

Page 1

s
SC 6002XL Patient Monitor
Field Service Manual
Field Service Manual
Field Service ManualField Service Manual
E331.E551U.719.01.01.02
Replaces/Ersetzt:
ASK-T941-04-7600
EM Guidelines, 1997-04-02
Product Drawing
Page 2

ADVISORY
Siemens is liable for the safety of its equipment only if maintenance, repair, and modifications are performed by
authorized personnel, and if components affecting the equipment's safety are replaced with Siemens spare parts.
Any modification or repair not done by Siemens personnel must be documented. Such documentation must:
• be signed and dated
• contain the name of the company performing the work
• describe the changes made
• describe any equipment performance changes.
It is the responsibility of the user to contact Siemens to determine warranty status and/or liabilities if other than
an authorized Siemens Service Representative repairs or makes modifications to medical devices.
Page 3

Field Service Manual SC 6002XL Patient Monitor
Table of Contents
Chapter 1: Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.1 Service Strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.2 Replaceable Parts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.3 Technical Manual Conventions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2 Product Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.1 Monitored Patient Parameters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.2 SC 6002XL Monitor Controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.3 TFT-LCD Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.4 Alarms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2.5 Monitor/Software Tracking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
3 Preventative Maintenance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
3.1 General . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
3.2 Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
4 Technical Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
4.1 General . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Table 1-1 General Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
4.2 Environmental . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Table 1-2 Environmental Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
4.3 Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Table 1-3 Display Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
4.4 Outputs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Table 1-4 Output Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
4.5 Connectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Table 1-5 Connector Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
5 Monitor Controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
5.1 Main Screen Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
5.2 Menu Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
5.3 Alarm Limits Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
5.4 Alarm Silence Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
5.5 All Alarms Off Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
5.6 NBP Start/Stop Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
5.7 Zoom Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
5.8 Record Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers i
6k2XLSMftcvr.cd-rom.fm/06-00/kaupp
Page 4

Field Service Manual SC 6002XL Patient Monitor
Chapter 2: Functional Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
1 Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Figure 2-1 SC6002XL Patient Monitor Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2 Parameter Inputs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
3 Main PC Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
3.1 LCD Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.2 Network Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.3 Front Panel Circuitry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.4 Pod Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.5 Battery Control and ON/OFF Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.6 BOOT Process, Flash Memory, and DRAM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.7 SRAM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3.8 68HC11 Microcontroller . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
4 Front End . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
4.1 NIBP Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
4.2 Safety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Figure 2-2 Front End . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
5 Physiological Parameter Data Acquisition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
5.1 ECG/Resp . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Table 2-1 Parameter Sampling Table . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
5.1.1 ECG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 2-3 Lead-Forming Network . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
5.1.2 Lead Selection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
5.1.3 Lead-Off Detection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
5.1.4 Low-Pass Filtering and Common Mode Enhancement . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
5.2 Respiration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Figure 2-4 SpO2 Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
5.3 SpO
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
2
5.3.1 SpO
Front End . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
2
Figure 2-5 Sensor LED Timing Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
5.3.2 Input Stage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
5.3.3 Brightness Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
5.3.4 Ambient Light Rejection Amplifier . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Figure 2-6 IBP Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
5.4 Invasive Blood Pressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
5.5 Non-Invasive Blood Pressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
5.5.1 NBP Subsystem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Figure 2-7 NBP Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers ii
6k2XLSMftcvr.cd-rom.fm/06-00/kaupp
Page 5

Field Service Manual SC 6002XL Patient Monitor
5.5.2 NBP System Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
5.5.3 Operation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
5.5.4 NBP Hardware . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
5.5.5 Valve Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
5.5.6 Power Supplies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
5.5.7 Power Supply Monitor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
5.5.8 Safety Timer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
5.5.9 Pressure Channels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Figure 2-8 Temperature Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
5.6 Temperature Circuit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
5.6.1 Reference Networks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
5.6.2 A/D Converter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Figure 2-9 etCO2 Sensing Process Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
6 etCO2 Pod . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Figure 2-10 Power System Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
6.1 Power Supply System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
6.1.1 Main Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
6.1.2 AC Power Adapter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Chapter 3: Subassembly Replacement Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
2 Safety Precautions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
3 Service Policy and Replaceable Parts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
4 Non-Invasive Replacement Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
4.1 Replacing Rotary Knob . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
4.2 Replacing Foot Pads . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
5 Accessing Replaceable Subassemblies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Figure 3-1 Right Side Panel Removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
5.1 Removing Side Panels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
5.1.1 Removing Right-Hand Side Panel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Figure 3-2 Removing Left Side Panel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
5.1.2 Removing Left Side Panel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27
5.1.3 Reinstalling Side Panels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Figure 3-3 Bezel Retaining Screws . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
5.2 Front Bezel Removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Figure 3-4 Front Bezel Removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
5.3 Replacing Optical Encoder Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Figure 3-5 Optical Encoder Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers iii
6k2XLSMftcvr.cd-rom.fm/06-00/kaupp
Page 6

Field Service Manual SC 6002XL Patient Monitor
5.4 Front Bezel Installation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Figure 3-6 TFT-LCD Display Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
5.5 Removing/Installing TFT-LCD Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30
5.5.1 Removing TFT-LCD Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
5.5.2 Installing TFT-LCD Display Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Figure 3-7 Speaker Subasssembly Connector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
5.6 Speaker Replacement. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Figure 3-8 TFT-LCD Display Subassembly (Back View). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
5.7 Front Panel PC Board Replacement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
5.8 Inverter Board Replacement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Figure 3-9 Backlight Retaining Tabs Location . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
5.9 TFT-LCD Display Backlight Replacement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
5.10PodPort PC Board Removal/Installation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
5.10.1 Removing PodPort PC Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Figure 3-10 Removing PodPort PC Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
5.10.2 Installing PodPort PC Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Figure 3-11 Removing Intermediate Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
5.11Replacing Intermediate Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
5.11.1 Removing Intermediate Subssembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
5.11.2 Installing Intermediate Subssembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
5.12Replacing Main Processor Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
5.12.1 Removing Main Processor Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Figure 3-12 Securing Screw Access Cover . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Figure 3-13 Accessing Main Processor Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Figure 3-14 Connector Locations on Main Processor Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . 37
5.12.2 Installing Main Processor Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
5.13Monitor Handle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
5.13.1 Removing Handle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Figure 3-15 Removing Handle retaining Plate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
5.13.2 Installing Handle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Figure 3-16 Location of NBP Subassembly in Rear Housing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
5.14Replacing NBP Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
5.14.1 Removing NBP Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
5.14.2 Installing NBP Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40
5.15Replacing NBP Air Filters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Figure 3-17 NBP Air Intake Filter Access . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
5.15.1 Replacing Air Intake Filter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Figure 3-18 NBP Manifold Filter Replacement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers iv
6k2XLSMftcvr.cd-rom.fm/06-00/kaupp
Page 7

Field Service Manual SC 6002XL Patient Monitor
5.15.2 Replacing Manifold Filter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
5.16Replacing Battery Connector Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Figure 3-19 Battery Connector Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Figure 3-20 Battery Connector Subassembly Access Inside Rear Housing . . . . . . . . . . . . . . . . . . . . 43
5.17Correcting Hardware Revision Number Stored in Monitor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
5.17.1 Windows 3.1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
5.17.2 Windows 95 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
5.17.3 Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Figure 3-21 Support Menu (Item numbers may differ in different versions of installed software.) . . 45
Chapter 4: Functional Verification and Calibration . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
1 Functional Verification Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
1.1 Power Circuits and Startup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
1.2 Optical Encoder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
1.3 TFT-LCD Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
1.4 Fixed Keys . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
1.5 ECG/RESP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
1.6 Asystole . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
1.7 SpO2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
1.8 Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
1.8.1 Functional Verification Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
1.8.2 Temperature Calibration Check . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Table 4-1 Resistance Value vs. Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
1.9 etCO2 (if installed) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Figure 4-1 Test Setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
1.10Non-Invasive Blood Pressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
1.10.1 System Setup and Pneumatics Leakage Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
1.10.2 Functional and Calibration Check . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .53
Figure 4-2 IBP Test Setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
1.11Invasive Blood Pressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
2 Leakage Current Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
Table 4-2 Leakage Current Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
Figure 4-3 Block Diagram: Earth Leakage Current (AC/DC Power Adapter) . . . . . . . . . . . . . . . . . . . 56
Figure 4-4 Block Diagram: Earth Leakage Current (CPS/Docking Station) . . . . . . . . . . . . . . . . . . . . 56
Figure 4-5 Block Diagram: Earth Leakage Current (Infinity Docking Station) . . . . . . . . . . . . . . . . . . 56
3 Calibrating NBP System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Table 4-3 NBP Calibration Test Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers v
6k2XLSMftcvr.cd-rom.fm/06-00/kaupp
Page 8

Field Service Manual SC 6002XL Patient Monitor
3.2 Calibration Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
Figure 4-6 Calibration Potentiometer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3.3 Characterization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
Figure 4-7 NBP Characterization Setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .59
3.3.1 Characterization Setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
3.3.2 Windows 3.1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
3.3.3 Windows 95 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
3.3.4 Complete Characterization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .60
Figure 4-8 Support Menu (Item numbers may differ between versions of installed software.) . . . . 61
Chapter 5: Troubleshooting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
1 Troubleshooting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
1.1 Power Problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
1.1.1 No Response When POWER ON/OFF Key Pressed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
Table 5-1 Power-On Problems 63
1.1.2 Power On/Off Piezo Tone Fails to Sound. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Table 5-2 Power-off Alarm Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
1.1.3 Power-Up Sequence Fails to Complete Properly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Table 5-3 Power-up Process Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
1.2 Optical Encoder Malfunction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Table 5-4 Rotary Knob Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
1.3 TFT-LCD Display Malfunction.Fixed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Table 5-5 LCD Display Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
1.4 Fixed Key Fails to Function. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Table 5-6 Fixed Key Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
1.5 Visual or Audible Alarm Reporting Failure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
Table 5-7 Alarm Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
1.6 NBP Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
Table 5-8 NBP Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
1.7 etCO2 Malfunction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
Table 5-9 etCO2 Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
1.8 No Printout from Recorder. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
Table 5-10Recorder Problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
1.9 Isolating Cable Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
1.10Patient-Related Data Not Retained or Monitor Fails to Compute Trends . . . . . . . . . . . . . . . . . . . . . 69
Appendix A: Replaceable Parts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
Table A-1 SC 6000XL - Replaceable Parts and Subassemblies . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
Figure A-1 SC 6002XL Exploded View 73
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers vi
6k2XLSMftcvr.cd-rom.fm/06-00/kaupp
Page 9

Field Service Manual SC 6002XL Patient Monitor
Figure A-2 NBP Subassembly (shown with filters exposed) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
Appendix B: Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Figure B-1 IBP Connector (see Table B-1) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .75
Figure B-2 MultiMed Pod Connector (see Table B-2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Table B-1 IBP Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Table B-2 MultiMed Pod Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Figure B-3 Docking Station Connector (see Table B-3) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
Figure B-4 SHP ACC CBL ALARM UNTERM 5M (see Table B-4) . . . . . . . . . . . . . . . . . . . . . . . . . . 76
Table B-3 Docking Station Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
Table B-4 Remote Alarm Cable Color Code . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
Figure B-5 Interface Plate Connector (see Table B-5) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
Figure B-6 SHP ACC CBL Y RECORDER/ALARM (see Table B-6) . . . . . . . . . . . . . . . . . . . . . . . . . . 77
Table B-5 Interface Plate Connectors Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
Table B-6 Remote Alarm Cable Color Code . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
Figure B-7 Basic/Device CPS Connectors - Infinity Network (see Table B-7) . . . . . . . . . . . . . . . . . . 78
Table B-7 InfinityNet CPS Connector Pins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78
Figure B-8 Infinity Docking Station Connectors(Refer to Table B-8.) . . . . . . . . . . . . . . . . . . . . . . . . 79
Table B-8 Infinity Docking Station Connectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
Figure B-9 PodPort Connector (see Table B-9) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
Table B-9 PodPort Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .80
Appendix C: Error and Diagnostic Codes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
1.1 Startup Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
1.2 Diagnostic Log . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
Table C-1 Support Menu . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
1.3 Severity Codes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
1.4 Reset Causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
2 Diagnostic Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Table C-2 Startup Diagnostic Log Codes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Table C-3 Exception Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Table C-4 Hardware-related Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
Table C-5 Intertask Mail Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
Table C-6 Miscellaneous Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .85
Table C-7 Alternative Memory Manager to PSOS OSL Messages . . . . . . . . . . . . . . . . . . . . . . . . . 86
Table C-8 NP Subsystem Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
Table C-9 Diagnostic Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
Table C-10INTER Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
Table C-11Print Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers vii
6k2XLSMftcvr.cd-rom.fm/06-00/kaupp
Page 10

Field Service Manual SC 6002XL Patient Monitor
Table C-12MAIN Processor Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
Table C-13ACT Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
Table C-14Audio Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
Table C-15Database Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
Table C-16Front End Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
Table C-17Alarm Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Table C-18Monitoring Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Table C-19SpO2 Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Table C-20HCOM Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
Table C-21LCOM Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101
Table C-22NET Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Table C-23etCO2 Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Appendix D: Functional Verification Checklist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
Appendix E: Supplemental Documents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
Software Installation Instructions - Software Version VE0 . . . . . . . . . . . . . 109
Service Setup Instructions - Software Version VE0 . . . . . . . . . . . . . . . . . . . 110
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers viii
6k2XLSMftcvr.cd-rom.fm/06-00/kaupp
Page 11

Chapter 1: Introduction
1Introduction
1.1 Service Strategy
1.2 Replaceable Parts
In keeping with the service strategy for the SC6002XL, this service manual
provides the necessary information required to service an SC 6002XL patient
monitor in the field. The SC 6002XL is both a stationary and a portable
monitor designed to monitor patient vital signs (refer to user’s guide for
monitoring options). For stationary operation near a bedside, the monitor is
connected to an AC/DC power adapter or placed on a specially designed
docking station attached to a shelf, wall, or rolling stand that securely locks
it into place. While on the docking station, the monitor is powered by a CPS
or an IDS power supply. When the monitor is detached from a CPS or IDS, it
is powered by a lead acid battery or by an optional Lithium ion battery. The
monitor is reattached to the AC/DC Power Adapter or placed back on a
CPS or IDS to recharge the battery.
The monitor has been designed for high reliability, with an estimated
MTBF of 50,000 hours (5.7 yrs.) of continuous operation.
Therefore, the service strategy is based on few failures in the field, a clear
definition of failure analysis by field service personnel, and a quick repair
turnaround. The field repair philosophy is based on the distributed and
approved spare parts list. Refer to Appendix A: Replaceable Parts.
This manual is intended to serve as a source of technical information, for
qualified field service personnel to use in servicing SC6002XL patient
monitor in accordance with the Siemens Service Strategy. Field service is
expected to be successful “First-Time Every Time.”
SC 6002XL monitors have several replaceable subassemblies, each of
which also has replaceable subassemblies and/or components.
1.3 Technical Manual Conventions
• Front Bezel Subassembly
• Front Panel PC Board
• TFT-LCD Display Subassembly,
• Main Processor Subassembly,
• NBP Subassembly, and
• Rear Housing Subassembly with integrated serial number chip.
Individual “consumable” replaceable parts include the battery, fluorescent
backlight, and NBP filters. A complete listing of spare parts is included in
Appendix A: Replaceable Parts of this manual. Replacement of components
other than those listed in Appendix A should be performed only at Siemens
service depots in Danvers, MA, U.S.A. or in Solna, Sweden, where
specialized repair and testing equipment can assure product reliability.
The following conventions are employed in this manual:
A NOTE calls attention to items of special interest or provides additional
related information about a specific topic:
Note: Attempting to repair any PC board to the component level may
void any warranty, either express or implied.
A Caution indicates a potentially hazardous situation which, if not avoided,
may result in minor or moderate property damage. It may also alert against
unsafe practices.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 1
6k2XLSMC1.cd-rom.fm/06-00/kaupp
Page 12
SC 6002XL Patient Monitor Field Service Manual
Caution
3
Printed circuit boards in these monitors contain components that
are easily damaged by static electricity. Open monitors only in a
static-protected environment. Observe proper procedures to
prevent damage to the equipment resulting from static discharge.
A Warning indicates a potentially hazardous situation which, if not avoided,
may result in death or serious injury.
Warning
Do not operate this product in the presence of flammable gasses
or liquids. If this device is operated where flammable anesthetics,
skin cleansers, or disinfectants are used, the possibility of an
explosion cannot be excluded. This product must be operated
only in strict conformance with local fire prevention regulations.
2Product Overview
2.1 Monitored Patient Parameters
2.2 SC 6002XL Monitor Controls
SC 6002XL Patient Monitors are light-weight, battery-equipped, hand-held
or semi-permanently mounted devices for general purpose monitoring of
a preconfigured set of physiological parameters. When not connected to a
hospital’s main ac power, they use a battery with approximately 1¼ hours
(3 hrs. for Li option battery) of operating time. A power adapter, CPS/
docking station combination, or IDS, which also charges the battery, can
be used to operate the monitor from the hospital’s main ac power circuit.
The SC6002XL monitors the following physiological parameters:
• ECG (three-lead, five-lead, or six-lead pod)
• Respiration
• Pulse Oximetry (SpO
• Temperature
•NBP
• IBP1, IBP2 (locked option)
•etCO
•Arrythmia
• OCRG (locked option)
• Dual Lead S-T Segment Analysis (locked option, ≥VF0 SW required)
All functions are controlled by a 16-position rotary knob and nine front
panel fixed keys - Alarm Silence, Record, Alarm Limits, NBP Start/Stop, All
Alarms Off, Zoom, Main Screen, Menu, and ON/OFF. Turning the rotary
knob locates different menu items, and pressing the knob in selects the
item. Depending on the item selected, pressing the knob in may either
bring up another menu or initiate an action. See Section 5. For detailed
operating instructions, consult the SC 6002XL Patient Monitor User Guide
applicable to the installed software.
via PodComm Port (locked option)
2
and PR)
2
2.3 TFT-LCD Display
2 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
The SC 6002XL monitor has a 6.5 inch (16.5cm), 3-channel color TFT-LCD
display. Waveforms display in Erase Bar mode at 25 ±20% mm/s (except
for respiration and etCO
All displays for a given parameter (label, unit of measure, and waveform)
are in the same color. If a waveform is not displayed for a parameter, its
label is gray.
waveforms which display at 6.25 ±20% mm/s).
2
6k2XLSMC1.cd-rom.fm/06-00/kaupp
Page 13
Field Service Manual SC 6002XL Patient Monitor
2.4 Alarms
2.5 Monitor/Software Tracking
3Preventative
Maintenance
3.1 General
Alarm limits can be set either on a user-definable setup table, or
automatically based on current parameter values. Three alarm grades,
each with a distinct alarm tone, announce alarm situations of varying
severity:
• life-threatening (asystole or ventricular fibrillation - red)
• serious (parameter limit alarms - yellow)
• advisory (technical alarms - white)
The message field background and parameter field of the parameter in
alarm are displayed in the color associated with the alarm grade as given
above.
Each monitor has a unique ID chip installed in its rear housing for diagnostic
and tracking purposes, and un/locking optional software features.
SC 6002XL monitors require replacement of the lead-acid battery (12 months),
NBP air intake filter (24 months) and fluorescent bulb (45K - 50K hours).
Siemens recommends that a full functional verification be performed
annually. See Chapter 4: Functional Verification and Calibration. Also, some
national jurisdictions require that a temperature calibration (see Section
1.8.2 in Chapter 4) and an NBP calibration be performed at least every two
years. Refer to Section 3, Calibrating NBP System in Chapter 4 for the NBP
calibration procedure.
3.2 Battery
Note: Replace the internal manifold filter on the NBP subassembly
only if the NBP subassembly should fail characterization.
To obtain maximum life from a new lead-acid battery, install the battery
into the monitor and run the monitor on battery power for a period of 15
minutes. After the 15 minute period, either plug in the monitor’s power
adapter or lock the monitor onto a powered docking station and charge the
battery, or remove the battery from the monitor and connect the battery to
an external charger. (This initial sequence is not needed for Li batteries.)
When in storage or not in use for an extended period of time, lead-acid
batteries self-discharge and develop a “float-charge” as a characteristic of
the self-discharge process. The “float charge” must be drained off before
the battery can be properly charged. If a new battery is immediately placed
on a charger, the “float charge” provides an incorrect indication of the
battery’s charge condition, and the charger may not fully charge the battery.
Between discharges, the lead-acid battery must be recharged as soon as
possible. Once charged, it can be stored for ª 4 months without recharging.
Siemens recommends that the battery charge be maintained at >80% to
maximize the battery’s capacity and cycle life. Starting at a 100% charge
level, at room temperature the battery will self-discharge below the
acceptable minimum in about 6 months on a shelf and in about 2 months
in an unpowered spare monitor.
Warning
Dispose of used batteries in accordance with local regulations
governing disposal of hazardous materials.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 3
6k2XLSMC1.cd-rom.fm/06-00/kaupp
Page 14
SC 6002XL Patient Monitor Field Service Manual
4Technical Data
Technical Data included in this Section is as of publication date of this
Manual. Changes are reported in User Guide applicable to installed SW.
4.1 General
Table 1-1 General Specifications
Parameter Specification
Power Requirements 100-250 VAC through AC power adapter
Mains Frequency 50/60 Hz
AC Power Consumption 60 VA AC
Battery Type Lead-acid: PANASONIC LC-T121R8PU or equivalent
Lithium-ion: Siemens Li+ Battery Pack
DC Input 11 - 14 V; 32 W continuous, 49 W peak
Battery Operating Time (means
running with NBP measurement
every 15 min @ 25°C temperature,
no etCO
Battery Recharging Time Lead-acid: 5 ½ hours, typical
Battery Charge/Discharge/Charge: Lithium-ion only (operating as defined above): 2 hours, charging for 2
running
2
Lead-acid: 75 mins
Lithium-ion: 180 mins
Lithium-ion: 8 hours, typical
hours, operating 2 hours
Patient Leakage Current <10 µA @ 110 V and 60 Hz (per UL 544)
<10 µA @ 220 V and 50 Hz (per IEC 601-1)
Chassis Leakage Current with
battery eliminator
<100 µA @ 110 V and 60 Hz (per UL 544)
<500 µA @ 220 V and 50 Hz (per IEC 601-1)
4.2 Environmental
Table 1-2 Environmental Specifications
Parameter Environmental Specification
Cooling Method Convection and cooling chimney (no fan)
Temperature:
Operating
Storage
Relative Humidity:
Operating
Storage
Altitude:
Operating
Storage
0°C to +40°C (without recorder)
-20°C to +50°C
>30% and <95%, non-condensing
>10% and <95% non-condensing
-381 to +3048 m (-1250 to 10,000 ft.)
525 to 795 mmHg (70.0 to 106 kPa)
-381 to 5486 m (-1250 to 18,000 ft.)
375 to 795 mmHg (50.0 to 106 kPa)
Water Resistance Drip-Proof
Dimensions (H x W x D): 196 x 223 x 134 mm (7.7 x 8.8 x 5.3 in) (w/ rotary knob)
4 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6k2XLSMC1.cd-rom.fm/06-00/kaupp
Page 15
Field Service Manual SC 6002XL Patient Monitor
Table 1-2 Environmental Specifications (Continued)
Parameter Environmental Specification
Weight:
SC 6002XL (w/o etCO
)
2
3.42 kg (7.54 lb) w/ lead-acid battery
3.22 kg (7.10 lb) w/ lithium-ion battery
2.87 kg (6.32 lb)) w/o battery
Battery
Lead-acid: 0.55 kg (1.22 lb)
Lithium-ion: 0.35 kg (0.78 lb)
Finish:
according to Siemens
Corporate Design Guidelines
Front: white
Rear and Handle: anthracite gray
Material: ABS Polycarbonate Blend (injection molded plastic)
4.3 Display
Table 1-3 Display Specifications
Parameter Specification
Type Color Thin Film Transistor - Liquid Crystal Display (TFT-LCD)
Size 170 mm (6.7 in) diagonal
Resolution 640 x 480 pixels
Active Viewing Area 132.5 x 99.4 mm
Pixel pitch 0.207 mm x 0.207 mm
Sweep Speeds fixed 25 mm/s ±20% for ECG, SpO
fixed 6.25 mm/s ±20% for Rsp and etCO
, and IBP curves
2
curves
2
Display Mode Erase bar (updates waveforms from left to right)
4.4 Outputs
Table 1-4 Output Specifications
Parameter Specification
QRS Synchronization:
Timing:
Output Pulse:
Alarm Output 12 V Open collector output for external alarm indicator
Recorder UART interface w/ recorder through interface plate or docking station
Debug Port UART interface w/ a PC to retrieve diagnostic information through
External VGA Video signals sent to external VGA display for remote viewing of
Export Protocol UART interface w/ external devices using proprietary export protocol. --
Network Serial connection to Infinity Network through Infinity Serial Hub interface
For heart rates from 30 to 250 [1/min], with QRS widths from 40 to 120
msec and QRS amplitudes from 0.5 to 5 mV, a sync pulse is delayed no
more than 35 msec from peak of R-wave for each valid QRS complex.
+12 V, 100 ms duration
connector
interface plate or docking station connector
SC6002XL screen. -- not available when Infinity Serial Hub interface plate
in use.
not available when Infinity Serial Hub interface plate in use.
plate or docking station connector.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 5
6k2XLSMC1.cd-rom.fm/06-00/kaupp
Page 16
SC 6002XL Patient Monitor Field Service Manual
4.5 Connectors
Table 1-5 Connector Specifications
Parameter Specification
DC Input Siemens 2-pin power connector
Docking Station Siemens 28-pin connector to provide Alarm Output, Recorder, Debug
Port, Network, External VGA and Power
Memory Card PCMCIA slot
QRS Sync Phone jack connector
MultiMed Pod 16-pin shielded female input connector
IBP 7-pin shielded female input connector
NBP Hose One-hand coupling system
etCO
2
Note: For patient parameter specifications, refer to User Guide applicable to installed software version.
7-pin shielded female PodComm connector
5Monitor Controls
5.1 Main Screen Key
5.2 Menu Key
The rotary knob in the lower right corner of the front panel is a pointing and
selecting device. Turn the knob to select a screen area or menu item or to
change a default value, and press the knob in to confirm your selection and
to set a default value. Press Main Screen key to return to the MAIN screen.
Note: Instructions in this chapter are intended to provide only a
cursory overview of basic monitor controls for accessing and
performing service-related functions. Refer to the User Guide for the
installed software version for complete operating information.
Pressing the Main Screen key exits the current menu or screen and
displays the home screen.
-- provides access to the Main menu. In general, functions of direct
concern to the CSE or Biomed are accessed via Monitor Setup →
Biomed on the Main menu. Password-protected service-related
functions are to be performed by only authorized technical
personnel. Use Biomed password (375) to access the following:
• Save Setups - Confirm or Cancel
• Locked Options - four locks into which monitor-specific 2-digit codes
must be entered to enable locked options
• Diagnostic Logs
•Units
- Temperature - °C or °F
- Pressure - mmHg or kPa
• Service - requires Service password. (The password is given on the
Service Setup Instructions for the installed software version.)
- Update Software
- Line Frquency - set the frequency equal to the ac mains line
according to local conditions (50 or 60 Hz).
Note: An incorrect setting of line frequency can cause artifact or excessive waveform noise on the ECG waveform.
- Language - selection appropriate for clinical site
6 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6k2XLSMC1.cd-rom.fm/06-00/kaupp
Page 17

Field Service Manual SC 6002XL Patient Monitor
- Test Pulse - Confirm or Cancel, one-shot test pulses for ECG
(1mV spike) and Temp (–5°C and +50°C, respectively). An
additional test is performed for IBP, Resp Pulse, and SpO
indication is reported in the trend table.)
•Exit
. Test
2
5.3 Alarm Limits Key
5.4 Alarm Silence Key
5.5 All Alarms Off Key
5.6 NBP Start/Stop Key
5.7 Zoom Key
5.8 Record Key
-- calls up a setup table for alarms.
1) Turn rotary knob to select desired parameter field and limits, and
press knob in to activate your selection.
2) The number representing the limit value turns black on a blue background, indicating that you can change it. Turn knob to change value.
3) When desired setting is displayed, press knob in to set value.
4) Press MAIN Screen key to return to MAIN screen.
-- silences an active alarm tone for 1 minute ±5 seconds, and turns active
blinking parameter areas into active steady parameter areas
-- suspends alarms for a fixed 3-minute ±5 second period.
-- starts and stops non-invasive blood pressure measurement.
-- used for fast access to all parameters or NBP parameter box bottom
channel screen setups, choice made from a user menu.
With an R50™ recorder connected, press the Record fixed key to start a
manual, timed recording.
Note: If a recorder is not connected, pressing the Record fixed key
writes 15 seconds of waveform and vital signs information to internal
memory. SC 6002XL monitors can store up to five recordings, which
are automatically printed as soon as the recorder is connected.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 7
6k2XLSMC1.cd-rom.fm/06-00/kaupp
Page 18

Field Service Manual SC 6002XL Patient Monitor
This page intentionally left blank.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 8
6k2XLSMC1.cd-rom.fm/06-00/kaupp
Page 19
Chapter 2: Functional Description
Overview
1
SC 6002XL monitors are configured patient monitors running on one
processor, an MPC821 Power PC processor, which attends to all
monitoring functions, controls all graphics functions, generates video and
timing signals for the LCD screen, and interfaces with the PCMCIA. It also
performs several peripheral control functions, such as NIBP control, audio
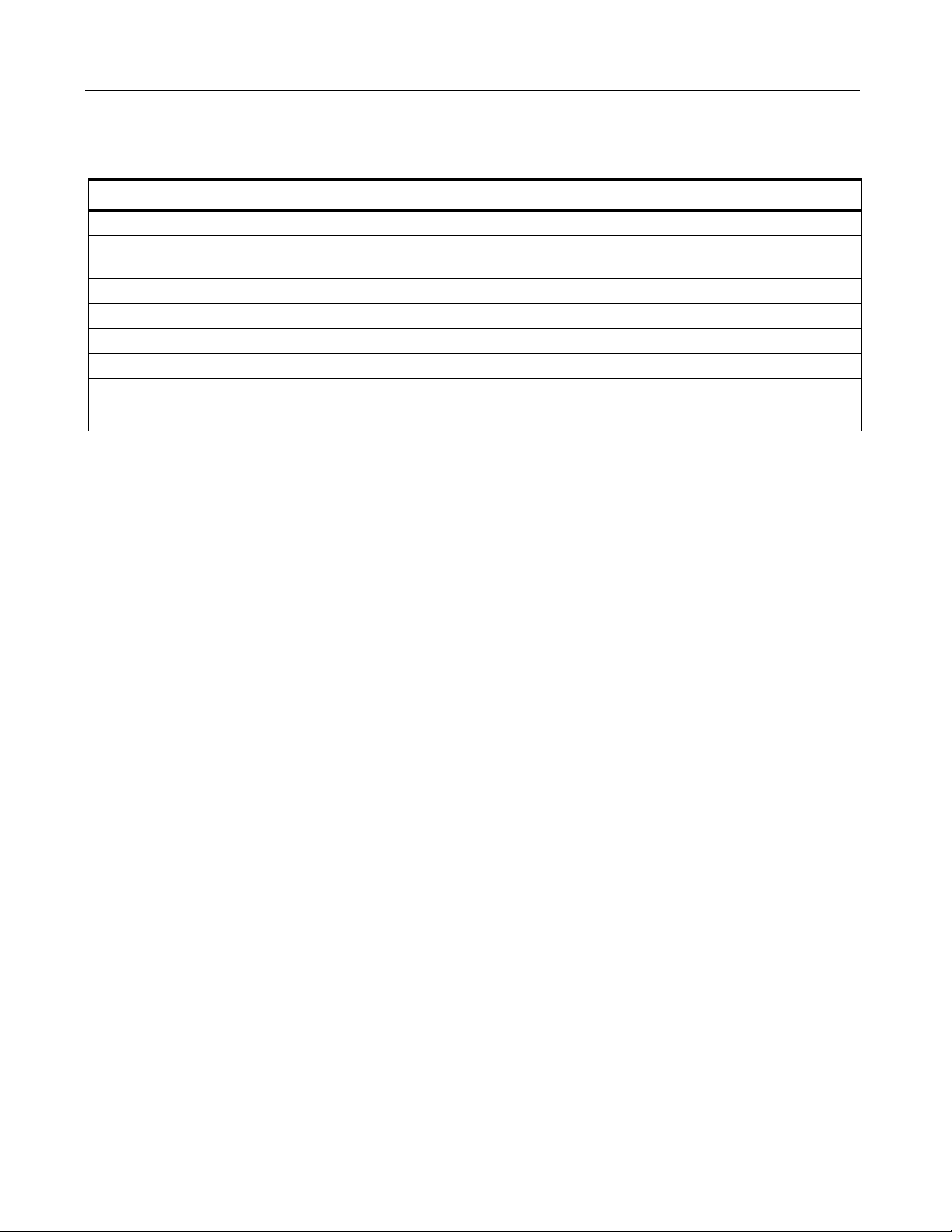
volume control, and timing generation for the front end. See Figure 2-1.
SpO
IBP1
IBP2
Temp
Resp
2
ECG
M
U
X
LED Drive
M
U
X
NIBP
A
D
C
Front End
Record
Debug
Export
To
etCO
2
Front Panel
Double
Xducer
Meas.
Safety
A
S
I
I
s
C
o
l
a
t
i
o
n
CUFF
NIBP
Driver
µController
(68HC11)
832 16
SRAM
Memory
(512KB)
Audio Keyboard
LCD
Control
CP
Processor
(MPC821)
DRAM
Memory
(4MB)
Video
DAC
Network
(HDLC/
CEPT)
PCMCIA
Card
Flash
Memory
(2MB)
LCD
(640 x 480)
X
F
M
R
Quad
UART
PodCom
Option
RGB
Network
+12
11 - 15v
POWER
CONVERSION
+3.3V
+5V
+18
+42
-5V
BATTERY
CHARGER
(Li or Pb)
Main Board
Figure 2-1 SC6002XL Patient Monitor Block Diagram
2 Parameter Inputs
The data acquisition front end acquires and digitizes signals derived from a
three-, five-, or six-electrode ECG patient lead set, a Nellcor® SpO
2
transducer, an Impedance respiration measurement system, a thermistorbased Temperature transducer, and two strain-gauge IBP transducers
(IBP2 = locked option). The NIBP main transducer signal is digitized
together with the rest of the front end parameters. See Section 4 and
Section 5 for more detailed information.
3 Main PC Board
The Main MPC821 Power PC processor not only attends to monitoring
functions, but also controls all graphics functions, generates the video and
timing signals for the LCD screen, interfaces with the PCMCIA, and
controls the network link. In addition, it performs a host of peripheral
control functions, such as NIBP control, audio volume control, and timing
generation for the front end.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 9
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 20

SC 6002XL Patient Monitor Field Service Manual
3.1 LCD Control
3.2 Network Interface
3.3 Front Panel Circuitry
3.4 Pod Interface
3.5 Battery Control and ON/OFF Control
A set of buffer/drivers are used to drive the 6.5” screen. In parallel, a triple
video DAC generates analog RGB signals for an external monitor (typically
a CRT).
The SC 6002XL monitor interfaces with the physical interface device (e.g.,
CPS, IDS or IHUB) automatically when connection to the device has been
detected. Connections to I
maintained by software components resident on both the SC 6002XL and
the physical interface device.
The front panel circuit processes the audio information, drives the
fluorescent tubes on the LCD, implements a secondary alarm in case the
unit resets or turns off, and routes the video and timing signals to the
screen. It also routes the UART signal coming from the Pod interface to the
main board Quad UART.
The Pod Interface generates an isolated voltage to power the pod and also
converts the Pod Comm protocol from the pod into a UART stream that can
be interpreted by the microprocessor.
The Pb-acid or Lithium battery charging and discharging cycles are
controlled by a special charger circuit. The circuit initiates a charge cycle
when commanded by the microcontroller. The charge cycle for a Pb-acid
consists of a bulk charge period in which the battery is being supplied a
constant current of ~400mA, a constant voltage period in which the battery
voltage is held constant at ~14.8V and the current is allowed to diminish as
the charge approaches 100%, and a float cycle in which the voltage is
maintained at ~13.7V. For Lithium batteries, the charger circuit acts as a
constant voltage source of 16.8V. The battery is charged from a switching
supply controlled by the charger chip. The microcontroller also reads the
front panel keys and the rotary knob, encodes the information coming from
them, and routes it to the main processor. When the On/Stdby key is
pressed, it turns the monitor on and off. In addition, the microcontroller
controls the NIBP safety timer.
NFINITY
network services are established and
3.6 BOOT Process, Flash Memory, and DRAM
3.7 SRAM
3.8 68HC11 Microcontroller
10 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
The BOOT EPROM contains the boot code and must be preprogrammed
at the factory. It cannot be programmed after being installed on the Main
board, and therefore cannot be updated in the field via a software
download.
The executable software normally resides as compressed operational code
in Flash memory. When the 68HC11 microprocessor senses that the on/
off switch on the front panel has been pressed, it turns on (or turns off) the
3.3V and 5V supplies. As the 3.3V supply turns on, it wakes up the MPC821
main processor, which begins execution from the BOOT PROM. During
boot initialization, the main processor attempts to read the Memory Card
to detect legal software. If a legal software memory card is present, the
software is loaded from the card. Otherwise, the main processor loads
software from the Flash to the main processor DRAM, from which it
completes initialization and enters operational mode. DRAM contains
expanded operational code, and data space variables and stacks.
The 512K x 8 SRAM is battery backed up and is used for error logs, trends,
recordings and other non-volatile memory uses.
The 68HC11 Microcontroller, with 2K of EEPROM and 256 bytes of RAM,
is powered as long as there is a main supply plugged into the system or
when the user presses the ON/OFF button. The code is stored in its
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 21

Field Service Manual SC 6002XL Patient Monitor
internal flash memory, but can be downloaded from the MPC821. The
microcontroller performs the following functions:
On/Off control When the ON/OFF pushbutton (either local or remote is pressed), the
microcontroller activates the 3.3V and 5V supplies, which wakes up the
MPC821 through a power-on reset. In addition, the microcontroller has
control over a flyback supply, which comes on any time the unit is plugged
into AC power (in order to charge the battery) or is turned on.
The microcontroller also reads the front panel keys and the rotary knob,
encodes the information coming from them, and routes it to the main
processor.
NBP Valve modulation When directed by the main processor, the microcontroller supplies
modulation signals for the two NBP manifold valves.
NBP Safety Timer When the pump or the valve V2 are turned on, the microcontroller initiates
a 128 sec. timer (90 sec. or 60 sec. for neonates) which, if exceeded,
produces an NBP fault and results in cut off of main 12V power to the NBP
manifold.
Battery Charger The microcontroller initiates a battery charge when needed, and stops the
charging process when the battery reaches full capacity. It can recognize
whether a Pb or Lithium battery is connnected into the sytem, and directs
the battery controller chip to charge to different levels depending on the
battery type. See Section 3.5. The microcontroller also acquires the battery
voltage and current for monitoring purposes.
Recorder Power The microcontroller controls the power applied to a stand-alone R50
Recorder.
Main Audio Generator The microcontroller generates the fundamental audio frequency of the
unit’s tone generator, as directed by the main microprocessor.
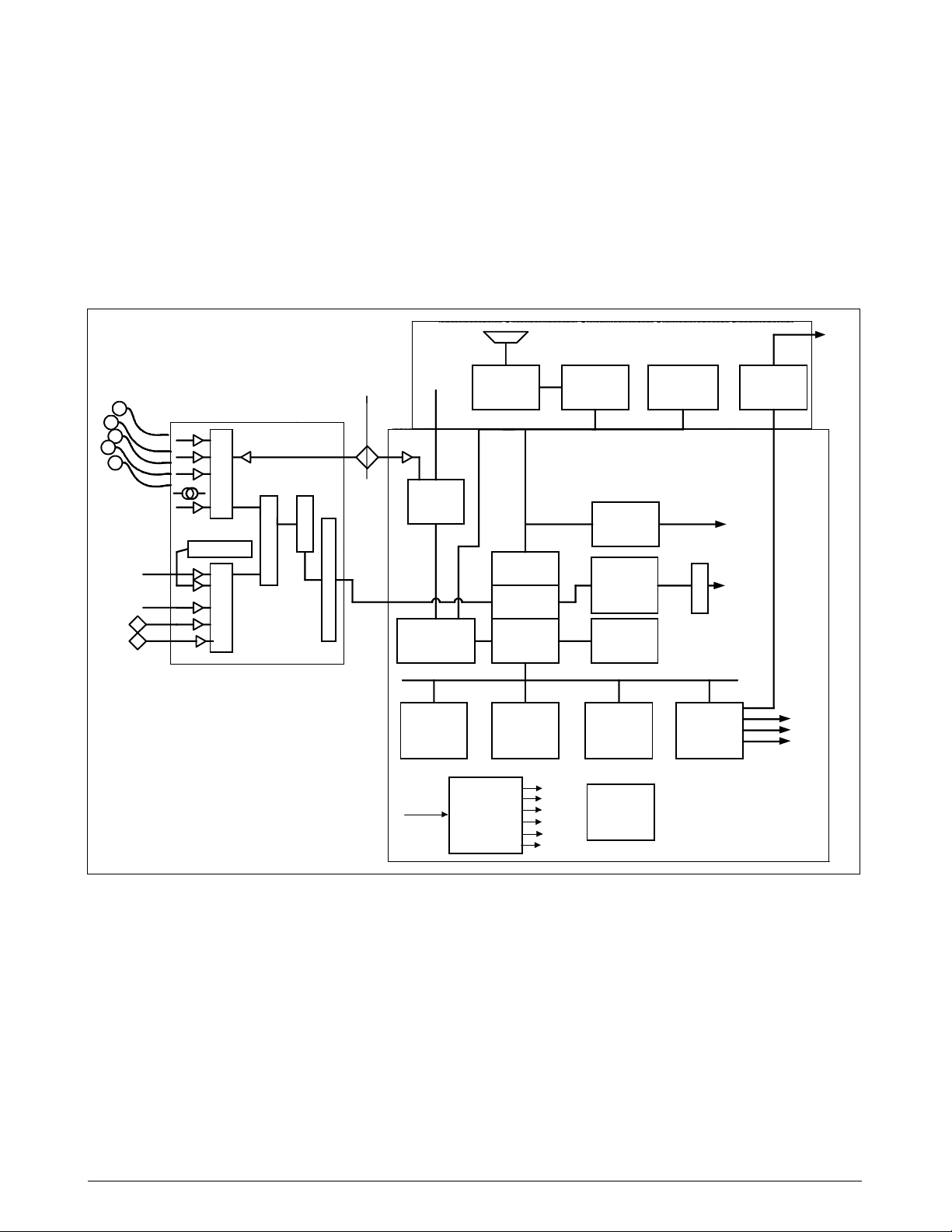
4Front End All physiological signals (except etCO
multiplexing system and a common 16 bit ADC. The data is then
transferred through the isolation barrier to an HDLC port in the main
processor, where it is digitally filtered and processed.
4.1 NIBP Control
4.2 Safety
The NIBP main transducer signal is digitized together with the rest of the
front end parameters. However, the redundant (overpressure) transducer
is processed separately on the grounded end of the board, and the pump
on/off signal and valve enable signals are generated off of the MPC 821
microprocessor. The PWM signals for the valve flow control and the
redundant safety timer are implemented in a separate microcontroller
(MC68HC11).
• Patient isolation withstands 5kV during defib.
• Leakage currents are limited to safe values normally and during single
fault conditions.
• Patient is protected against electrosurgical burns at the electrodes.
• Defibrillation protection does not drain excessive current away from
the patient.
) are digitized through a high speed
2
• Specially shielded connectors and cables are used to provide
excellent immunity up to 1000MHz and can not be touched by the
patient even when disconnected.
• Single cable from MultiMed Pod to main SC6002XL unit reduces
clutter between bed and monitor.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 11
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 22
SC 6002XL Patient Monitor Field Service Manual
Temp
ECG
Resp
SpO
MultiMed
Protection
2
Defib
ESU
NBP
Hose
RF Filter
Lead Off
Neutral
SW
Modulator
Pressure
Transducer
Pre-
Amp
Modulator
Demodulator
LED Drive
Linearizer
Low-Pass
Filter
Bandpass
Filter
Current
Sources
Bandpass
Filter
Power Monitor
Amp
Amp
Amp
NBP
Amp
Temp
Temp Ref.
ECG
Pace
Resp
Amp
Cal Resistor
4
2
2
6
4
2
M
U
X
2
Converter
Control
Power
16 Bit
A / D
Asic
Data Control
Figure 2-2 Front End
5 Physiological
Parameter Data
Acquisition
5.1 ECG/Resp
Differential
I/V
Converter
Red
Ambient
Light
Rejection
Demodulator
I/R
HDLC
(to MPC821)
Transducers gather physiological data at the patient and feed them into the
small MultiMed Pod at the bed. The MultiMed Pod in turn is connected via
a 3-meter cable to the front end in the main unit where analog ECG,
Respiration, Temperature, and SpO
signals are converted to digital form
2
and sent through isolators for processing.
The MultiMed Pod located close to the patient accepts a set of 3, 5 or 6
shielded ECG electrode leads, an SpO
(Nellcor) cable adapter, and a
2
temperature sensor. The ECG section contains RF filters, and overvoltage
clamps that include 1k series resistors to limit shunting of defibrillator
current. The SpO
and temperature sections also contain RF filters.
2
Impedance respiration is sensed through the ECG electodes. Void-free
potting and internal shielding enable compact containment of high voltage
defibrillator and electrosurgery pulses. The small interconnecting cable to
the main assembly is captive at the MultiMed POD but plugs into the
MultiMed front end via a specially shielded connector.
The front end accepts physiological signals from the MultiMed POD
connector and feeds temperature, respiration, and ECG signals via RF
filters, configuration multiplexers, and pre-amplifiers to a high-speed
12 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 23

Field Service Manual SC 6002XL Patient Monitor
multiplexer driving a 16-bit analog-to-digital (A/D) converter. The data
stream is sent to the Main Processor board via an opto-isolator. Control
commands from the Processor are sent out to the front end on a similar
isolating link. Isolated DC power is also provided.
The ECG signals are conductively coupled to the isolated circuits via
current-limiting series resistors, whereas the SpO
isolated at the transducer. Temperature signals are doubly insulated at the
patient by disposable boots on the sensors. AC (40kHz) excitation currents
for respiration monotoring are dc-isolated by high-voltage ceramic
capacitors.
The A/D samples the following parameters:
Table 2-1 Parameter Sampling Table
Parameter # of Channels
signals are optically
2
ECG 4
Pace 2
Red 1
SpO
2
IR 1
SpO
2
NBP 1
Resp 1
Temp 2
The hardware pace detector monitors the ECG signal in two of the four
channels (those not connected to the chest leads). All other signals are
decimated and filtered using digital signal processing in the MPC821. High
oversampling rate is required to minimize the requirements (and size) of
the analog anti alias filters. Superior rejection to ESU and other types of
interference is achieved with this type of design.
5.1.1 ECG • Bandwidth is set flexibly by software filters.
• Reconfigurable neutral selector can drive any electrode.
• Lead-on detection functions with even poor electrodes.
• Calibration voltages can be superimposed on patient wave-forms or
onto flat baselines.
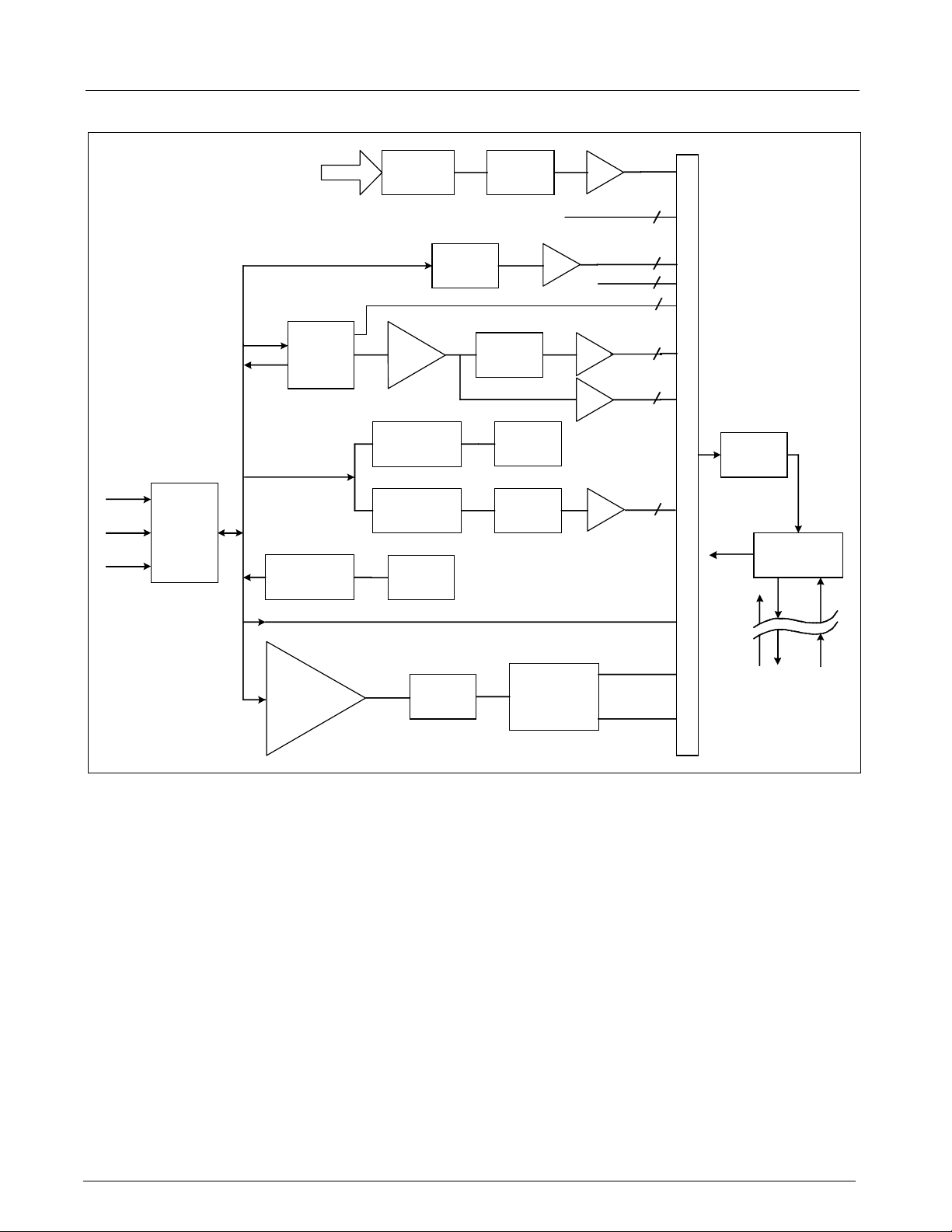
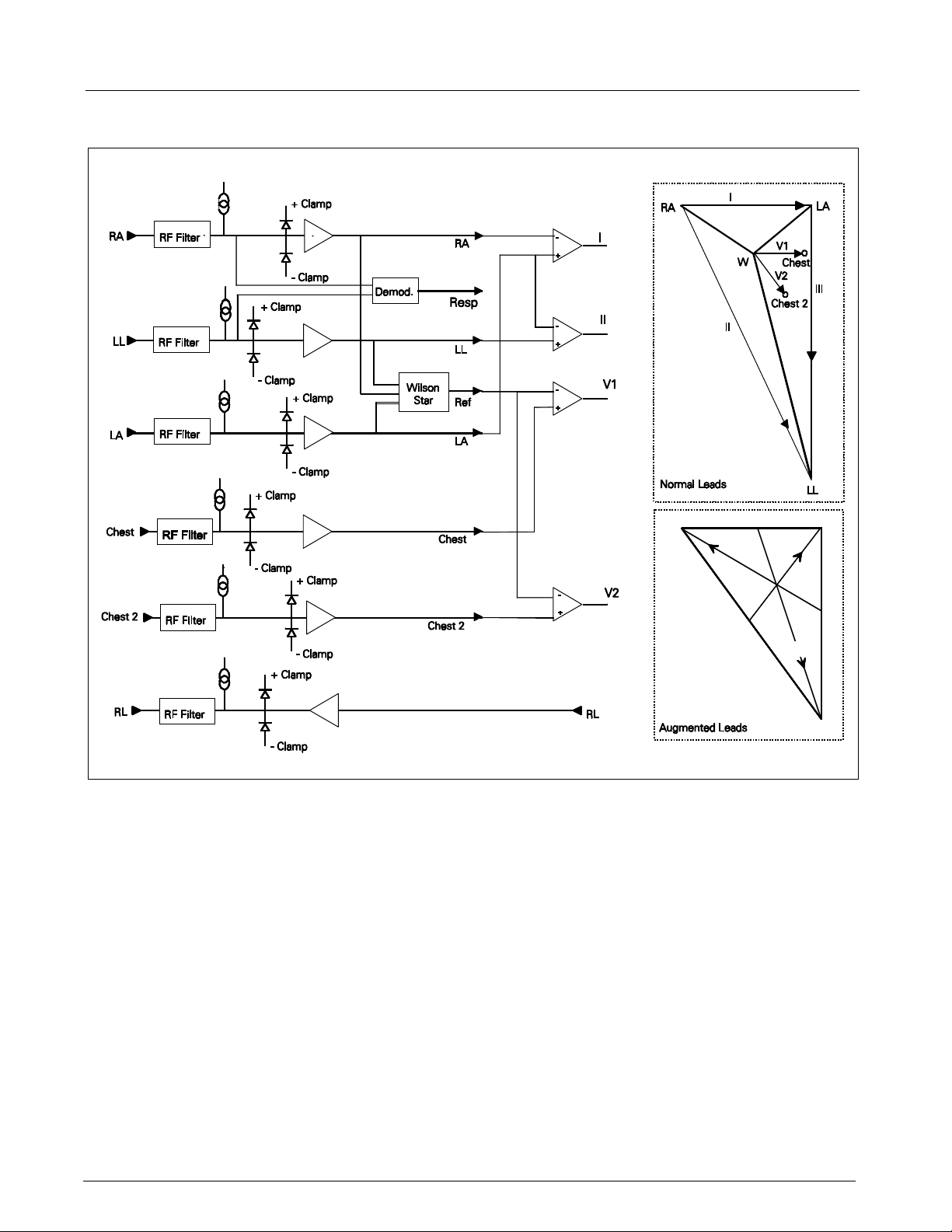
See Figure 2-3. Composite electrocardiographic (ECG) signals generated
by the heart and by a pacemaker are filtered to reduce RF interference
from impedance respiration and electrosurgery and then injected with dc
lead-off detection currents. Over-voltage clamps protect the
semiconductors from the surges passing the sparkgaps in the MultiMed
Pod and also reduce the dc current applied to the patient due to a
component fault.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 13
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 24
SC 6002XL Patient Monitor Field Service Manual
RA
aVLaVR
LA
aVF
LL
Figure 2-3 Lead-Forming Network
5.1.2 Lead Selection A lead-forming network following the RF filter generates the necessary reference points for electrocardiographic measurements. Both normal leads (I, II, III, V1 and V2) and augmented leads (aVL, avR, and avF) can be obtained. See Figure 2-3.
Four differential channels generate the main axes I, II, V1 and V2. The
remaining leads are derived mathematically as indicated in the vector
diagram of Figure 2-3.
5.1.3 Lead-Off Detection Lead-off detection is accomplished by introducing a very small current into each patient electrode, which would drive the corresponding input high if it were disconnected. A set of five comparators detects a lead-off condition.
5.1.4 Low-Pass Filtering and
Common Mode
Enhancement
The ECG preamplifier has a flat frequency response of 0.5 - 40Hz, with a
software notch filter at 50/60 Hz. A 180° combined signal drives the neutral
electrode to increase the CMMR.
14 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 25
Field Service Manual SC 6002XL Patient Monitor
5.2 Respiration
5.3 SpO
2
Impedance respiration is monitored by injecting a 40 kHz square wave of
current into the RA electrode. The resulting 40 kHz voltage drop between
the RA + LL electrodes is proportional to the impedance. Especially
balanced true current sources do not load the ECG electrodes or distort the
ECG morphology. The returning 40 kHz differential voltage is amplified,
synchronously demodulated, and low-pass filtered. An AC-coupled stage
with an “autobloc” DC restorer feeds the input to the A/D converter with
a nominal output of 60 mV per Ohm.
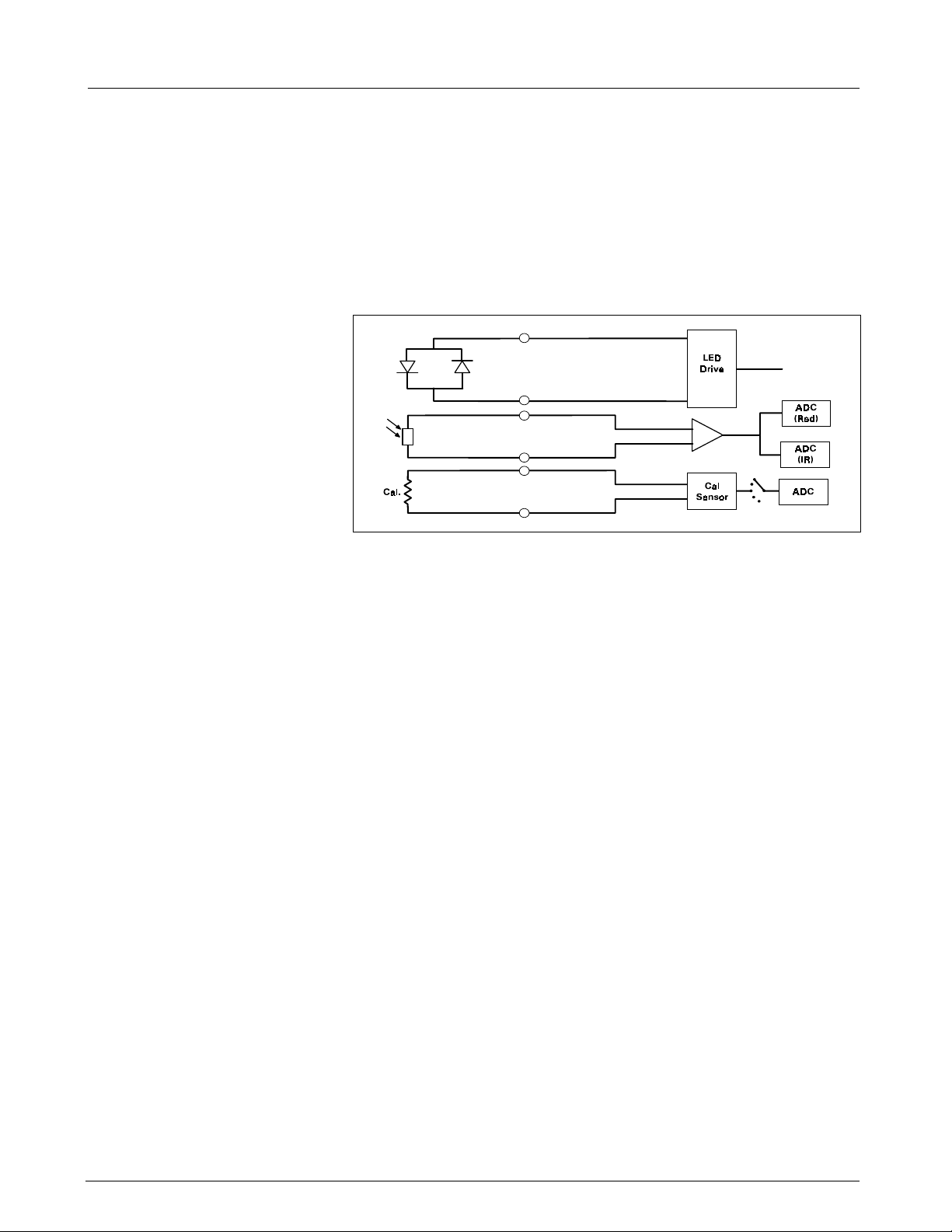
Figure 2-4 SpO
Functional Block Diagram
2
The pulse oximeter circuit uses a Nellcor® sensor to detect the oxygen
saturation level in arterial blood flow. Determination of the concentration
of oxygen in the blood is based upon the principle that the absorption of
red (R) light depends on the degree of oxygenation of the blood, whereas
the absorption of infrared (IR) radiation is relatively independent of
oxygenation and causes only constant attenuation. See Figure 2-4. In the
SpO
sensor, R and IR light emitting diodes (LEDs) are alternately pulsed
2
ON at a 25% duty cycle. The light is transmitted through a well-perfused
part of the body, such as a fingertip or an ear lobe. The intensity of light
(including ambient) transmitted through or scattered by the blood is
converted to a current by a photodiode in the sensor. The current that
appears when both LEDs are OFF depends mainly on the ambient light,
which is later subtracted to leave only the R or IR signal levels. The large
dynamic range of the light intensities requires constant automatic
monitoring and adjustment.
The intensities of the R and IR sources are independently controlled by two
digital-to-analog converters (DACs) attenuating the 2.5 V reference. These
levels or zero are sequentially selected by a multiplexer, and converted to
a driving current which is further guided or inverted by an output
multiplexer to the LEDs in the sensor.
5.3.1 SpO
Front End The primary purpose of the SpO2 front end is to convert the sensor’s
2
analog signal into individual digitized signals for the red and infrared analog
signals for processing by the microprocessor. See Figure 2-5 on page 16.
Circuitry in the front end first eliminates the non-pulsatile component in the
input signal, then demultiplexes the resulting pulsatile signal to separate
the R and IR signal components, and finally converts the demultiplexed R
and IR analog signals into serial digital data streams.
A sequence of light pulses, driven from the chopped current source in the
sensor LEDs, are passed through a finger or an earlobe to a photodiode.
The sensor LEDs are connected in an anti-parallel fashion on one pair of
wires.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 15
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 26
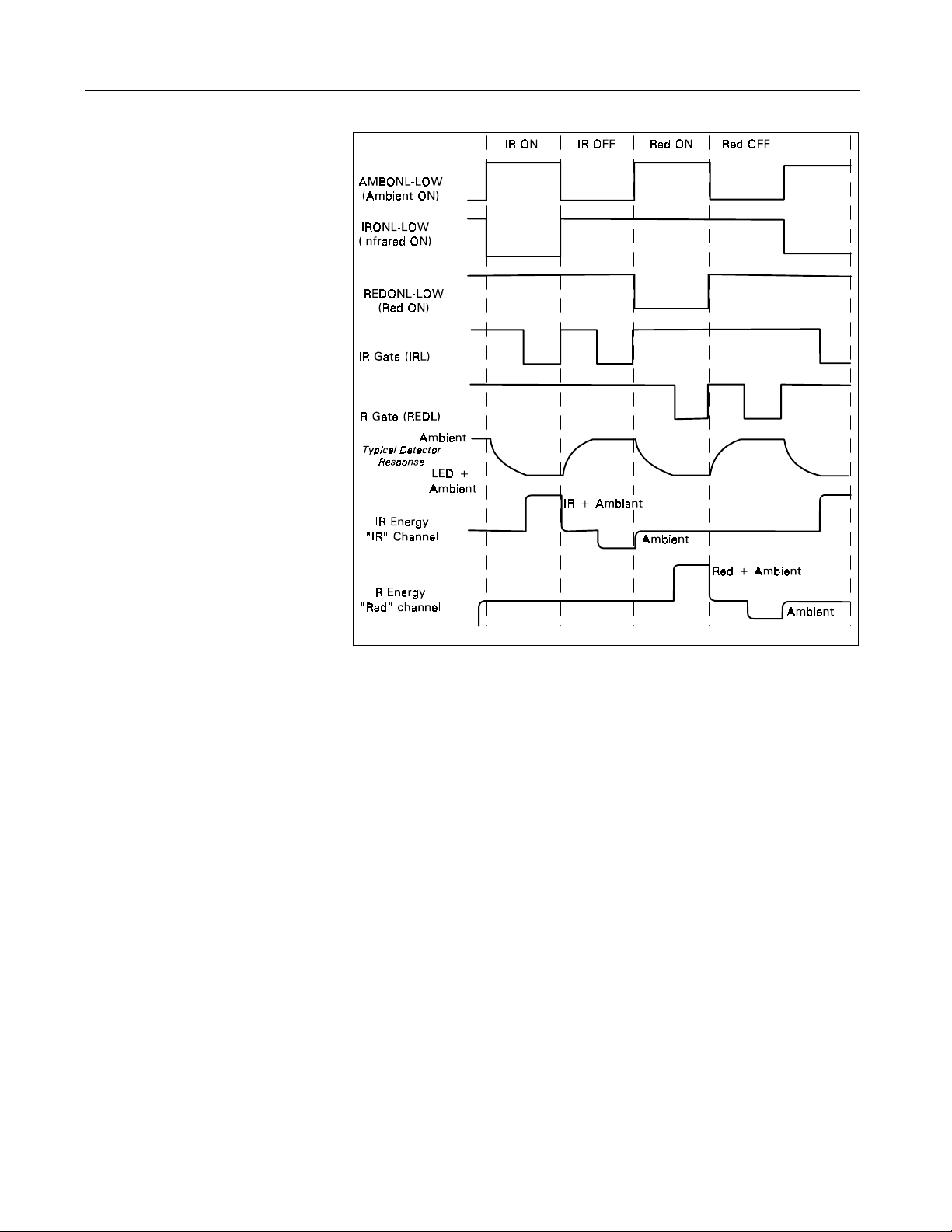
SC 6002XL Patient Monitor Field Service Manual
Figure 2-5 Sensor LED Timing Diagram
A timing generator controls the sensor LEDs and signal multiplexing/
demultiplexing (see Figure 2-5) by means of three control signals:
• IRONL (infrared LED)
• AMBONL (LEDS not lit)
• REDONL (red LED)
5.3.2 Input Stage A preamplifier converts the photocurrent to an equivalent voltage, and applies it to a 20 Hz high-pass filter that removes the non-pulsatile component. The output of the preamplifier is fed to a saturation detector.
5.3.3 Brightness Control If the output of the preamplifier is in saturation, the gate array provides a signal to the digital-to-analog converters (DACs), which controls the drive current to increase or decrease the brightness of the LEDs.
Controlling LED brightness extends the system dynamic range. For a very
transparent subject it may not be possible to reduce the gain to prevent
saturation. In that event, the brightness must be reduced. An additional
purpose is to equalize the received amplitude of each wavelength. If both
LEDs are turned ON to maximum brightness, and the software finds an
extraordinary difference between the two, the microprocessor tends to
reduce that difference by equalizing the R or IR brightness signals.
5.3.4 Ambient Light Rejection
Amplifier
The ambient rejection amplifier is a synchronous detector. The signal
appied to its inverting input is a composite of R, IR, and ambient signals.
The non-inverting input is the same signal gated by the timing generator.
This synchronously multiplexes the IR, ambient, and R analog signals.
16 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 27
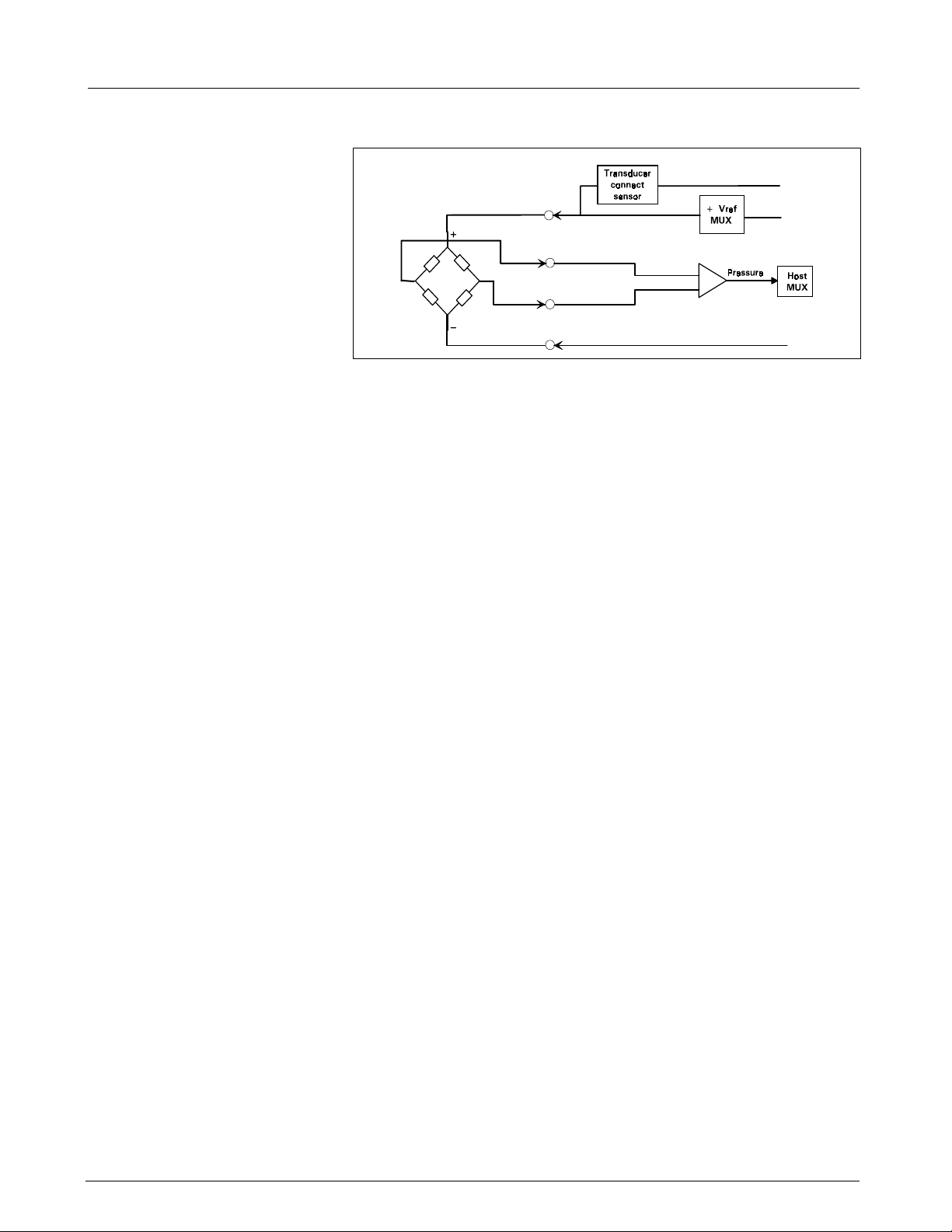
Field Service Manual SC 6002XL Patient Monitor
+2.6V
-2.6V
Figure 2-6 IBP Functional Block Diagram
5.4 Invasive Blood
Pressure
The IBP circuit has been designed to be used with a strain gauge pressure
transducer. See Figure 2-6. The analog portion of the IBP circuit provides
excitation voltages for resistance bridge transducers. These voltages are
derived from a reference which is also used to derive the A/D converter
reference voltage. At the circuit input, a resistor divider network provides
for transducer unplugged detection. R-C filtering and protection diodes
limit the effects produced during electrosurgery, defibrillation, and other
such procedures. A selector multiplexer allows for the insertion of
calibration signals into the amplifier stage. The multiplexor feeds the
pressure signal to a buffer amplifier, which in turn feeds the AD converter
analog input. This allows the monitor to measure pressure signals in a
range greater than ±700 mmHg with a resolution of approximately
.02mmHg/LSB.
When no pressure transducer is plugged into the monitor, the resistor
divider network puts a negative signal into the instrumentation amplifier,
which propagates through the system to indicate the unplugged condition.
5.5 Non-Invasive Blood
Refer to Figure 2-7 on page 18.
Pressure
5.5.1 NBP Subsystem The NBP subsystem consists of the following components:
•pump
•two modulating valves
• strain-gauge pressure transducer
• overpressure sensor
• pneumatic manifold
In addition, an electronic data acquisition and control system measures and
digitizes the pressure pulses as the cuff inflates and deflates. Pump and
valve control circuitry engage these elements as needed in the
measurement cycle. Several interlock systems and expiration timers
ensure the safety of the equipment in case of single point failures.
The SC6002XL NBP circuit uses a cuff and the oscillometric method to
determine blood pressure without using a microphone. A strain-gauge
pressure transducer is DC-coupled to a 16-bit A/D converter, so that cuff
pressure is measured with adequate resolution to detect blood pressure
pulses. This eliminates the need for a separate ac-coupled measurement
channel, with its associated distortion and long transient recovery.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 17
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 28
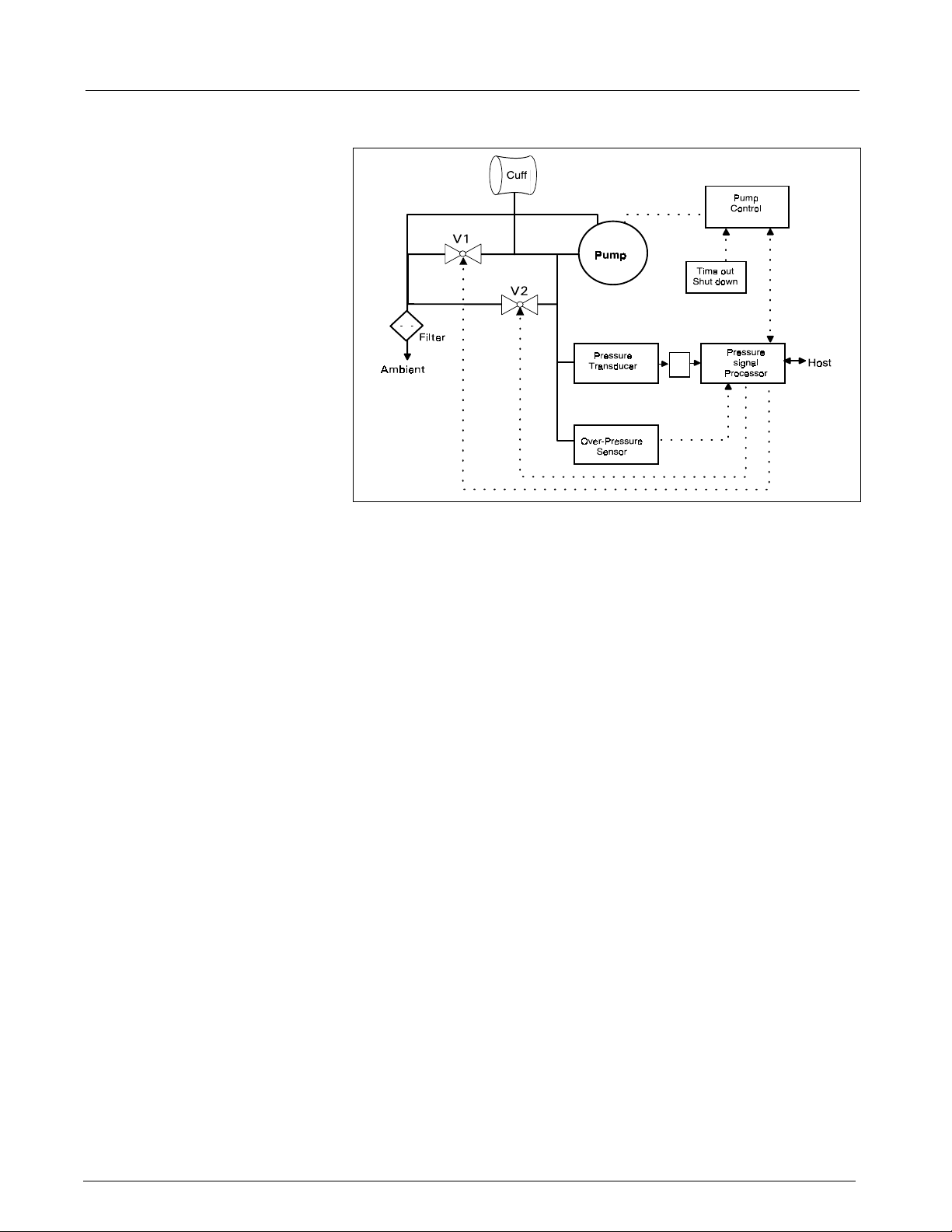
SC 6002XL Patient Monitor Field Service Manual
A/D
Figure 2-7 NBP Functional Block Diagram
5.5.2 NBP System Description The combination of high-resolution A/D conversion and digital filtering, together with wide-range linear deflation control allows the circuit to measure blood pressure very rapidly and accurately, and to recover quickly from motion artifacts. The non-invasive pressure system is composed of the following components:
• pneumatic assembly
• electronic circuitry, mounted on the Main CPU Board
Pneumatic Assembly The pneumatic assembly contains a pump, two modulating valves (V1 and
V2), two air filters (intake and manifold), and a manifold assembly which
interconnects these components. The pump provides the pressurized air
to inflate the blood pressure cuff. V1 and V2 control the air flow during the
deflation phase of a blood pressure measurement. V1 is a normally-closed
exhaust valve with a relatively small orifice (relative to V2). V2 is a normallyopen exhaust valve with a relatively large orifice. The pump speed can be
controlled to permit accurate inflation pressures for special applications.
The filters prevent potential contamination of pneumatic components by
debris coming from the cuff or hose.
Electronic Circuitry The electronic circuitry, mounted on the Main CPU Board, contains the
electrical drivers for the pump, the valves, and its power supplies. In
addition, the readback from the pressure transducer is processed through
the floating section ADC. The software data acquisition and algorithm
processing is performed in the MPC821 main processor.
5.5.3 Operation The measurement sequence consists of an inflation phase, in which the air pump inflates the cuff, which has been wrapped around the patient’s limb (typically the upper arm or thigh) to a predetermined pressure. At this point, the blood circulation to the limb is occluded. The monitor then linearly deflates the cuff at a software-controlled rate during which time the blood pressure parameters are determined by digital filtering and analysis of waveform data obtained from the pressure transducer during the deflation cycle.
18 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 29

Field Service Manual SC 6002XL Patient Monitor
Inflation Phase When a blood pressure measurement is initiated (via software or front
panel fixed key), V2 closes, the pump turns ON, and the pressure
transducers monitor the ensuing pressure rise. When the pressure has
reached the target inflation pressure, the pump turns OFF and a dynamic
braking circuit rapidly brings the pump to a halt. The target inflation
pressure adapts to the patient’s systolic pressure, just occluding the blood
flow. The software monitors the slope of the pressure curve during
inflation to estimate the cuff volume, a factor used in the deflation
sequence.
Deflation Phase After the pump stops, there is a short delay to allow thermal transients to
settle. Either V1 or V2 is modulated to control the deflation rate. The choice
of V1 or V2 and the initial pulse width is made based on the estimated cuff
volume determined during the inflation cycle. The chosen valve is
modulated at a 20 Hz rate, and the pulse width (open time) is continuously
adjusted to provide a linear deflation rate. If initial deflation was started with
V1, the software may determine that it needs to switch to V2 to maintain
proper deflation. In either case, V2 opens fully (de-energizes) when the
measurement cycle is ended to allow for rapid and complete deflation.
5.5.4 NBP Hardware Pump control circuitry provides the following three functions:
• limits the current to the pump when it starts, to prevent power supply
overload
• dynamically brakes the pump when the pump is shut off
• provides a closed-loop speed control for special low-flow operations
Speed Control Pump speed is controlled by measuring the back-EMF generated by the
motor winding, which is directly proportional to the speed. However, to
obtain a measurement of the back-EMF, the drop caused by copper losses
must be added to the voltage appearing on the motor winding. The speed
control effectively drives the pump at constant full speed.
Current Limit Dedicated circuitry limits the current to the pump. When the current on the
pump is approx. 363 mA, the current loop takes over and limits its value.
The microprocessor and an N-channel FET turn the pump ON.
5.5.5 Valve Control A relatively high pulse voltage is used to drive V1 and V2 to get quick response and extend the pulse-width flow control range.
5.5.6 Power Supplies Separate control logic supplies voltage (+12V) to the pump and V2 to provide them with redundant turn-off capability. Without +12V the pump cannot run, and V2 can neither close nor remain closed. Power supplies necessary for operation of the NBP circuitry are derived as follows:
+5V and -5V Supply The +5V and -5V for the NBP analog circuitry are derived from the floating
section.
+12V Supply The +12V drives the NBP pump and both modulating valves. The 6002XL
flyback supply produces the +12V. This circuit produces several voltages
needed for monitor operation. The main flyback regulation loop is closed
around the +12V output, therefore making it the best regulated of the
multiple voltages generated.
In operation, a resistor network samples the +12V output and feeds it into
the controller chip error amplifier, which compares it to an internal
reference. The duty cycle of the switching transistor is adjusted to null this
reference. A separate current feedback loop is used to stabilize the circuit
and provide current limiting protection.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 19
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 30
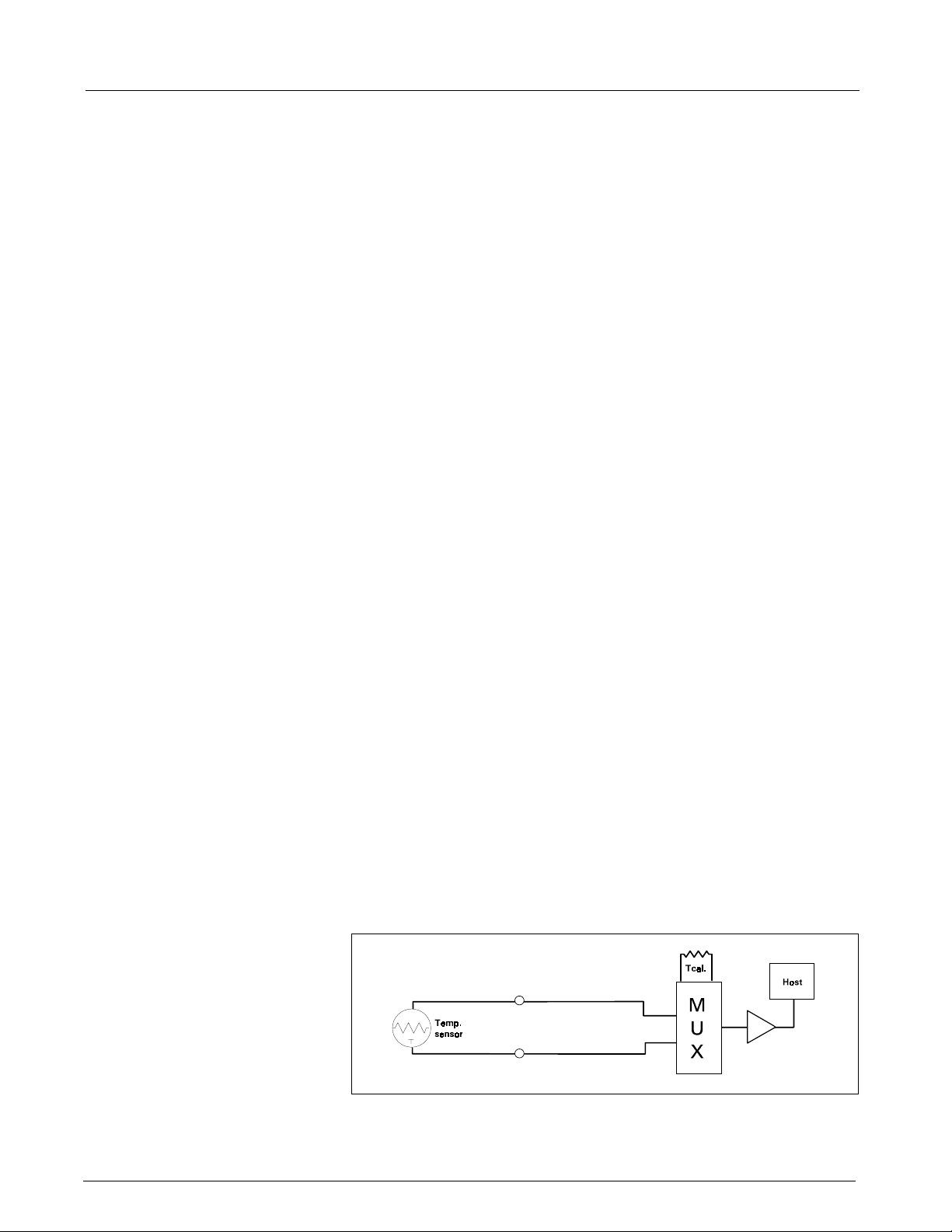
SC 6002XL Patient Monitor Field Service Manual
+36V Regulator A +36V supply used to accelerate the energizing of the valve coils is
derived from the 42V raw supply generated by the flyback supply.
5.5.7 Power Supply Monitor The power supply monitor circuit provides reset logic to the microprocessor, and the redundant power switch circuit, both at power-up and in the event of a power failure or voltage drop. The heart of the monitor is a power supervisor chip. At power-up, the control line is held low for a period of about 200 ms, after which the voltage rises to the +5V level. After start-up, any dip in the +5V that causes the output to go to less than +4.75V causes the same sequence. A resistor network is used to monitor the +12V supply. When the voltage on the reference signal falls below +1.25V, a reset sequence similar to the one described above ensues. The +5V and -5V are monitored via the floating section ADC.
5.5.8 Safety Timer The safety timer becomes active only after starting the pump at least one time. Once the pump has been activated, the timer circuit operates regardless of whether the pump has been turned off. Starting of the pump is sensed by voltage developed across the pump sense resistor. If as a result of some failure, hardware or software, the pump continues to run longer than the timer expiration period, a microcontroller output rises and opens a redundant switch, which causes the pump to turn off and V2 to open.
The safety timer period is derived from the microcontroller clock. Note
that, for redundancy purposes, the safety timer is implemented not in the
MPC821 but in the 68HC11 microcontroller.
Among other signals multiplexed into the floating section data stream are
power supply monitor voltages. Measuring these voltages gives an
indication of the integrity of the power supplies and the A/D converter
voltage reference.
5.5.9 Pressure Channels Pressure fluctuations in the cuff change the balance of the pressure measurement bridge, resulting in a differential voltage which is fed into an amplifier. The gain of the amplifier is determined by the setting of a calibration potentiometer. This potentiometer is initially adjusted in the factory, and from then on the calibration should be checked every year.
The overpressure hardware is fed by a single power source. This increases
safety of the system, since a failure of the reference voltages does not
impact operation of the overpressure channel. An overpressure test is
performed at each power-up cycle to ensure that the overpressure
circuitry is working. Any error detected in the overpressure comparator
circuit is fed to the redundant power switch circuitry described above. The
software overpressure detection is completely independent of the
overpressure circuitry.
Figure 2-8 Temperature Functional Block Diagram
5.6 Temperature Circuit
Temperature measurements are made using a thermistor probe that is
electrically equivalent to YSI
400 series probes. See Figure 2-8.
20 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 31
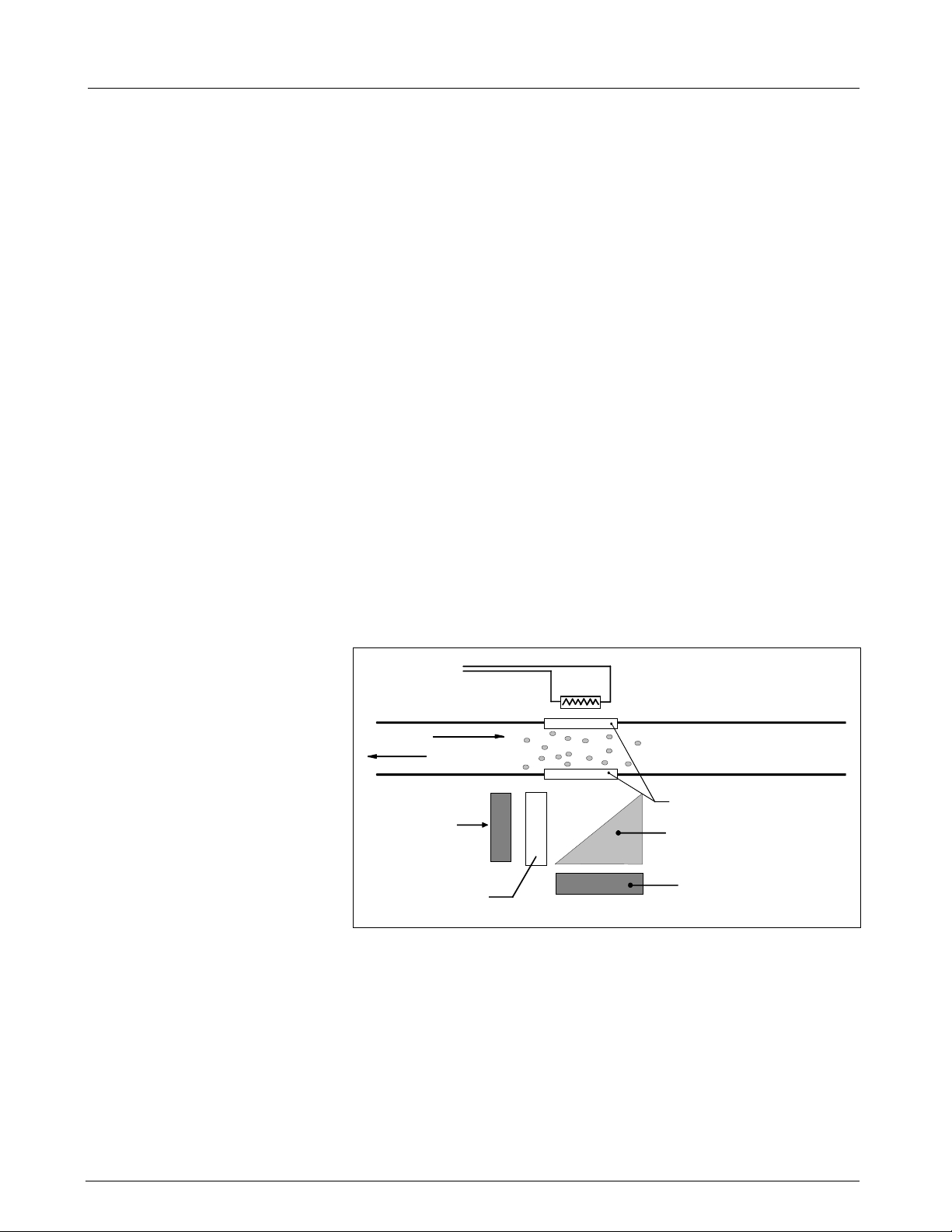
Field Service Manual SC 6002XL Patient Monitor
5.6.1 Reference Networks Two independent reference networks are used to verify correct circuit function by measuring the difference between the reference network ratio values (simulating -5°C and +50°C temperatures), and reporting an error if that difference exceeds the expected range of values. The reference networks are also used to cancel offset and gain errors in the measurement circuits. The measurements of the two references allows for the determination of circuit offset and gain within the accuracy of the reference networks.
5.6.2 A/D Converter A resistor network linearizes the voltage versus temperature curve of the thermistor to within ±2°C. Later the curve is further linearized to 0.01°C, using a look-up table in the microprocessor. The maximum power to the thermistor element is limited to 50 µW. To maintain high accuracy, all signal voltages are ratiometric to the A/D converter voltage reference. The sensitive electronics are protected from damage by an RF filter and an overvoltage clamp.
A multiplexer selects one of three inputs: T1, T-5, or T50. T-5 and T50 are
used in a two-point error correction algorithm, to measure the actual gain
and offset of the measurement circuit. The T-5 and T50 voltages are
created by precision resistor dividers, and are calculated to simulate the
voltage that would appear at T1 when a thermistor probe is at a
temperature of -5°C and 50°C, respectively.
6etCO2 Pod
When a thermistor probe is disconnected from the measurement circuit,
the voltage at the input to the A/D converter reaches a value that is above
positive full scale. The microprocessor is programmed to interpret a
positive full scale value from the A/D converter as a probe disconnect.
IR Source - TFR
AIR
AIR & CO
Light Sensor
Filtered = CO
Optical Filter
@ 4.24 µm
Figure 2-9 etCO
2
Heated "windows"
Prism
2
Light Sensor
(Normal)
Sensing Process Functional Block Diagram
2
The etCO2 pod non-invasively monitors end-tidal CO2 using a technique
that relies on the selective absorption properties of the CO
to specific
2
frequencies of infra-red radiation. See Figure 2-9.
In the sensor a thick film infra-red source is pulsed at a rate of
approximately 87 Hz, generating a broad- band spectrum of IR. Selective
filtering separates this into two narrow regions, one inside and one outside
the band of CO
the band of CO
energy since the signal it receives is not affected by CO
baseline which serves as a Reference for the level of CO
absorption. The detector associated with the filter outside
2
absorption records the maximum level of the source
2
. It provides a
2
in the airway.
2
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 21
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 32

SC 6002XL Patient Monitor Field Service Manual
Level
Detector
Eliminator
Switch
ON/OFF
Logic
Battery
V Bus
Regulator
5V
Flyback Converter
Battery Charger
Logic
12V
8V
42V
AC Power
Adapter
From CPS
or IDS
2-Pin Power
Connector
Docking
Station
SC6000P/6002/5000
Figure 2-10Power System Block Diagram
The other detector senses a filtered energy level modified by the presence
of CO
. As the level of CO2 increases, the CO2 gas molecules in the airway
2
absorb more of the light energy and less signal reaches the detector. This
signal, converted by the detector, is referred to as the Data signal. Current
through the thick-film source is bidirectional to offset the tendency of
particles within the source to migrate when exposed to a strong
unidirectional electric field caused by current flow only in one direction.
This keeps the structure of the source uniform and enhances system
integrity and life of the product.
To acquire a precise level of CO
sampled and the level of CO
, both channels are simultaneously
2
is determined from the ratio of the Data and
2
the Reference channels. The ratio is compared to a look-up table in
memory to establish the correct value in units of mmHg.
6.1 Power Supply System
The pod then sends the results to the PodCom input of the SC 6002XL for
further processing and display.
The monitor can be powered from any of several sources --
• A lead-acid or lithium-ion battery, housed in the monitor
• A CPS (Communication/Power Supply), through a docking station,
•An IDS (I
NFINITY
Docking Station)
• An AC power adapter
As illustrated in Figure 2-10, the ac power adapter and the CPS/IDS are
connected in parallel. The monitor is normally powered by a CPS via a
docking station, or an IDS, in a “pick-and-go” application, and by the ac
power adapter in a stand-alone application. If both supplies were to be
connected simultaneously the one with a higher voltage would take over.
Two solid state switches, the eliminator switch and the battery switch,
govern supply of power to the monitor and charging of the battery. In
addition, there are three DC/DC converters, two buck regulators that
produce the main +5V and +3.3V, and a multi-output flyback supply that
generates three auxiliary voltages, including the voltage that is used to
charge the battery.
On/Off logic circuitry manages the condition of the switches and the DC/
DC converters under different circumstances, and responds to the On/Off
pushbutton on the monitor front panel. The logic is implemented in the
microcontroller.
22 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 33

Field Service Manual SC 6002XL Patient Monitor
6.1.1 Main Battery A lead-acid main battery should sustain autonomous operation of the monitor for approximately 75 minutes. A lithium-ion main battery should sustain autonomous operation of the monitor for approximately 180 minutes. When the battery eliminator is connected, power to the load and charging power for the battery is provided from the AC mains.
To be fully charged, lead-acid batteries require a voltage of approximately
2.45 V/cell at 25°C (14.7 V in SC 6002XL monitors). This voltage should not
be sustained after full charge has been reached, however, because the
battery starts to outgas which reduces its life. Therefore, voltage to the
battery must be reduced to 2.30 V/cell at 25°C. This is known as the “float”
voltage. At this voltage the battery can remain indefinitely connected to the
monitor, ready to deliver current when necessary. The charging circuitry in
the SC 6002XL automatically varies the charging cycle. Lithium-ion
batteries require a constant charging voltage. See Section 3.5 above.
6.1.2 AC Power Adapter The ac power adapter is a regulated 12V (nominal) supply with enough current capability to supply the load and charge the battery at the same time. The eliminator switch (see Figure 2-10) is turned ON when the input voltage exceeds 11.25 V, allowing the ac power adapter to feed the rest of the monitor circuitry. The battery is charged from the output of the flyback supply through a regulating FET and a low-value sense resistor.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 23
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 34

Field Service Manual SC 6002XL Patient Monitor
This page intentionally left blank.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 24
6k2XLSMC2.cd-rom.fm/06-00/kaupp
Page 35

Chapter 3: Subassembly Replacement Procedures
1Introduction
2 Safety Precautions
This chapter describes how to replace hardware that Siemens has
identified as field-replaceable in an SC 6000XL Patient Monitor. Siemens
recommends use of a small common-blade screwdriver such as Stanley
64-846 or equivalent, for removing side panels and opening the monitor.
Individual field-replaceable parts and subassemblies can be replaced using
only the small common-blade screwdriver or Siemens side-panel removal
tool (Art. No. 47 24 667 E533U), and a small Phillips-head screwdriver.
Disconnect all external power, and remove the battery cover and
battery before opening the monitor.
Caution
• Failure to remove the battery before opening the monitor may
result in damage to the Main Board.
• SC 6002XL monitors contain electronic components that can be
damaged by electrostatic discharge. Open the monitor
case only in a static-protected environment. Observe
3
• Open monitor only in a dust-free environment. This is
particularly important when replacing subassemblies or
components in the Front Panel Subassembly.
standard procedures for protecting the equipment from
static electricity.
3 Service Policy and
Replaceable Parts
Qualified service personnel may replace the following specific items in the
field. Component-level repairs should not be attempted, and void any
warranty or exchange allowance for returned subassemblies. Siemens
recommends a full functional verification following replacement of
any internal subassembly in the Monitor. Refer to Appendix A for
Replacement part numbers.
• Battery Door and Main Battery (see User’s Guide)
• Rotary Knob
•Foot Pads
• Backlights
•Speaker
• Optical Encoder
• Main Processor Subassembly
• Monitor Handle
• TFT-LCD Display
• Front Panel PC Board
• Inverter PC Board
•PodCom PC Board
• Intermediate Subassembly
• Side Panels
• NBP Pneumatic Assy
• NBP Air Filters
• Battery Connector Subassembly
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 25
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 36

SC 6002XL Patient Monitor Field Service Manual
4 Non-Invasive
Replacement
Procedures
4.1 Replacing Rotary Knob
4.2 Replacing Foot Pads
Only the Battery, Battery Compartment Door, Rotary Knob, and Foot Pads
can be replaced without requiring the monitor to be opened. Refer to any
User Guide for the SC6002XL Patient Monitor for the procedure to replace
the battery or battery compartment door.
The rotary knob is press fitted onto the metal shaft of the optical encoder
subassembly, and can be reinstalled if carefully removed. If damaged
during removal, it must be replaced.
To remove the knob, grip it very firmly with vise-grip pliers or a similar tool,
and pull it straight out and off of the metal shaft of the optical encoder.
Avoid turning the knob in the process.
Note: Placing a small piece of soft cloth on the knob before gripping
it with vise-grip pliers can help protect the knob.
To install a new knob (or reinstall a knob), firmly press knob onto the shaft.
Two feet are on the bottom of the Front Bezel Subassembly, and two are
on the bottom of the rear housing. The pads are secured in foot wells with
adhesive. Replace the pads as follows:
1. Remove all remnants of existing pad and adhesive from foot well.
2. Remove protective covering from adhesive surface of replacement
pad.
3. Position replacement pad in foot well, and press firmly on pad to
secure it in well.
5 Accessing
Replaceable
Subassemblies
To view the process,
click on the picture.
In order to access replaceable subassemblies, the monitor must be
opened. First remove the battery compartment cover and battery, and set
safely aside. Then remove the left and right side panels in order to enable
removal of the Front Bezel and opening the monitor.
E:\rtbtnpnlrmvl.avi
Figure 3-1 Right Side Panel Removal
5.1 Removing Side Panels
26 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
The Right and Left Side Panels are secured to the rear housing by locking
tabs and a latching tab. Complete the following steps to remove side panels.
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 37

Field Service Manual SC 6002XL Patient Monitor
5.1.1 Removing Right-Hand Side Panel
1. Remove and save ejection shaft cover, using either a or b to remove
ejection shaft cover, before attempting to remove Right Side Panel.
See Figure 3-1.
a) Insert PCMCIA card into the slot to make ejection button accessible
b) Insert pointed end of small screwdriver between cover and side
panel, as shown in Figure 3-2, and pry cover out of hole.
2. Carefully rock cover off of ejection shaft using back and forth motion.
Caution
Pulling on the cover with excessive force can pull the shaft
completely out of the ejector mechanism, requiring depot
repair of the monitor.
3. Set cover aside, remove PCMCIA card (if used), push shaft back into
monitor, and go to Section 5.1.1.
4. Turn monitor left side down on a clean flat surface.
5. Carefully insert small screwdriver into ejection button opening on
panel, at a shallow angle as shown in Figure 3-1, and use tool as a
lever to lift side of panel approximately 1/8” (3mm). Do not angle
tool toward memory card slot.
Note:This lifts the locking tab out of its slot in the monitor housing,
permitting the panel to move.
6. With side of panel lifted, carefully slide panel in direction shown, to
release locking tabs from slots and remove panel.
aaaa
ssss
Figure 3-2 Removing Left Side Panel
5.1.2 Removing Left Side Panel 1. Carefully insert screwdriver or side-panel removal tool into MultiMed connector opening (a in Figure 3-2), at a shallow angle as shown. Use tool as a lever to lift side of panel approximately 1/8” (3mm) at s in
Figure 3-2. This releases panel latch.
2. With side of panel lifted, carefully slide panel in direction illustrated by
heavy arrow, to release locking tabs from slots and remove panel.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 27
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 38

SC 6002XL Patient Monitor Field Service Manual
5.1.3 Reinstalling Side Panels 1. For each side panel, position planel so that locking tabs and latching tabs are aligned with appropriate slots in rear housing.
2. Press into housing with a slight upward motion, in direction opposite
to that indicated in Figure 3-1 or Figure 3-2, until panel seats properly
and clicks into place.
3. Press ejection shaft cover onto ejection shaft on Right Side Panel.
Note: Cover can be properly installed in only one orientation (so that
slot in cover is toward back of Monitor) and installs easily when
properly oriented.
5.2 Front Bezel Removal
aaaa
Figure 3-3 Bezel Retaining Screws
1. After removing battery compartment cover and battery, remove and
save side panels (refer to Section 5.1).
2. Remove and save two bezel retaining screws in upper corners of
Intermediate Subassembly frame (a in Figure 3-3) and one in bottom
center of bezel (s in Figure 3-3).
ssss
ssss
To view the process,
click on the picture.
E:\bezelopen.avi
aaaa
Figure 3-4 Front Bezel Removal
28 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 39

Field Service Manual SC 6002XL Patient Monitor
3. Carefully insert flat blade of Siemens Side Panel Removal Tool into
rear slot of Front Bezel Subassembly as shown in Figure 3-4, and
apply pressure away from monitor to depress internal locking tab and
partially release bezel.
4. Repeat step 3 to depress remaining three tabs, working in a counterclockwise fashion, and carefully separate Front Bezel Subassembly
from rear housing subassembly.
5. Place monitor backside down, with bottom of monitor facing you, and
carefully lift left side of Front Bezel Subassembly up from rear housing
subassembly. Refer to Figure 3-4.
6. Unplug optical encoder connector from connector on Front Panel PC
Board.
7. Unplug flat cable from connector on Front Panel PC Board.
8. Do either a or b below, as appropriate.
a) If removing Front Bezel Subassembly only to replace Optical
Encoder Subassembly, set rest of monitor safely aside and go to
Section 5.3.
b) If removing Front Bezel Subassembly to access other sub-
assemblies in monitor set Front Bezel Subassembly safely aside
and go on to appropriate Section.
5.3 Replacing Optical Encoder Subassembly
1. Remove rotary knob, a in Figure 3-5, (see Section 4.1) and then
separate Front Bezel Subassembly from rear housing (Section 5.2.
2. Unscrew securing nut on front bezel (s in Figure 3-5 on page 29) to
free Optical Encoder Subassembly (d in Figure 3-5) from Front Panel
Subassembly and remove optical encoder from back of front panel.
3. Position new Optical Encoder Subassembly in front bezel, oriented as
illustrated in Figure 3-5, and secure subassembly to bezel.
Note: Keyed washer (f in Figure 3-5) assures proper orientation of
Optical Encoder Subassembly in Front Panel Subassembly, and
prevents turning of the optical encoder when rotary knob is turned in
normal operations. Be sure to reinstall lock washer (g in Figure 3-5).
ffff
gggg
dddd
ssss
aaaa
Figure 3-5 Optical Encoder Subassembly
4. Orient knob properly with flat area on shaft of optical encoder, and
press knob firmly onto shaft.
5. Reinstall Front Bezel Subassembly on monitor. Refer to Section 5.4.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 29
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 40

SC 6002XL Patient Monitor Field Service Manual
5.4 Front Bezel Installation
To view the process,
click on the picture.
1. Place monitor on a clean flat surface so that face (TFT-LCD display) of
monitor is up and bottom side of monitor (feet side) is positioned in
front of you.
2. Reverse procedure of Section 5.2 to reinstall Front Bezel
Subassembly. Press front bezel and rear housing together to assure
four locking tabs on sides of front bezel lock into place in Intermediate
Subassembly.
3. Reinstall and tighten screws removed in step 2 of Section 5.2 above.
4. Reinstall Side Panels (see Section 5.1.3), battery, and battery
compartment cover.
5. Functionally verify proper operation of Monitor. Refer to “Chapter 4:
Functional Verification and Calibration” on page 47.
ssss
aaaa
5.5 Removing/Installing TFT-LCD Subassembly
5.5.1 Removing TFT-LCD
Subassembly
E:\TFT_LCDasyremvl.avi
dddd
ffff
Figure 3-6 TFT-LCD Display Subassembly
1. After removing Front Bezel Subassembly (see Section 5.2), remove
and set aside TFT-LCD Display Subassembly screws as shown in
Figure 3-6.
Note: Note screw sizes and types so that they can be reinstalled in
same locations when reassembling monitor.
2. Insert flat blade of removal tool into PC board latch and lift slightly up on
board and metal plate to release from latch, as shown.
3. Gently lift metal plate and Front Panel PC Board to unplug Front Panel
PC Board connector from P
installed) and Front Panel PC Board interface connector from
Intermediate Subassembly.
ODPORT
PC Board connector (if Option
4. Unplug speaker cable from Front Panel PC Board.
5. Remove TFT-LCD Display Subassembly from monitor chassis and
place face down on clean flat surface in static-protected environment.
30 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 41

Field Service Manual SC 6002XL Patient Monitor
dddd
5.5.2 Installing TFT-LCD Display Subassembly
1. Reverse procedure of Section 5.5.1 to install TFT-LCD Display
Subassembly.
Note: If installing a new TFT-LCD display, remove protective film
from TFT-LCD display screen prior to installing Front Bezel.
2. Refer to Section 5.4 to reinstall Front Bezel Subassembly and
reassemble monitor.
ssss
gggg
aaaa
aaaa
ffff
ssss
hhhh
5.6 Speaker Replacement.
Figure 3-7 Speaker Subasssembly Connector
1. After removing TFT-LCD Display Subassembly (refer to Section 5.5)
remove and save screw (s in Figure 3-7 on page 31).
2. Lift Speaker Subassembly out of positioning well.
3. To install new Speaker Subassembly, locate speaker in positioning
well in Intermediate Subassembly, and then reinstall screw saved in
step 1.
4. Refer to procedure of Section 5.5.2 to reinstall TFT-LCD Subassembly
and reassemble monitor.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 31
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 42

SC 6002XL Patient Monitor Field Service Manual
Figure 3-8 TFT-LCD Display Subassembly (Back View)
5.7 Front Panel PC Board Replacement
Removing Front Panel PC
Board
1. Remove TFT-LCD Display Subassembly from monitor chassis (refer to
Section 5.5).
~
h
hh
ggggffff ffff
aaaa ssssddddjjjjh
2. With back of TFT-LCD display facing up as shown in Figure 3-8,
3. Remove securing screw (h in Figure 3-8) and lift Front Panel PC
Installing Front Panel PC
Board
4. Complete steps 1- 4 above in reverse order to install Front Panel PC
5. Refer to Section 5.5.2 to reinstall TFT-LCD Display Subassembly and
5.8 Inverter Board Replacement
Removing Inverter Board 1. Remove Front Bezel Subassembly (see Section 5.2) and TFT-LCD
2. With back of TFT-LCD display facing up as shown in Figure 3-8,
3. Remove two screws (f in Figure 3-8), and lift Inverter PC Board (g in
Installing Inverter Board 4. Complete steps 1-3 above in reverse order to install Inverter PC Board
5. Refer to Section 5.5.2 to reinstall TFT-LCD Display Subassembly and
unplug front panel board cable from connector from X3 (d).
board (j in Figure 3-8) off of TFT-LCD Display Subassembly.
Board and reassemble TFT-LCD Display Subassembly.
reassemble monitor.
Subassembly (see Section 5.5) from monitor chassis.
unplug backlight cable connectors from X1 and X2 (a and s in Figure
3-8), and front panel board cable from connector from X3 (d in Figure
3-8)).
Figure 3-8) off of TFT-LCD Display Subassembly.
and reassemble TFT-LCD Display Subassembly.
reassemble monitor.
32 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 43

Field Service Manual SC 6002XL Patient Monitor
5.9 TFT-LCD Display Backlight Replacement
Removing Backlights 1. After removing TFT-LCD Display Subassembly from monitor (refer to
a
ssssaaa
dddd
ffff
Figure 3-9 Backlight Retaining Tabs Location
Always replace both backlights, even though only one may be defective,
to assure even lighting of the display screen.
Section 5.5), and with back of TFT-LCD display facing up as shown in
Figure 3-8, unplug cable connectors from X1 and X2 (a and s in
Figure 3-8 and Figure 3-9).
2. Depress each black plastic retaining tab, d and f in Figure 3-9, and
extract corresponding backlight from TFT-LCD display guide slot in
direction indicated by heavy arrows in Figure.
Installing Backlights 3. Slide new backlights into TFT-LCD display guide slots until retaining
tabs snap into position.
4. Plug backlight cables into X1 and X2 (a and s in Figure 3-8 and
Figure 3-9).
5. Reverse steps of Section 5.5.2 to reinstall TFT-LCD Display
Subassembly and reassemble monitor.
5.10 PODPORT PC Board Removal/Installation
The following is a procedure for removal/installation of a PODP
Board without requiring that the TFT-LCD Display Subassembly be
removed from the Monitor. If installing the P
that did not have the option previously installed, slide the insert out of the
P
5.10.1 Removing P
Board
ODPORT
PC
ODPORT
discard before attempting to install the P
1. After removing Front Bezel (refer to Section 5.2), place monitor
connector channel in left side of Intermediate Subassembly and
backside down on clean flat surface.
ODPORT
ODPORT
ORT
Option into a monitor
connector sleeve.
PC
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 33
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 44

SC 6002XL Patient Monitor Field Service Manual
aaaa
To view the process,
click on the picture.
E:\pdprtpcbremvl.avi
ssss
aaaa
Figure 3-10 Removing PODP
2. Carefully insert side panel removal tool between port sleeve and
chassis, as shown in Figure 3-10.
Note: This releases latching tab on the bottom of sleeve, enabling
sleeve to slide up and out of side of Intermediate Subassembly.
3. Apply upward pressure on sleeve to slide sleeve off of P
connector and out of opening in side of Intermediate Subassembly.
Note: When sliding port sleeve onto P
reassembly, be sure that tab on bottom of sleeve engages
Intermediate Subassembly frame to lock sleeve into place.
ORT
PC Board
ODPORT
ODPORT
connector during
4. Remove and save screws as shown in Figure 3-10.
5. Depress Front Panel PC Board securing tab, using side-panel removal
tool, and gently lift up simultaneously on metal plate and circuit board
to free board from latch and to unplug Front Panel PC Board
connector from connector on P
6. Lift and slide P
5.10.2 Installing P
Board
34 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
ODPORT
PC
1. With Front Bezel removed (refer to Section 5.2), and monitor backside
down on clean flat surface, remove screws as shown in Figure 3-10 (if
not already removed) to free Front Panel PC Board and metal plate.
2. Depress Front Panel PC Board securing tab, using side-panel removal
tool, and gently lift up simultaneously on metal plate and circuit board
) to free circuit board from retaining clip.
3. Locate P
Subassembly.
4. Carefully align Front Panel PC Board connector into connector on
P
ODPORT
Board to secure board under latching tab.
5. Slide P
Interface Subassembly.
ODPORT
ODPORT
ODPORT
PC Board, and press on metal plate and Front Panel PC
connector sleeve into access slot in left side of
PC Board out of Monitor.
PC board on positioning posts on Intermediate
ODPORT
PC Board.
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 45

Field Service Manual SC 6002XL Patient Monitor
6. Reinstall screws removed in step 4 of Section 5.10.1 above.
7. Refer to Section 5.5.2 to reinstall TFT-LCD Display Subassembly and
reassemble monitor.
To view the process,
click on the picture.
E:\intasyremvl.avi
5.11 Replacing Intermediate Subassembly
5.11.1 Removing Intermediate
Subssembly
aaaa
Figure 3-11 Removing Intermediate Subassembly
The Intermediate Subassembly constitutes a framework for positioning
the TFT-LCD Displaly Subassembly, and shields the Front Panel
Subassembly and associated circuitry from the Main Processor, While the
Intermediate Subassembly needs to be removed to access components of
the rear housing, normally the subassembly should need to be replaced
only if it becomes physically damaged.
1. After removing TFT-LCD Display Subassembly (see Section 5.5) and
P
ODPORT
clean flat surface (open side up).
2. Remove 6 screws and save for use in reinstallation. See Figure 3-11.
Note: Screws are of different sizes. Identify screws removed so that
each can be reinserted into the same position during reassembly.
3. Insert blade of side-panel removal tool into four slots in sides of rear
housing to release latches that secure intermediate subassembly in
rear housing.
4. Apply firm pressure between rear housing and external flange on
Intermediate Subassembly to separate subassembly from housing.
PCB, place rear housing subassembly back side down on a
5. Place Intermediate Subassembly safely aside for use in reassembly.
5.11.2 Installing Intermediate Subssembly
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 35
6kXLSMC3.CD-ROM.fm/06-00/kaupp
1. Place rear subassembly on a clean flat surface so that the Main
Processor Subassembly is facing up.
2. Reverse procedure of Section 5.11.1 to install Intermediate
Subassembly.
Page 46

SC 6002XL Patient Monitor Field Service Manual
5.12 Replacing Main Processor Subassembly
5.12.1 Removing Main Processor Subassembly
The main processor PC board is sandwiched between metal shields and a
heat sink, which altogether constitute the Main Processor Subassembly.
aaaa
Figure 3-12 Securing Screw Access Cover
1. With Intermediate Subassembly removed from rear housing (refer to
Section 5.11), remove and save screw (located in back of battery
compartment under label, a in Figure 3-12) that secures Main
Processor Subassembly in rear housing.
To view the process,
click on the picture.
2. Place rear housing normal side down with its open side facing you, as
shown in Figure 3-13.
3. Carefully pull NBP tubing off of port on NBP transducer on main
processor board as shown in Figure 3-13.
aaaa
aaaa
E:\mainbdremvl.avi
Figure 3-13 Accessing Main Processor Subassembly
4. Carefully separate Main Processor Subassembly from rear housing on
left side as shown, and then lift plastic funnel off of subassembly and
store for future reinstallation.
36 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 47

Field Service Manual SC 6002XL Patient Monitor
Note: The memory card ejector shaft (d in Figure 3-13) must be
pushed in all the way when removing the Main Processor
Subassembly from the rear housing.
5. Reach behind subassembly and carefully pull NBP tubing all the way
back through hole in main processor board.
6. Unplug ground connector (a in Figure 3-14) above hole through
which NBP tubing was removed), to permit better access to cable
connectors plugged into main processor board.
7. As carefully as you can in the limited area of access, unplug red/black/
white main power cable connector (s in Figure 3-14), 2-wire black/
white NBP engine pump cable in 3-pin connector (d in Figure 3-14) ,
4-wire black/white/black/white valves cable in 4-pin connector (f in
Figure 3-14), and 4-wire red/orange/yellow/black ID chip cable in 5-pin
connector (g in Figure 3-14) from main processor board.
8. Separate Main Processor Subassembly out of rear housing and set
aside in static protected environment.
hhhh
aaaa
aaaa
dddd
5.12.2 Installing Main Processor Subassembly
ffff
aaaa
gggg
W
B
ssss
Figure 3-14 Connector Locations on Main Processor Subassembly
1. With monitor positioned as in Figure 3-13, as carefully as you can in
limited area of access, plug in red/black/white main power cable
connector.
Caution
Observe proper polarity to avoid damage to the Main board.
Refer to Figure 3-14. Orient the connector so that the red
wire plugs into and the black wire into .
R
R
B
2. Then plug in following cables into main processor PC board
connectors in sequence listed. Refer to Figure 3-14.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 37
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 48

SC 6002XL Patient Monitor Field Service Manual
a) 4-wire red/orange/yellow/black ID chip cable in 5-pin connector (g)
b) 4-wire black/white/black/white valves cable in 4-pin connector (f)
c) 2-wire black/white NBP engine pump cable in 3-pin connector (d)
d) ground cable connector into terminal lug (a) above hole for NBP
tubing
3. Dress cables through cable restraint on back of Main Processor
Subassembly.
4. Route NBP tubing through hole provided in main processor board (h
in Figure 3-14).
5. Install funnel on top of Main Processor Subassembly so that
positioning flanges are inside spacers on metal shield on main
processor board, and channel is fully seated in channel guide along
top of both metal shields.
6. Tuck ferrite on power cable into cavity in lower right back of rear
housing. (See d in Figure 3-20 on page 43.
7. Carefully position Main Processor Subassembly in rear housing.
Note: When properly positioned, by funnel and shield around Docking
Station Connector, Main Processor Subassembly slides easily into
rear housing.
Do not try to force Subassembly into housing
.
8. Pull gently on air hose to take up any slack and connect end of hose to
transducer on main processor board.
9. Holding Processor Subassembly firmly in position in rear housing, turn
housing over and secure subassembly to housing using screw
removed in step 1 of Section 5.12.1.
10. Install replacement label over securing screw in battery compartment.
Note: Installation of a replacement Main Processor Subassembly
requires that the hardware revision number stored in EEPROM in the
monitor be corrected. Refer to Section 5.17 for the procedure.
11. Refer to Section 5.11.2 to install Intermediate Subassembly and
reassemble Monitor.
5.13 Monitor Handle
5.13.1 Removing Handle Remove the handle as follows:
1. With Main Processor Subassembly removed from rear housing, place
housing backside down on clean flat surface. See Figure 3-15
2. Insert common-blade screwdriver or flat end of side panel removal
tool sequentially into each of two slots, d and f in Figure 3-15, as
you apply a slight downward pressure on handle (see arrow).
Note: This releases the locking tabs on the bottom of the plate, and
pressure on the handle lifts and holds up bottom edge of plate.
3. Using your fingers, lift up bottom edge of plate enough to fully release
locking tabs.
4. Pull on retainer plate to draw tabs on top of plate out of handle shaft
holes in top of rear housing and remove it.
5. Pull handle out through top of housing.
38 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 49

Field Service Manual SC 6002XL Patient Monitor
aaaa
ssss
ffff
dddd
To view the process,
click on the picture.
Figure 3-15 Removing Handle retaining Plate
5.13.2 Installing Handle 1. Insert handle through slots in top of housing, so that smooth sides of handle shafts ride on channels in housing (rectangular locking pads on shafts should be visible).
2. Route cables from ID chip and from NBP subassembly through slot
provided beside bottom right-hand locking tab in retainer plate.
E:\hndlretpltremvl.avi
3. Route main processor board transducer air hose from NBP subassembly through slot provided at bottom of retainer plate .
4. Slide plate’s top tabs into handle shaft holes on top of handle shafts
and press bottom tabs into slots in rear housing to lock plate in
position.
Note: Tilt the handle slightly to permit the plate’s top tabs to be
inserted easily.
5. Refer to Section 5.12.2 to reinstall Main Processor Subassembly and
reassemble monitor.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 39
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 50

SC 6002XL Patient Monitor Field Service Manual
dddd
aaaa
E:\nbpasyremvl.avi
To view the process,
click on the picture.
ffff
ssss
Figure 3-16 Location of NBP Subassembly in Rear Housing
5.14 Replacing NBP Subassembly
5.14.1 Removing NBP
Subassembly
5.14.2 Installing NBP Subassembly 1. Dress pneumatic tubing of NBP subassembly as shown in Figure
Replacing the NBP subassembly invalidates pneumatic tolerance values
previously stored. Replacing this subassembly, therefore, involves the
following steps:
a) Replace NBP Subassembly, and reassemble monitor.
b) Check for leaks in pneumatic system
c) Calibrate NBP Function in Monitor
d) Characterize pneumatic tolerances
Refer to Figure 3-16. Remove NBP Subassembly as follows:
1. Remove Main Processor Board Subassembly (refer to Section 5.12.1).
and handle-retaining plate (Section 5.13.1).
2. Slide air intake filter out of its retaining slot in top of battery
compartment in rear housing.
3. Slip NBP air hose off of metal cuff connector.
4. Slide NBP Subassembly partially out of its cavity in rear housing, and
unplug ID chip ground connector.
5. Slide NBP Subassembly completely out of rear housing.
Figure 3-18 on page 42, and slide subassembly into guide channels in
NBP cavity of rear housing.
Note: Route transducer hose behind cuff connector hose and then
through hole in lower section of assembly so that the hose exits
under manifold subassembly as in Figure 3-16. Position air intake
hose beside cuff connector hose. Ensure all hoses are not
constricted or pinched when sliding NBP Subassembly into place in
cavity in rear housing.
2. Partially slide NBP subassembly into guide channels in rear housing,
and reconnect ID chip ground wire to ground connector on NBP
Subassembly.
40 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 51

Field Service Manual SC 6002XL Patient Monitor
3. Be sure wires of pump and valve cables are not trapped behind or
under NBP subssembly guides, and seat NBP Subassembly
completely into NBP cavity in rear housing.
4. Secure NBP air hose onto metal cuff connector in side of rear
housing.
5. Slide air intake filter into retaining slot in top of battery compartment
of rear housing.
6. Route transducer hose through access slot in bottom of handle
retainer plate.
7. Dress cables from I/O chip, NBP and ground cable through slot
provided in retainer plate and reinstall plate (see step 4 in Section
5.13.2).
8. Refer to Section 5.12.2 to reinstall Main Processor Subassembly and
reassemble monitor.
5.15 Replacing NBP Air Filters
There are two NBP air filters -- an air intake filter (s in Figure 3-16 and in
Figure 3-18, also see a in Figure 3-17), and a manifold filter (a in Figure
3-18). The first is accessible from the top of the battery compartment; and
does not require that the monitor be opened. The second is located in the
manifold subassembly itself.
aaaa
Figure 3-17 NBP Air Intake Filter Access
5.15.1 Replacing Air Intake Filter 1. Open battery compartment door and remove battery.
2. Remove plastic cap covering air intake filter (a in Figure 3-17) through
opening in top of battery compartment as shown in Figure 3-17.
3. Remove filter with a pair of needle-nose pliers.
4. Fully insert new filter into filter housing, open end first, and replace
cap.
Note: NBP filters have an opening in one end. The end with the
opening must be inserted into the filter housing for the filter to
function properly.
5. Reinstall battery and battery compartment door.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 41
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 52

SC 6002XL Patient Monitor Field Service Manual
To view the process,
click on the picture.
Figure 3-18 NBP Manifold Filter Replacement
5.15.2 Replacing Manifold Filter It is necessary to open the monitor and remove the Main Processor Subassembly to access the NBP Subassembly and replace the manifold filter. Replace the filter as follows:
Note: Replace manifold filter only if monitor fails characterization.
1. With Main Processor Subassembly removed from rear housing (see
Section 5.12.1), slide NBP Subassembly partially out of rear housing to
access manifold filter.
Note: It is not necessary to completely remove NBP Subassembly
from rear housing, as shown in Figure 3-18, if only replacing filter.
2. Remove plastic cap covering manifold filter.
E:\mnfldfltrrepl.avi
3. Remove manifold filter with a pair of needle-nose pliers as shown.
4. Fully insert new filter (see Note in step 4 above), and replace cap.
5. Reinstall NBP Subassembly. Refer to Section 5.14.2.
5.16 Replacing Battery
Connector
Subassembly
42 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
1. Open Monitor and remove Main Processor Subassembly (refer to
Section 5.12.1).
2. With battery compartment door and battery removed, disconnect
inline battery connector (s in Figure 3-19) from battery terminal
connector (a in Figure 3-19) in battery compartment.
Note: The battery terminal connector subassembly (a in Figure 3-19)
is inserted into the battery compartment from inside the rear housing,
through an opening in the back of the rear housing (g in Figure 3-19
and in s in Figure 3-20), and held in place by the spring action of two
locking tabs (d in Figure 3-19).
3. Slide a thin metal wedge, such as a small flat-blade screwdriver,
between locking tab and battery connector subassembly (see f in
Figure 3-19) on each side as you press subassembly into rear housing.
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 53

Field Service Manual SC 6002XL Patient Monitor
aaaa
dddd
ffff
gggg
Figure 3-19 Battery Connector Subassembly
ssss
ffff
ssss
dddd
Figure 3-20 Battery Connector Subassembly Access Inside Rear Housing
Note: Figure 3-19 shows right hand locking tab wedged open (f in
Figure 3-19). Pressing on the top of the subassembly keeps the right
hand locking tab unlocked while you wedge left hand tab open.
4. Remove power cable (a in Figure 3-20) from inside rear housing
assembly.
5. Insert replacement power cable (a in Figure 3-20) into rear housing
assembly, ensuring female in-line battery connector enters battery
compartment through opening in rear housing (f in Figure 3-20).
6. Position ferrite on power cable (d in Figure 3-20) into cavity in lower
right hand back of rear housing.
7. From inside of rear housing (Figure 3-20), insert battery terminal (a in
Figure 3-19) through opening in rear housing (s in Figure 3-20 and
also g in Figure 3-19).
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 43
6kXLSMC3.CD-ROM.fm/06-00/kaupp
aaaa
Page 54

SC 6002XL Patient Monitor Field Service Manual
8. Squeeze locking tabs (d in Figure 3-19) in battery compartment
together while pressing on battery connector from inside rear housing
to lock replacement battery connector subassembly in place.
9. Reinstall Main Processor Subassembly (refer to Section 5.12.2) and
reassemble monitor.
5.17 Correcting Hardware
Revision Number
Stored in Monitor
5.17.1 Windows 3.1 1. On PC/laptop computer, double-Click on Accessories window.
The terminal emulation program in a laptop or PC equipped with
Microsoft® Windows 3.1, Win95, or other equivalent terminal emulator, is
required to correct the hardware revision number stored in EEPROM in the
monitor. In addition, Diag UART cable Art. No. 47 14 346 E530U is also
required. Use the following procedure to enter the correct hardware
revision into EEPROM.
Connect diagnostic cable, CBL DIAG UART 47 14 346 E530U, into serial
port on PC/laptop. If PC/laptop is equipped with Windows 3.1, go on to
Section 5.17.1. If PC/laptop is equipped with Windows 95, go to Section
5.17.2.
2. Double-click on Terminal Icon.
3. Select Settings, and then Communications.
4. Set following parameters as given, and click on OK.
• Connector: Com X (X = PC/laptop serial port to which
diagnostic cable is attached)
• Baud: 19200
• Data bits: 8
• Stop bit: 1
• Parity: none
• Flow Control: none
• Parity Check: leave blank
• Carrier detect: leave blank
5. Press <Enter> and proceed to Section 5.17.3.
5.17.2 Windows 95 1. Select "Start" and scroll to "Programs", then "Accessories", then "Hyperterminal".
2. At "Hyperterminal" window, select "Hypertrm.exe" icon.
3. If asked to set up for modem use, select NO.
4. At "Connection Description" window, enter SC6002XL in "Name" box,
select any icon, and select OK.
5. At "Phone Number" window, "Connect using:" box pull-down menu,
select Direct to Com X (X = serial port on PC/laptop to which
diagnostic cable is attached) and click on OK.
6. At "Com X Properties" window, set following parameters and click OK.
• Bits per second: 19200
• Data bits: 8
• Parity: none
• Stop bit: 1
• Flow Control: none
7. Press <Enter> and go on to Section 5.17.3.
44 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 55

Field Service Manual SC 6002XL Patient Monitor
5.17.3 Procedure 1. Do either of the following as required:
• If monitor equipped with interface plate, plug other end of cable into
X7 on interface plate.
• If monitor mounted on docking station or I
NFINITY
Docking Station,
plug other end of cable into X3 on CPS or IDS.
2. Plug in monitor power adapter and power-up monitor.
3. After MAIN screen displays on monitor, press <Esc> on PC/laptop
keyboard.
SC6002XL SUPPORT MENU
00) Error Display 01)Event Log
02) Database Defaults 03)Real-time Clock
04) Set EEPROM H/W Rev. 05)Set NBP Constants
06) Verify NBP Constants 07)Display Service Data
Press ENTER to exit
Figure 3-21 Support Menu (Item numbers may differ in different versions
of installed software.)
4. When “Enter Password” prompt displays, type in 7412 and press
<Enter> to bring up SC6002XL SUPPORT MENU (See Figure 3-21).
5. Type in 4 and press <Enter> to select “Set EEPROM H/W Rev.”
Note: A message displays H/W Rev. presently stored in EEPROM. If
H/W Rev. indicated is same as on Rev. label located on replacement
board between RFI shield and heat sink, type N at next prompt to
exit program.
6. At “Update hardware revision (<Y>es or <N>o)” prompt, type in Y or
N as required.
7. Type in major hardware revision number (numerical part of H/W Rev.)
from label on replacement board.
8. Type in minor hardware revision letter (alphabetical part of H/W Rev.)
from label on replacement board.
9. Press <Enter> to exit program.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 45
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 56

Field Service Manual SC 6002XL Patient Monitor
This page intentionally left blank.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 46
6kXLSMC3.CD-ROM.fm/06-00/kaupp
Page 57

Chapter 4: Functional Verification and Calibration
1 Functional
Verification Tests
1.1 Power Circuits and Startup
AC Power Adapter 1. With power cord connected to a hospital-grade power source, plug ac
Power-Up Sequence 3. Press ON/OFF switch on front panel, and verify following sequence of
Complete the following Functional Verification Tests. Document test
results on a copy of the Functional Checklist in Appendix D: Functional
Verification Checklist.
The following procedures check the monitor’s power circuits, power-up
sequence, and power off indicator. Begin this procedure with monitor
turned off, main battery removed, and ac power adapter disconnected.
power adapter into monitor
2. Verify that green Battery Charger LED on front panel of monitor
illuminates.
events:
3.1) Power ON LED in ON/OFF key turns on, display illuminates and
monitor emits a brief tone.
3.2) Startup screen containing displays character changing colors as
it descends towards Siemens Logo.
3.3) Monitor emits a brief tone and screen goes blank for a few
seconds.
3.4) Pressure relief valve pulses.
3.5) Display reappears containing Siemens copyright notice, installed
software version, and message “Loading software, please wait...”.
.
Power Off Indicator 4. Press ON/OFF switch, and verify that monitor powers-down and a
Battery and Charging
Circuit
1.2 Optical Encoder
3.6) MAIN screen replaces Startup Screen after several seconds.
high pitched tone sounds for ≈ 7 seconds.
5. Disconnect external power source from monitor, and verify that
Battery Charger LED turns off.
6. Install main battery.
Note: Battery should have at least 50% charge level, as indicated by
the charge level bar graph in the display message area.
7. Press ON/OFF switch on front panel, and verify the following:
• Monitor powers-up according to normal power-up sequence of
events. (Refer to power-up sequence in step 3.)
• Battery charge level indicator appears in message field on bottom left
hand side of display.
8. Plug in ac power adapter, and verify that the Green Battery Charger
LED on front panel of monitor illuminates, screen brightness
increases, and after ≈ 14 seconds, charge level indicator disappears.
The Rotary Knob on the front panel controls an optical encoder for pointing
to and selecting fields and functions on the display.
1. After power-up sequence has completed, press Rotary Knob and
verify that fill color of New Patient NO prompt changes to white
indicating that you can now confirm value NO or change it to YES.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 47
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 58

SC 6002XL Patient Monitor Field Service Manual
2. Turn knob one notch (detent, click) in either direction, and verify that
value in NO field changes to YES. Turn knob another notch, and verify
that value changes back to NO.
3. Choose YES, and verify that New Patient prompt disappears.
1.3 TFT-LCD Display
1.4 Fixed Keys
ON/OFF Key The ON/OFF key initiates the power-on sequence if the monitor is powered
The SC6002XL display is composed of an active-matrix, 6.5 inch TFT-LCD
screen with backlite. Test the TFT-LCD display as follows:
1. Verify that backlite provides sufficient and consistent background
illumination for TFT-LCD.
2. Verify that there are ≤ 17 inoperative pixels (“stuck” ON or OFF).
The following tests verify that membrane switches on the front panel are
functioning properly, and that the signal from the key is processed by the
Front Panel Control PCB.
Note: Before beginning Key tests access Main menu. Select Monitor
Setup → Monitor Options → Speaker Volumes, and assure that
Attention Tone Volume is set to other than OFF.
off, and powers-off the monitor, initiating a brief power-off piezo alarm, if
the monitor is powered-on.
Note: This test can be omitted if the procedure in step 3 of Section
1.1 has already been performed.
1. Press and momentarily hold ON/OFF key.
2. Verify that powered state of monitor changes from ON to OFF or from
OFF to ON.
3. Set monitor to powered-on state, if monitor powered off.
Main Screen and Menu
Keys
Alarm Silence Key The Alarm Silence key silences an alarm tone for one minute.
Alarm Limits Key The Alarm Limits fixed key calls up a setup table on which upper and lower
The Main Screen key sets the display to the MAIN screen.
4. Press Menu key to display Main menu.
5. Press Main Screen key, and verify that Main menu extinguishes, and
display returns to MAIN screen.
6. Assure that HR alarm is enabled, and without any input applied to
MultiMed POD, plug MultiMed or MultiMed 6 cable into monitor.
Monitor should Alarm.
7. Press Alarm Silence key and verify that alarm ceases.
alarm limits for physiologic parameters can be assigned, and alarms and
alarm recordings can be enabled or disabled.
8. Attach patient simulator to MultiMed cable and set simulator as
follows:
• ECG = Normal Sinus
• HR = 60 beats per minute (bpm)
9. With MAIN screen displayed, press Alarm Limits fixed key.
10. Verify that Alarms Setup Table displays.
11. Set Upper HR alarm parameter to 55.
48 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 59

Field Service Manual SC 6002XL Patient Monitor
All Alarms Off Key The All Alarms Off key silences all alarms for a period of 3 minutes.
12. When alarm sounds (setup in previous step),press All Alarms Off key.
13. Verify message “All Alarms Off” appears on display.
14. Verify that after 3 minutes, alarm sounds and “All Alarms
Off”message disappears.
15. Set alarm parameter within alarm condition (Q 60).
Record Key The Record key initiates a recording when monitor is connected, either
directly or via a network, to an R50 Recorder and otherwise initiates a
stored recording.
16. Press Record key.
17. Verify “Recording Started” appears in message field.
NBP Start/Stop Key The NBP Start/Stop key initiates or terminates the inflation cycle for the
non-invasive blood pressure monitor function.
18. Press Menu key. Access Monitor Setup → Monitor Options →
Speaker Volume → Medium.
19. Press NBP Start/Stop key.
Zoom Key The Zoom key allows NBP data displayed in either large characters across
1.5 ECG/RESP
ECG/RESP Test Setup 2. Select HR parameter box and press rotary knob in to bring up ECG
20. Verify that monitor sounds a tone. (Cuff must Not be plugged into
cuff connector.)
the bottom of the SC6002XL display or in a small parameter box in the
lower right section of the display. Displaying NBP in the small parameter
box allows 3 additional parameter boxes to be available across the bottom
of the display.
21. Press Zoom key, Access Bottom Channel → All.
22. Verify that 4 parameter boxes displayed across bottom of display.
23. Access Bottom Channel → NBP.
24. Verify NBP parameter boxes across bottom of display
1. Connect either a 3-lead, 5-lead, or 6-lead ECG cable from the Patient
Simulator into the MultiMed POD.
menu.
3. Set all ECG Lead settings at default values and remaining parameters
as follows:
• Tone Source ECG
• Tone Volume Low
• Pacer Detection On
•QRS Marks On
• ECG Processing ECG1
• ECG Leads (set for type cable installed in step 1)
•Arrhythmia On
• Relearn depress knob to update Arrhythmia
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 49
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 60

SC 6002XL Patient Monitor Field Service Manual
4. Set simulator as follows:
• ECG = Normal Sinus
• HR = 80 beats per minute (bpm)
• amplitude = 1.0 mV
• RESPIRATION = Normal Rest.
• rate = 20 breaths per minute (BPM)
• ohms = 1.0
• LEAD SELECT = II/RA-LL
• BASELINE IMPEDANCE = 500
Waveforms/Digital
Readouts/Tones
Lead-Off Indicators 1. One at a time, disconnect each ECG lead from simulator.
Alarm Function This procedure also tests that the alarm function of the monitor, as
1. Verify the following:
• Waveform and HR correspond to data provided by simulator.
• Heart symbol (
complex.
• White spike present at each QRS complex.
• RESP and HR digital readout correspond to settings of simulator.
2. Vary Tone Volume setting and verify that pulse tone volume changes.
3. Set Tone Volume to OFF, and verify that pulse tone stops.
2. Verify “Lead-Off” message appears in message area, pulse tone
ceases, and *** replaces digital heart rate in HR field for each lead
removed in step 1.
3. Reconnect all leads to simulator.
applicable to all other patient parameters, is operational in the monitor.
1. In Alarm Limits Table, set HR alarm parameters as follows:
• Upper limit = 110 bpm
• Lower limit = 40 bpm
♥
) blinks and pulse tone sounds for each QRS
•Alarm = ON
2. Set simulator to HR = 120 bpm.
3. Verify that monitor responds with following Serious Alarm indications:
• HR in parameter field = 120
• HR parameter field blinks and color changes.
• Serious Alarm tone sounds.
• Message HR > 110 appears in message area at bottom of display.
4. Reset simulator to HR = 80 bpm.
5. Verify the following:
• HR parameter field returns to normal color
• HR returns to 80
• Message area continues to report cause of most recent alarm
50 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 61

Field Service Manual SC 6002XL Patient Monitor
6. Press Alarm Silence fixed key.
7. Verify that “HR > 110” ceases to be reported.
1.6 Asystole
1.7 SpO2
SpO
Switch power to simulator OFF. Verify that HR parameter field reports
ASY, “Asystole” appears in message area at bottom of display, and
monitor responds with Life-Threatening alarm.
Switch power to simulator ON.
The SC 6002XL monitors oxygen saturation (SpO2) and pulse rate using
the spectrophotometric method. SpO
software is checked on monitor
2
power-up and also periodically while the monitor is in operation.
Test Setup 1. Select SpO2 parameter box to access menu. Set parameters as
2
follows:
• Pulse Tone Source SpO
2
• Pulse Tone Volume Low
• Bargraph ON
• Averaging Normal
2. On Main Screen, highlight Channel 2 field and access menu. Set
parameters as follows:
•Curve SpO
2
• Size 20-30%
3. Apply SpO
4. Verify an SpO
sensor to finger.
2
reading of W 94 in the monitors SpO2 parameter box.
2
Note: Allow approx. 20 seconds for reading to stabilize.
Waveforms/Digital
Readouts/Tones
1.8 Temperature
1.8.1 Functional Verification Procedure
1.8.2 Temperature Calibration Check
Recommended
Equipment
1. Verify the following:
• Channel 2 displays SpO
waveform, and digital SpO2 and pulse rate
2
(PLS) values.
• Pulse strength bar graph pulses SpO
in field, ♥ symbol blinks in PLS
2
field, and pulse tone sounds for every detected pulse.
Using the Temperature Y Cable input to the MultiMed Pod, set up the
patient simulator to supply a temperature input.
Set the simulator for a standard 37°C.
1. Verify that monitor indicates temperature of 37±0.1°C.
2. Change simulator to temperature above and then below 37°C.
3. Verify that monitor readout agrees with simulator settings ±0.1°C.
4. Perform Temperature Calibration Check, if required by local
Regulatory Standards.
In some national jurisdictions temperature calibration must be checked
periodically as specified in the Operating Instructions or User Guide (at
least every two years). Use the following procedure.
Decade Resistor with ±0.1% accuracy (or fixed resistors with same
accuracy)
Siemens Temp Adapter Cable, Art. No. 51 98 333 E530U (Optional)
Procedure 1. Connect MultiMed pod to input of patient monitor.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 51
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 62

SC 6002XL Patient Monitor Field Service Manual
2. Connect temp adapter cable to MultiMed Pod (if needed).
3. Connect temperature input to decade resistor.
Table 4-1Resistance Value vs. Temperature
Resistance
Setting (Ω)
Set
Temperature
Monitor
Reading
Tolerance Pass
6990 1.0 0.9 to 1.1
3539 15.0 14.9 to 15.1
1355 37.0 36.9 to 37.1
843.2 49.0 48.9 to 49.1
4. For each resistance value in Table 4-1, verify that monitor reports “Set
Temperature” value ±0.1°C.
5. Document test results on a copy of the Functional Verification
Checklist in Appendix D.
1.9 etCO2 (if installed)
The etCO2 Pod enables the SC6002XL to non-invasively monitor end-tidal
CO
(etCO2) using a technique that relies on the selective absorption
2
properties of CO
to specific frequencies of infrared radiation. The pod
2
automatically compensates for variations in ambient barometric pressure if
set to automatic mode. Before beginning this procedure, use a mercury
column barometer or equivalent other device to determine local
atmospheric pressure. Record this value_________.
1. Press Main screen key.
2. Connect Sensor (without adapter) to etCO
pod and pod to monitor.
2
Note: Observe“etCO2 Sensor Warming Up” in message field at
bottom of monitor.
3. After “etCO2 Sensor Warming Up” disappears (approximately 2
minutes), select etCO
parameter box and in etCO2 setup menu
2
select “More”.
4. Select Atm. Press Mode - Manual.
5. Select Atm Pressure and set value as recorded above.
6. Press Main Screen key.
7. Select etCO
parameter box and in etCO2 Setup menu, select
2
“Sensor Cal.”.
8. After “etCO2 Place Sensor On Zero Cell” appears at bottom of
screen, place sensor on Zero Cell.
9. Verify “etCO2 Calibrating Sensor” appears in message field, followed
by “etCO2 Place Sensor on Ref Cell”.
10. After “etCO2 Place Sensor on Ref Cell” appears, place sensor on
Reference Cell.
11. Verify that”etCO2 Verifying Sensor Cal”, appears, then “etCO2
Sensor Cal Verified” appears simultaneously with a tone.
12. Verify reading in etCO2 parameter box = 38 ±2mmHg.
13. Remove reference cell, insert adaptor into sensor and press Main
Screen key.
52 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 63
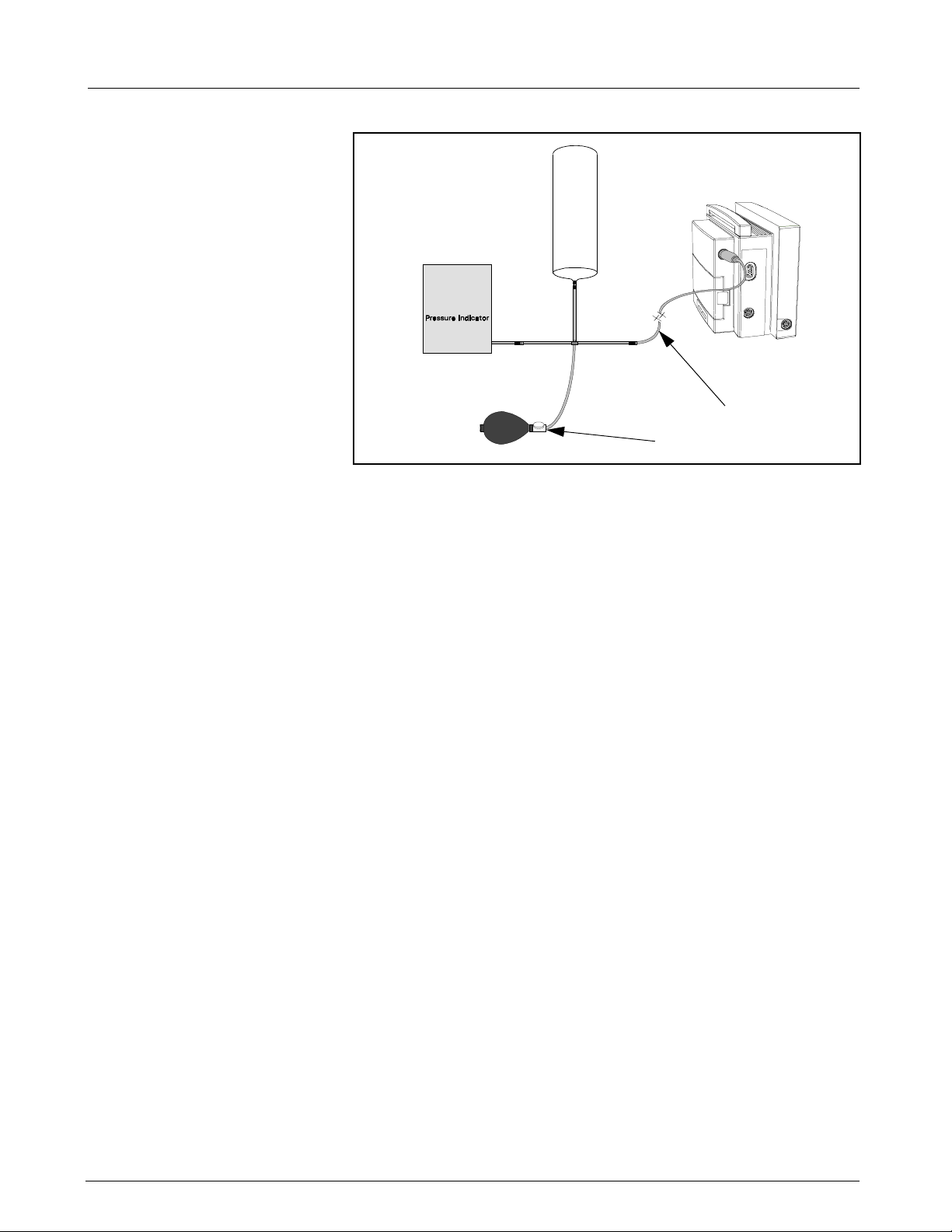
Field Service Manual SC 6002XL Patient Monitor
a
s
Figure 4-1 Test Setup
1.10 Non-Invasive Blood Pressure
1.10.1 System Setup and
Pneumatics Leakage Test
Set up NBP Calibration assembly (Art. No. 28 77 855 EE54U) as illustrated
in Figure 4-1. Assure that pneumatic leakage is within specifications before
continuing to Section 1.10.2, Calibration Check.
1. Power-up monitor.
2. After MAIN screen displays on monitor, double-click rotary knob to
accept “New Patient”.
3. Turn rotary knob until NBP field is highlighted, then depress knob.
4. Set following in NBP parameter field menu:
• Interval Mode: OFF
• Calibration Mode: ON (Observe “NBP Cuff 0 mmHg” appears in
• Inflation Mode: Adult:270
5. Clamp pneumatic hose (with hemostat or clamp) between
T-connector and monitor (
increase pressure to 250 ±5 mmHg. Then clamp hose at inflation bulb
s
(
in Figure 4-1), and let pressure stabilize for 1 minute. Do NOT run
pump.
6. Observe pressure drop for an additional 5 minutes. Drop should be
<2 mmHg in 5 minutes. If not, tighten all connections and fittings and
retest equipment for leakage. When leakage test OK, go on to step 7.
7. With both clamps removed, reinflate to 250±5 mmHg, if necessary,
and then re-clamp hose at inflation bulb.
8. Observe pressure drop for 1 minute. Drop should be <4 mmHg. If
not, service monitor’s internal pneumatics system and retest system
for leakage. When leakage test OK, remove clamp at inflation bulb
and go on to Section 1.10.2.
lower right area of NBP field
a
in Figure 4-1), and using pressure bulb,
1.10.2 Functional and Calibration Check
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 53
6kXLSMC4.cd-rom.fm/06-00/kaupp
1. Using hand bulb, increase pressure to 250 ±5 mmHg, if necessary,
and allow it to stabilize for 1 minute.
Page 64

SC 6002XL Patient Monitor Field Service Manual
2. Verify that pressure values displayed on monitor (lower left message
area) and pressure indicator are within ±3 mmHg of each other.
3. Slowly release pressure in decrements of 50 mmHg. At pressures of
200, 150, 100, and 50 mmHg, verify that pressure values on monitor
and pressure indicator are within ±3 mmHg of each other at each
level.
4. If NBP function fails calibration check, go to Section 3 and calibrate
NBP system. Then return to step 5. Otherwise, if NBP function is OK,
Set Calibration Mode to “OFF” as described in steps 3 and 4 of
Section 1.10.1 and continue.
5. Document test results on a copy of Functional Verification Checklist in
Appendix D.
1.11 Invasive Blood Pressure
IBP Test Setup 1. Connect simulator BP output to IBP input on monitor’s left side panel,
Calibration 1. Apply a static pressure of 0 mmHg from patient simulator.
1
Figure 4-2 IBP Test Setup
using adapter cable (a in Figure 4-2) Art. No. 33 68 383 E530U.
2. On MAIN Screen, select Channel 2 waveform field, and select
following on Channel 2 menu:
• Waveform - GP1
• Size - 200 mmHg
3. Return to MAIN Screen.
2. Select pressure parameter box.
3. Select “Zero” in IBP Setup window.
4. Verify that “GP1 Zero Accepted” exhibits in message field, and that a
flat pressure curve is displayed at 0 line in second waveform channel.
5. Change static pressure to 100 mmHg at patient simulator.
6. Select Manometer Cal. in IBP Setup window.
54 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 65

Field Service Manual SC 6002XL Patient Monitor
7. Set Manometer Cal. to 100.
Note: Even if Manometer Cal. reads 100, select field and reset value
to 100.
8. Verify that “GP1 Cal. Accepted” exhibits in message field
simultaneously with a tone.
9. Return to MAIN screen.
IBP Limits Alarms 1. In Alarm Limits Table select AutoSet.
2 Leakage Current
Test
10. Verify that M
100 mmHg ±2 mmHg, and that a flat pressure curve is displayed
exactly in the middle of waveform channel.
11. Increase static pressure to 200 mmHg
12. Verify that M
mmHg, and that flat pressure curve is displayed in waveform channel.
2. In Alarm Limits Table set Syst/Dia/Med Alarm to ON.
3. Set simulator to stat < 50.
4. Verify that monitor responds with following Serious Alarm indications:
•M
ean, Diastolic and Systolic values = simulator stat setting.
• GP1 parameter field changes to yellow.
• Serious Alarm tone sounds.
• Messages “GP1 Static”, “GP1 Dia <170” and “GP1 Mean
<170”blink on and off in message field.
5. In Alarm Limits Table set Sys/Dia/Med Alarm to OFF.
The SC6002XL is a battery operated device, isolated from ground by the
transformer in an ac power adapter, or grounded through the CPS or IDS
power supply, when operated from an external ac power source. Leakage
current tests assure that under both normal and fault conditions, any
leakage current does not exceed values given in Table 4-2. Use the
following general procedure to measure leakage currents.
ean, Diastolic and Systolic values displayed read
ean, Diastolic and Systolic values displayed are 200 ±2
Table 4-2 Leakage Current Tests
TEST Max. Current
Combined Lead Leakage <10µA
Individual Lead Leakage <10µA
Paired Lead Leakage <10µA
Leakage with Line Voltage on Leads <50µA
1. Perform leakage current tests on a SC6002XL series monitor with ac
power adapter (see Figure 4-3), CPS Communications/Power Supply
(see Figure 4-4), or IDS power supply (see Figure 4-5) plugged into
leakage tester.
2. Attach MutiMed cable (a in Figure 4-3, Figure 4-4, and Figure 4-5) to
Monitor.
3. Attach MutiMed cable ECG leads (s in Figure 4-3, Figure 4-4, and
Figure 4-5) to corresponding posts at Leakage Tester.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 55
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 66

SC 6002XL Patient Monitor Field Service Manual
fda
RL
LL RA LA V1
Leakage Tester
Figure 4-3 Block Diagram: Earth Leakage Current (AC/DC Power Adapter)
f
s
s
AC/DC
Power
Adapter
da
ODPORT
P
Connector
MultiMed
Connector
Patient
Monitor
ODPORT
P
Connector
MultiMed
Connector
LL RA LA V1
RL
Leakage Tester
Figure 4-4 Block Diagram: Earth Leakage Current (CPS/Docking Station)
CPS
Docking
Station
Patient
Monitor
fdas
P
ODPORT
Connector
MultiMed
Connector
LL RA LA V1
RL
Leakage Tester
IDS
Power
Supply
IDS
Docking
Station
Patient
Monitor
Figure 4-5 Block Diagram: Earth Leakage Current (I
56 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
NFINITY
Docking Station)
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 67

Field Service Manual SC 6002XL Patient Monitor
4. Follow leakage tester manufacturer’s instructions to measure each
leakage current given in Table 4-2, for each of following conditions:
• Combined Lead Leakage
• Individual Lead Leakage
• Paired Lead Leakage
• Leakage with Line Voltage on Leads
5. Verify that current does not exceed values shown in Table 4-2.
6. Document test results on a copy of Functional Verification Checklist in
Appendix D.
7. Disconnect MutiMed cable ECG leads (s in Figure 4-3, Figure 4-4,
and Figure 4-5) from corresponding posts at Leakage Tester.
8. Short together all leads to shield at end of PodCom Leakage Test
Cable (f in Figure 4-3, Figure 4-4, and Figure 4-5) and connect leads
and shield to RL post of Leakage Tester.
9. Attach Pod Com Leakage Test Cable (d in Figure 4-3, Figure 4-4, and
Figure 4-5) to SC 6002XL P
10. Follow leakage tester manufacturer’s instructions to measure each
leakage current given in Table 4-2, for each of following conditions:
ODPORT
connector.
• Individual Lead Leakage
• Leakage with Line Voltage on Leads
11. Verify that current does not exceed values shown in Table 4-2.
12. Document test results on a copy of Functional Verification Checklist in
3Calibrating NBP
System
3.1 Introduction
Table 4-3 NBP Calibration Test Equipment
Test Equipment Description
N.B. Regulations in some national jurisdictions may place specific
requirements on who may perform this procedure.
The NBP function requires external intervention for calibration of the
internal transducer and characterization of the internal pneumatics. The
calibration procedure consists of the following tasks:
Use tools listed in the table below as required, to check calibration, and
when necessary, calibrate the non-invasive pressure transducer: Note
pressure indicator required for NBP calibration.
Appendix D.
Step 1) Testing for leaks in the pneumatic system
Step 2) Calibrating the transducer
Step 3) Characterizing pneumatic tolerances (if required)
Either:
a) PC or laptop computer equipped with terminal emulation
software and serial port, or
b) terminal equipped with a serial port
e.g., Microsoft® Windows™
e.g., VT100 terminal-emulation
software package (e.g., SmartTerm)
SHP ACC CBL DIAG UART Art. No. 47 14 346 E530U
NBP Calibration Assembly Art. No. 28 77 855 EE54U
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 57
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 68

SC 6002XL Patient Monitor Field Service Manual
Table 4-3 NBP Calibration Test Equipment (Continued)
Test Equipment Description
NBP Hose Art. No. 12 75 275 EH50U
Side Panel Removal Tool Art. No. 47 24 667 E533U
Interface Plate Art. No. 33 76 493 E530U
*Dynatech cuff link or *Baumonometer
*For calibration check. For calibration, Paroscientific Pressure Meter, Model 740-12D, or equivalent,
is recommended. An equivalent must be accurate to ±0.3 mmHg from 0 to 330 mmHg.
Note: For NBP calibration, the Pressure Indicator must be accurate to ±0.3 mmHg from 0.0 mmHg to 330.0
mmHg, and must be calibrated. The calibration must be traceable to National Standards.
3.2 Calibration Procedure
Complete the following steps to calibrate the NBP system.
1. Power down monitor.
2. Disconnect monitor from docking station (if mounted).
3. Remove left side panel. Refer to Section 5.1.2 in Chapter 3:
Subassembly Replacement Procedures.
4. Assure that system has been set up and checked for leakage as
described in Section 1.10.1.
5. Connect AC power adapter (Art. No. 59 53 539 E530U or Art No. 51
88 607 E530U) and power up monitor.
6. After MAIN screen displays on monitor, double-click rotary knob to
accept “New Patient”.
7. Turn rotary knob until NBP field is highlighted, then depress knob.
8. Set following in NBP parameter field menu:
• Interval Mode: OFF
• Calibration Mode: ON (Observe “NBP Cuff 0 mmHg” appears in
• Inflation Mode: Adult:270
9. Using hand bulb, increase pressure to 260±2 mmHg.
10. Adjust calibration potentiometer (
access port in left side of monitor, until monitor (lower right area of
NBP field) and pressure indicator readings match + 1mmHg.
lower right area of NBP field)
a
in Figure 4-6 on page 59) through
Note: Siemens recommends using a small flathead jewelers
screwdriver to make potentiometer adjustments.
11. Using deflation valve on hand bulb, reduce pressure in steps to 200,
150, 100, and 50 ±5 mmHg. Allow pressure to stabilize at each level,
then verify that pressures displayed on monitor and pressure indicator
are within ±1 mmHg of each other at each level.
12. Repeat steps 10 and 11 until all pressures steps displayed on monitor
(200, 150, 100, and 50 ±5 mmHg) are within ±1 mmHg of each other
at each level.
13. Set Calibration Mode to “OFF.”
14. Power-down monitor.
15. Enter date of calibration on a copy of Functional Verification Checklist
in Appendix D.
58 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 69

Field Service Manual SC 6002XL Patient Monitor
a
Figure 4-6 Calibration Potentiometer
3.3 Characterization
Pneumatics in the monitor have tolerances that affect flow control of pump
and valves during NBP measurements. To accurately represent flow data
to NBP software, tolerances must be determined and characterized, to
allow software to compensate for variations. Tolerances are represented
as “pneumatic characterization constants” stored in EEPROM, each of
which is unique to its set of pneumatics. Characterization is required after
NBP subassembly or Main Processor Subassembly have been replaced, or
if there is a suspected problem such as difficulty in calibrating NBP. The
process for determining and storing constants is programmed into the
monitor’s software.
d
a
s
Figure 4-7 NBP Characterization Setup
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 59
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 70

SC 6002XL Patient Monitor Field Service Manual
3.3.1 Characterization Setup 1. Install Interface Plate (a in Figure 4-7), Art. No. 33 76 493 E530U, on monitor.
2. Connect diagnostic cable, CBL DIAG UART 47 14 346 E530U (
Figure 4-7), between serial port on PC/laptop and X7 on interface
plate. If PC/laptop is equipped with Windows 3.1, go to Section 3.3.2.
If PC/laptop is equipped with Windows 95, go to Section 3.3.3.
3.3.2 Windows 3.1 1. On PC/laptop computer, double-Click on Accessories window.
2. Double-click on Terminal Icon.
3. Select Settings, and then Communications.
4. Set following parameters as given, and click on OK.
• Connector: Com X (X = PC/laptop serial port to which diagnostic
cable was attached in Section 3.3.1)
• Baud: 19200
• Data bits: 8
• Stop bit: 1
• Parity: none
• Flow Control: none
• Parity Check: leave blank
• Carrier detect: leave blank
5. Press <Enter> and proceed to section 3.3.4.
s
in
3.3.3 Windows 95 1. Select "Start" and scroll to "Programs", then "Accessories", then "Hyperterminal".
2. At "Hyperterminal" window, select "Hypertrm.exe" icon.
3. If asked to set up for modem use, select NO.
4. At "Connection Description" window, enter SC6002XL in "Name" box,
select any icon, and select OK.
5. At "Phone Number" window, "Connect using:" box pull-down menu,
select Direct to Com X (X = serial port on PC/laptop to which
diagnostic cable was attached in Section 3.3.1) and click on OK.
6. At "Com X Properties" window, set following parameters and click OK.
• Bits per second: 19200
• Data bits: 8
• Parity: none
• Stop bit: 1
• Flow Control: none
7. Press <Enter> and proceed to 3.3.4.
3.3.4 Complete Characterization 1. Plug in monitor power adapter and power-up monitor.
2. After MAIN screen displays on monitor, press <Esc> on PC/laptop
keyboard.
60 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 71

Field Service Manual SC 6002XL Patient Monitor
SC6002XL SUPPORT MENU
00) Error Display 01)Event Log
02) Database Defaults 03)Real-time Clock
04) Set EEPROM H/W Rev. 05)Set NBP Constants
06) Verify NBP Constants 07)Display Service Data
Press ENTER to exit
Figure 4-8 Support Menu (Item numbers may differ between versions
of installed software.)
3. When “Enter Password” prompt displays, type in 7412 and press
<Enter> to bring up SC6002XL SUPPORT MENU (See Figure 4-8).
4. Type in 5 and press <Enter> to access NBP Characterization function.
Note: The item number to access the NBP function may be different
for different versions of installed software.
5. Connect half-liter standard volume to monitor (
follow instructions on terminal display.
6. After Characterization is complete (i 30 seconds), verify “Pneumatic
Characterization was SUCCESSFUL!” is displayed at PC/laptop.
Note: If the test fails because of a constant out-of-range condition,
examine NBP pneumatics and replace if out-of-range condition persists.
7. Power down monitor.
8. Document test results on a copy of Functional Verification Checklist in
Appendix D: Functional Verification Checklist.
d
in Figure 4-7) and
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 61
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 72

SC 6002XL Patient Monitor Field Service Manual
This page left intentionally blank.
62 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC4.cd-rom.fm/06-00/kaupp
Page 73

SC 6002XL Patient Monitor Field Service Manual
Chapter 5: Troubleshooting
1 Troubleshooting
1.1 Power Problems
1.1.1 No Response When
Table 5-1 Power-On Problems
POWER ON/OFF Key
Pressed
Conditions Possible Cause(s) Troubleshooting and Remedial Action
Monitor connected
directly to Power
Adapter; Battery
Power Adapter
malfunction
Monitor Malfunction
Charger LED not
illuminated*
If the Monitor should fail to respond properly to procedures prescribed in
the User Guide for the installed software version, use the procedures
below to aid in identifying and remedying the problem.
There are several possible reasons why a Monitor might not respond when
the Power ON/OFF key is pressed. Required troubleshooting procedures
depend on power sources connected to the monitor. Refer to Table 5-1.
1. Assure Power Adapter is connected to an active
hospital power source.
2. Disconnect power adapter from Monitor and
measure Power Adapter output voltage.
• If voltage = 11.6 to 13.8 VDC, continue to step 3.
• If voltage q 11.6 VDC or Q 13.8 VDC, replace Power
Adapter.
3. Replace Front Bezel.
4. If problem persists, replace Front Panel PC Board.
* AC/DC Power Adapter, Art. No. 51 88 607 E530U
does not have an LED.
Monitor on docking
station; Battery
charger LED not
illuminated
IDS Power Supply
malfunction
CPS/IDS malfunction
Monitor malfunction
11 12
5. If problem persists, replace Main Processor
Subassembly.
6. If problem persists, contact TSS in Solna or Danvers.
1. • If IDS, assure that IDS power supply is connected
to an active hospital power source.
• If CPS, assure that CPS is connected to active
hospital power source and switched ON.
NOTE:If CPS or IDS power supply LED is not
illuminated, check power source and power
cable. If O.K., replace CPS or IDS power
supply.
2. Measure voltage between pins 11 and 12 at docking
connector on docking station. (See left.)
• If voltage = 11.6 to 13.8 VDC, continue to step 3.
•If voltage q 11.6 VDC or Q 13.8 VDC, replace IDS
Power Supply or CPS.
3. Replace Front Bezel.
4. If problem persists, replace Front Panel PC Board.
5. If problem persists, replace Main Processor
Subassembly.
6. If problem persists, contact TSS in Solna or Danvers.
63 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC5.cd-rom.fm/06-00/kaupp
Page 74

SC 6002XL Patient Monitor Field Service Manual
Table 5-1 Power-On Problems (Continued)
Conditions Possible Cause(s) Troubleshooting and Remedial Action
Monitor on docking
station or directly
connected to Power
Adapter; Battery
charger LED
illuminated
NO power. Monitor
not connected to AC
Power Adapter or
docking station;
battery installed
Corrupted Software
Front Bezel malfunction
Front Panel PCB
malfunction
Main Processor
malfunction
Battery discharged or
needs to be replaced
Battery charger circuitry
malfunction
1. Press Power On key to power monitor ON.
2. Try booting with monitor software PCMCIA card
inserted into card slot.
3. If problem persists, replace Front Bezel.
4. If problem persists, replace Front Panel PC Board.
5. If problem persists, replace Main Processor
Subassembly.
6. If problem persists, contact TSS in Solna or Danvers.
1. Connect monitor to AC Power Adapter or Docking
Station.
2. When Battery charger LED illuminates, press
POWER ON/OFF key to power monitor ON and
access MAIN screen.
NOTE: If Battery charger LED fails to illuminate,
refer to section above on Condition - “Monitor
connected directly to Power Adapter; Battery
Charger LED not illuminated or “Monitor on
docking station; Battery charger LED not
illuminated”
3. Allow monitor or remain on Power Adapter or
powered Docking Station for i 1 hr. Disconnect
monitor from Power Adapter or powered Docking
Station. After i 30 sec. check battery level bar
graph, located at bottom left side of display, and
verify that a portion of the bar graph is green.
• If a portion of the bar graph is green, reconnect
monitor to Power Adapter or powered Docking
Station. Leave monitor connected an additional 4.5
hrs for Lead-acid type battery or 7 hrs for an optional
Lithium-ion type battery, then go to step 4.
• If no portion of the bar graph is green, replace
main battery, and then repeat step 3. If charge
level remains constant, go to step 5.
4. After charging the Main battery (≥4.5 hrs for Leadacid type battery or ≥7 hrs for optional
type battery) recheck battery charge level.
• If charge level = 100%, return monitor to clinical
service.
• If charge level <100% replace Main battery.
5. If problem persists with new main battery, replace
Main Processor Subassembly.
6. If problem persists, contact TSS in Solna or Danvers.
64 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC5.cd-rom.fm/06-00/kaupp
Lithium-ion
Page 75

Field Service Manual SC 6002XL Patient Monitor
1.1.2 Power On/Off Piezo Tone
Table 5-2 Power-off Alarm Malfunction
Fails to Sound.
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Piezo tone fails to
sound when monitor
powered on, if
monitor loses
power, or when
Front Panel PCB
malfunction
Main Processor
malfunction
1. Replace Front Panel PC Board
2. If problem persists, replace Main Processor
Subassembly.
3. If problem persists, contact TSS in Solna or Danvers.
monitor poweredoff.
1.1.3 Power-Up Sequence Fails to Complete Properly
Table 5-3 Power-up Process Malfunction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Power inputs all OK
but monitor fails to
complete power-up
sequence
Software program
corrupted
Main PCB malfunction
If power ON LED illuminates but monitor fails to
complete power-up sequence, reinstall software
as follows:
1. With monitor powered off, insert PCMICA card into
slot at right side of monitor.
2. Power monitor on.
3. If monitor fails to properly complete power-up
sequence, replace Main Processor Subassembly,
4. If problem persists, contact TSS in Solna or Danvers.
1.2 Optical Encoder Malfunction.
Table 5-4 Rotary Knob Malfunction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Rotary knob fails to
properly select
fields, or pressing
the knob in fails to
activate a menu or
select a default.
Front Panel PC Board
malfunction
Optical Encoder
malfunction
Main Processor
malfunction
1. Replace Front Panel PC Board.
2. If problem persists, replace optical encoder.
3. If problem persists, replace Main Processor
Subassembly.
4. If problem persists, contact TSS in Solna or Danvers.
1.3 TFT-LCD Display Malfunction.Fixed
Table 5-5 LCD Display Malfunction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
>
17 inoperative
pixels (“stuck” ON
LCD screen
malfunction
Replace TFT-LCD Display.
or OFF).
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 65
6kXLSMC5.cd-rom.fm/06-00/kaupp
Page 76

SC 6002XL Patient Monitor Field Service Manual
Table 5-5 LCD Display Malfunction (Continued)
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Areas of display
missing or color
contaminated
Backlight fails to
provide sufficient
and consistent
background
illumination for the
LCD display.
Front Panel PC Board
malfunction
Processor on Main
PCB malfunction
TFT-LCD Display
malfunction
Inverter malfunction
Front Panel PC Board
malfunction
Main Processor
malfunction
1. Replace Front Panel PC Board.
2. If problem persists, replace Main Processor
Subassembly.
3. If problem persists, contact TSS in Solna or Danvers.
1. Replace TFT-LCD Display Backlights.
2. If problem persists, replace Inverter PC Board.
3. If problem persists, replace Front Panel PC Board.
4. If problem persists, replace Main Processor
Subassembly.
5. If problem persists, contact TSS in Solna or Danvers.
1.4 Fixed Key Fails to Function.
Table 5-6 Fixed Key Malfunction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
A Fixed Key fails to
initiate change
Front Bezel
malfunction
Front Panel PC Board
malfunction
Main Processor
malfunction
1. Replace Front Bezel Subassembly.
2. If problem persists, replace Front Panel PC Board.
3. If problem persists, replace Main Processor
Subassembly.
4. If problem persists, contact TSS in Solna or Danvers.
1.5 Visual or Audible Alarm Reporting Failure.
Table 5-7 Alarm Malfunctions
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Audible Alarm O.K.,
Software problem
but Visual Alarm
Fails.
Visual Alarm O.K.,
but Audible Alarm
Fails.
Speaker malfunction
Front Panel PC Board
malfunction
Main Processor
malfunction
66 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
1. Try reinstalling software.
2. If problem persists, contact TSS in Solna or Danvers.
1. Power-cycle monitor and listen for tone after icon
appears on power-up screen (not the piezo, which
sounds before the icon appears).
2. If tone fails to sound, replace speaker.
3. If problem persists, replace Front Panel PC Board.
4. If problem persists, replace Main Processor
Subassembly.
5. If problem persists, contact TSS in Solna or Danvers.
6kXLSMC5.cd-rom.fm/06-00/kaupp
Page 77

Field Service Manual SC 6002XL Patient Monitor
1.6 NBP Malfunction
Table 5-8 NBP Malfunctions
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
NBP fails to zero
properly, fails
characterization, or
fails calibration
check
NBP pump fails to
start/stop when NBP
key on front panel is
pressed
NBP pump starts,
but cuff fails to
inflate/deflate
properly
NBP pneumatic
system malfunction
Main Processor
malfunction
Front Bezel
malfunction
Front Panel PC Board
malfunction
NBP pump
subassembly
malfunction
Main Processor
malfunction
Cuff assembly
malfunction
NBP pneumatic
system malfunction
1. If monitor fails calibration, perform characterization
procedure (see Section 3.3 in Chapter 4: Functional
Verification and Calibration).
2. If monitor fails characterization or problem
persists,replace Main Processor Subassembly.
3. If problem persists, contact TSS in Solna or Danvers.
1. If monitor reporting NBP in fault mode, or error
message displays, power-cycle monitor.
2. Otherwise, replace front bezel Subassembly.
3. If problem persists, replace Front Panel PC Board.
4. If problem persists, replace NBP Pump
Subassembly.
5. If problem persists, replace Main Processor
Subassembly.
6. If problem persists, contact TSS in Solna or Danvers.
1. Recheck cuff assembly and installation, and replace
cuff assembly if defective.
2. If problem persists, check NBP tubing in rear
housing of monitor.
3. If tubing OK, replace NBP Pump Subassembly.
4. If problem persists, contact TSS in Solna or Danvers.
1.7 etCO2 Malfunction.
Table 5-9 etCO2 Malfunctions
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Parameter box fails
to appear when
sensor plugged into
pod
Sensor fails
calibration
Persistent Adapter
Failure message
Sensor or cable
malfunction
etCO
Pod malfunction
2
PodPort PC Board
malfunction
Main Processor
malfunction
Airway adapter or
sensor window
occluded
Airway adapter
malfunction
Sensor malfunction
1. Replace etCO2 Sensor.
2. If problem persists, replace etCO
3. If problem persists, replace PodPort PC Board.
4. If problem persists, replace Main Processor
Subassembly.
5. If problem persists, contact TSS in Solna or Danvers.
1. If adapter or sensor window occluded, clean window.
2. If problem persists, replace airway adapter.
3. If problem persists, replace sensor.
4. If problem persists, replace etCO
5. If problem persists, contact TSS in Solna or Danvers.
Pod.
2
Pod.
2
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 67
6kXLSMC5.cd-rom.fm/06-00/kaupp
Page 78

SC 6002XL Patient Monitor Field Service Manual
1.8 No Printout from Recorder.
Table 5-10 Recorder Problems
Symptoms Possible Cause(s) Troubleshooting and Remedial Action
Recorder Power LED
NOT illuminated
when Record key
depressed
Interface Plate, Auxiliary
Docking Station Docking Connector
2
1
CPS Recorder CPS
2
15
Recorder malfunction
Cabling malfunction
Interface Plate (if
installed) malfunction
CPS / IDS (if installed)
malfunction
Main Processor
malfunction
Monitor Docking
Connector
12
2
15
2
15
1. Assure that all units in the power chain are properly
connected and powered ON.
2. If problem persists do either a or b. Refer to
illustrations below left.
a If Recorder has installed Interface Plate, detach
Interface Plate from Recorder, depress Record key
at monitor and check voltage between pins 1 and 2
on Interface Plate docking connector.
b If Recorder mounted on Auxiliary Docking Station,
depress Record key and check voltage between pins 1
and 2 on Auxiliary Docking Station connector.
3. If voltage O.K., replace Recorder.
4. If voltage NOT O.K., check for +12VDC between pins 1
and 2 on monitor docking connector.
• If voltage O.K., check for +12VDC between pins 1
and 2 of all docking connectors in path between
monitor and recorder, and between pins 2 and 15
of X13 on CPS or IDS. Replace component that
fails to provide 12VDC at the appropriate pins.
• If voltage not O.K. on monitor docking connector,
continue.
X13X12
Local Recorder
connected directly to
Monitor in standalone
configuration
X13 X13
Recorder malfunction
Interconnecting cable
or connection
malfunction
Recorder or Monitor
Interface Plate
malfunction
Main Processor PCB
malfunction
5. If problem persists, replace Recorder.
6. If problem persists, replace Main Processor
Subassembly
7. If problem persists, contact TSS in Solna or Danvers.
1. With an ECG waveform from patient simulator on
Monitor display, press Record key.
• If “Recording Started” followed by double-tone,
then “Recording Stored” message appears in the
message field, continue to step 2.
• If no message or recording appears, go to step 5.
2. If problem persists, and Recorder Cable Art. No. 43 18
130 E530U is installed, replace Recorder cable.
3. If problem persists, and separate Interface Plates and
Recorder cable are installed, replace each item one at
a time to isolate possible malfunction.
4. If problem persists, replace Recorder.
5. If problem persists, replace Main Processor
Subassembly
6. If problem persists, contact TSS in Solna or Danvers.
68 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC5.cd-rom.fm/06-00/kaupp
Page 79

Field Service Manual SC 6002XL Patient Monitor
Table 5-10 Recorder Problems (Continued)
Symptoms Possible Cause(s) Troubleshooting and Remedial Action
Local Recorder
connected to Monitor
through CPS or IDS
1.9 Isolating Cable Malfunctions
Recorder malfunction
CPS/IDS - Recorder
cable malfunction
Recorder Interface
Plate malfunction
CPS or IDS malfunction
Docking Station or CPS
Bridge Plate
malfunction
Main Processor
malfunction
A general troubleshooting and repair approach for cable malfunctions is to
use a known input signal for any given parameter, and then replace a cable
or sensor found to be malfunctioning. Cable malfunctions, including those
associated with connectors on the cables, fall into one of three categories
-- Open circuits, Short circuits, and Intermittent conditions
Open circuits and short circuits manifest themselves as a loss of signal.
Software in the Monitor senses the loss, and generates an error message
such as “ECG Leads Off” and “SpO2 Transparent.” Typically, short
circuits result in software resets.
An intermittent condition (e.g. ECG lead not making good skin contact)
may manifest itself as noise displayed at the monitor screen. A source of
ECG noise can often be isolated by removing the signal and shorting all
ECG leads together. Then flex along the cable, particularly at connectors,
while watching for noise indications on the monitor display.
1. With an ECG waveform from patient simulator on
Monitor display, press Record key.
• If “Recording Started” followed by double-tone,
then “Recording Stored” message appears in the
message field, check cables and connections
between Monitor, CPS/IDS, and Recorder, then
continue to step 2.
• If no message or recording appears, go to step 3.
2. Substitute Recorder connection by installing Recorder
cable, Art. No. 47 21 770 E530U or 43 13 560 E530U,
in place of Docking Station, CPS/IDS, and cabling.
• If problem persists, replace Recorder.
• If problem disappears, replace each component
bypassed by Recorder cable, Art. No. 47 21 770
E530U or 43 13 560 E530U, to isolate source of
problem and replace malfunctioning component.
3. If problem persists, replace Main Processor
Subassembly
4. If problem persists, contact TSS in Solna or Danvers.
1.10 Patient-Related Data
Not Retained or
Monitor Fails to
1) Replace Main PCB Subassembly.
2) If problem persists, contact TSS in Solna or in Danvers.
Compute Trends
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 69
6kXLSMC5.cd-rom.fm/06-00/kaupp
Page 80

SC 6002XL Patient Monitor Field Service Manual
This page left intentionally blank.
70 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMC5.cd-rom.fm/06-00/kaupp
Page 81

Appendix A: Replaceable Parts
Refer to the Table and Figures on page 72 and page 73.
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 71
6kXLSMAA.cd-rom.fm/06-00/kaupp
Page 82

SC 6002XL Patient Monitor Field Service Manual
Table A-1 SC 6000XL - Replaceable Parts and Subassemblies
Item
No.
Description
Siemens Article
Number
1 E/M SPR LNGLBL 6002XL
E/M SPR LNGLBL 6002XL ENG 57 43 799 E551U
E/M SPR LNGLBL 6002XL DEU 57 43 807 E551U
E/M SPR LNGLBL 6002XL FRN 59 53 661 E551U
E/M SPR LNGLBL 6002XL SPN 59 53 711 E551U
E/M SPR LNGLBL 6002XL ITA 59 53 703 E551U
E/M SPR LNGLBL 6002XL POR 59 53 729 E551U
E/M SPR LNGLBL 6002XL NOR 59 53 695 E551U
E/M SPR LNGLBL 6002XL SVE 59 53 687 E551U
E/M SPR LNGLBL 6002XL NLD 59 57 399 E551U
E/M SPR LNGLBL 6002XL DEN 59 53 679 E551U
2 E/M SPR BEZEL/LENS SC6002XL 59 53 968 E551U
3 E/M SPR OPTIC ENCODR SC SERIES 43 11 622 E533U
4 E/M SPR ROTARY KNOB SC 600X SERIES 43 16 662 E533U
5 E/M SPR FOOT .40 SQ X .25 THK (PKG-12) 43 11 374 E533U
6 E/M SPR DISLCD 6.5" TFT 256K 59 50 790 E551U
7 E/M SPR BACKLIGHT 6.5" TFT LCD (PKG'2) 72 58 945 E551U
8 PCB SPR A124 FT PNL SC6002XL NEC 59 57 258 E551U
9 E/M SPR DCAINV NEC + 5V 2 TUBE 59 50 808 E551U
10 E/M SPR PCB A140 POD COM INT 57 41 959 E547U
11 E/M SPR INTERMEDIATE SC6002XL 57 42 304 E551U
12 E/M SPR SPEAKER SC6002XL 59 47 218 E551U
13 E/M SPR A100 SHDL/HS SC6002XL(PROCESSOR
57 42 296 E551U
(shipped w/SW installed and w/SW version label)
14 E/M SPR MANIFOLD NP SC 6002XL 59 50 782 E551U
15 E/M SPR FILTER MFLD NBP (PKG-10) 28 66 726 E516U
16 E/M SPR RT RET PLATE 6002XL COND (incl. LBL ) 72 61 907 E551U
17 E/M SPR LFT RET PLT SC6002XL (incl. LNG LBL ) 72 58 168 E551U
18 E/M SPR RAM CARD EJECTOR BUTTN (PKG-10) 33 76 865 E522U
19 E/M SPR HANDLE SC6000/6000P 47 16 424 E533U
20 E/M SPR CBL HNS BATT SC6002XL 59 54 974 E551U
21 E/M SPR LATCH BATTERY RETAINER 33 79 943 E533U
22 SHP ACC BATTERY (Lead-acid) 59 47 697 E533U
SHP ACC BATTERY (Lithium-ion) 57 32 354 E533U
23 E/M SPR CVR BATTERY SC6000/6000P 33 77 491 E 533U
24 E/M SPR HOUSING REAR SC6002XL (Monitor serial
59 54 784 E551U
number required to order replacement housing
25 E/M SPR PLATE RETAINER SC600X 33 77 533 E533U
26 E/M SPR FUNNEL SC6002XL 57 41 033 E551U
27 E/M SPR NBP CAL PORT CVR 43 28 816 E533U
72 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAA.cd-rom.fm/06-00/kaupp
Page 83

Field Service Manual SC 6002XL Patient Monitor
21
21
2121
27
27
26
26
2626
25
25
2525
J
2727
L
22
22
2222
23
23
2323
24
24
2424
A
l
h
D
H
j
~
20
20
2020
s
;
S
K
l
l
l
a
f
Figure A-1 SC 6002XL Exploded View
G
k
d
g
4pl
G
F
Figure A-2 NBP Subassembly (shown with filters exposed)
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 73
6kXLSMAA.cd-rom.fm/06-00/kaupp
Page 84

SC 6002XL Patient Monitor Field Service Manual
This page intentionally left blank.
74 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAA.cd-rom.fm/06-00/kaupp
Page 85

Appendix B: Connector Pinouts
Figure B-1 IBP Connector (see Table B-1)
Table B-1IBP Connector Pinouts
Pin No. Signal
1 +VREF
2 −VREF
5+IBP
6 −IBP
3, 4, 7 GND
8, 9 SHIELD
Figure B-2MultiMed Pod Connector (see Table B-2)
Table B-2 MultiMed Pod Connector Pinouts
Temp SPO2 ECG
Pin No. Signal Pin No. Signal Pin No. Signal Pin.No. Signal
1 TA 1 DETA 1 SHGND 2 LA
2 TB* 2 DETK SH 3 SHGND 4 LL
3 TCOM 3 NC 5 SHGND 6 RA
4 NC 4 REDK 7 SHGND 8 V
5 NC 5 RCALRTN 9 SHGND 10 RL
6NC 6RCALIB
7NC 7IRK
*
Not Used in SC6000 Series
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 75
6kXLSMAB.cd-rom.fm/06-00/kaupp
Page 86

SC 6002XL Patient Monitor Field Service Manual
Figure B-3Docking Station Connector (see Table B-3)
Table B-3 Docking Station Connector Pinouts
Pin No. Signal Pin No. Signal
1 RCDRPWR 15 DUTX2
2 DCGND 16 DURX2
3 PTXD3 17 DCGND
4 PRXD3 18 VGARED
5 DCGND 19 VGAGRN
6 EXTAUD 20 VGABLU
7 ALARM 21 DCGND
8 PSNL 22 VSYNCLB
9 DUTX1 23 HSYNCLB
10 DURX1 24 RCV−
11 DCGND 25 RCV+
12 DSPWR 26 TX−
13 DURTS 227 TX+
14 DUCTS2 28 SW6
Figure B-4 SHP ACC CBL ALARM UNTERM 5M (see Table B-4)
Table B-4 Remote Alarm Cable Color Code
Color Code
Connector Pin No. Relay Input Wire Color SPDT Relay Output Circuit Status
1Tan BrownRTN
2 - 8 NC Green Inactive Open
9 Orange White Inactive Closed
10 - 14 NC
76 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAB.cd-rom.fm/06-00/kaupp
Page 87

Field Service Manual SC 6002XL Patient Monitor
X7X5
Figure B-5 Interface Plate Connector (see Table B-5)
Table B-5 Interface Plate Connectors Pinouts
Pin No CRT - X5 Recorder/Alarm - X7
1Ext RedGND
2 VGND +12VDC
3Ext GrnRec Tx
4 VGND +12VDC
5Ext BluDiag Tx
6 VGND +12VDC
7 GND Rec RTS
8H SyncRec CTS
9V SyncAlarm Out
10 Rem TxD Rec GND
11 Rem RxD Rec GND
12 Power Switch Rec Rx
13 Rem Audio Rec GND
14 Rem Audio Ret Diag Rx
Figure B-6SHP ACC CBL Y RECORDER/ALARM (see Table B-6)
Table B-6 Remote Alarm Cable Color Code
Color Code
Connector Pin No. Relay Input Wire Color SPDT Relay Output Circuit Status
1Tan BrownRTN
2 - 8 NC Green Inactive Open
9 Orange White Inactive Closed
10 - 14 NC
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 77
6kXLSMAB.cd-rom.fm/06-00/kaupp
Page 88

Field Service Manual SC 6002XL Patient Monitor
8
1
14-Pin 20-Pin 26-PinNetwork
Figure B-7 Basic/Device CPS Connectors - Infinity Network (see Table B-7)
Tab le B - 7 I
ALM/KB/DIAG/COMM-1 (X4) ALM/KB/DIAG/COMM-2 (X3) External CRT (X5) AUX/MIB/CANBUS(X12) Recorder (X13)
Pin No. Signal Pin No. Signal Pin No. Signal Pin.No. Signal Pin.No. Signal
10 GND 10 GND 10 Remote TxD 10 AUX1 ID1 10 AUX Pwr2
11 H W B o o t L 11 NMI 11 Remote RxD 11 AUX 1 ID2 11 AU X 2 I D 0
12 COMM-1 Rx 12 COMM-2 Rx 12 Power
13 COMM-1 Tx 13 COMM-2 Tx 13 Rem Audio 13 GND 13 AUX ID2
14 Diag RxD 14 Diag RxD 14 Rem Audio
NFINITYNET
CPS Connector Pins
1 GND 1 GND 1 Ext Red 1 MIB1 D+ 1 R50A TxD
2 Tx Data KB 2 Tx Data KB 2 VGND 2 MIB1 Pwr 2 AUX Pwr2
3 Rem Kbd Pwr 3 Rem Kbd Pwr 3 Ext Grn 3 MIB1 D- 3 R50A RxD
4 ISD Power 4 ISD PWR 4 VGND 4 MIB2 Pwr 4 AUX Pwr2
5 Diag TxD (CPS) 5 Diag TxD 5 Ext Blu 5 MIB1 S+ 5 R50A CTS
6 DEBUG1 6 MCBOOTL 6 VGND 6 CAN+ 6 AUX Pwr2
7 ISD GND 7 ISD GND 7 GND 7 MIB1 S- 7 R50A RTS
8 RxData KB 8 RxData KB 8 H-Sync 8 CAN R
L
8AUX Pwr2
9 Alarm Out 9 Alarm Out 9 V-Sync 9 AUX1 ID0 9
12 MIB2 D+ 12 AUX ID1
Switch
14 MIB2 D- 14 AUX P Enb
Ret
15 GND 15 P GND
16 MIB2 S+ 16 AUX Tx+
17 GND 17 P GND
18 MIB2 S- 18 AUX Tx-
19 CANBUS+ 19 P GND
20 Chassis GND 20 AUX Rx+
Network (X14)
21 P GND
Pin No. Signal 22 AUX Rx-
1Tx+ 23 P GND
2Tx- 24
3Rx+ 25 GND
6Rx- 26 GND
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 78
6kXLSMAB.cd-rom.fm/06-00/kaupp
Page 89

SC 6002XL Patient Monitor Field Service Manual
8
18
14
14-pinNetwork
10 1
20-pin
14
26
26-pin
Figure B-8 Infinity Docking Station Connectors(Refer to Table B-8.)
Table B-8 Infinity Docking Station Connectors
ALM/KB/DIAG/COMM-1 (X4) ALM/KB/DIAG/COMM-2 (X3) External CRT (X5) AUX/MIB/CANBUS(X12) Recorder (X13)
Pin Signal Pin Signal Pin Signal Pin Signal Pin Signal
1 GND 1 GND 1 Ext Red 1 MIB1 D+ 1 R50A TxD
2 Tx Data KB 2 Tx Data KB 2 VGND 2 MIB1 Pwr 2 AUX Pwr2
3 Rem Kbd Pwr 3 Rem Kbd Pwr 3 Ext Grn 3 MIB1 D- 3 R50A RxD
4 ISD Power 4 ISD PWR 4 VGND 4 MIB2 Pwr 4 AUX Pwr2
5 Diag TxD (CPS) 5 Diag TxD 5 Ext Blu 5 MIB1 S+ 5 R50A CTS
6 DEBUG1 6 MCBOOTL 6 VGND 6 CAN+ 6 AUX Pwr2
7 ISD GND 7 ISD GND 7 GND 7 MIB1 S- 7 R50A RTS
8 RxData KB 8 RxData KB 8 H-Sync 8 CAN R
L
8AUX Pwr2
9 Alarm Out 9 Alarm Out 9 V-Sync 9 AUX1 ID0 9
10 GND 10 GND 10 Remote TxD 10 AUX1 ID1 10 AUX Pwr2
11 HWBootL 11 NMI 11 Remote RxD 11 AUX1 ID2 11 AUX2 ID0
12 COMM-1 Rx 12 COMM-2 Rx 12 Pwr Switch 12 MIB2 D+ 12 AUX2 ID1
13 COMM-1 Tx 13 COMM-2 Tx 13 Rem Audio 13 GND 13 AUX2 ID2
14 Diag RxD 14 Diag RxD 14 Rem Aud Ret 14 MIB2 D- 14 AUX2 P Enb
15 GND 15 P GND
16 MIB2 S+ 16 R100A TxD+
Signal
Pin
1 GND
2PWR
PSL (X20)
Network (X14)
Pin Signal
Tx+
1
Tx-
2
Rx+
3
Rx-
6
17 GND 17 P GND
18 MIB2 S- 18 R100A TxD-
19 CANBUS+ 19 P GND
20 Chassis GND 20 R100A RxD+
21 P GND
22 R100 RxD-
23 P GND
24
25 Chassis GND
26 Chassis GND
79 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAB.cd-rom.fm/06-00/kaupp
Page 90

Field Service Manual SC 6002XL Patient Monitor
Figure B-9 PodPort Connector (see Table B-9)
Table B-9 PodPort Connector Pinouts
Pin No. Signal
1TXDATA+
2NC
3TXDATA-
4RXDATA+
5POD GND
6POD PWR
7RXDATA-
8,9 POD1 SHD
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 80
6kXLSMAB.cd-rom.fm/06-00/kaupp
Page 91

Appendix C: Error and Diagnostic Codes
1Introduction
1.1 Startup Messages
1.2 Diagnostic Log
This section describes startup, diagnostic, and error messages produced
by SC6002XL Patient Monitors. Codes listed in this appendix are typical.
Codes are sometimes different, however, in different versions of SW.
Upon power-up, the monitor runs internal diagnostics that check various
functions. The Startup Screen remains in place for several seconds after
the last message. All hardware and software for the various functions
checked is assumed to be functioning properly if no error messages
display during the startup sequence.
Messages stored in the Diagnostic Log refer to startup diagnostics,
hardware and software errors, and designated exception conditions such
as a user-initiated language change. Some diagnostic codes, such as
“Software Option Unlocked” are only informational and require no action.
Classes of Error/Diagnostic codes are as follows:
• Power-Up
• MPC821 (Main Processor)
• PSOS
• Front End
• Diagnostic
• Taskmail
• Peripherals
• Database
•NBP
•SpO2
• User Interface
• Data Processing
• High Temperature
• Language Change
• Software Update
•Network
• Software Option Unlocked
•etCO2
To access the Diagnostic Log, select BIOMED on the Main menu and then
DIAG. LOG.
Diagnostic Log messages have the form --
Date/Time Code Description (3P/VB2.3-W)
↑↑↑
four-digit hexadecimal code
The four-digit hexadecimal code can help service personnel identify a
subassembly or module that may need to be replaced in a malfunctioning
monitor and provide quick remedial action. Specific codes help developers
diagnose the actual cause of a problem. The first 80 entries in the Log can
be printed on a Recorder by pressing the Record key while the diagnostic
log is displayed. Logs may also be downloaded onto a PC by setting up the
PC and connecting it to the monitor as described in either Section 5.17.1
or Section 5.17.2 of Chapter 3, and using the following procedure:
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 81
6kXLSMAC.cd-rom.fm/06-00/kaupp
Main Board H/W Rev./SW Rev.
Page 92

SC 6002XL Patient Monitor Field Service Manual
1) Do either of the following as required:
• If monitor equipped with interface plate, plug other end of cable into
X7 on interface plate.
• If monitor mounted on docking station or I
other end of cable into X3 on CPS or IDS.
2) Plug in monitor power adapter and power-up monitor.
3) After MAIN screen displays on monitor, press <Esc> on PC/laptop
keyboard.
SC6002XL SUPPORT MENU
00) Error Display 01)Event Log
02) Database Defaults 03)Real-time Clock
04) Set EEPROM H/W Rev. 05)Set NBP Constants
06) Verify NBP Constants 07)Display Service Data
Press ENTER to exit
Table C-1 Support Menu (Item numbers may differ between different
versions of installed software.)
4) When SC6002XL SUPPORT MENU displays, select option 0, Error
Display and press <Enter>.
5) Either press any key if more than one page, until prompt “Enter <R>
to Reset Buffer, <CR> to exit appears, or press E to print to end of
file.
NFINITY
Docking Station, plug
1.3 Severity Codes
1.4 Reset Causes
6) Save file on floppy disk.
Note: If Win95 installed on PC or laptop, include date in file name.
Error Severity listed in the Diagnostic Log are interpreted as follows:
Type Code Result
Note 0 -- not an error -Informational only
Warning 1 -- error logged, no sys reset
Fatal 2 -- from non-interrupt code, sys reset
Trap 3 -- from interrupt code, sys reset
Diagnostic 4 -- from diagnostics, diag mst on display
Database 5 -- like fatal error, with db factory reset
Shutdown 6 -- shuts down everything except the monitor
-- used to define reset cause slot in error buffer.
Power-up 0 Low-voltage Shutdown 5
SW Trap Error 1 Debug Shutdown 6
Watchdog 2 Language Change 7
3-min. Timeout 3 SW Option Unlocked 8
High-temp Shutdown 4 SW Watchdog 9
82 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAC.cd-rom.fm/06-00/kaupp
Page 93
Field Service Manual SC 6002XL Patient Monitor
2Diagnostic
Messages
Table C-2 Startup Diagnostic Log Codes
Description Code Class
MONITOR_POWERUP 0x0000 Power-Up
SOFTWARE_VERSION_CHANGE 0x0001 Software Update
USER_LANGUAGE_CHANGE 0x0002 Language Change
ARRHYTHMIA_UNLOCKED 0x0003 Software Option Unlocked
NEONATAL_UNLOCKED 0x0004 Software Option Unlocked
TEMP_ALARMS_UNLOCKED 0x0005 Software Option Unlocked
DEMO_SOFTWARE_UNLOCKED 0x0006 Software Option Unlocked
SC9015_UNLOCKED 0x0007 Software Option Unlocked
OCRG_UNLOCKED 0x0008 Software Option Unlocked
NCO_UNLOCKED 0x0009 Software Option Unlocked
SECOND_IBP_UNLOCKED 0x000A Software Option Unlocked
ST_SEGMENT_UNLOCKED 0x000B Software Option Unlocked
Note: Messages listed in Table C-2 are only informational.
OLYMPUSNET_UNLOCKED 0x000C Software Option Unlocked
ETCO2_UNLOCkED 0x000D Software Option Unlocked
Table C-3 Exception Messages
Description Code Class
SVC_PARAM_ERROR 0x0801 MPC821
BUS_ERROR_CODE 0x0802 MPC821
ADDR_ERROR_CODE 0x0803 MPC821
ILL_INST_CODE 0x0804 MPC821
ZERO_DIVIDE_CODE 0x0805 MPC821
CHK_INST_CODE 0x0806 MPC821
TRAPV_INST_CODE 0x0807 MPC821
PRIV_VIOLATION_CODE 0x0808 MPC821
TRACE_CODE 0x0809 MPC821
UNASSIGNED_CODE 0x080C MPC821
SPURIOUS_CODE 0x080D MPC821
TRAPS_CODE 0x080E MPC821
UNUSED_VECTOR_CODE 0x080F MPC821
EXC_RESET 0x0810 MPC821
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 83
6kXLSMAC.cd-rom.fm/06-00/kaupp
Page 94

SC 6002XL Patient Monitor Field Service Manual
Table C-3 Exception Messages (Continued)
Description Code Class
EXC_MACH_CK 0x0802 MPC821
EXC_DA 0x0811 MPC821
EXC_IA 0x0812 MPC821
EXC_INTRPT 0x0813 MPC821
EXC_ALIGN 0x0814 MPC821
EXC_PROGRAM 0x0815 MPC821
EXC_FLOAT 0x0816 MPC821
EXC_DCRMNTR 0x0817 MPC821
EXC_SYSCALL 0x0818 MPC821
EXC_TRACE 0x0809 MPC821
EXC_FP821 0x0819 MPC821
EXC_SEI821 0x0804 MPC821
EXC_IMTLB821 0x0820 MPC821
EXC_DMTLB821 0x0821 MPC821
EXC_IETLB821 0x0822 MPC821
EXC_DETLB821 0x0823 MPC821
EXC_DA_BP821 0x0824 MPC821
EXC_IA_BP821 0x0825 MPC821
EXC_PBK821 0x0826 MPC821
EXC_NMIBK821 0x0827 MPC821
EXC_BUS_ERR 0x0828 MPC821
Table C-4 Hardware-related Messages
Description Code Class
IM_SPURIOUS_INTERRUPT 0x082f MPC821
BAD_DATE_FORMAT 0x0830 PERIPHERALS
BAD_TIME_FORMAT 0x0831 PERIPHERALS
RTC_HARDWARE_PROBLEM 0x0832 PERIPHERALS
HW_WATCHDOG_TIMEOUT 0x0833 MPC821
NP_3_MIN_TIMEOUT 0x0834 NBP
NP_OVERPRESSURE_OCCURRED 0x0835 NBP
HW_PUMP_OR_VALVE_FAILURE 0x0836 NBP
PSOS_TIME_NOT_SET 0x0837 DATA_PROCESSING
84 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAC.cd-rom.fm/06-00/kaupp
Page 95
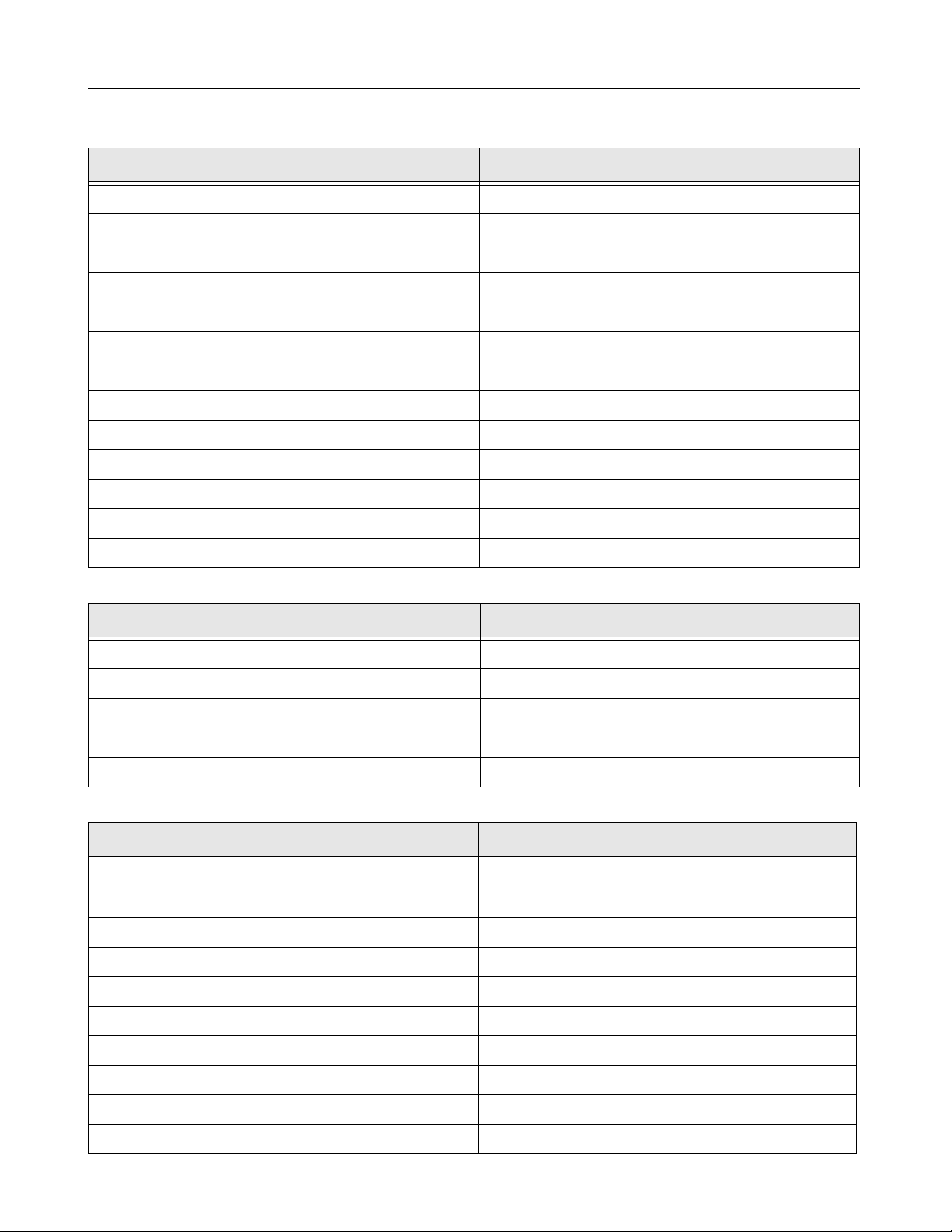
Field Service Manual SC 6002XL Patient Monitor
Table C-4 Hardware-related Messages (Continued)
Description Code Class
SHUTDOWN_BATTERY_VOLTAGE_LOW 0x0838 PERIPHERALS
BATTERY_CHARGE_RATE_ERROR 0x0839 PERIPHERALS
BATTERY_DISCHARGE_RATE_ERROR 0x083A PERIPHERALS
SHUTDOWN_TEMPERATURE_TOO_HIGH 0x083B HIGH_TEMPERATURE
MARGINAL_PCMCIA_BATTERY 0x083C PERIPHERALS
PSN_CONNECT_CONFLICT 0x083D NETWORK
BAD_HW_REVISION 0x083E PERIPHERALS
TEMPERATURE_TOO_LOW 0x083F DATA_PROCESSING
HDLC_ERROR_LIMIT_EXCEEDED 0x0840 NETWORK
OLYNET_TIME_CHANGE 0x0841 NETWORK
RTC_BEING_READ 0x0842 PERIPHERALS
SW_WATCHDOG_TIMEOUT 0x0843 MPC821
SYS_TRACEBACK 0x0844 DIAGNOSTIC
Table C-5 Intertask Mail Messages
Description Code Class
ERROR_WORDCOUNT_ZERO 0x0850 TASKMAIL
ERROR_FULL_QUEUE 0x0851 TASKMAIL
STATUS_EMPTY_QUEUE 0x0852 TASKMAIL
ERROR_NOT_ENOUGH_BUFFER 0x0853 TASKMAIL
ERROR_BAD_QUEUE_ID 0x0854 TASKMAIL
Table C-6 Miscellaneous Messages
Description Code Class
PSOS_TIMER_ERROR 0x08E1 PSOS
BAD_FRONTEND_TYPE 0x08E2 FRONTEND
BAD_SCC1_STATE 0x08E3 NETWORK
SID_ERROR 0x08E4 DATA_PROCESSING
PID_ERROR 0x08E5 DATA_PROCESSING
PBOX_ERROR 0x08E6 DATA_PROCESSING
INVALID_BP_LABEL 0x08E7 DATA_PROCESSING
ILLEGAL_DATABASE_ACTIVITY 0x08E8 DATABASE
BAD_ARRHY_EVENT 0x08E9 DATA_PROCESSING
PSOS_ERROR 0x08EA PSOS
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 85
6kXLSMAC.cd-rom.fm/06-00/kaupp
Page 96

SC 6002XL Patient Monitor Field Service Manual
Table C-7 Alternative Memory Manager to PSOS OSL Messages
Description Code Class
EXT_OSL_BAD_TASK_ID 0x0700 PSOS
EXT_OSL_INIT_FAILED 0x0701 PSOS
EXT_OSL_STACK_OVERRUN 0x0702 PSOS
EXT_OSL_NULL_LIST 0x0703 PSOS
EXT_OSL_BAD_LIST 0x0704 PSOS
EXT_OSL_BAD_PARAM 0x0705 PSOS
EXT_OSL_LIST_CORRUPT 0x0706 PSOS
EXT_OSL_EMPTY_SEARCH 0x0707 PSOS
EXT_OSL_NULL_NODE 0x0708 PSOS
EXT_OSL_NODE_ALREADY_REMOVED 0x0709 PSOS
EXT_OSL_NO_BLOCKS 0x070a PSOS
EXT_OSL_BAD_PGROUP 0x070b PSOS
EXT_OSL_NO_PID 0x070c PSOS
EXT_OSL_NOT_A_BLOCK 0x070d PSOS
EXT_OSL_Q_MSG_RECEIVED 0x070e PSOS
EXT_OSL_BAD_QID 0x070f PSOS
EXT_OSL_Q_TIMEOUT 0x0710 PSOS
EXT_OSL_Q_FULL 0x0711 PSOS
EXT_OSL_BAD_QMODE 0x0712 PSOS
EXT_OSL_BAD_INDEX 0x0713 PSOS
EXT_OSL_BAD_TASK_GROUP 0x0714 PSOS
EXT_OSL_BAD_TASK_PRIORITY 0x0715 PSOS
EXT_OSL_IDLE_TASK 0x0716 PSOS
EXT_OSL_BAD_SEM_ID 0x0717 PSOS
EXT_OSL_BAD_FLAG_ID 0x0718 PSOS
EXT_OSL_BAD_ENTITY 0x0719 PSOS
EXT_OSL_EXCESSIVE_DELAY 0x0720 PSOS
EXT_OSL_ILLEGAL_CALL_IN_PREOS 0x0721 PSOS
EXT_OSL_ILLEGAL_CALL_IN_INTR 0x0722 PSOS
EXT_OSL_INVALID_FREE_PTR 0x0723 PSOS
EXT_OSL_FREE_BLOCK_OVERLAP_PREV 0x0724 PSOS
EXT_OSL_FREE_BLOCK_OVERLAP_NEXT 0x0725 PSOS
86 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAC.cd-rom.fm/06-00/kaupp
Page 97

Field Service Manual SC 6002XL Patient Monitor
Table C-7 Alternative Memory Manager to PSOS OSL Messages (Continued)
Description Code Class
EXT_OSL_INVALID_POOL_ID 0x0726 PSOS
EXT_OSL_INVALID_NBYTES 0x0727 PSOS
EXT_OSL_OUT_OF_MEMORY 0x0728 PSOS
EXT_OSL_CORRUPT_BLOCK 0x0729 PSOS
EXT_OSL_COPROC_FAILURE 0x0730 PSOS
Table C-8 NP Subsystem Messages
Description Code Class
BAD_FEATURE_ID 0x6001 DATABASE
BAD_DB_OFFSET 0x6002 DATABASE
NP_DBG_ERROR 0x6600 DATABASE
NP_DBP_ERROR 0x6700 DATABASE
ERROR_BAD_SP_ACTION 0x6100 NBP
ERROR_BAD_SP_INPUT 0x6101 NBP
ERROR_BAD_SP_STATE 0x6102 NBP
AD_CAL_FAILURE 0x6103 NBP
OVERPRESS_TEST_FAIL 0x6104 NBP
OVERPRESS_WONT_CLEAR 0x6105 NBP
PING_PONG_UNDERFLOW 0x6106 NBP
ERROR_BAD_AUTO_ZERO 0x6107 NBP
ERROR_BAD_VALVE_SETTING 0x6108 NBP
SHORT_TERM_INDEX_TOO_LARGE 0x6109 NBP
PROFILE_INDEX_TOO_LARGE 0x610A NBP
BAD_PULSE_EXTRACT_STATE 0x610B NBP
BAD_USER_MODE 0x610C NBP
BAD_V3_MODULATION_GAIN 0x610D NBP
BAD_NP_CP2SP_MSGTYPE 0x610E TASKMAIL
BAD_MEAS_TYPE 0x610F NBP
TOO_MANY_PULSES 0x6110 NBP
SP_BAD_PULSE_LIST 0x6111 NBP
SP_BAD_TIME_BASED_LIST 0x6112 NBP
BAD_TREND_STATE 0x6113 NBP
BAD_PULSE_COUNT 0x6114 NBP
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 87
6kXLSMAC.cd-rom.fm/06-00/kaupp
Page 98

SC 6002XL Patient Monitor Field Service Manual
Table C-8 NP Subsystem Messages (Continued)
Description Code Class
BAD_SMOOTHING_TYPE 0x6115 NBP
SP_BAD_PULSE_INDEX 0x6116 NBP
PROFILE_INDEX_TOO_SMALL 0x6117 NBP
BAD_CUFF_PRESS_INDEX 0x6118 NBP
TOO_MANY_TIME_BASED_PULSES 0x6119 NBP
TOO_MANY_EVEN_SAMPLE_POINTS 0x611A NBP
BAD_EVEN_SAMPLE_AMP 0x611B NBP
SP_SINGULAR_MATRIX 0x611C NBP
SP_LINK_DOWN 0x611D NBP
SP_RAPID_ROC 0x611E NBP
SW_OVERPRESSURE_OCCURED 0x611F NBP
CROSSOVER_OVERRUN 0x6120 NBP
CROSSOVER_TIMEOUT 0x6121 NBP
ICV_CALC_PROBLEM 0x6122 NBP
BAD_COLLECT_DEFINE 0x6123 NBP
BAD_EVAL_REQUEST 0x6124 NBP
AD_DISCONTINUTIY 0x6125 NBP
AD_VALUE_OOR_HIGH 0x6126 NBP
AD_VALUE_OOR_LOW 0x6127 NBP
AD_NO_ACTIVITY 0x6128 NBP
BAD_CF2SP_MSGTYPE 0x6129 TASKMAIL
BAD_EVAL_STATE 0x612A NBP
BAD_EVAL_STATUS 0x612B NBP
CF_TIMER_EXPIRED 0x612C NBP
CF_RQ_BLK_STILL_ACTIVE 0x612D NBP
BAD_PNEUM_STATE 0x612E NBP
PNEUM_CHAR_FAILED 0x612F NBP
HW_SAFETY_TIMER_EXPIRED 0x6130 NBP
HW_SAFETY_TIMED_OUT_IN_CAL 0x6131 NBP
BAD_INFLATION_LIMIT 0x6132 NBP
ERROR_BAD_AC2NP_MSGTYPE 0x6300 TASKMAIL
ERROR_BAD_SP2CP_MSGTYPE 0x6301 TASKMAIL
88 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAC.cd-rom.fm/06-00/kaupp
Page 99

Field Service Manual SC 6002XL Patient Monitor
Table C-8 NP Subsystem Messages (Continued)
Description Code Class
ERROR_BAD_MO2NP_MSGTYPE 0x6302 TASKMAIL
ERROR_BAD_NP2AC_MSGTYPE 0x6303 TASKMAIL
ERROR_BAD_CP2SP_MSGTYPE 0x6304 TASKMAIL
ERROR_BAD_MC_INPUT 0x6305 NBP
ERROR_BAD_MC_STATE 0x6306 NBP
ERROR_BAD_MC_ACTION 0x6307 NBP
ERROR_BAD_MC_QUEUE 0x6308 TASKMAIL
NPCOOR_BAD_EF_IMAGE 0x6309 DIAGNOSTIC
SP2CP_RING_DEQUEUE_ERROR 0x630A TASKMAIL
BAD_SP2CF_MSGTYPE 0x6500 TASKMAIL
CF_SINGULAR_MATRIX 0x6501 NBP
SP2CF_PROBLEM 0x6502 TASKMAIL
NPCF_BAD_EF_IMAGE 0x6503 DIAGNOSTIC
CF2SP_RING_DEQUEUE_ERROR 0x6504 TASKMAIL
Table C-9 Diagnostic Messages
Description Code Class
DIAG_ERROR_NON_PRESERVED_RAM 0x0901 DIAGNOSTIC
DIAG_ERROR_PRESERVED_RAM 0x0902 DIAGNOSTIC
DIAG_ERROR_LITHIUM_BATTERY_DEAD 0x0903 DIAGNOSTIC
DIAG_ERROR_BAD_CHKSUM_ADDRESS 0x0904 DIAGNOSTIC
DIAG_ERROR_STACK_OVERFLOW 0x0905 DIAGNOSTIC
DIAG_ERROR_ROM_CHECKSUM 0x0906 DIAGNOSTIC
DIAG_ERROR_NOT_ENOUGH_SAVE_AREA 0x0907 DIAGNOSTIC
DIAG_ERROR_TMS_INITIALIZATION 0x0908 DIAGNOSTIC
DIAG_ERROR_TASK_CREATION 0x0909 DIAGNOSTIC
DIAG_ERROR_TASK_INITIATION 0x090A DIAGNOSTIC
DIAG_ERROR_QUART_INITIALIZATION 0x0B00 DIAGNOSTIC
Table C-10 INTER Messages
Description Code Class
DM_NO_MORE_STREAMS 0x0A01 FRONTEND
DM_INVLD_STREAM 0x0A02 FRONTEND
BAD_SCC1_EVENT 0x0A03 FRONTEND
ASK-T941-04-7600 Siemens Medical Systems, EM-PCS Danvers 89
6kXLSMAC.cd-rom.fm/06-00/kaupp
Page 100

SC 6002XL Patient Monitor Field Service Manual
Table C-10 INTER Messages (Continued)
Description Code Class
SCC1_BUFFER_NOT_FULL 0x0A04 FRONTEND
BAD_STRM_GET 0x0A10 DIAGNOSTIC
BAD_STRM_CREATE 0x0A20 DIAGNOSTIC
BAD_STRM_PUT 0x0A30 DIAGNOSTIC
SCC3_TX_BUFFERS_FULL 0x0A40 PERIPHERALS
Table C-11 Print Messages
Description Code Class
PRINT_BAD_EF_IMAGE 0x1001 DIAGNOSTIC
PRINT_UNDEFINED_SYSTEM_STATE 0x1002 DIAGNOSTIC
MA2PR_UNDEFINEDMSG 0x1003 TASKMAIL
MA2PR_RING_DEQUEUE_ERROR 0x1004 TASKMAIL
PR2MA_UNDEFINEDMSG 0x1005 TASKMAIL
ERROR_BAD_PRINT_INPUT 0x1006 DATA_PROCESSING
ERROR_BAD_PRINT_STATE 0x1007 DATA_PROCESSING
ERROR_BAD_PRINT_ACTION 0x1008 DATA_PROCESSING
CORD_ERROR_INV_GRID_COMBINATION 0x1009 PERIPHERALS
CORD_ERROR_TEXT_BUFFER_OVERFLOW 0x100A PERIPHERALS
CORD_ERROR_DELAYED_TEXT_OVERFLOW 0x100B PERIPHERALS
CORD_ERROR_INV_TEXT_FIELD 0x100C PERIPHERALS
CORD_ERROR_INV_ANN_LINE 0x100D PERIPHERALS
CORD_ERROR_CURVE_BUFFER_OVERFLOW 0x100E PERIPHERALS
CORD_ERROR_INV_DATA_CONVERSION 0x100F PERIPHERALS
CORD_ERROR_INV_SPEED 0x1010 PERIPHERALS
CORD_ERROR_NOT_ENOUGH_MEMORY 0x1011 PERIPHERALS
CORD_ERROR_CMD_OVERFLOW 0x1012 PERIPHERALS
CORD_ERROR_INV_SPECIAL_TREND_PARAM_TYPE 0x1013 PERIPHERALS
CORD_ERROR_MALLOC_ERROR 0x1014 PERIPHERALS
CORD_ERROR_FREE_ERROR 0x1015 PERIPHERALS
CORD_ERROR_AR42_QUEUE_NOT_EMPTIED 0x1016 PERIPHERALS
CORD_ERROR_AR42_SEND_ERROR 0x1017 PERIPHERALS
CORD_ERROR_AR42_CONTROL_ERROR 0x1018 PERIPHERALS
CORD_ERROR_SMPL_RATE_CREATE_FAILED 0x1019 PERIPHERALS
90 Siemens Medical Systems, EM-PCS, Danvers ASK-T941-04-7600
6kXLSMAC.cd-rom.fm/06-00/kaupp
 Loading...
Loading...