior). The following figures convey an impression
of the approximate frequency of the individual presentations:
100 deliveries
Longitudinal Cephalic Regular cephalic
presentations presentations presentations
(99%) (96%) (94%)
Transverse Breech Irregular cephalic
presentations presentations presentations
(1%) (3%) (2%)
Occipito-anterior presentations (fig. 4 and 5)
Among 100 deliveries, there are approximately 94 regular normal cephalic presentations.
Fig. 4: 1st occipito-anterior presentation: most frequent position
Fig. 5: 2nd occipito-anterior presentation
The occipito-anterior presentation is the most favourable presentation imaginable as it entails the least
jeopardy to mother and child in comparison with other presentations.
presentations) of the child points to the left side of the mother
Occipito-posterior presentations (fig. 6 and 7)
Irregular cephalic presentations (occipito-posterior presentations, vertex presentations, brow and face
presentations) occur in approximately 2 % of the deliveries.
Fig. 6: 1st occipito-posterior presentation: most frequent position
Fig. 7: 2nd occipito-posterior presentation
The difference from the occipito-anterior presentation is the more backwards turned position of the infantile back (dorso-posterior position). The occiput (and thus the back) can still turn forwards during the delivery so that the further course of the delivery corresponds with the course in case of an occipito-anterior
presentation.
4
Page 5

®
English
Presentations of the child prior
to the delivery
The more exceptional irregular cephalic presentations (vertex, brow and face presentations) increase the
jeopardy to mother and child or are even unsuitable for a delivery.
Breech presentations (fig. 8, 9 and 10)
The presentation in question is a breech presentation if in case of a longitudinal presentation the head is
not the anterior part. This is the case in approxi-mately 3 % of all deliveries. The breech presentations are
given special designations according to the fact whether the breech, both feet, the breech and both feet or
the breech and one foot are anterior:
The figures 8, 9 and 10 display 1st breech presentations (back to the left):
Fig. 8: perfect breech presentation
Fig. 9: double footling presentation
Fig. 10: complete footling presentation
Breech presentations increase the risk of delivery for mother and child so that under certain circumstances
a caesarian section must be done. As the anterior part of the child always has a smaller circumference than
the head in case of breech presentations, the dilatation of the cervical os of the uterus which commences
with the beginning of the labour is inadequate and delayed. This will result in a considerable extension of
the duration of labour with an increasing jeopardy to mother and child.
Transverse presentations (fig. 11)
Transverse presentations which amount to approximately 1 % of all deliveries are at issue when the longitudinal axis of the child cuts the longitudinal axis of the mother square or at an angle. Among the possible
positions of transverse presentations, the frequent 1st dorso-anterior transverse presen-tation (head to the
left, back pointing forwards) is displayed in fig. 11. Transverse presentations are unsuitable for deliveries
which (unattended) will lead to the death of mother and child.
The origin of a transverse presentation is mostly based on disturbances of the normal presentation of the
head as the leading part (twins, deformed pelvis, malformations of the uterus, placenta located in front of
the cervical os etc.).
Twins (fig. 12 and 13)
One twin delivery falls to 80 - 90 deliveries. The displayed images do not indicate whether the twins in question are monozygotic or dizygotic twins.
The presentation of both children to each other is equal or different. The presentation of both children is
mostly a cephalic presentation (fig. 12; 45 % of the twin deliveries) or one child in cephalic presentation,
the other one in pelvic presentation (fig. 13; 35 % of the twin deliveries). According to the frequency, the
next presentations are: both children in breech presentation, cephalic presentation combined with transverse presentation, breech presentation combined with transverse presentation, both children in transverse
presentation.
The delivery is mostly spontaneous in the course of which the second child follows approximately 30
minutes after the delivery of the first child.
5
Page 6

®
DeutschLagen des Kindes vor der Geburt
Die Entwicklungsdauer des Kindes beträgt mit individuellen Abweichungen ungefähr 270 Tage. Da der
Zeitpunkt der Befruchtung der Eizelle meist unbekannt ist, wird der erste Tag der letzten aufgetretenen
Regelblutung als Berechnungstermin gewählt. Somit beträgt die Schwangerschaftsdauer annähernd 280
Tage, d. h. 10 (Mond-) Monate zu je 28 Tagen (40 Wochen). Im Verlaufe der Schwangerschaft dreht sich
der Keimling wiederholt und nimmt innerhalb seiner Eihäute mehrmals wechselnde Lagen ein. In den
letzten 3-4 Schwangerschaftswochen erhält ein bestimmter Abschnitt des Kindes (meist der Kopf) engere
Beziehungen zum Durchtrittskanal des mütterlichen Beckens und behält diese Lage auch bei. Erst jetzt
trifft die Bezeichnung „Geburtslage“ zu.
Vergrößerung der Gebärmutter in den einzelnen Schwangerschaftsmonaten (Abb. 1 bis 3)
Abb. 1 gibt die durch äußerliche Untersuchung feststellbare Vergrößerung der Gebärmutter vom 4. - 10.
Schwangerschaftsmonat wieder. Die eingetragenen Zahlen entsprechen dem Ende des jeweiligen Monats.
Bis zum Beginn des 4. Monats ist die Gebärmutter äußerlich (durch die Bauch-decke hindurch) nicht tastbar. Von der Mitte des 4. Monats an steigt der obere Teil der Gebärmutter (Fundus uteri) aus dem „kleinen
Becken“ heraus über die Schambeinfuge (Symphyse), erreicht am Ende des 9. Monats beide Rippenbögen
und sinkt im 10. Schwangerschaftsmonat wieder ab.
Am Ende des jeweiligen Schwangerschaftsmonats steht der Fundus in folgender Höhe:
4. Monat: dicht unterhalb der Symphyse
5. Monat: unterhalb des Nabels
6. Monat: genau in Nabelhöhe
7. Monat: oberhalb des Nabels
8. Monat: Mitte zwischen dem Nabel und dem Schwertfortsatz des Brustbeins
9. Monat: Fundus erreicht den Rippenbogen (höchster Stand)
10. Monat: Fundus sinkt auf den Stand des 8. Monats
Das Absinken des Fundus, das bei erstgebärenden Frauen 4 Wochen, bei mehrgebärenden 3 Wochen vor
der Geburt erfolgt, bedingt eine Veränderung der Bauchform der Schwangeren: der Bauch sinkt ab und
wölbt sich stärker vor (Abb. 3 gegenüber Abb. 2), die Gebärmutter wird breiter (s. Abb. 1: Stand am Ende des
10. Monats). Der Nabel verstreicht, oft wölbt er sich vor.
Die Abb. 2 und 3 geben das Profil des Bauches einer Schwangeren, die Stellung der Gebärmutter und der
Höhenstand des kindlichen Kopfes am Ende des 9. Monats (Abb. 2) und im Verlauf des 10. Monats (Abb.
3) wieder. Der höchste Punkt der Gebärmutter entspricht jeweils dem Scheitel der auf Abb. 1 eingetragenen Konturen. Am Ende des 9. Monats (Abb. 2) ist die Gebärmutter hoch aufgerichtet, sie berührt den
Rippenbogen. Der Kopf steht locker über dem Beckeneingang.
Im Verlauf des 10. Schwangerschaftsmonats (Abb. 3) sinkt der Fundus ab, der Bauch „rutscht“ tiefer, die
Gebärmutter wird breiter (s. Abb. 1, 10. Monat). Der untere Abschnitt der Gebärmutter ist infolge der
Einbeziehung des unteren Uterinsegments verkürzt und der kindliche Kopf in das Becken eingetreten.
Geburtslagen (Abb. 4 bis 13)
Die Abbildungen dienen der Erläuterung einiger wesentlicher Kindeslagen und -stellungen. Es werden
unterschieden:
Lagen: Verhältnis der Längsachse des Kindes zu der der Mutter
Stellungen: Richtung des kindlichen Rückens zu den Seiten der Mutter (links, rechts-vorn u. a.)
Haltungen: Neigung des kindlichen Kopfes zur Längsachse des kindlichen Körpers (Beugung,
Streckung)
Einstellungen: Vorangehender Teil des K ind es beim D urchtritt durch den G ebu rtskanal
(Hinterhaupt, Vorderhaupt, Stirn, Füße, Steiß, u. a.)
6
Page 7
®
Deutsch
Lage und Stellung werden wie folgt ausgedrückt:
Lagen des Kindes vor der Geburt
I. (erste) Lage: der Rücken (bei Längslagen) oder der Kopf (bei Querlagen) des Kindes weist zur
II. (zweite) Lage: entgegengesetzt der I. Lage
Außer der genauen Richtung des kindlichen Rückens nach links oder rechts gibt es Zwischen-stellungen,
bei denen der Rücken bei Längslagen mehr nach vorn (dorso-anterior), nach hinten (dorso-posterior) oder
bei Querlagen nach vorn (dorso-anterior), nach hinten (dorso-posterior), nach oben (dorso-superior) oder
nach unten (dorso-inferior) zeigen kann. Die folgenden Zahlen vermitteln einen Eindruck der annähernden
Häufig-keit der einzelnen Kindeslagen:
100 Geburten
Längslagen Schädellagen regelrechte
Schädellagen
(99 %) (96 %) (94 %)
Querlagen Beckenendlage regelwidrige
Schädellagen
(1 %) (3 %) (2 %)
Vordere Hinterhauptslagen (Abb. 4 und 5)
Unter 100 Geburten finden sich ca. 94 regelrechte, normale Schädellagen.
Abb. 4: I. vordere Hinterhauptslage: häufigste Stellung
Abb. 5: II. vordere Hinterhauptslage
Die vordere Hinterhauptslage ist die denkbar günstigste Geburtslage, da sie im Vergleich mit anderen
Kindeslagen die geringste Gefährdung für Mutter und Kind mit sich bringt.
linken Seite der Mutter
Hintere Hinterhauptslagen (Abb. 6 und 7)
Regelwidrige Schädellagen (hintere Hinterhaupts-lagen, Vorderhauptslagen, Stirn-, Gesichtslagen) kommen
in ca. 2 % der Geburten vor.
Abb. 6: I. hintere Hinterhauptslage: häufigste Stellung
Abb. 7: II. hintere Hinterhauptslage
Der Unterschied zur vorderen Hinterhauptslage besteht in der mehr nach hinten gerichteten Stellung des
kindlichen Rückens (dorso-posteriore Stellung). Während der Geburt kann sich das Hinterhaupt (und damit
der Rücken) noch nach vorn drehen, so daß der weitere Geburtsverlauf dem der vorderen Hinterhauptslage
entspricht.
Die selteneren regelwidrigen Schädellagen (Vorder-- haupts-, Stirn-, Gesichtslage) erhöhen die Gefahr für
Mutter und Kind oder sind sogar gebärunfähig.
Beckenendlagen (Abb. 8, 9 und 10)
Ist bei einer Längslage nicht der Kopf der voran-gehende Teil, handelt es sich um eine Beckenend-lage.
7
Page 8

®
DeutschLagen des Kindes vor der Geburt
Diese machen ca. 3 % aller Geburten aus. Je nachdem, ob der Steiß, beide Füße, der Steiß und beide Füße,
oder der Steiß und ein Fuß vorliegen, werden die Beckenendlagen besonders benannt:
Die Abbildungen 8, 9 und 10 stellen I. Beckenendlagen (Rücken links) dar:
Abb. 8: reine Steißlage
Abb. 9: vollkommene Fußlage
Abb. 10: vollkommene Steiß-Fuß-Lage
Beckenendlagen erhöhen das Geburtsrisiko für Mutter und Kind, so daß unter bestimmten Vorbedingungen der Kaiserschnitt ausgeführt werden muß. Da der vorangehende Kindesteil bei Beckenendlagen stets einen kleineren Umfang hat als der Kopf, ist die mit Wehenbeginn einsetzende Weitung
des Muttermundes der Gebärmutter mangelhaft und zeitlich verzögert. Daraus ergibt sich eine erhebliche
Verlängerung der Geburtsdauer mit zunehmender Gefährdung von Mutter und Kind.
Querlagen (Abb. 11)
Querlagen, die ca. 1 % aller Geburten ausmachen, liegen vor, wenn die Längsachse des Kindes die der
Mutter rechtwinklig oder schräg schneidet. Unter den möglichen Stellungen von Querlagen ist auf Abb. 11
die häufige I. dorso-anteriore Querlage (Kopf links, Rücken zeigt nach vorn) dargestellt. Querlagen sind
gebärunfähige Kindeslagen, die (unbehandelt) zum Tode von Mutter und Kind führen.
Der Entstehung einer Querlage liegen meist Behinderungen der normalen Einstellung des Kopfes als führendem Teil zugrunde (Zwillinge, verformtes Becken, Mißbildungen der Gebärmutter, vor dem Muttermund
liegender Mutterkuchen u. a.).
Zwillinge (Abb. 12 und 13)
Auf 80-90 Geburten entfällt eine Zwillingsgeburt. Die dargestellten Abbildungen geben keinen Hinweis, ob
es sich um eineiige oder zweieiige Zwillinge handelt.
Die Lage beider Kinder zueinander ist gleich oder verschieden. Meist befinden sich beide in Schädel-lage
(Abb. 12; 45 % der Zwillingsgeburten) oder ein Kind in Schädellage, das andere in Beckenlage (Abb. 13; 35 %
der Zwillingsgeburten). Der Häufigkeit nach geordnet folgen: beide Kinder in Beckenendlage, Schädellage
kombiniert mit Querlage, Beckenendlage kombiniert mit Querlage, beide Kinder in Querlage.
Meist kommt es zur spontanen Geburt, wobei der Zwilling ca. 30 Minuten nach der Geburt des ersten
Kindes folgt.
8
Page 9

®
Español
Posiciones del niño antes del
alumbramiento
La duración del desarrollo del niño, con excepciones particulares, asciende a aproximadamente 270 días.
Teniendo en cuenta que el momento de la fecundación del óvulo es en la mayoría de los casos desconocido, se elige el primer día de la última menstruación sucedida como la fecha para el cálculo. De esta forma
asciende la duración del embarazo a aproximadamente 280 días, es decir, 10 meses lunares de, cada uno,
28 días (40 semanas). En el transcurso del embarazo el embrión se revuelve repetidas veces y adquiere,
dentro de sus membranas ovulares, posiciones cambiantes. En las últimas 3-4 semanas del embarazo una
determinada parte del niño (con frecuencia la cabeza) adquiere una estrecha relación respecto al canal
de conducción de la pelvis materna y mantiene esa posición. Sólo entonces es adecuada la denominación
“posición o presentación del alumbramiento“.
Expansión de la matriz en cada uno de los meses del embarazo (Figuras 1 a 3)
La Figura 1 reproduce la expansión de la matriz del cuarto al décimo mes del embarazo, determinada
mediante reconocimiento externo. Las cifras consignadas corresponden al final del respectivo mes. Hasta
comienzos del cuarto mes la matriz no es palpable exteriormente (a través de la pared abdominal). Desde
mediados del cuarto mes sale de la “pelvis pequeña“ hacia arriba la parte superior de la matriz (fundus
uteri), sobre la sínfisis (symphyse), alcanza a finales del noveno mes ambos arcos costales y decae de nuevo
en el décimo mes del embarazo.
Al final de cada uno de los respectivos meses del embarazo el fundus alcanza la siguiente altura:
Cuarto mes: muy por debajo de la sínfisis
Quinto mes: por debajo del ombligo
Sexto mes: exactamente a la altura del ombligo
Séptimo mes: por encima del ombligo
Octavo mes: a media altura entre el ombligo y el apéndice xifoides del esternón
Noveno mes: el fundus alcanza el arco costal (posición más alta)
Décimo mes: el fundus desciende a la posición del octavo mes
El hundimiento del fundus, que sucede cuatro semanas antes del alumbramiento en mujeres del primer
parto y tres semanas antes en mujeres de varios partos, condiciona una variación de la forma del vientre
de las embarazadas: el vientre se hunde y se abomba notablemente (Figura 3 respecto a la Figura 2), la
matriz se ensancha (ver la Figura 1: estado al final del décimo mes). El ombligo se tapa; con frecuencia se
abomba.
Las Figuras 2 y 3 reproducen el perfil del vientre de una embarazada, la posición de la matriz y la posición
elevada de la cabeza del niño al final del noveno mes (Figura 2) y en el curso del décimo mes (Figura 3). El
punto más elevado de la matriz corresponde respectivamente a la coronilla de los contornos trazados en
la Figura 1. Al final del noveno mes (Figura 2) se ha ensalzado al máximo la matriz y roza el arco costal. La
cabeza se presenta suelta sobre la entrada de la pelvis.
En el transcurso del décimo mes del embarazo (Figura 3) se hunde el fundus, el vientre “se desliza“ hacia
abajo, la matriz se ensancha (ver la Figura 1, décimo mes). La sección inferior de la matriz está representada acortada, como consecuencia de la inclusión del segmento uterino inferior y de la entrada de la cabeza
del niño en la pelvis.
Posiciones del alumbramiento (Figuras 4 a 13)
Las figuras sirven para el esclarecimiento de algunas de las posiciones y presentaciones más importantes
del niño. Se diferencian:
Posiciones: Relación del eje longitudinal del niño al de la madre
9
Page 10

®
Posiciones del niño antes del
Español
alumbramiento
Posturas: Dirección de la espalda del niño respecto al costado de la madre (hacia la izquierda, hacia
Actitudes: Tendencia de la cabeza del niño respecto al eje longitudinal del cuerpo del niño (flexión,
Colocaciones: Parte avanzada del niño en el paso a través del canal del alumbramiento (parte posterior de
La posición y la postura se expresan del siguiente modo:
la derecha, hacia el frente, entre otras)
distensión)
la cabeza, parte anterior de la cabeza, frente, pies, trasero, etc.)
I. (primera) posición: la espalda (en posiciones longitudinales) o la cabeza (en posiciones transversales) del
II. (segunda) posición: contraria a la posición I.
Además de la dirección exacta de la espalda del niño hacia la izquierda o hacia la derecha, se dan posturas
intermedias, en las que la espalda, para posiciones longitudinales, puede mostrarse más hacia adelante
(dorso-anterior), hacia atrás (dorso-posterior), o, para posiciones transversales, más hacia adelante (dorsoanterior), hacia atrás (dorso-posterior), hacia arriba (dorso-superior) o hacia abajo (dorso-inferior). Las siguientes cifras facilitan una impresión de la frecuencia aproximada de cada una de las posiciones del niño:
100 nacimientos
Posiciones Posiciones Posiciones cefálicas
longitudinales cefálicas correctas
(99%) (96%) (94%)
Posiciones Presentacíon de Posiciones cefálicas
transversales extremidad pélvica irregulares
(1%) (3%) (2%)
Posiciones occipitales anteriores (Figuras 4 y 5)
De entre 100 alumbramientos se dan aprox. 94 presentaciones cefálicas normales.
Figura 4: I. posición occipital anterior: la postura más frecuente
Figura 5: II. posición occipital anterior
La posición occipital anterior se la supone como la posición del alumbramiento más favorable, ya que ésta,
en comparación con otras posiciones del niño, lleva consigo el menor peligro para la madre y para el niño.
niño señala el costado izquierdo de la madre
Posiciones occipitales posteriores (Figura 6 y 7)
Posiciones cefálicas irregulares (posiciones occipitales posteriores, posiciones occipitales anteriores, posiciones de la frente y de la cara) se presentan en aprox. 2% de los alumbramientos.
Figura 6: I. posición occipital posterior: la postura más frecuente
Figura 7: II. posición occipital posterior
La diferencia respecto a la posición occipital anterior consiste en la postura orientada más hacia atrás de
la espalda del niño (posición dorso-posterior). Durante el alumbramiento se puede todavía girar la parte
occipital de la cabeza (y con ello la espalda) hacia adelante, de forma que el ulterior transcurso del alumbramiento se corresponde con el de la posición occipital anterior.
10
Page 11

®
Español Posiciones del niño antes del
alumbramiento
Las posiciones cefálicas irregulares muy poco frecuentes (posición de la cabeza anterior, de la frente, de
la cara) acrecientan el peligro para la madre y para el niño o incluso no son aptas para el alumbramiento.
Presentaciones de extremidad pélvica (Figuras 8, 9 y 10)
Cuando en una posición longitudinal no es la cabeza la parte más adelantada, se trata de una presentación
de extremidad pélvica. Estas constituyen aprox. el 3% de todos los alumbramientos. Según se presenten el
trasero, ambos pies, el trasero y ambos pies o el trasero y un pie, tienen las diferentes posiciones diferente
denominación:
Las Figuras 8, 9 y 10 representan las presentaciones de extremidad pélvica I. (espalda a la izquierda):
Figura 8: posición del trasero pura
Figura 9: posición perfecta del pie
Figura 10: posición perfecta de trasero-pie
Las presentaciones de extremidad pélvica incrementan el riesgo de alumbramiento para la madre y el
niño, de forma que, bajo determinadas condiciones, sea necesario realizar la operación cesárea. Dado
que la parte del niño que precede en las presentaciones de extremidad pélvica tiene un perímetro menor
que la cabeza, el ensanchamiento del orificio uterino de la matriz, que se inicia con los comienzos de las
contracciones del alumbramiento, es deficiente y retardado. De aquí resulta un notable alargamiento de la
duración del parto, con incremento creciente de la peligrosidad para la madre y para el niño.
Posiciones transversales (Figura 11)
Las posiciones transversales, que representan aprox. el 1% de todos los alumbramientos, se presentan
cuando el eje longitudinal del niño corta al de la madre en ángulo recto u oblicuamente. De entre las
posibles posturas de posiciones transver-sales se representa en la Figura 11 la posición transversal más
frecuente I. dorso-anterior (la cabeza señala hacia la izquierda y la espalda hacia adelante). Posiciones
transversales son posturas del niño no aptas para el alumbramiento, las cuales, si no se corrigen, llevan a
la muerte de la madre y del niño.
El origen de una posición transversal tiene como causa frecuentemente impedimentos de la colocación
normal de la cabeza, como parte conductora (gemelos, pelvis deformada, deformación de la matriz, placenta dispuesta delante del orificio uterino, entre otras).
Gemelos (Figuras 12 y 13)
De cada 80-90 alumbramientos se da un nacimiento de gemelos. Las figuras presentadas no muestran ninguna indicación, de si se trata de gemelos uniovulares o biovulares.
La posición de ambos niños entre sí es la misma o diferente. Con frecuencia se hallan ambos en presentación cefálica (Figura 12; 45% de los nacimientos de gemelos), o bien un niño en presentación cefálica y el
otro en presentación de extremidad pélvica (Figura 13; 35% de los nacimientos de gemelos). El orden de
frecuencia es como sigue: ambos niños en presentación de extremidad pélvica, presentación cefálica combinada con posición transversal, presentación de extremidad pélvica combinada con posición transversal,
ambos niños en posición transversal.
Con frecuencia se presenta un alumbramiento espontáneo, en el que el gemelo sigue aprox. 30 minutos
después del nacimiento del primer niño.
11
Page 12

®
Positions de l’enfant avant la naissance
En tenant compte des écarts individuels, la durée de développement de l’enfant est d’environ 270 jours.
Etant donné que la plupart du temps, la date de fécondation de l’ovule n’est pas connue, pour calculer
la date de la naissance, on prend le premier jour des dernières règles. Ainsi, la durée de grossesse est
d’environ 280 jours, i.e. 10 mois (lunaires) de 28 jours chacun (40 semaines). Au cours de la grossesse,
l’embryon se retourne de façon répétée et change de position plusieurs fois à l’intérieur du chorion. Dans
les 3 à 4 dernières semaines de la grossesse, une certaine partie de l’enfant (le plus souvent la tête) a des
rapports plus étroits avec le canal de passage du bassin maternel et conserve cette position. Ce n’est qu’à
partir de ce moment-là que l’on peut parler de « position de naissance ».
Augmentation de l’utérus au cours de chaque mois de la grossesse. (Fig. 1 à 3)
Fig. 1 représente par examen extérieur l’augmentation constatable de l’utérus du 4e au 10e mois de grossesse. Les nombres qui y figurent corres-pondent à la fin du mois respectif. Jusqu’au début du 4e mois,
l’utérus n’est pas palpable extérieurement (à travers l’abdomen). A partir du milieu du 4e mois, le fond de
l’utérus (Fundus uteri) croît et sort du « petit bassin » par la symphyse pubienne, et atteint les deux rebords
costaux à la fin du 9e mois et descend à nouveau au 10e mois de grossesse.
A la fin de chaque mois de la grossesse le fond se trouve aux hauteurs respectives suivantes :
4e mois : tout juste au dessous de la symphyse
5e mois : sous le nombril
6e mois : exactement à la hauteur du nombril
7e mois : au-dessus du nombril
8e mois : au milieu entre le nombril et l’extrémité inférieure du sternum
9e mois : le fond atteint le bord des côtes (état le plus haut)
10e mois : le fond descend au niveau du 8e mois
La descente du fond qui, chez les femmes dont c’est le 1er enfant, se produit 4 semaines avant la naissance, et chez celles qui en ont déjà eu, 3 semaines avant. Ceci provoque un changement de la forme du
ventre de la femme enceinte : le ventre descend et se courbe plus vers l’avant (fig. 3 par rapport à la fig. 2),
l’utérus s’élargit (cf. fig. 1 : état à la fin du 10e mois). Le nombril s’étend, il est fréquent qu’il ressorte.
Français
Les fig. 2 et 3 représentent le profil du ventre d’une femme enceinte, la position de l’utérus et le niveau
de hauteur de la tête de l’enfant à la fin du 9e mois (fig. 2) et au cours du 10e mois (fig. 3). Le point le
plus haut de l’utérus correspond respectivement au sommet porté sur la fig. 1. A la fin du 9e mois (fig. 2),
l’utérus est très haut, il touche le rebord costal. La tête se trouve au-dessus de l’entrée du bassin.
Au cours du 10e mois de la grossesse (fig. 3), le fond descend, le ventre « glisse » vers le bas, l’utérus
s’élargit (cf. fig. 1, 10e mois). La partie inférieure de l’utérus est raccourci par suite de tirage du segment
utérin inférieur et la tête de l’enfant est engagée dans le bassin.
Positions de naissance (Fig. 4 à 13)
Les figures servent à expliquer quelques positions importantes de l’enfant. On fait la différence entre :
Positions : Rapport de l’axe longitudinal de l’enfant à celui de la mère
Présentations : Sens du dos de l’enfant par rapport aux côtés de la mère (à droite, gauche, devant entre
Tenues : Inclinaison de la tête de l’enfant par rapport à l’axe longitudinal du corps de l’enfant
Attitudes : Partie de l’enfant qui passe en premier par la filière pelvigénitale (sommet occipito-
12
autres)
(courbure, allongement)
antérieur, postérieur, front, pieds, siège entre autres.)
Page 13

®
Français
La position et la présentation sont exprimées comme suit :
Positions de l’enfant avant la naissance
1ère (première) position : le dos (présentation longitudinale) ou la tête (en positions de l’épaule) de
2e (deuxième) position : opposée à la 1ère position.
En dehors de la direction exacte du dos de l’enfant vers la gauche ou vers la droite, il y a des positions
intermédiaires dans lesquelles le dos en présentations longitudinales est plus vers l’avant (dorso-anterior),
vers l’arrière (dorso-posterior), ou dans les positions d’épaule vers l’avant (dorso-anterior), vers l’arrière
(dorso-posterior), vers le haut (dorso-superior) ou vers le bas (dorso-inferior). Les nombres suivants donnent
une idée de la fréquence approximative des différentes positions de l’enfant :
100 naissances
Positions Positions Positions du sommet
longitudinales du sommet normales
(99%) (96%) (94%)
Positions Positions Positions du sommet
d’épaule du siège anormales
(1%) (3%) (2%)
Positions du sommet-occipito antérieures (Fig. 4 et 5)
Sur 100 naissances, il y a env. 94 positions du sommet occipito-iliaque correctes, normales.
Fig. 4: I. position du sommet occipito-antérieure : position la plus fréquente
Fig. 5: II. position du sommet occipito-antérieure
La position du sommet occipito-antérieure est la position de naissance la plus favorable puisqu’en comparaison avec d’autres présentations de l’enfant, elle présente le risque le plus faible pour la mère et l’enfant.
l’enfant est dirigé vers le côté gauche de la mère.
Positions du sommet occipito-postérieure (Fig. 6 et 7)
Des positions du sommet occipito-iliaque anormales ( positions du sommet occipito-postérieures, positions
du bregma, positions du front, positions de la face) se présentent dans env. 2% des naissances.
Fig. 6: I. position du sommet occipito-postérieure : position la plus fréquente
Fig. 7: II. position du sommet occipito-postérieure
La différence avec la position du sommet occipito-antérieure réside dans la position du dos de l’enfant
(position dorso-posteriore) qui est orienté plus vers l’arrière. Pendant la naissance, il est possible que le
sommet-occipito (et en même temps le dos) se retourne vers l’avant de telle sorte que la suite du déroulement de la naissance corresponde à la position du sommet-occipito antérieure.
Les positions sommet-occipito anormales plus rares (positions du bregma, position du front, position de la
face) augmentent les risques pour la mère et l’enfant ou rendl’accouchement même impossible.
Positions du siège (Fig. 8, 9 et 10)
Si, dans une présentation longitudinale, la tête n’est pas la partie qui précède, il s’agit alors d’une position du siège. Celle-ci représente env. 3% de toutes les naissances. Selon que ce sont, soit le siège, les deux
pieds, le siège et les deux pieds, soit le siège et un pied qui précèdent, les positions du siège dorso-iliaque
portent les noms suivants :
13
Page 14

®
Positions de l’enfant avant la naissance
Les figures 8, 9 et 10 représentent I. positions du siège dorso-iliaque (le dos à gauche) :
Fig. 8 : position du siège pure
Fig. 9 : présentation parfaite des pieds
Fig. 10 : présentation parfaite du siège-pieds
Les présentations du siège augmentent les risques de la naissance pour la mère et l’enfant de telle sorte
que dans certaines conditions, une césarienne s’impose. Etant donné que dans les cas de présentation de
siège, la partie de l’enfant qui précède a toujours une circonférence plus petite que la tête, l’ouverture de
l’orifice utérin qui commence dès les premières douleurs est insuffisante et retardée. Il en résulte donc
une grande augmentation de la durée de la naissance entraînant de plus grands risques pour la mère et
l’enfant.
Positions de l’épaule (Fig. 11)
Les positions de l’épaule qui représentent env. 1% de toutes les naissances arrivent quand l’axe longitudinal
de l’enfant recoupe celui de la mère à angle droit ou incliné. Parmi les présentations possibles des positions de l’épaule, la fig. 11 représente la position I. de l’épaule en dorso-antérieure (tête à gauche, le dos
étant dirigé vers l’avant) la plus fréquente. Les positions de l’épaule sont des présentations qui ne permettent pas d’accoucher, et lesquelles, si elles ne sont pas traitées entraînent la mort de la mère et de l’enfant.
Les raisons d’une position de l’épaule sont le plus souvent dues à des empêchements de la position normale de la tête en tant que partie qui précède ( jumeaux, bassin déformé, malformations de l’utérus, placenta
se trouvant devant l’orifice utérin entre autres).
Jumeaux (Fig. 12 et 13)
Sur 80 à 90 naissances, il y a une naissance de jumeaux. Les figures représentées n’indiquent pas s’il s’agit
de vrais ou de faux jumeaux.
Français
La position des deux enfants l’un par rapport à l’autre est pareille ou différente. Le plus souvent, ils se
trouvent tous les deux en position du sommet (fig. 12 ; 45% de naissances de jumeaux) ou un enfant est en
position du sommet, l’autre en position du siège (fig. 13 ; 35% des jumeaux). La fréquence est la suivante
par ordre : les deux enfants en présentation du siège, présentation du sommet combinée avec la position
de l’épaule, position du siège combinée avec la position de l’épaule, les deux enfants en position de
l’épaule.
La plupart du temps, il y a naissance spontanée, le jumeau venant au monde env. 30 minutes après le premier enfant.
14
Page 15

®
Português
Apresentações da criança antes
do parto
O período de desenvolvimento de uma criança incluindo-se suas diferenças individuais é de aproximadamente 270 dias. Como a data de fertilização do óvulo é normalmente desconhecida, o primeiro dia do
último período mensal é escolhido como base para os cálculos. No entanto, a duração da gravidez é de
aproximadamente 280 dias, ou seja, 10 meses lunares com 28 dias cada (40 semanas). O embrião move-se
repetidas vezes durante o processo de gravidez e repetidas vezes assume posições diferentes em suas membranas extra-embriônicas. Uma certa parte da criança (na maioria dos casos a cabeça) entra em contato
muito próximo com o canal parturiente da pelve materna no decorrer das últimas 3 ou 4 semanas de gravidez e mantém essa posição. Até esse momento não é usado o termo “apresentação“.
Aumento do útero durante cada mês da gravidez (figs. 1 a 3)
A figura 1 mostra o aumento do útero que pode ser determinado através de um exame externo à partir do
4º até o 10º mês de gravidez. Os números registrados correspondem aos do final de cada mês respectivo. O
útero não pode ser tocado externamente (através da parede abdominal) até o início do 4º mês. Da metade
do 4º mês em diante, a parte superior do útero (fundo uterino) ascende sobre a “pequena pelve“ acima
da sínfise púbica, alcançando os dois arcos costais ao final do 9º mês e então descendendo novamente
durante o 10º mês de gravidez.
Ao final do respectivo mês de gravidez, o fundo uterino está localizado na seguinte posição:
4º mês: um pouco abaixo da sínfise púbica
5º mês: abaixo do umbigo
6º mês: exatamente ao nível do umbigo
7º mês: acima do umbigo
8º mês: na metade entre o umbigo e a vesícula ensiforme do osso xifóide
9º mês: o fundo atinge o arco costal (posição mais elevada)
10º mês: o fundo descende à posição do 8º mês
A descendência ao fundo - que ocorre 4 semanas antes do parto em mulheres primíparas e 3 semanas para
mulheres multíparas - condicionam uma alteração no formato do abdome da mãe: o abdome desce e projeta-se mais intensamente (figura 3 comparada à figura 2), o útero torna-se maior (vide figura 1: condição
no final do 10º mês). O umbigo cai e geralmente ressalta-se.
As figuras 2 e 3 mostram o perfil do abdome de uma mulher grávida, a posição do útero e a posição da
cabeça da criança ao final do 9º mês (figura 2) e durante o 10º mês (figura 3). A posição mais alta do útero
corresponde respectivamente ao pico das marcas apresentadas na figura 1. Ao final do 9º mês (figura 2), o
útero está elevado e toca o arco costal. A cabeça do feto está livremente posicionada por entre a abertura
pélvica superior.
Durante o 10º mês de gravidez (figura 3), o fundo descende, o abdome „escorrega“ para baixo, o útero fica
maior (vide figura 1; 10º mês). A seção mais baixa do útero é estreitada devido a integração do segmento
uterino inferior e da cabeça da criança já haver entrado na pelve.
Apresentações (figs. 4 a 13)
As figuras são ilustrações de algumas apresentações e posições essenciais. As seguintes distinções são feitas:
Apresentações: Proporção da criança ao eixo longitudinal materno
Posições: Direção das costas da criança em proporção aos lados da mãe (esquerdo, direito, frontal, etc.)
Posturas: Ângulo de inclinação da cabeça da criança em proporção ao eixo longitudinal de seu corpo
(flexão, extensão).
Ocupações: Parte anterior da criança durante o surgimento através do canal parturiente (sincipúcio,
occiput, testa, pés, nádegas, etc)
15
Page 16

®
Apresentações da criança antes
do parto
A apresentação e a posição são determinadas como segue:
Português
1ª (primeira) apresentação: as costas (em apresentações longitudinais) ou a cabeça (em apresentações
2ª (segunda) apresentação: oposta à 1ª apresentação
Além da exata direção das costas da criança para a esquerda ou direita, existem posições intermediárias
nas quais as costas, em apresentações longitudinais, podem apontar mais para a frente (dorso-anterior),
para as costas (dorso-posterior) ou em apresentações transversas para a frente (dorso-anterior), para as
costas (dorso-posterior), para cima (dorso-superior) ou para baixo (dorso-inferior). Os seguintes dados dão
uma idéia da freqüência aproximada das apresentações individuais:
100 partos
Apresentações Apresentações Apresentações
longitudinais cefálicas cefálicas normais
(99%) (96%) (94%)
Apresentações Apresentações Apresentações
transversas de nádegas cefálicas irregulares
(1%) (3%) (2%)
Apresentações occipito-anteriores (figs. 4 e 5)
Entre 100 partos, existem aproximadamente 94 apresentações cefálicas normais.
Fig. 4: 1ª apresentação occipito-anterior (posição mais freqüente )
Fig. 5: 2ª apresentação occipito-anterior
A apresentação occipito-anterior é a apresentação mais favorável possível, pois ela requer o mínimo de
risco para a mãe e a criança em comparação com as outras apresentações.
transversas) da criança para o lado esquerdo da mãe
Apresentações occipito-posteriores (figs. 6 e 7)
Apresentações cefálicas irregulares (apresentações occipito-posteriores, apresentações em vertex, apresentações de rosto e ombro) ocorrem em aproximadamente 2% dos partos.
Fig. 6: 1ª apresentação occipito-posterior: ( posição mais freqüente )
Fig. 7: 2ª apresentação occipito-posterior
A diferença entre as apresentações occipito-anterior e occipito posterior está na posição das costas da
criança, mais voltada para trás (posição dorso-posterior). O occiput (bem como as costas) podem ainda
virar-se para frente durante o parto de forma que este ainda possa se transformar em um caso de apresentação occipito-anterior.
As apresentações cefálicas irregulares mais excepcionais (apresentações em vertex, ombro e rosto) aumentam o risco para a mãe e a criança ou podem mesmo tornar impossível o parto normal.
16
Page 17

®
Português
Apresentações da criança antes
do parto
Apresentações de nádegas (figs. 8, 9 e 10)
A apresentação em questão (de nádegas) acontece quando a cabeça do feto não se encontra na posição
anterior. Este é o caso em aproximadamente 3% de todos os partos. As apresentações de nádegas recebem
tratamentos diferentes de acordo com cada caso. Nádegas, ambos os pés, a nádega e ambos os pés ou as
nádegas e um pé. Todas essas apresentações podem acontecer de forma anterior:
As figuras 8, 9 e 10 mostram primeiramente as apresentações de nádegas (da esquerda para a direita):
Fig. 8: apresentação de nádegas perfeita
Fig. 9: apresentação dupla trivial
Fig. 10: apresentação trivial completa
Apresentações de nádegas aumentam o risco do parto para a mãe e para a criança, tanto que sob certas
circunstâncias uma operação cesariana deve ser efetuada. Como a parte anterior da criança sempre tem
uma circunferência menor do que a cabeça, nos casos de apresentações de nádegas, a dilatação do osso
cervical do útero que se dá no começo do trabalho de parto, é inadequada e atrasada. Isso irá resultar em
uma extensão considerável da duração do trabalho de parto com um aumento de risco para a mãe e a
criança.
Apresentações transversas (fig. 11)
Apresentações transversas que representam aproximadamente 1% de todos os partos, acontecem quando o
eixo longitudinal da criança corta o eixo longitudinal do quadrilátero da mãe ou em um de seus ângulos.
Entre as possíveis posições de apresentações transversas, a mais freqüente é a dorso-anterior (cabeça para
esquerda, costas apontando para trás) como mostra a figura 11. Apresentações transversas não resultam
em partos normais, os quais quando feitos sem acompanhamento, podem levar à morte a mãe e a criança.
A origem da apresentação transversa é na maioria das vezes causada por distúrbios na apresentação normal da cabeça (gêmeos, pelve deformada, malformação do útero, placenta localizada à frente do osso
cervical, etc.).
Gêmeos (figs. 12 e 13)
Um parto de gêmeos ocorre à cada 80-90 partos. As imagens apresentadas não indicam se os gêmeos em
questão são monozigóticos ou dizigóticos.
No caso de parto geminado, as crianças podem se apresentar na mesma posição ou em posições diferentes.
A apresentação de ambas as crianças é, em sua maioria, cefálica (fig. 12; 45% dos partos de gêmeos) ou
de uma criança em apresentação cefálica e a outra em apresentação pélvica (fig. 13; 35% dos partos do
gêmeos). De acordo com a freqüência, as outras apresentações são: ambas as crianças em apresentação de
nádegas, apresentação cefálica combinada com apresentação transversa, apresentação de nádegas combinada com apresentação transversa, ambas as crianças em apresentação transversa.
O parto é na maioria das vezes espontâneo, no curso do qual, a segunda criança aparece aproximadamente
30 minutos após o nascimento da primeira.
17
Page 18

®
Presentazioni del bambino prima
Italiano
della nascita
La durata dello sviluppo del bambino è di circa 270 giorni, tenendo conto delle differenze individuali.
Poiché il momento della fecondazione della cellula uovo nella maggior parte dei casi è sconosciuto, si inizia il conteggio a partire dal primo giorno dell’ultima mestruazione. La durata della gravidanza è di circa
280 giorni, cioè 10 mesi (lunari) di 28 giorni ciascuno (40 settimane). Nel corso della gravidanza, l’embrione
si gira ripetutamente e cambia più volte posizione all’interno della membrana fetale. Nelle ultime 3-4 settimane di gravidanza una determinata parte del bambino (nella maggior parte dei casi la testa) si mette in
rapporto più stretto con il canale di passaggio del bacino materno e conserva questa posizione. Da questo
momento si può parlare di “presentazione del feto”.
Ingrandimento dell’utero nei singoli mesi della gravidanza (Figg. da 1 a 3)
La fig. 1 riproduce l’ingrandimento dell’utero dalla quarta alla decima settimana di gravidanza, appurabile
mediante una visita esterna. Le cifre indicate corrispondono alla fine di ciascun mese. Fino all’inizio del
quarto mese, l’utero non è palpabile esternamente (attraverso la parete addominale). Dalla metà del quarto mese, la parte superiore dell’utero (fondo dell’utero) fuoriesce dal “piccolo bacino” salendo attraverso la
sinfisi pubica, e alla fine del nono mese raggiunge entrambi gli archi costali, per abbassarsi nuovamente al
decimo mese.
Alla fine di ciascun mese di gravidanza, il fondo dell’utero si trova alla seguente altezza:
4° mese: immediatamente al di sotto della sinfisi
5° mese: al di sotto dell’ombelico
6° mese: esattamente all’altezza dell’ombelico
7° mese: al di sopra dell’ombelico
8° mese: a metà tra l’ombelico e l’estremità inferiore dello sterno
9° mese: il fondo dell’utero raggiunge l’arco costale (posizione più elevata)
10° mese: il fondo dell’utero si abbassa alla posizione dell’ottavo mese
L’abbassamento del fondo dell’utero, che nelle donne alla prima gravidanza avviene 4 settimane prima del
parto, mentre nelle altre donne si verifica 3 settimane prima del parto, determina un cambiamento della
forma della pancia delle gestanti: la pancia si abbassa e si curva fortemente in avanti (fig. 3 rispetto alla
fig. 2), l’utero si allarga (v. fig. 1: posizione alla fine del decimo mese). L’ombelico si distende e spesso si
inarca in avanti.
Le figure 2 e 3 ritraggono il profilo della pancia di una gestante, la posizione dell’utero e l’altezza della
testa del bambino alla fine del nono mese (fig. 2) e nel corso del decimo mese (fig. 3). Il punto più elevato
dell’utero corrisponde al vertice delimitato dai contorni riportati nella figura 1. Alla fine del nono mese
(fig. 2), l’utero è rivolto verso l’alto e tocca l’arco costale. La testa si trova rilassata sopra l’entrata del bacino.
Nel corso del decimo mese di gravidanza (fig. 3), il fondo si abbassa, la pancia “scivola” più in profondità,
l’utero si allarga (v. fig. 1, decimo mese). In seguito all’integrazione del segmento inferiore dell’utero, la
parte inferiore dell’utero risulta accorciata e la testa del bambino entra nel bacino.
Presentazioni del feto (Figg. da 4 a 13)
Le figure illustrano alcune presentazioni e posizioni del feto. Si distinguono:
Presentazioni: rapporto tra l’asse longitudinale del bambino e quello dell’utero
Posizioni: direzione della schiena del bambino rispetto ai lati dell’utero (sinistra, destra avanti, ecc.)
Posture: inclinazione della testa del bambino rispetto all’asse longitudinale del proprio corpo (pie-
gamento, allungamento)
Atteggiamenti: parte del bambino che precede al passaggio nel canale del parto (occipitale anteriore, pos-
teriore, fronte, piedi, natiche, ecc.)
18
Page 19

®
Italiano
Presentazione e posizione vengono espresse come segue:
Presentazioni del bambino prima
della nascita
I (prima) presentazione: la schiena (nelle presentazioni longitudinali) o la testa (nelle presentazioni
II (seconda) presentazione: contrapposta alla I presentazione
Oltre alla direzione precisa della schiena del bambino verso sinistra o verso destra, ci sono posizioni intermedie, in cui la schiena nelle presentazioni longitudinali può essere rivolta più in avanti (dorso-anteriore),
all’indietro (dorso-posteriore) oppure nelle presentazioni trasversali in avanti (dorso-anteriore), all’indietro
(dorso-posteriore), verso l’alto (dorso-superiore) oppure verso il basso (dorso-inferiore). Le cifre che seguono
danno un’idea della frequenza approssimativa delle singole presentazioni fetali.
100 nascite
Posizioni Posizioni cefaliche Posizioni cefaliche regolari
longitudinali
(99%) (96%) (94%)
Posizioni trasversali Posizioni podaliche Posizioni cefaliche irregolari
(1%) (3%) (2%)
Presentazioni di vertice occipitale anteriore (Figg. 4 e 5)
Su 100 nascite, circa 94 sono in posizioni cefaliche regolari.
Fig. 4: I presentazione di vertice occipitale anteriore (posizione più frequente)
Fig. 5: II presentazione di vertice occipitale anteriore
La presentazione di vertice occipitale anteriore è la presentazione fetale migliore perchè in confronto ad
altre presentazioni fetali risulta meno pericolosa per la mamma e il bambino.
Presentazioni di vertice occipitale posteriore (Figg. 6 e 7)
Posizioni cefaliche irregolari (presentazioni di vertice occipitale posteriore, presentazioni di bregma, presentazioni di fronte o di faccia) compaiono in circa il 2% dei parti.
trasversali) del bambino è rivolta verso il lato sinistro dell’utero
Fig. 6: I presentazione di vertice occipitale posteriore (posizione più frequente)
Fig. 7: II presentazione di vertice occipitale posteriore
La differenza rispetto alla presentazione di vertice occipitale anteriore consiste nella posizione della schiena del bambino orientata più all’indietro (posizione dorso-posteriore). Durante il parto, il vertice occipitale
(e così anche la schiena) può ancora girarsi in avanti, cosicché il parto prosegue come nel caso della presentazione di vertice occipitale anteriore.
Le presentazioni cefaliche irregolari meno frequenti (presentazione di bregma, di fronte o di faccia)
aumentano i rischi per la mamma e il bambino oppure rendono il parto addirittura impossibile.
Posizioni podaliche (Figg. 8, 9 e 10)
Se in un asse longitudinale la parte che precede non è la testa, si tratta di una presentazione podalica. È il
caso del 3% dei parti. A seconda che le parti che precedono siano le natiche, entrambi i piedi, le natiche ed
entrambi i piedi, o le natiche ed un piede, le presentazioni cefaliche vengono definite diversamente.
19
Page 20

®
Presentazioni del bambino prima
Italiano
della nascita
Le figure 8, 9 e 10 rappresentano le I presentazioni cefaliche (schiena rivolta a sinistra).
Fig. 8: presentazione di natiche vera e propria
Fig. 9: presentazione di piedi completa
Fig. 10: presentazione di natiche e piede completa
Le presentazioni podaliche aumentano il rischio nel parto per la mamma e il bambino, cosicché in presenza di determinate condizioni si deve ricorrere al parto cesareo. Poiché nelle presentazioni podaliche la
parte del bambino che precede ha sempre una circonferenza minore rispetto alla testa, l’allargamento del
collo dell’utero che si attua con l’inizio dei dolori del parto è insufficiente e ritardato. Il risultato è un notevole prolungamento della durata del parto con rischi crescenti per la mamma e il bambino.
Posizioni trasversali (Fig. 11)
Le presentazioni trasversali, che rappresentano circa l’1% di tutti i parti, si verificano quando l’asse longitudinale del bambino taglia ad angolo retto oppure obliquo quello della mamma. Tra le possibili posizioni
delle presentazioni trasversali, nella fig. 11 è rappresentata la I presentazione trasversale dorso-anteriore
(testa avanti, schiena rivolta in avanti) che si verifica frequentemente. Le posizioni trasversali sono presentazioni del feto che rendono impossibile il parto e (se non trattate) possono portare alla morte della
mamma e del bambino.
La genesi di una presentazione trasversale è dovuta nella maggior parte dei casi a impedimenti del normale atteggiamento della testa quale parte che precede (gemelli, bacino deformato, deformazioni dell’utero,
placenta situata davanti al collo dell’utero ecc.)
Gemelli (Figg. 12 e 13)
Su 80-90 nascite si verifica un parto gemellare. Le figure rappresentate non specificano se si tratta di
gemelli omozigoti o eterozigoti.
La presentazione dei bambini uno rispetto all’altro è uguale o diversa. Nella maggior parte dei casi, entrambi si trovano in presentazione cefalica (Fig. 12; 45% dei parti gemellari) oppure un bambino si trova
in presentazione cefalica e l’altro in presentazione podalica (fig. 13; 35% dei parti gemellari). In ordine di
frequenza seguono: entrambi i bambini in presentazione podalica, presentazione cefalica combinata con
presentazione trasversale, presentazione podalica combinata con presentazione trasversale, entrambi i
bambini in presentazione trasversale.
Nella maggior parte dei casi si verifica un parto spontaneo, in cui la nascita del gemello avviene 30 minuti
dopo quella del primo bambino.
20
Page 21

4 13
1
100
件
4 5
6 7
21
Page 22

11
8 9
22
12 13
Page 23

®
Русский Положение плода перед родами
Период развития плода с учетом индивидуальных расхождений составляет приблизительно 270 дней.
Поскольку момент оплодотворения яйцеклетки зачастую точно не известен, то за отправную точку
для расчетов принимается первый день последней менструации. Таким образом, продолжительность
беременности составляет примерно 280 дней, то есть 10 (лунных) месяцев по 28 дней (40 недель). Во
время беременности зародыш неоднократно поворачивается и принимает различные положения внутри
оболочек плодного пузыря. В последние 3-4 недели беременности определенная часть тела ребенка
(чаще всего головка) наиболее близко располагается к родовому каналу таза матери и фиксируется в
данном положении. Лишь тогда можно говорить о таком понятии, как «предлежание».
Увеличение матки во время беременности по месяцам (рисунки 1-3)
На рисунке 1 представлено увеличение матки с 4-го по 10-й месяцы беременности, которое можно
определить при наружном обследовании. Цифры обозначают конец соответствующего месяца. До
начала 4-го месяца снаружи (через брюшную стенку) матка не прощупывается. Начиная с середины
4-го месяца верхняя часть матки (дно матки) выходит за пределы малого таза - за лобковое сочленение
(симфиз) - и в конце 9-го месяца достигает реберных дуг, а на 10-м месяце беременности снова
опускается.
В конце каждого месяца беременности дно матки находится на следующем уровне:
4-й месяц: прямо под симфизом
5-й месяц: ниже уровня пупка
6-й месяц: точно на уровне пупка
7-й месяц: выше уровня пупка
8-й месяц: на середине расстояния между пупком и мечевидным отростком грудины
9-й месяц: матка достигает уровня реберной дуги (наивысший уровень)
10-й месяц: матка опускается до уровня 8-го месяца
Опускание матки, которое происходит у первородящих женщин за 4 недели, а у повторнородящих
за 3 недели до родов, вызывает изменение формы живота беременных: живот опускается и сильнее
выпячивается (сравните рис. 3 и рис. 2), матка становится шире (см. рис. 1: положение в конце 10-го
месяца). Пупок сглаживается, часто он выпячивается.
Рисунки 2 и 3 демонстрируют профиль живота беременной, положение матки и уровень расположения
головки плода в конце 9-го месяца (рис. 2) и в течение 10-го месяца (рис. 3). Наивысшая точка матки
соответствует в каждом случае вершине нанесенных на рис. 1 контуров. В конце 9-го месяца (рис. 2)
матка высоко поднята, она соприкасается с реберной дугой. Головка располагается свободно над
входом в таз.
В течение 10-го месяца беременности (рис. 3) матка опускается, живот как бы «сползает» вниз, матка
становится шире (см. рис. 1, 10-й месяц). Нижняя часть матки укорачивается вследствие сглаживания
нижнего маточного сегмента, и головка плода входит в полость таза.
Предлежания плода (рис 4-13)
Иллюстрации разъясняют некоторые основные положения и предлежания плода. Различают:
Положение плода: отношение продольной оси плода к продольной оси матки
Позиция и вид: отношение спинки плода к стороне матки (левой, правой, передней и т. д.)
Членорасположение плода: отношение головки плода к продольной оси тела плода (сгибательное,
разгибательное)
Предлежание плода: идущая вперед по родовому каналу часть плода (затылочное, переднеголовное,
лобное, ножное, ягодичное и др.)
Положение и вид определяются следующим образом:
I (первая) позиция: спинка (при продольном положении) или головка (при поперечном положении) плода
направлена к левой стороне матки.
23
Page 24

®
РусскийПоложение плода перед родами
II (вторая) позиция: противоположная первой позиции.
Помимо точного направления спинки плода влево или вправо бывают промежуточные положения,
при которых спинка может быть больше обращена вперед (передний вид) или назад (задний вид)
при продольном положении, а при поперечном положении – вперед (передний вид), назад (задний
вид), вверх (верхний вид) или вниз (нижний вид). Следующие данные представляют информацию о
приблизительной частоте некоторых положений плода.
100 родов
Продольное Головное Правильное головное
положение предлежание предлежание
99% 96% 94%
Поперечное Тазовое Неправильное головное
положение предлежание предлежание
1% 3% 2%
Передний вид затылочного предлежания (рисунки 4 и 5)
На 100 родов приходится примерно 94 нормальных правильных головных предлежаний.
Рис. 4: Затылочное предлежание, I позиция, передний вид: наиболее частое положение
Рис. 5: Затылочное предлежание, II позиция, передний вид
Передний вид затылочного предлежания наиболее благоприятен из всех возможных положений плода,
потому что по сравнению с другими положениями плода он влечет за собой наименьшую опасность для
матери и плода.
Задний вид затылочного предлежания (рисунки 6 и 7)
Неправильные головные предлежания (задний вид затылочного предлежания, переднеголовное, лобное и
лицевое предлежания) встречаются примерно в 2% родов.
Рис. 6: Затылочное предлежание, I позиция, задний вид: наиболее частое положение
Рис. 7: Затылочное предлежание, II позиция, задний вид
Отличие от переднего вида затылочного предлежания состоит в том, что спинка плода более обращена
назад (задний вид). Во время родов затылок (а вместе с ним и спинка) еще может повернуться вперед,
таким образом, дальнейшее течение родов будет соответствовать их течению при переднем виде
затылочного предлежания.
Более редкие аномальные положения головки (переднеголовное, лобное, лицевое) увеличивают риск для
матери и плода, или даже делают невозможными самопроизвольные роды.
Тазовое предлежание плода (рисунки 8, 9 и 10)
Если при продольном положении головка не является впереди идущей частью, говорят о тазовом
предлежании плода. Такое предлежание встречается в 3% всех родов. В зависимости от того, что является
предлежащей частью - ягодицы, обе ножки, ягодицы и обе ножки или ягодицы и одна ножка, выделяют
разные подвиды тазовых предлежаний.
На рисунках 8, 9 и 10 изображена I позиция тазового предлежания (спинка плода обращена налево):
Рис. 8: чисто ягодичное предлежание
Рис. 9: полное ножное предлежание
Рис.10: смешанное (полное) ягодично-ножное предлежание
24
Page 25

®
Русский Положение плода перед родами
Тазовое предлежание повышает риск осложнений при родах для матери и плода, таким образом,
при наличии определенных предпосылок необходимо кесарево сечение. Поскольку идущая вперед
часть плода при тазовом предлежании всегда имеет меньший размер по сравнению с головкой, то
начинающееся с началом схваток раскрытие шейки матки является недостаточным и замедленным.
Результатом является значительное увеличение продолжительности родов с возрастающим риском для
матери и ребенка.
Поперечное положение (рис. 11)
Поперечные положения, которые составляют 1% от всех родов, имеют место тогда, когда продольная
ось плода располагается под прямым углом или по диагонали по отношению к оси матери. Среди
возможных видов поперечных положений на рисунке 11 изображено часто встречающееся поперечное
положение, I позиция, передний вид (головка слева, спинка направлена вперед). Поперечные положения
являются такими положениями, при которых самопроизвольные роды невозможны и (при отсутствии
вмешательства) могут вызвать гибель матери и плода. В основе возникновения поперечных положений
чаще всего лежат препятствия для нормального установления головки как ведущей части (близнецы,
деформации таза, деформации матки, предлежание плаценты и прочие факторы).
Близнецы (рисунки 12 и 13).
На 80-90 родов приходится один случай рождения близнецов. На представленных рисунках не
уточняется, какие близнецы изображены - однояйцевые или разнояйцевые.
Положение обоих плодов по отношению друг к другу может быть одинаковым или различным. Зачастую
оба находятся в головном предлежании (рис. 12; 45% случаев рождения близнецов), или один ребенок
находится в головном предлежании, а другой - в тазовом (рис. 13, 35% случаев рождения близнецов).
Остальные виды предлежания близнецов распределяются в следующем порядке (по убыванию частоты):
оба ребенка в тазовом предлежании; головное предлежание в сочетании с поперечным положением;
тазовое предлежание в сочетании с поперечным положением; оба ребенка в поперечном положении.
Роды чаще всего происходят естественным путем, при этом второй ребенок появляется на свет примерно
через 30 минут после первого.
25
Page 26

®
分娩前胎先露 英文
幼儿发育期包括个体差异大约为270天。由于通常不知道卵母细胞的授精日期,末次月经的第一天
将作为推算的依据。因此,妊娠时间大约为280天,也就是农历28天为一月,共10月(40周)。妊娠
期间胎儿在胎膜腔里反复转动、改变姿势。胎儿的某一部分(通常是头)在怀孕的最后3-4周和母体
骨盆的产道获得密切关系并且维持胎位。该术语 “胎先露”迄今都是正确的。
妊娠期子宫每月增大(图1-3)
图1显示妊娠4-10月外测子宫的增大。每个月底记录对应的数值。子宫直到第4个月初才能在外面(
通过腹壁)触及。从第4个月中期开始,子宫上端部分(宫底)从“小骨盆”上升超过耻骨联合,
至第9个月底到达双侧肋弓,然后在第10个月再次下降。
妊娠的每个月底,子宫底处于以下各个位置:
第4个月:紧靠耻骨联合下面
第5个月:脐下
第6个月:脐平
第7个月:脐上
第8个月:脐与剑突之间
第9个月:子宫底到达肋弓(最高位)
第10个月:子宫底下降至第8个月的位置
初产妇的子宫下降发生在临产前4周,非初产妇的在临产前3周。孕妇腹部的外形改变:腹部下沉和
更明显突出(图3和图2相比),子宫变宽(参照图1,第10个月底的情况),脐滑落并突出。
图2和图3显示孕妇腹部侧面,子宫和胎头在第9个月底的位置(图2)以及在第10个月期间的位置(
图3)。图1显示了不同妊娠月底的子宫底最高位置。在第9个月底(图2):子宫垂直达肋弓。胎头
松散地位于骨盆上面。
在妊娠的第10个月期间(图3),宫底下降,腹部“滑”低,子宫变宽,(参照图1,第10个月)。
由于子宫下段形成和胎头入盆的因素,子宫下面部分变短。
先露(图4-13)
图表说明了一些基本的胎先露和胎方位。下面是一些特性:
胎先露:胎儿与子宫纵轴的关系。
胎方位:胎儿背部方向与子宫册侧面的关系(左,右,前等)
姿势:胎头歪曲的角度和胎儿身体纵轴的关系(歪曲,延伸)
衔接:通过产道的胎儿先露部位(前顶,后枕,前额,脚,臀部等)
胎先露和胎方位由下面因素决定:
第一胎位:胎儿背部(纵产式)或头(横产式)指向子宫左侧。
第二胎位:和第一胎位相反。
除了胎儿背部会指向子宫左侧或右侧的准确方向,还可以是中间的胎方位,其中背部纵胎位可指向
更前(背前位),指向更后(背后位),指向更上(背上位),指向更下(背下位)。下面的图将
显示出各个胎位的发生频率:
枕前先露(图4和图5)
在100次分娩中,大约有94个正常头先露。
图4:第一枕前位:最常见胎方位
图5:第二枕前位。。
枕前位是最有利的胎位,和其他胎位相比,承担的危险性最小。
枕后先露(图6和图7)
不规则的头先露(枕后先露,顶先露,额先露,面先露)在分娩中出现的纪律约为2%。
图6:第一枕后位:最常见的胎方位
图7:第二枕后位。
与枕前位不同的是胎儿背部更向后转(后背卧位)。枕(和背)在分娩中还能转向前,因此分娩的
进一步过程相当于枕前位。其他的不规则枕先露(顶先露,额先露,面先露)会增加母婴危险性甚
至不适合分娩。
臀先露(图8,9,10)
26
Page 27

®
英文 分娩前胎先露
臀先露是假设头纵先露不在前面,是有问题的胎位。这类情形在所有分娩中约占3%。臀先露根据
臀,双足,臀和双足或者臀和单足是否先露给予特别名称的。
图8,9,10显示第一臀先露(背向左)
图8:良好的臀先露
图9:双足先露
图10:完整足先露
臀先露会增加母婴在分娩时的危险性,因此在确定情况下需做剖腹产。因为胎儿先露部分总是比臀
先露情况下的胎头周径小,分娩初期宫颈扩张不够,分娩会延迟。这会导致分娩时间延长,母婴危
险性增加。
横产式(图11)
横产式是胎儿身体纵轴和母体纵轴垂直或成角,在分娩中的出现约为1%。在可能发生的横产式中
最多的是枕前横产式(头向左,背向前),如图11所示。横产式不适于分娩,(在每人照看的情况
下)将会导致母婴死亡。
横产式大多数是由于正常头先露受干扰(双胞胎,不正常的骨盆,子宫畸形,胎盘前置于宫颈等)
Twins (fig. 12 and 13)
双胞胎(图12和13)
80至90次分娩中有一次双胞胎。显示的迹象并不表示双胞胎来自单卵双生或双卵双生。
双胞胎的先露可以是相同或不同。两个胎儿的先露大都是枕先露(图12:45%的双胞胎分娩)或一
个胎儿是头先露另一个是骨盆先露(图13:35%的双胞胎分娩)。根据发生频率,依次常见的先露
是:两个胎儿臀先露、头先露兼横位、臀先露兼横位、两个胎儿横位。
双胞胎的分娩大都是同时的,在第一个胎儿分娩后30分钟左右分娩第二个胎儿。
27
Page 28

V2068_1001226_4006562-08/12-3
®
3B S C I E NT I F I C
3B Scientific GmbH
Rudorffweg 8 • 21031 Hamburg • Germany
Tel.: + 49-40-73966-0 • Fax: + 49-40-73966-100
www.3bscientific.com • 3b@3bscientific.com
© Copyright 1999 / 2012 for instruction manual and design of product:
3B Scientific GmbH, Germany
P R O D U C T S
5002075
 Loading...
Loading...