

Page 1
Operative Technique
KnifeLight
Carpal Tunnel Ligament Release
T2
Recon Nailing System R2.0
Operative Techn ique
Hip & Femur Fractures
Hip
Femur
Page 2
T2 Recon Nailing System
We greatly acknowledge and
appreciate the contributions to this
operative technique made by:
Kevin W. Luke, M.D.
Parkview Orthopaedic Group
Assistant Clinical Professor
Department of Orthopaedic Surgery
University of Illinois
Illinois, Chicago
USA
Anthony T. Sorkin, M.D.
Rockford Orthopaedic Associates, LLP
Clinical Instructor
Dep. of Surgery University of Illinois
College of Medicine
Director Orthopaedic Traumatology
Rockford Memorial Hospital
Rockford, Illinois
USA
Ariaan D.P. van Walsum, MD
Trauma surgeon
Medical Spectrum Twente
Enschede
Netherlands
Don Weber, MD, FRCSC
Associate Clinical Professor of
Orthopaedics
Chief of Orthopaedics
University of Alberta Hospital
Edmonton, Alberta
Canada
Contributing Surgeons
2
Page 3

This publication sets forth detailed
recommended procedures for using
Stryker Osteosynthesis devices and
instruments.
It offers guidance that you should
heed, but, as with any such technical
guide, each surgeon must consider
the particular needs of each patient
and make appropriate adjustments
when and as required.
A workshop training is required prior
to first surgery.
All non-sterile devices must be
cleaned and sterilized before use.
Follow the instructions provided in
our reprocessing guide (L24002000).
Multi-component instruments must
be disassembled for cleaning. Please
refer to the corresponding assembly/
disassembly instructions.
See package insert (L22000007) for
a complete list of potential adverse
effects, contraindications, warnings
and precautions. The surgeon must
discuss all relevant risks, including
the finite lifetime of the device, with
the patient, when necessary.
Warn ing :
Fixation Screws:
Stryker Osteosynthesis bone
screws are not approved or
intended for screw attachment
or fixation to the posterior elements (pedicles) of the cervical,
thoracic or lumbar spine.
3
Page 4

Contents
Page
1. Introduction & Features 5
Implant Features 5
Technical Specifications 6
Instrument Features 7
2. Indications, Precautions & Contraindications 8
3. Pre-operative Planning 9
4. Locking Options 10
5. Operative Technique 11
Patient Positioning and Fracture Reduction 11
Incision 11
Entry Point 12
Re a ming 14
Nail Selection 16
Assembly of the Targeting Device and the Nail 17
Nail Insertion 18
Final Seating with Impactor 18
Guided Locking for the Recon Mode 19
Guided Locking for Antegrade Femoral Mode 29
Freehand Distal Locking 32
Set Screw or End Cap Insertion 34
Nail Removal 34
Ordering Information – Implants 35
Ordering Information – Instruments 37
4
Page 5

Introduction
Over the past decades antegrade
and retrograde femoral nailing have
become widely accepted choices for
the treatment of femoral fractures.
The T2 Recon nail is one of the first
femoral nailing systems to offer a
greater trochanter entry point with
both recon and antegrade locking
options.
Through the development of a
common, streamlined instrument
system and intuitive surgical approach,
both in principle and in detail, the T2
Recon Nail offers the potential for
more efficient treatment of fractures
as well as simplifying the training
requirements for all person nel
involved.
Furthermore, the T2 Recon Nail offers
the following competitive advantages:
• Versatility-offerstheabilityto
switch from antegrade to a recon
option without changing either
the nail or targeting arm.
• ReconSetScrew-thisoptional
screw sets the most proximal
Lag Screw thus minimizing
the potential for screw sliding
(Z-effect).
• LockingOptions-distaloptions
include dynamic as well as static.
• DistalTargeting-eliminatesthe
need for freehand locking of either
the static or dynamic modes.
RequiresoptionalGamma3/T2
ReconDTSR2.0
The T2 Recon Nail is the realization
of excellent biomechanical intramedullary stabilization for internal
femoral fixation with several locking
options to address fracture variability.
As with all other T2 Nails, the T2
Recon Nail is made of Type II
anodized Titanium Alloy (Ti6Al4V)
for enhanced biomechanical and
biomedical performance*.
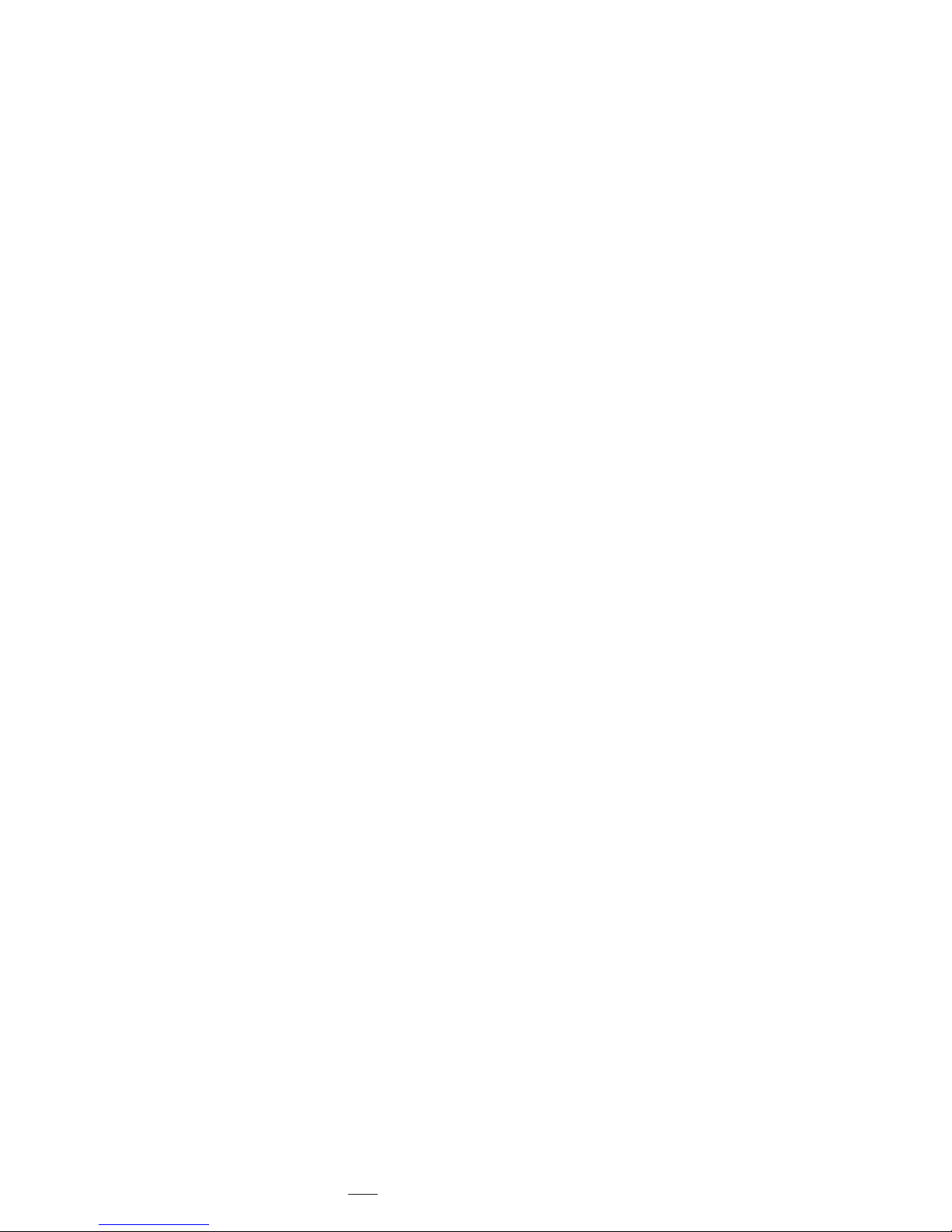
The T2 Recon Nail features a 125°
CCDanglewitha10°anteversion
angle. The 2 proximal holes, each
utilize 6.5mm cannulated Lag
Screws. This CCDangle allows easy
insertion of the 2 lag screws into the
femoral head.
Alternatively a proximal 70° Oblique
hole with 7° retroversion provides
a 5mm Fully Threaded Screw for
targeting the lesser trochanter in the
Femoral Antegrade mode.
The 6.5 mm Cannulated Lag Screws
have a unique thread design that
provide an excellent grip. Improved
front cutting flutes allow for lesser
insertion torque and thinner flanks for
less bone removal.
Secure placement of the Lag Screws
within small neck diameters can be
achieved due to 10mm separating the
two 6.5mm lag screws or 17mm outer
distance between the 6.5mm Lag screws.
Two Set Screws are available:
- Recon Set Screw: Tightens the
6.5mm proximal Lag Screw (Recon
Mode) and
- Antegrade Set Screw: Tightens the
oblique 5mm Fully Threaded Screw
(Femoral Antegrade Mode).
Available as left and right versions,
the T2 Recon Nail incorporates an
antecurvature radius of 2.0M, as
well as a 4° medial lateral bend for
trochanteric insertion.
The distal locking configuration
features a round and an oblong hole to
allow for staticand/ordynamic
distal locking.
Low profile 5mm cortical screws,
common to the T2 Nailing System,
are designed to simplif y the surgical
procedure and promote a minimally
invasive approach.
5mm Fully Threaded Locking Screws
are available for distal locking (Recon
or Femoral Antegrade Mode) and
for the proximal locking in Femoral
Antegrade Mode.
End Caps are available in various
lengths to provide a better fit.
See the detailed chart on the next page
for the design specifications and size
offerings.
Implant FeaturesIntroduction
* Axel Bauman n, Nils Zander, Ti6Al4V with
Anodization Type II: Biological Behaviour and
Biomecha nical Effects, White Paper, March 2005.
5
Page 6
Introduction
NailDiameter 9, 11, 13 and 15mm
(Left and Right)
Sizes 280−480mm,
in 20mm increments
Note:
• Proximal diameter is 13mm for
the 9 and 11mm Nails and 15mm
for the 13 and 15mm Nails.
• Check with your local
representative regarding
availability of nail sizes.
5.0mm Fully Threaded
Locking Screws
L = 25–120mm
6.5mm Cannulated
Lag Screws
L = 65–130mm
Antegrade Set Screw
End Caps
Stand ard +5mm +10mm +15mm
0mm
Antecurvature
radius 2.0M
40mm
20mm
15mm
0mm
4° Medial Lateral bend
44mm
70°
125°Nail angle
0mm
26mm
10.5 mm
Technical Specifi cations
Recon Set Screw
17.0 mm
Note:
Screw length is measured
from top of head to tip.
6
Page 7

Introduction
Instrument Features
A major advantage of the T2
instrument platform is the integration
of core instruments that can be
used not only for the complete T2
Nailing System, but for future Stryker
Osteosynthesis nailing systems,
thereby, reducing complexity and
inventory.
The T2 instrument platform offers
precision and usability, as well as
ergonomically styled targeting devices.
Except for the addition of a small
number of dedicated instruments, the
T2 Femur instrument platform is used
for the T2 Recon Nail.
The T2 Recon targeting device is
designed to provide two proximal locking
options: Recon or Antegrade Femoral
Modes.
Reconmode: Provides two (2)
proximal holes targeting the femoral
neck and head:
• B Targets the Proximal Recon
6.5 mm Lag Screw
• A Targets the Distal Recon
6.5 mm Lag Screw
Antegrade Femoral Mode : Provides a
single 5mm Oblique Screw targeting
the lesser trochanter. LEFT is used for
a left nail and RIGHT for a right nail.
With the exception of the carbon
fi ber targeting device, dedicated
instruments for the recon mode are
color coded with “bronze”.
This makes it easy to differentiate
them from the core T2 instrument
platform.
Drills
Drillsfeaturecolorcodedrings:
4.2mm = Green
(Consistent with the Gamma3 and
T2 Instrument Plat form, this drill
features a green color ring.)
The 4.2mm drills are used for 5.0mm
Fully Threaded Locking Screws (either
for distal locking or for proximal
oblique locking).
6.5mm
The Solid Stepdrill for the Lag Screw
is color coded with “bronze”.
Targeting holes
for Recon Mode
B
A
Targeting holes
for Antegrade
Femoral Mode
Left
Right
7
Page 8
Indications, Precautions & Contraindications
Indications
The T2 Recon Nail is indicated for:
• Subtrochanteric fractures
• Intertrochanteric fractures
• Ipsilateral neck/shaft fractures
• Comminuted proximal femoral
shaft fractures
• Femoral fi xation required as a
result of pathological disease
• Temporary stabilization of
fractures of the femoral shaft ranging from the femoral neck to
the supracondylar regions of the
femur.
Precautions
Contraindications
The physician’s education, training
and professional judgement must
be relied upon to choose the most
appropriate device and treatment.
Conditions presenting an increased
risk of failure include:
• Any active or suspected latent
infection or marked local
infl ammation in or about the
affected area.
• Compromised vascularity that
would inhibit adequate blood
supply to the fracture or the
operative site.
• Bone stock compromised by
disease, infection or prior
implantation that can not provide
adequate support and/or fi xation
of the devices.
• Material sensitivity, documented
or suspected.
• Obesity. An overweight or obese
patient can produce loads on the
implant that can lead to failure
of the fi xation of the device or to
failure of the device itself.
Stryker Osteosynthesis systems have
not been evaluated for safety and use
in MR environment and have not been
tested for heating or migration in the
MR environment, unless specified
otherwise in the product labeling or
respective operative technique.
Antegrade Mode
Recon Mode
• Patients having inadequate tissue
coverage over the operative site.
• Implant utilization that would
interfere with anatomical
structures or physiological
performance.
• Any mental or neuromuscular
disorder which would create an
unacceptable risk of fi xation
failure or complications in
postoperative care.
• Other medical or surgical
conditions which would preclude
the potential benefi t of surgery.
8
Page 9
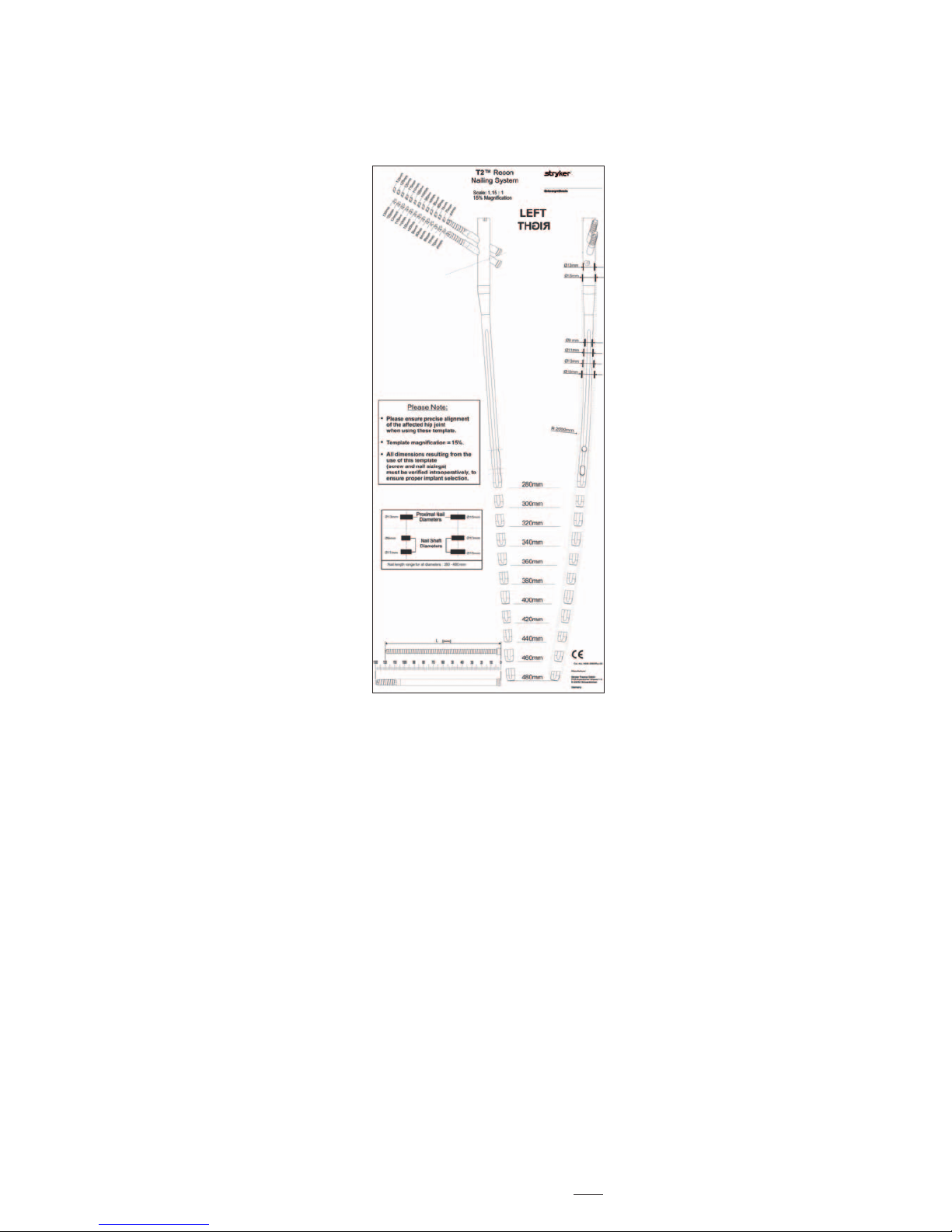
An X-Ray Recon Template (1806-3080)
is available for pre-operative planning.
Thorough evaluation of pre-operative
radiographs of the affected extremity
is critical. Careful radiographic
examination of the trochanteric
region and neck regions can reduce
the potential of intra-operative
complications.
Note:
TheX-RayReconTemplate
features a scale of 1.15:1 which
is adapted to conventional
analoguousX-Rays.Fordigital
X-Rays,attentionhastobe
paid that the magnification is
corresponding with the template.
According to the fracture type either
Recon or Antegrade Femoral Mode
can be chosen.
Evaluation of the femoral neck
angle on the pre-operative X-Rays is
mandatory as the T2 Recon Nail has a
fixed 125° neck angle for the two Lag
Screws. Proper placement of both Lag
Screws in the femoral head is essential.
If possible, X-Rays of the contralateral
side should be used to determine the
normal neck angle and length of the
femur.
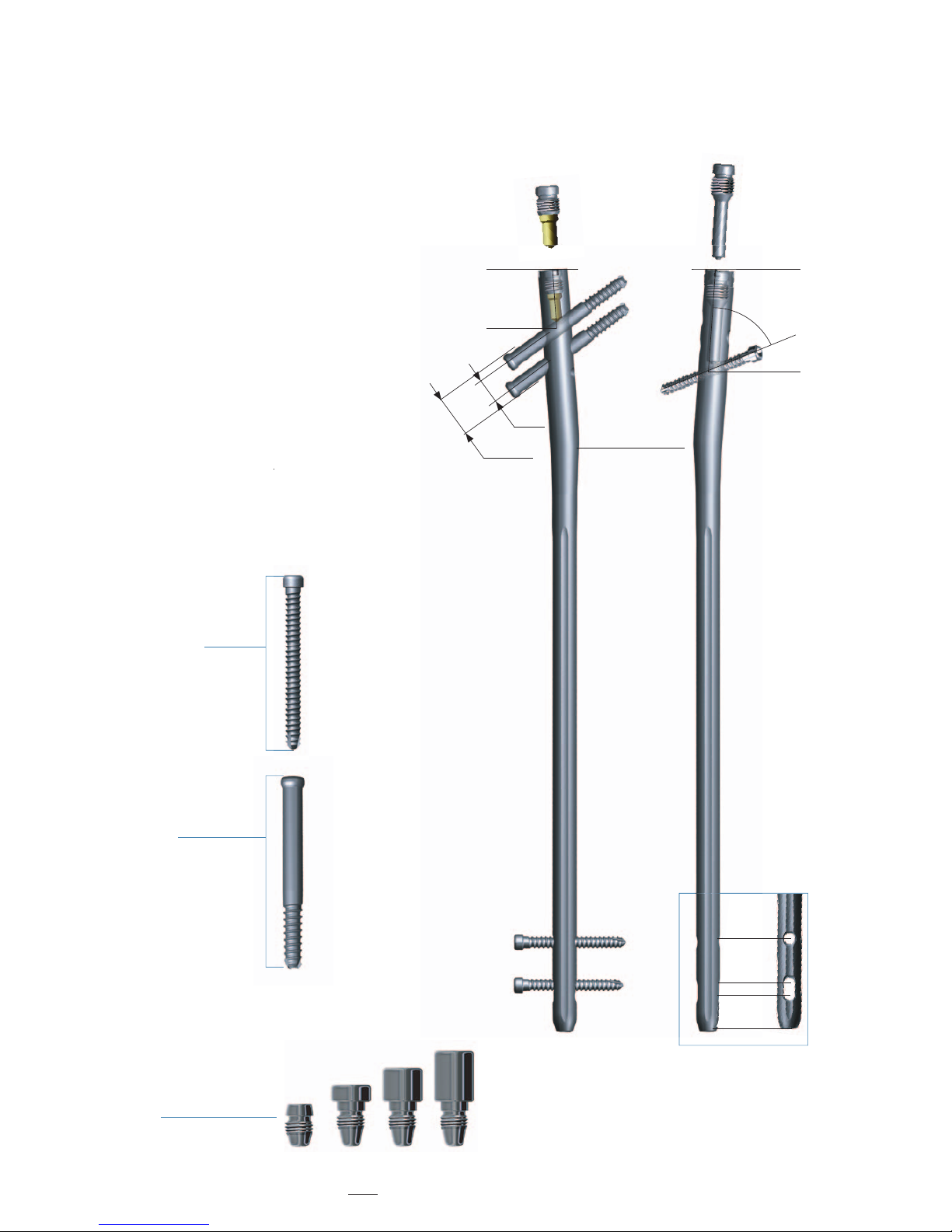
The proper nail length should extend
from the tip of the greater trochanter
to the epiphyseal scar.
Note:
Check with your local
representative regarding
availability of nail sizes.
Pre-Operative Planning
9
Page 10

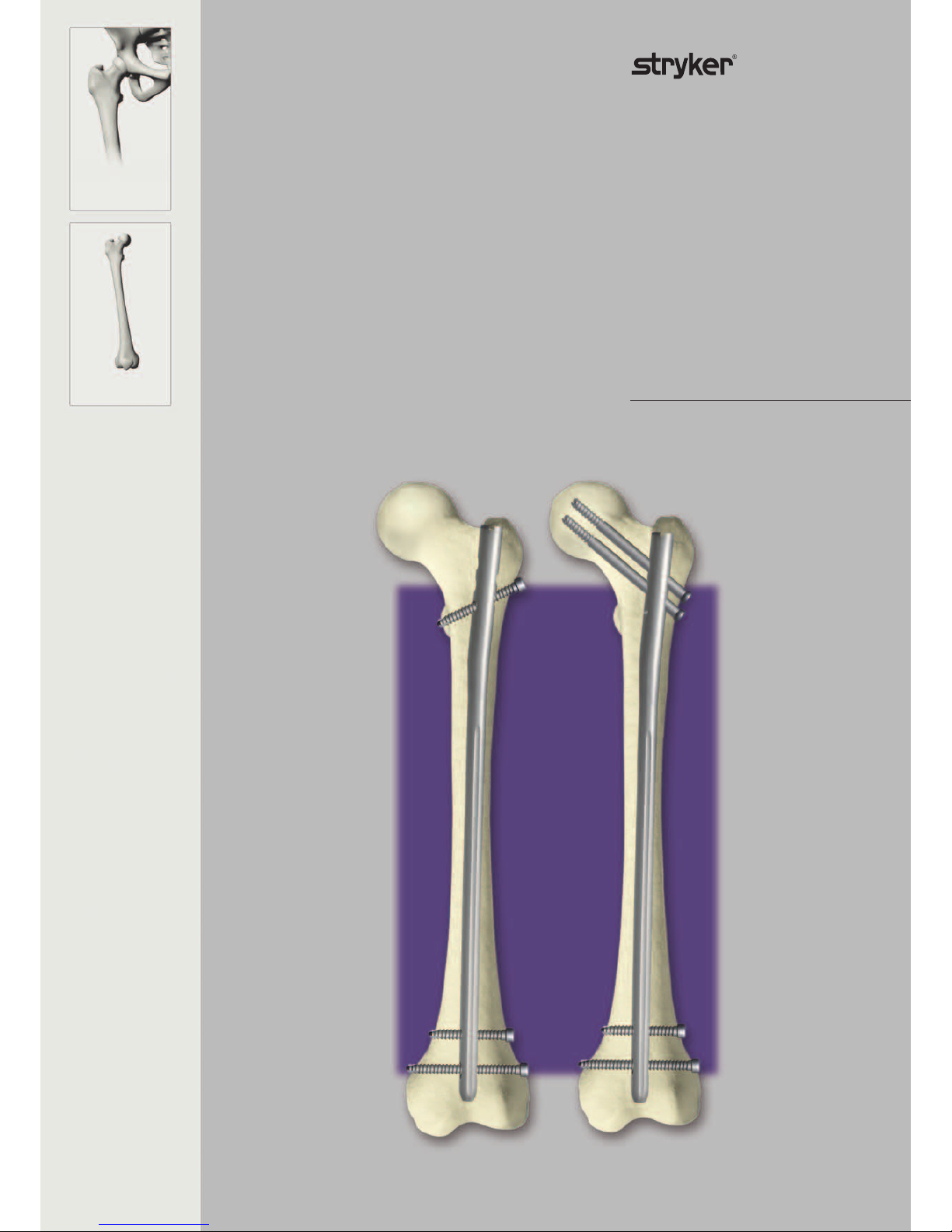
Locking Options
The T2 Recon Nail can be locked
proximally with two 6.5mm Lag
Screws (Recon Mode, Fig. 1) or with
one 5mm Fully Threaded Screw
(Antegrade Femoral Mode, Fig. 2).
For both Recon and Antegrade
Femoral applications, depending
on fracture pattern, either static or
dynamic distal locking can be used.
Fig. 1
Fig. 2
Recon Mode
Antegrade Femoral Mode
10
Page 11
Operative Technique
Fig. 3
Fig. 5
Fig. 4
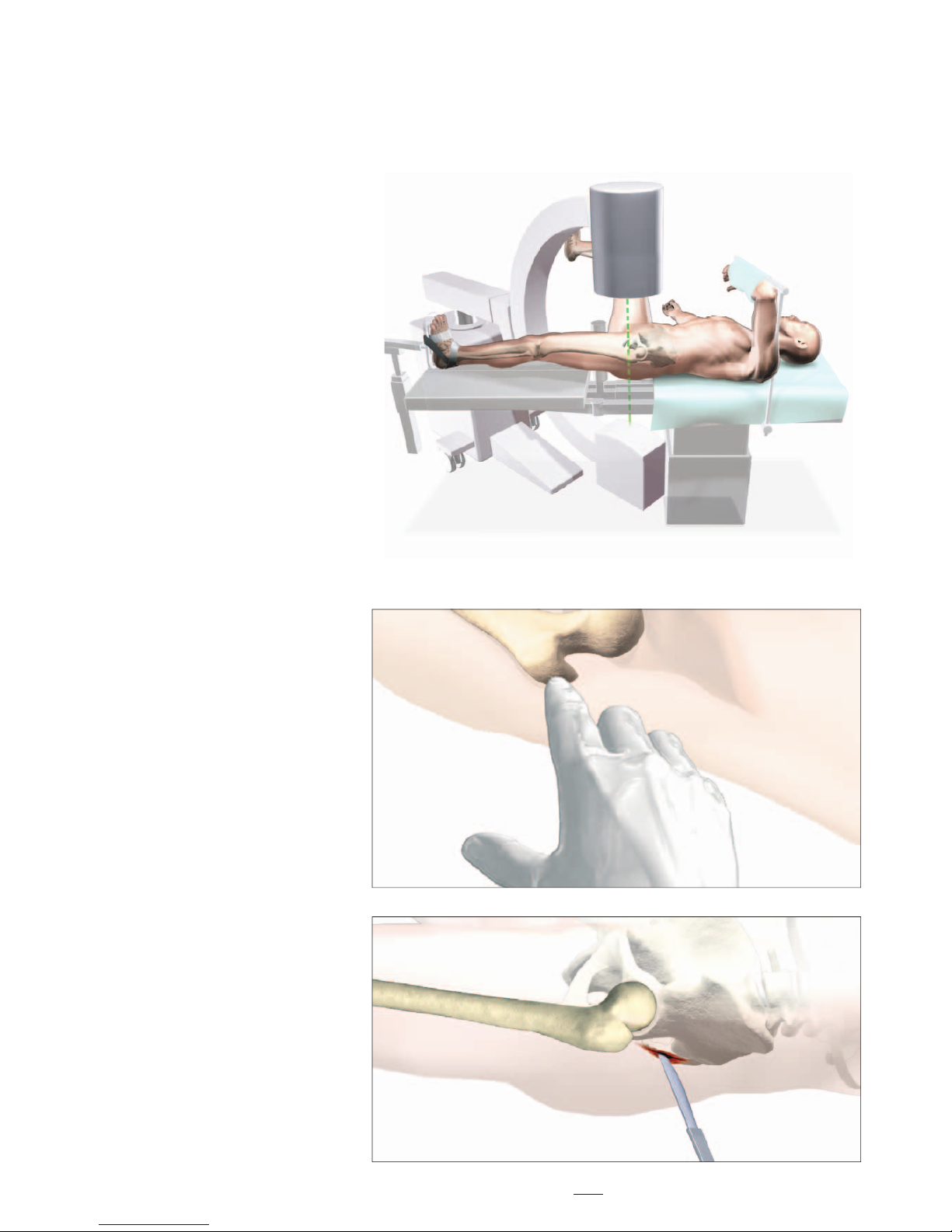
Patient positioning for T2 Recon
Nail insertion is surgeon dependent.
However, it is recommended that
patients are positioned in either the
supine or lateral position on a fracture
table to allow closed reduction of the
frac ture (Fig. 3).
Manipulate and reduce the fracture
in the usual fashion, according to the
fracture type. Reduction should be
achieved as anatomically as possible.
If this is not possible, reduction in
one plane should be complete, leaving
reduction in the other plane to be
achieved prior to reaming and nail
insertion.
The unaffected leg is abducted as far
as possible to ease image intensifi er
positioning. This will also allow easier
access to entry point.
Patient Positioning and Fracture Reduction
Incision
The design of the T2 Recon Nail, with
a 4° medial lateral bend, will only
allow for insertion through the tip of
the greater trochanter.
With experience, the tip of the greater
trochanter can be identifi ed by
palpation (Fig. 4).
A longitudinal skin incision of
approximately 3−5cm is made starting
just above the greater trochanter to the
iliac crest (Fig. 5). The incision is then
deepened to expose the tip of greater
trochanter.
Smaller or larger incisions may be
used based on individual patients
anatomy and at the surgeon’s
discretion.
Note:
The targeting instruments of the
T2ReconNailhavebeendesigned
to allow for a more percutaneous
approach.
11
Page 12
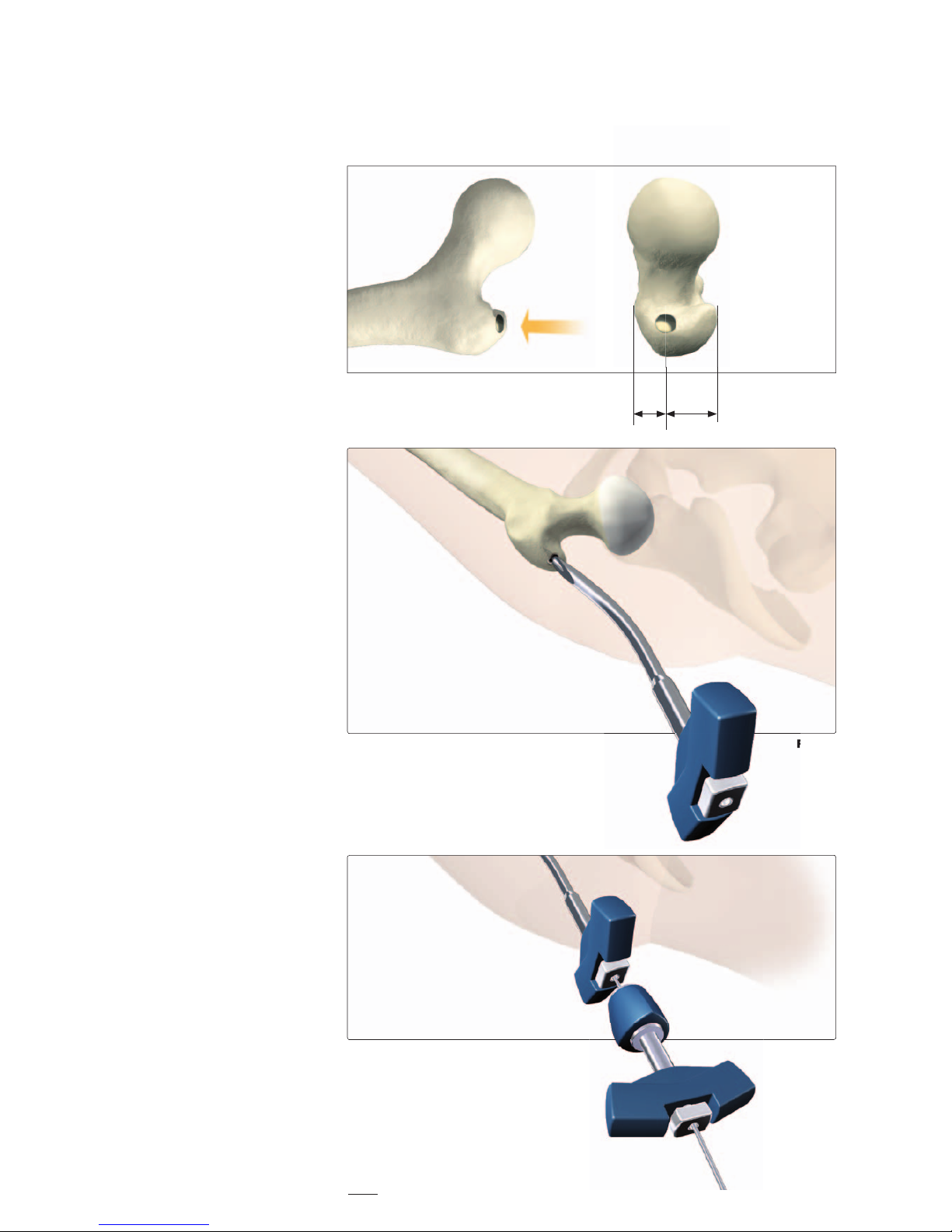
The entry point is located at the
junction of the anterior third and
posterior two-thirds of the greater
trochanter on the medial edge of the tip
itself (Fig. 6).
Note:
Before opening the tip of greater
trochanter, image intensifi er
views(A/PandM/L)should
be used to confi rm correct
identifi cation of the entry point.
The medullary canal can be opened
with the
• CurvedAwl/CurvedAwl,90°
Handle or
• OneStepConicalReamer.
Note:
Densecorticalbonemayblock
the tip of the Awl during opening
of the entry portal. Inserting
fi rst the optional Awl Plug into
the Awl will avoid penetration of
bone debris into the cannulated
Awl shaft. The Awl Plug is
thenremovedforGuideWire
insertion.
• Entry point with Curved Awl
Once the tip of the greater trochanter
has been opened (Fig. 7a), the
Ø3 × 1000mm Ball Tip Guide Wire
may be advanced through the
cannulation of the Curved Awl with
the Guide Wire Handle and Chuck
(Fig. 7 b).
The proximal femur may then be
prepared with the One Step Conical
Reamer.
anterior posterior
1
/
3
2
/
3
Fig. 6
Fig. 7a
Fig. 7b
Operative Technique
Entry Point
• The Tip of the
Greater Trochanter
Fig. 7a
12
Page 13
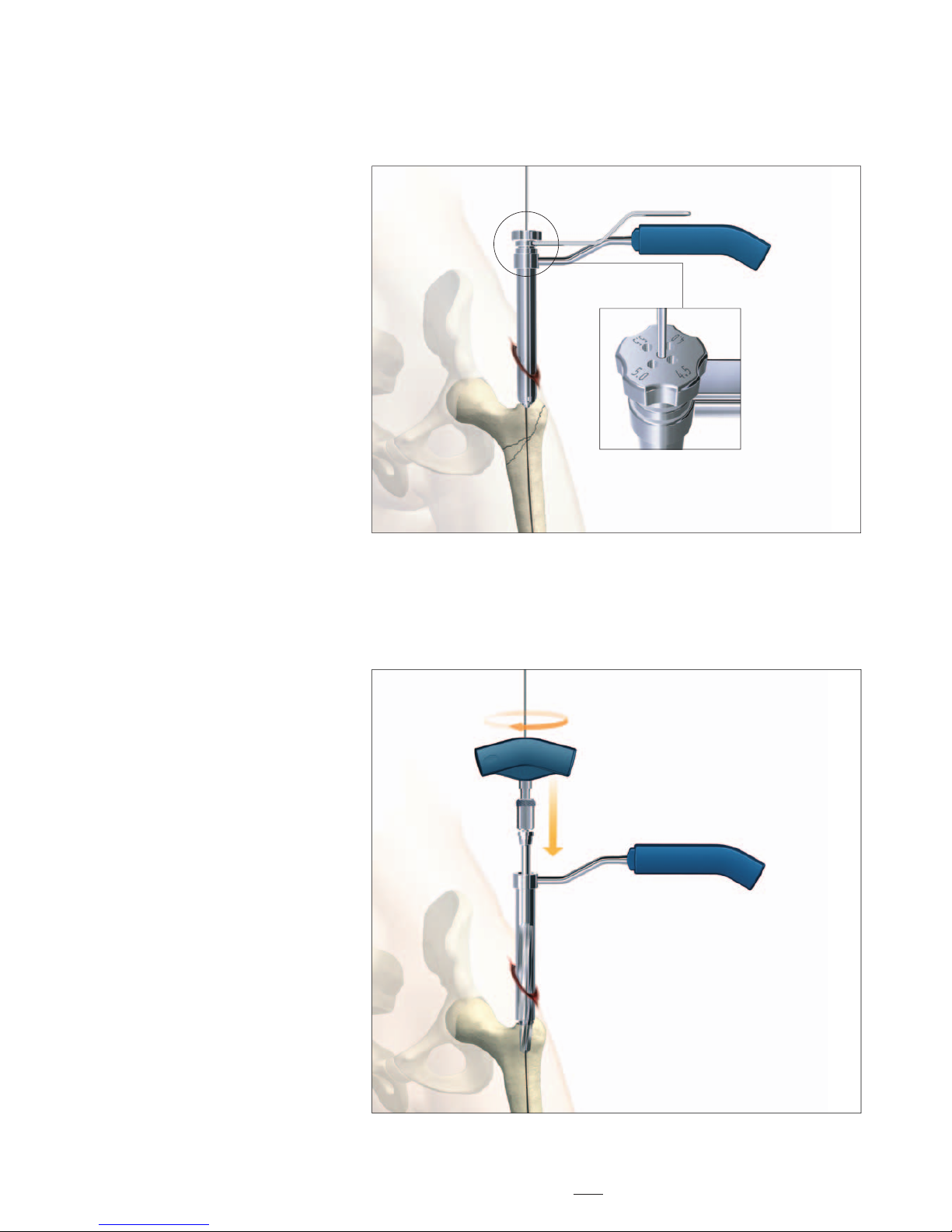
Fig. 9
Fig. 8
K-Wire
Fig. 8a
Operative Technique
• Entry point with
One Step Conical Reamer
Alternatively, the 13mm diameter
One Step Conical Reamer for the
9 and 11mm nails or the 15mm
diameter Reamer for the 13 and 15mm
nails may be used for opening the
medullary canal and reaming of the
trochanteric region.
Under image intensifi cation control,
the entry point is made with a
Ø3.2 × 400mm Recon K-Wire which
is attached to the Guide Wire Handle
and advanced into the medullary
canal. Confi rm its placement within
the center of the medullary canal
on A/P and lateral image intensifi er
views.
Note:
TheReconK-Wireusedforthe
entry point should not be used
again for the Lag Screw insertion.
It is recommended that a new
K-Wirebeutilized.
The Recon Protection Sleeve and
Multi-hole Trocar are positioned with
the central hole over the K-Wire.
Note:
The Multi-hole Trocar has a
special design for more precise
insertionoftheØ3.2mmRecon
K-Wire(Fig.8).Besidethecentral
hole, 4 other holes are located
eccentrically at different distances
from the center (Fig. 8a) to easily
revise insertion of the guiding
K-Wireintheproperposition
(entry point).
When correct placement of the guiding
Recon K-Wire is confi rmed on image
intensifi er views (A/P and lateral),
keep the Tissue Protection Sleeve
in place and remove the Multi-hole
Trocar.
The T-Handle is attached to the
One Step Conical Reamer and hand
reaming is performed over the Recon
K-Wire through the Tissue Protection
Sleeve (Fig. 9).
The Recon K-Wire is then removed
and replaced with the Ø3 × 1000mm
Ball Tip Guide Wire.
13
Page 14
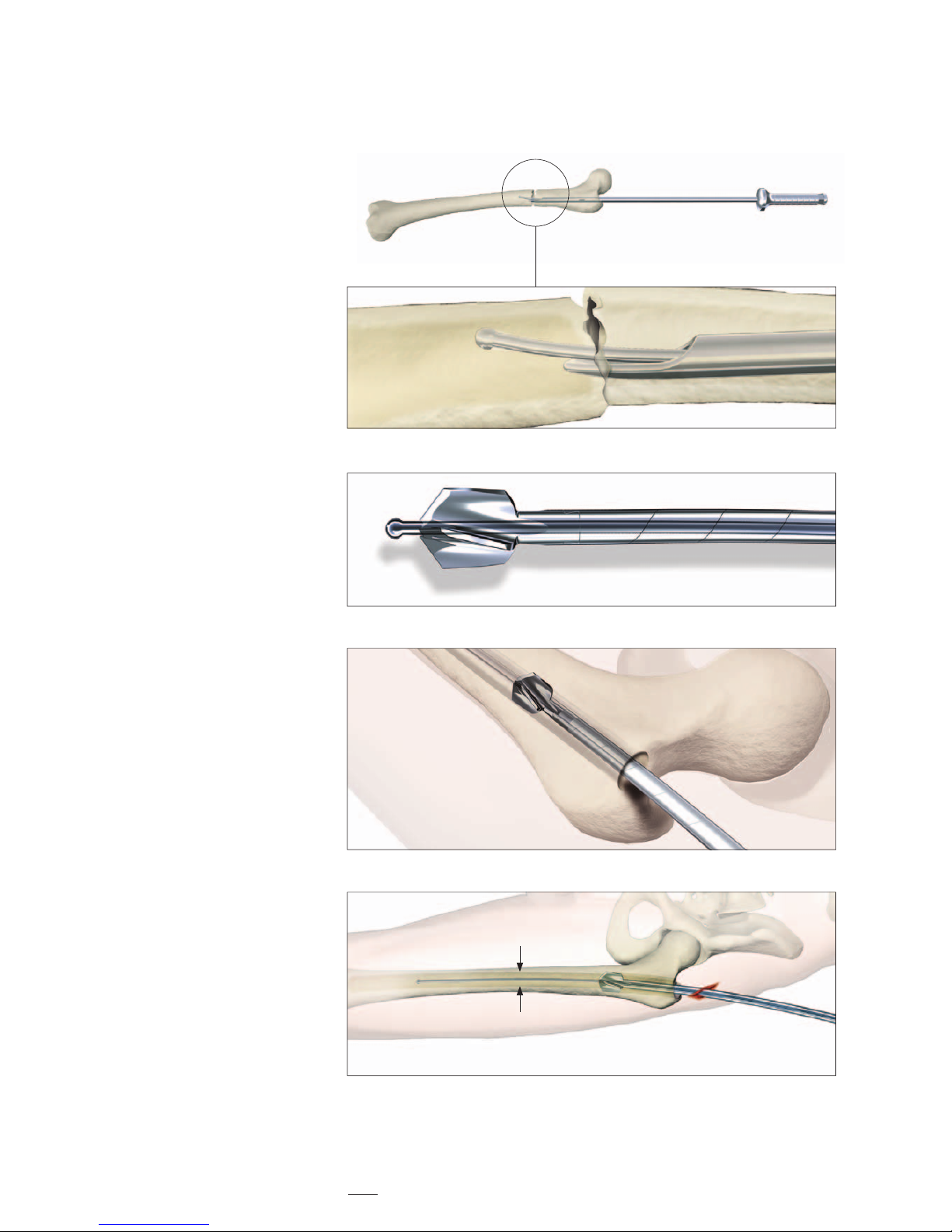
The Ø 3 × 1000mm Ball Tip Guide
Wire is inserted with the Guide
Wire Hand le throug h the frac tu re site
to the level of the epiphyseal scar.
The Ø 9mm Universal Rod with
Reduction Spoon may be used as a
fracture reduction tool to facilitate
Guide Wire insertion through the
fracture site (Fig. 10).
Note:
The Ball Tip at the end of the
GuideWirewillstoptheBixcut
reamer* head (Fig. 11).
Caution:
Prior to reaming, it is important
to check the centered
intramedullary position of the
GuideWirewiththeimagein-
ten sifi er. Lateral displacement
oftheGuideWirecouldleadto
resection of more bone on the
lateral side of the wire, which in
turn will lead to an offset position
of the nail and increase the risk of
a shaft fracture.
Note:
Make sure that the reduction
is maintained throughout the
reaming process.
Reaming is commenced in 0.5mm
in crements until cortical contact
occurs (Fig. 12).
For easier nail insertion, the
medullary canal should be reamed at
least 2mm more than the diameter of
selected nail (Fig. 13).
Fig. 10
Fig. 12
Fig. 13
Fig. 11
Operative Technique
Reaming
* see pages 36-37 for additiona l Bixcut Reamer
system details
+ 2mm more than the
selected nail diameter
14
Page 15

Note:
TheT2ReconNailmaybeinser-
ted without reaming of the
subtrochanteric and diaphyseal
region of the femur, particularly
in eldery patients with wide
medullary canals. If appropriate,
after the trochanteric region has
been prepared with the One Step
ConicalReamer,thenailcanbe
inserted without further reaming
of the medullary canal.
Operative Technique
The Guide Wire Pusher can be used to
keep the Guide Wire in position
during reamer shaft extraction. The
metal cavity at the end of the blue
Elastosil handle may be placed on the
end of Guide Wire. Applying pressure
to hold the Guide Wire in place while
removing the drill under power.
(Fig. 14).
When close to the Guide Wire end,
place the Guide Wire Pusher with its
funnel tip at the end of the power tool
cannulation (Fig. 15).
While removing the power tool the
Guide Wire Pusher will keep the
Guide Wire in place.
Guide Wire Pusher (1806- 0271)
Fig. 15
Fig. 14
Reaming of the trochanteric region is
needed (Fig. 13) as the proximal nail
diameter (driving end) is larger than the
nail diameter (13mm for the 9 and
11mm diameter nails and 15mm for
the 13 and 15mm diameter nails).
For both reamed or unreamed
applications, the proximal 5cm of the
trochanteric region must be opened to at
least 13mm or 15mm, depending on the
proximal diameter of the nail.
15
Page 16

Fig. 17a
Fig. 16a
Diameter
The diameter of the selected nail
should be at least 2.0mm smaller than
that of the last reamer used.
Length
Nail length may be determined by
measuring the remaining length of the
Guide Wire. The Guide Wire Ruler
may be used by placing it on the Guide
Wire and reading the correct nail
length at the end of the Guide Wire on
the Guide Wire Ruler (Fig. 16a, b).
Upon completion of reaming, the
appropriate size nail is ready for
insertion. A unique design feature
of the T2 Recon Nail is that the
Ø3 × 1000mm Ball Tip Guide Wire
does not need to be exchanged.
The selected nail is assembled onto the
Targeting Arm with the Nail Holding
Screw (Fig. 17a). Be sure to securely
tighten the Nail Holding Screw with
the Screwdriver Shaft, Ball Tip and
T-Handle so that it does not loosen
during nail insertion.
Caution:
Prior to the nail insertion,
check the correct assembly
by passing the Stepdrill for
LagScrewthroughtheRecon
Tissue Protection Sleeve and
DrillSleeve,Recon(placedin
the corresponding hole of the
Targeting Arm) and through the
holes of the nail (Fig. 17b).
For the Antegrade Femoral
Mode, use the targeting hole
for Antegrade with the Tissue
ProtectionSleeveandDrill
Sleeve assembly to pass the
Ø4.2×340mmDrillthroughthe
oblique hole of the nail.
Operative Technique
Nail Selection
Fig. 17b
Fig. 17a
Tissue Protection Sleeve and
DrillSleeve,Recon(placedin
the corresponding hole of the
Targeting Arm) and through the
holes of the nail (Fig. 17b).
For the Antegrade Femoral
Mode, use the targeting hole
for Antegrade with the Tissue
ProtectionSleeveandDrill
Sleeve assembly to pass the
Ø4.2×340mmDrillthroughthe
oblique hole of the nail.
Fig. 16b
End of Guide Wire Ruler
is measurement reference
16
Page 17

Fig. 18a Fig. 18b Fig. 18c
First, assemble the Knob to the Targeting Device by aligning the arrow on
the Knob with the white line on the
Target Sleeve, (Fig. 18a) then push
hard to click it.
By turning the Knob clockwise to the
position labeled (A), the sleeve inserted
in target (A) position, which is the
distal Recon Mode targeting hole, can
be locked. (Fig. 18b)
By further turning the Knob clockwise
to the position labeled (A+B), both
sleeves inserted in (A) and (B), which
are the both proximal and distal recon
mode targeting holes, can be locked.
(Fig. 18c)
Operative Technique
Assembly of Targeting Device
17
Page 18

Fig. 19
Operative Technique
The nail is advanced through the
entry point passing the fracture site to
the appropriate level.
If dense bone is encountered, fi rst
re-evaluate that suffi cient reaming
has been achieved, then, if necessary,
the Strike Plate can be attached to
the Targeting Arm and the Slotted
Hammer may be used to further insert
the nail (Fig. 19).
Caution:
The nail must progress smoothly,
without excessive force. If too
much resistance is encountered,
removal of the nail and additional
reaming is recommended.
Note:
RemovetheGuideWirepriorto
drillingorK-Wireinsertion.
The carbon fi ber guide should never
be struck as it may break or become
deformed. The impactor that is
provided can be utilized to assist with
fi nal seating of the nail. Gentle tapping
will produce small adjustments (in
the nail position) that can help to
optimize the ultimate position of the
lag screw in the femoral head. The nail
holding screw should be re-tightened
following any use of the impactor.
The impactor should not be utilized
to force the nail down the canal. If
the nail cannot be seated manually
or if there is no advancement each
time the impactor is tapped, A/P and
Lateral fl uoroscopic X-Rays should
be reviewed to determine the cause
of the impingement - there may be a
mismatch between the nail geometry
and the medullary canal. The starting
position, the femoral bow and the
canal diameter should all be examined
to ensure that the leading end of the
nail is not impinging on the medial
or anterior cortex and that the canal
itself has been suffi ciently reamed.
Nail Insertion
Final Seating with Impactor
Periodically, nail removal and further
reaming of the diaphysis may be
required.
The proximal metaphyseal fl air may
be undersized (particularly in young
patients or those of short stature) and
serve to prevent nail advancement. If
this situation is encountered, a fl exible
reamer may be used to further widen
this area to the level of the lesser
trochanter.
To facilitate manual passage, the
nail internally rotated 90° until the
fracture has been passed.
18
Page 19

Nail / La g S crews Posit ioning
Drive the T2 Recon Nail to the depth
that correctly aligns the proxi mal
screw holes parallel with the femoral
head and neck under fluoroscopic
control (Fig. 20) .
Two aspects regarding the Nail/Lag
Screws position must be carefully
checked with the image intensifier
before drilling into the femoral head:
- Alignment of the anteversion (M//L
view)
- Depth of nail insertion (A/P view).
The distal Lag Screw should run along
the calcar region (on the A/P view) and
centered into the femoral neck and
head (on the M/L view).
Note:
TheuseoftheOneShotDevice
(1213-3010) is recommended to
predetermine the optimal Lag
Screwplacement.Detailsare
described on Page 20 to 21.
Fig. 20
Fig. 20a
Operative Technique
Guided Locking for the Recon Mode
19
Page 20

Now attach the Recon Paddle Trocar
to the T-Handle, AO Medium
Coupling (Fig. 21).
Then, advance them together with the
Recon Tissue Protection Sleeve to the
skin through the hole on the Target
Device labeled (A). Make a small skin
incision and push the assembly
through until it is in contact with the
lateral cortex. Then turn the Knob
clockwise to the position labeled (A)
(Fig. 22).
Remove the Trocar and then insert the
Recon K-Wire Sleeve through the
Tissue Protection Sleeve. Place a Recon
K-Wire into the K-Wire Inserter and
attach it to the T-Handle.
The K-Wire is then man u ally
advanced through the K-Wire Sleeve
until it reaches the subchon dral bone
of the femoral head (Fig. 23).
Alternatively, the K-Wire Inserter can
be attached to a Power Tool and the
Recon K-Wire is inserted to the same
depth.
Fig. 22
Fig. 23
Fig. 21
Operative Technique
20
Page 21

Operative Technique
Note:
With the image intensifier, verify
iftheK-Wireisplacedalongthe
calcarregionintheA/Pview
and central on the lateral view
(correct anteversion) (Fig. 24).
If the K-Wire is incorrectly positioned,
the first step is to remove it and then
to correct the nail position.
More commonly, the nail is posi tioned
too proximal and correction of the
nail should be carried out either by
hand or by using the Strike Plate
placed into the Target Device. If a
higher position is required, the
Universal Rod and Slot ted Hammer
may then be at tached to the Strike
Plate to carefully and smoothly extract
the assembly (Fig. 25).
The new position is checked again
with the image intensifier as described
above.
Fig. 24
Fig. 25
21
Page 22

Nail/Lag Screws Positioning
with the One Shot Device
The use of the One Shot device
(1213-3010) is recommended to
predetermine the optimal Lag Screw
placement* (Fig. 26). The One Shot
Device is made of carbon fiber
and works by providing a target to
indicate the position of the K-Wire
on the fluoroscope screen. The
target contains 3 radio-opaque wires
embedded in the arm – a dashed inner
wire and two solid outer wires. These
wires work like a gun sight to indicate
the position of the K-Wire.
The One Shot Device is attached
by slightly pressing the grip and
releasing it when positioned onto the
Tissue Protection Sleeve. To correct
the position or remove the device, the
grip must be pressed.
Note:
TheuseoftheOneShotDevice
should not replace any steps in the
T2ReconOperativeTechnique.
While pressing the attachment grip,
the device is positioned between the
anterior aspect of the patient’s hip and
the fluoroscope screen positioned for
an A/P view of the hip (Fig. 26, 27).
Note:
It is important to drape the patient
so that the OneShotDevicedoes
not interfere with any drapes
anterior to the patient’s hip.
When positioned correctly, the target
will appear in the f luoroscopic image
(A/P view) with the dashed inner wire
in the middle of the two solid outer
wires (Fig. 27). If it does not, the One
Shot Device should be moved towards
or away from the patient by pressing
the grip slightly until the target is seen
as described above.
* Tokunaga et al, Correct lag screw positioning
for the Gamma Nail: Development for the
targeting device for inser tion, Osteo Trauma
Care 2005; 13:14-17
Operative Technique
Fig. 27
optimal nail position
too cranial nail position
A/Pview
too caudal nail position
Fig. 26
22
Page 23

Operative Technique
To identify the accurate position, the
dashed wire of the target must appear
between the two solid wires at the
desired position. If the position is
incorrect the T2 Recon Nail position
may be corrected by ei ther pulling
backwards or pushing forwards
(Fig. 28).
The K-Wire can then be placed into
the femur and the targeting arm
is held in place until the K-Wire’s
position in the lateral view has
been determined. When positioned
correctly, the target will appear in the
fluoroscopic lateral view (Fig. 29).
If the dashed wire of the target ap pears between the two solid wires,
then advance the Recon Tissue
Protection Sleeve and Trocar as shown
in Fig. 21.
Warn ing :
PriortoadvancingtheK-Wire,
check the correct guidance
throughtheK-WireSleeve.Do
notusebentK-Wires.
Note:
TheK-Wireinsertedintothemost
distal Lag Screw hole of the nail
helps in achieving the correct
positioning of the nail (depth and
rotation) with minimal resection
of bone in case correction of the
position is needed.
Lateral view
Fig. 2 9
Fig. 2 8
23
Page 24

Operative Technique
Solid Stepdrill Technique
For the insertion of proximal screws
in Recon Mode, the Solid Stepdrill
Technique, which is mentioned in this
chapter, is the recommended method
to optimize the proximal targeting
accuracy.
Attach the Recon Paddle Trocar to the
T-Handle, AO Medium Coupling as
demonstrated in Fig. 21. Then slide the
Tissue Protection Sleeve together with
the Paddle Trocar assembly to the
skin through the proximal target hole
labeled (B).
A small skin incision is made and the
assembly is pushed through until it
is in contact with the lateral cortex.
When the tip of the sleeve is in contact
with the lateral cortex, lock the sleeve
by turning the knob further to the
position labeled (A+B) (Fig. 30).
Then remove the Trocar assembly
and insert the Drill Sleeve for the
Recon Solid Stepdrill while the distal
K-Wire and K-Wire Sleeve are still
left in place. The Drill Sleeve for
the Recon Solid Stepdrill is inserted
through the proximal target hole
labeled (B) of the Targeting Device.
The Ø6.5mm Solid Stepdrill for Recon
Lag Screw is forwarded through the
Tissue Protection Sleeve and Drill
Sleeve assembly and pushed onto the
lateral cortex. There is a dedicated
Drill Sleeve for the Solid Stepdrill
Technique. This Sleeve is marked “Use
with Solid Step Drill“ as shown
(Fig. 31b).
Reaming is performed under
fluoroscopic control just until the tip
of the Solid Stepdrill for Lag Screw
reaches the subchondral bone. The
required length of the Lag Screw can
be read directly off the Recon Solid
Stepdrill for Lag Screw at the end of
the Drill Sleeve (Fig. 31a).
Fig. 31
Fig. 31a
Fig. 31b
Fig. 30
24
Page 25

Operative Technique
Using the Recon Screwdriver the
correct Lag Screw is inserted through
the Tissue Protection Sleeve and
threaded up to the subcondral part
of the femoral head. The screw is
near its proper seating position when
the groove around the shaft of the
screwdriver is approaching the end of
the Tissue Protection Sleeve (Fig. 32,
32a). The required length of the
second Lag Screw can be measured
using the Recon Lag Screw Gauge.
Remove the Distal K-Wire and K-Wire
Sleeve. Then insert the Sleeve for the
solid Stepdrill into the distal Tissue
Protection Sleeve.
Repeat the same surgical steps for
drilling and insertion of the distal Lag
Screw without K-Wire guidance.
After the completion of the distal Lag
Screw insertion, move on to the distal
locking procedure.
Fig. 32
Fig. 32 a
25
Page 26

Operative Technique
Alternatively, the K-Wire can be used
prior to drilling with the Solid Drill.
Place a second Recon K-Wire into the
K-Wire Inserter and attach it to the
T-Handle or power tool. The K-Wire
is then advanced through the K-Wire
Sleeve until it reaches the subchondral
bone of the femoral head.
Warn ing :
CorrectplacementoftheK-Wire
tip in subchondral bone must be
checked with image intensifier in
bothA/PandM/Lviews.
The required length of the Lag Screw
is measured using the Recon Lag
Screw Gauge.
Note:
Before starting to measure, ensure
that the Tissue Protection Sleeve
andK-WireSleeveassemblyis
firmly pressed against the lateral
cortex of the femur (Fig. 32b).
Take the Recon Lag Screw Gauge and
place it directly under the K-Wire
and against the K-Wire Sleeve (Fig.
32c). The correct Lag Screw length
corresponds to the measurement
indicated at the end of the K-Wire on
the Lag Screw Gauge.
After the measurement, remove the
K-Wire and drill the channel with the
Solid Stepdrill according to the Solid
Stepdrill technique described on
page 22.
Fig. 32 b
Fig. 32c
26
Page 27

Operative Technique
Fig. 35
Fig. 33
Fig. 34
The required length of the Lag Screw
is measured using the Recon Lag
Screw Gauge (1806-3035). Before
start ing to measure, ensure that the
Tissue Protection Sleeve and K-Wire
Sleeve assembly is fi rmly pressed
against the lateral cortex of the femur.
Take the Recon Lag Screw Gauge
and place it directly under the distal
K-Wire and against the K-Wire Sleeve
(Fig. 34).
As the Cannulated Stepdrill technique
was also discussed in a previous
version of the operative technique,
the insertion of the proximal screws
in Recon Mode using this method
will also be mentioned as a potential
option.
After achieving a satisfactory position
of the fi rst Recon K-Wire slide the
second Recon Tissue Protection Sleeve
together with the Recon K-Wire Sleeve
into the proximal target hole on the
Targeting Arm, labeled (B).
A small skin incision is made and the
assembly is pushed through until it
is in contact with the lateral cortex
(Fig. 33).
Place a second Recon K-Wire into the
K-Wire Inserter and attach it to the
T-Handle or power tool. The K-Wire
is then advanced through the K-Wire
Sleeve until it penetrates the
subchondral bone of the
femoral head.
Caution:
CorrectplacementoftheK-Wire
tip in subchondral bone must be
checked with image intensifi er in
bothA/PandM/Lviews.
Cannulated Stepdrill Technique
The correct Lag Screw length
corresponds to the measurement
indicated at the end of the K-Wire on
the Lag Screw Gauge. This length will
then be set on the cannulated Recon
Stepdrill for Lag Screw (Fig. 35).
27
Page 28

Operative Technique
Fig. 38
Caution:
Before proceeding with drilling
for the selected Lag Screw, check
theA/Pfluoroscopicviewsto
seeifthetwoReconK-Wiresare
parallel.
The distal K-Wire Sleeve is removed
while the Tissue Protection Sleeve
remains in position (Fig. 36a). The
cannulated Ø6.5mm Recon Stepdrill
for Lag Screw (REF 1806-3025)
is forwarded through the Tissue
Protec tion Sleeve and pushed onto
the lateral cortex. The stop on the
drill will only allow drilling up to
5mm before the K-Wire ends (Fig.
36b).
Warn ing :
Donotusethecannulated
ReconStepdrillforLagScrew
overadeflectedK-Wire.
Using the Recon Screwdriver, the
selected Lag Screw is inserted
through the Tissue Protection Sleeve
and threaded up to the subchondral
bone of the femoral head. The screw
is near its proper seating position
when the groove around the shaft of
the screw driver is approaching the
end of the Tissue Protection Sleeve
(Fig. 37).
Alternatively, the Recon Screwdriver
Shaft may be assembled into the
T-Handle and used for the Lag Screw
insertion.
The required length of the second
Lag Screw is measured using the
Recon Lag Screw Gauge. Repeat the
same surgi cal steps for drilling and
insertion of the proximal Lag Screw
(Fig. 38).
After the completion of the distal
Lag Screw insertion, move on to the
proximal locking procedure.
Fig. 36b
Fig. 36a
Fig. 37
28
Page 29

Operative Technique
Fig. 40
Now attach the Paddle Trocar,
Antegrade and the AO T-Handle
Medium Coupling (Fig. 39). Then,
advance them together with the Long
Tissue Protection Sleeve through
the targeting hole for the Antegrade
Femoral Mode (left or right) by
pressing the safety clip (Fig. 40). The
mecha nism will keep the sleeve in
place and prevent it from falling out.
It will also prevent the sleeve from
sliding during screw measurement. To
release the Tissue Protection Sleeve,
the safety clip must be pressed again.
A small skin incision is made and the
assembly is pushed through by manipulating the T-Handle until the Tissue
Protection Sleeve is in contact with the
lateral cortex (Fig. 41).
Guided Locking for Antegrade Femoral Mode
Fig. 41
Fig. 41
Fig. 39
29
Page 30

Pre-drilling the lateral cortex
Fig. 4 5a
65mm
65mm
Fig. 4 4
Fig. 4 5
Fig. 42
Fig. 4 3
Operative Technique
Pre-drilling opens the lateral cortex
for the drill entry. Pre-drilling helps
to prevent a possible slipping of the
drill on the cortex and may avoid
deflection within the cancellous bone.
The Paddle Trocar Assembly is
then removed and the Drill Sleeve
is inserted through the Long Tissue
Protection Sleeve (Fig. 42). With the
Long Tissue Protection Sleeve firmly
engaged in the cortex, the lateral
cortex should be opened using the
centered tip green coded 4.2mm Drill.
The Drill can be connected with
the AO Teardrop Handle Coupling
allowing pre-drilling by hand (Fig.
43). It also can be done using power.
Note:
For optimal stability, the tip
of the oblique screw should be
positioned at the level of the lesser
trochanter (Fig. 44).
Then use the center-tipped, calibrated
Ø4.2 × 340mm Drill and drill through
both cortices (Fig. 45).
The screw length may be read directly
from the Calibrated Drill at the end of
the Drill Sleeve (Fig. 45a).
Caution:
Start the drill before touching
the bone and then keep a gentle
pressure on the pre-dri lled c ortex
to ensure ac cu rate drilling.
Note:
The position of the drill end, as
it relates to the far cortex, is the
same position where the screw
will end.
30
Page 31

Operative Technique
Therefore, if the end of the Drill
is 3mm beyond the far cortex, the
end of the screw will also be 3mm
beyond (Fig. 46). Check the position
oftheendoftheDrillwithimage
intensification before measuring
the screw length. If the screw
measurement using the Long Screw
Gauge is preferred, first remove the
Long Drill Sleeve and read the screw
length directly at the end of the Long
Tissue Protection Sleeve.
Note:
• Before starting to measure,
ensure that the Tissue Protection
Sleeve/DrillSleeveAssemblyand
K-WireSleeveassemblyisfirmly
pressed against the lateral cortex
of the femur (Fig. 46, 47).
• TheLongScrewGaugeis
calibrated so that with the bend
at the end pulled back flush with
the far cortex, the screw tip will
end 3mm beyond the far cortex
(Fig. 47).
When the Drill Sleeve is removed,
the correct Locking Screw is inserted
through the Tissue Protection Sleeve
using the Long Screwdriver Shaft with
Teardrop Handle (Fig. 48). The screw
is ad vanced through both cortices.
The screw is near its proper seating
posi tion when the groove around the
shaft of the screwdriver is approach ing the end of the Tissue Protection
Sleeve (Fig. 48a).
Fig. 47
65mm
Fig. 46
Fig. 4 8
Fig. 4 8a
31
Page 32

The freehand technique is used to insert
Fully Threaded Locking Screws into
both distal transverse holes in the nail.
Rotational alignment must be checked
prior to locking the nail. This is
performed by checking a lateral view
at the hip and a lateral view at the
knee. The anteversion should be the
same as on the contralateral side.
Multiple locking techniques and
radiolu cent drill devices are available
for freehand locking. The critical step
with any freehand locking technique,
proximal or distal, is to visualize a
perfectly round locking hole with the
C-Arm.
The center-tipped ø4.2 × 180mm
Drill is held at an oblique angle to the
center of the locking hole (Fig. 49).
Upon X-Ray verification, the Drill is
placed perpendicular to the nail and
drilled through the lateral and medial
cortices (Fig. 50). Confirm in both the
A/P and lateral views by X-Ray that
the Drill passes through the hole in
the nail.
After drilling both cortices, the screw
length may be read directly off of the
Long Screw Scale at the green ring on
the center-tipped ø4.2 × 180mm Drill
(Fig. 51).
Alternatively, the Screw Gauge for
freehand technique can be used insted
of the Long Screw Scale to
determine the screw length.
Routine Locking Screw insertion
is employed with the assembled Long
Screwdriver Shaft and Teardrop Handle.
Note:
The Screwdriver Shaft can be used
in conjunction with the Long
Screw Capture Sleeve.
Operative Technique
Freehand Distal Locking
Fig. 49
Fig. 50
Fig. 51
Green Ring
32
Page 33

Operative Technique
Fig. 52
Repeat the locking procedure for the
insertion of the second 5mm Fully
Threaded Locking Screw into the
oblong hole in a static position
(Fig. 52).
The T2ReconNail may be used in the
dynamic locking mode. When the
fracture pattern permits, dynamic
lock ing may be utilized for transverse,
rotationally stable fractures. While
dynam ic locking can only be
performed at the end of the nail, this
will require a freehand distal targeting
of the oblong hole in a dynamic
position. This al lows the nail to move
and the fracture to settle while
torsional stability is maintained.
Note:
As an alternative for distal
locking, the guided distal
targeting system can be used. For
details, please refer to the separate
operativetechniques(Distal
TargetingSystemGamma3Long
NailR2.0,T2ReconnailR2.0)or
askStrykerRepresentativefor
further assistance.
Release the Nail Holding Screw using
the Screwdriver Shaft, Ball Tip and
T-Handle. Then remove the Targeting
Arm to complete surgery.
33
Page 34

End Caps
Stand ard +5mm +10mm +15mm
Operative Technique
After removal of the Target Device,
a Set Screw or End Cap can be used.
Two different Set Srews are available
(Fig. 53a):
- a ReconSetScrewto tighten
down on the Proximal Lag Screw
for the Recon Mode
- an Antegrade Set Screw to
tighten down on the oblique Fully
Threaded Screw for the Femoral
Antegrade Mode
Note:
If a Set Screw is used, an End Cap
can no longer be inserted.
Four different sizes of End Caps are
available to adjust nail length and to
reduce the potential for bony ingrowth
into the proximal thread of the nail
(Fig. 53b) .
The Set Screw or End Cap is inserted
with the Long Screwdriver Shaft and
Teardrop Handle after intra-operative
radio graphs confirm satisfactory
reduction and hardware implantation
(Fig. 54). Be sure to fully seat the End
Cap or Set Screw to minimize the
potential risk for loosening.
Nail Removal
The Set Screw or End Cap is removed
with the Long Screwdriver Shaft and
Tear drop Handle (Fig. 55).
The Universal Rod is inserted into
the driving end of the nail.
Alternatively, the Conical Extraction
Rod, can be attached to the Universal
Rod to facilitate extraction of the
nail. All 5mm Fully Threaded Locking Screws are removed with the
Screwdriver, Selfholding. The optional
Long Screw Capture Sleeve may be
used on the Screwdriver Shaft. For
removal of the Lag Screws, the Recon
Screwdriver or the Recon Screwdriver
Shaft and T-Handle are to be used.
The Slotted Hammer is used to ex tract
the nail in a controlled man ner (Fig. 56).
Set Screw or End Cap Insertion
Set Screw,
Antegrade
Set Screw,
Recon
Fig. 53b
Fig. 54
Fig. 55
Fig. 56
Fig. 53a
34
Page 35

Ordering Information – Implants
Titanium Diameter Length
REF mm mm
1846-0928S 9.0 280
1846-0930S 9.0 300
1846-0932S 9.0 320
1846-0934S 9.0 340
1846-0936S 9.0 360
1846-0938S 9.0 380
1846-0940S 9.0 400
1846-0942S 9.0 420
1846-0944S 9.0 440
1846-0946S 9.0 460
1846-0948S 9.0 480
184 6 -112 8S 11.0 280
184 6 -113 0S 11.0 30 0
184 6 -1132S 11.0 32 0
184 6 -113 4S 11. 0 34 0
184 6 -1136S 11.0 360
184 6 -1138S 11.0 380
184 6 -1140S 11.0 40 0
184 6 -1142S 11.0 420
184 6 -1144S 11.0 44 0
184 6 -1146S 11.0 46 0
184 6 -1148S 11.0 480
1846-1328S 13.0 280
1846-1330S 13.0 300
1846-1332S 13.0 320
1846-1334S 13.0 340
1846-1336S 13.0 360
1846-1338S 13.0 380
1846-1340S 13.0 400
1846-1342S 13.0 420
1846-1344S 13.0 440
1846-1346S 13.0 460
1846-1348S 13.0 480
1846-1528S 15.0 280
1846-1530S 15.0 300
1846-1532S 15.0 320
1846-1534S 15.0 340
1846-1536S 15.0 360
1846-1538S 15.0 380
1846-1540S 15.0 400
1846-1542S 15.0 420
1846-1544S 15.0 440
1846-1546S 15.0 460
1846-1548S 15.0 480
T2 Recon Nail, Left T2 Recon Nail, Right
Titanium Diameter Length
REF mm mm
1847-0928S 9.0 280
1847-0930S 9.0 300
1847-0932S 9.0 320
1847-0934S 9.0 340
1847-0936S 9.0 360
1847-0938S 9.0 380
1847-0940S 9.0 400
1847-0942S 9.0 420
1847-0944S 9.0 440
1847-0946S 9.0 460
1847-0948S 9.0 480
1847-1128S 11.0 28 0
1847-1130S 11.0 300
1847-1132 S 11.0 32 0
1847-1134S 11.0 340
184 7-1136 S 11 . 0 36 0
184 7-11 3 8S 11. 0 38 0
184 7-114 0 S 11.0 40 0
184 7-114 2 S 11 . 0 42 0
184 7-114 4 S 11.0 4 4 0
184 7-114 6 S 11.0 46 0
184 7-114 8 S 11 . 0 48 0
1847-1328S 13.0 280
1847-1330S 13.0 300
1847-1332S 13.0 320
1847-1334S 13.0 340
1847-1336S 13.0 360
1847-1338S 13.0 380
1847-1340S 13.0 400
1847-1342S 13.0 420
1847-1344S 13.0 440
1847-1346S 13.0 460
1847-1348S 13.0 480
1847-1528S 15.0 280
1847-1530S 15.0 300
1847-1532S 15.0 320
1847-1534S 15.0 340
1847-1536S 15.0 360
1847-1538S 15.0 380
1847-1540S 15.0 40 0
1847-1542S 15.0 420
1847-1544S 15.0 440
1847-1546S 15.0 460
1847-1548S 15.0 480
Note:
Check with your local representative regarding availability of nail
sizes.
35
Page 36

Ordering Information – Implants
Implants are in steri le pack aging.
Outside of the U. S., Locki ng Screws may be ordered
non-ster ile w ithout t he “S” at the end of the correspondi ng catalog number.
5mm Fully Threaded Locking Screws
6.5mm Lag Screws
Titanium Diameter Length
REF mm mm
1897-6065S 6.5 65
1897-6070S 6.5 70
1897-6075S 6.5 75
1897-6080S 6.5 80
1897-6085S 6.5 85
1897-6090S 6.5 90
1897-6095S 6.5 95
1897- 6100S 6 .5 100
1897- 6105S 6.5 10 5
1897-6110S 6.5 110
1897-6115S 6.5 115
1897-6120S 6.5 120
1897-6125S 6.5 125
1897-6130S 6.5 130
Titanium Diameter Length
REF mm mm
1847-0001S 8.0 Set Screw, Recon
1847-0003S 8.0 Set Screw, Antegrade
Titanium Diameter Length
REF mm mm
1822-0003S 8.0 Standard
1847-0005S 13.0 + 5mm
1847- 0010S 13.0 +10mm
1847-0015S 13.0 +15mm
Titanium
REF
1896-5025S
1896-5030S
1896-5035S
1896-5040S
1896-5045S
1896-5050S
1896-5055S
1896-5060S
1896-5065S
1896-5070S
1896-5075S
1896-5080S
1896-5085S
1896-5090S
1896-5095S
1896-5100 S
1896-5105S
1896-5110S
1896-5115 S
1896-5120S
5.0 25.0
5.0 30.0
5.0 35.0
5.0 40.0
5.0 45.0
5.0 50.0
5.0 55.0
5.0 60.0
5.0 65.0
5.0 70.0
5.0 75.0
5.0 80.0
5.0 85.0
5.0 90.0
5.0 95.0
5.0 100.0
5.0 105.0
5.0 110.0
5.0 115.0
5.0 120.0
End Caps Set Screws
DiameterLeng th
mm mm
Note:
Check with your local representative regarding availability of nail
sizes.
36
Page 37

REF Description
Ordering Information – Instruments
**Caution:
The coupling of Elastosil handles contains
a mechanism with one or multiple ba ll
bearings. In case of applied a xial stress on
the Elastosil handle, those components
are pressed into t he surrounding cyl inder
resulting in a complete blockage of t he
device and possible bending.
To help avoid intra- operative complications and promote long-term functionality, we mandate that Elastosi l handles be
usedonlyfortheirintendeduse.DONOT
HITthem.
*** item s a r e part of T2 B a si c L on g In s t rument
set (1806-9901); however, not used for
T2ReconNailingsurgery
T2 Basic Long
Teardrop Hand le, AO Coupling**
Protection Sleeve, Retrograde***
Guide Wire Ruler
Awl Plug
Awl
Universal Rod
Reduction Spoon
Wrench 8mm/10mm
Ins er tion Wrench, 10mm***
Stri ke Plate
Slotted Hammer
Tissue Protection Sleeve, Long
Screwdriver, Self-Holding, Extra Short (3.5)
Drill Sleeve, Long
Screwdriver Sha ft AO, Long
Screwdriver, Self-Holding, Long (3.5)
Screwdriver Shaft, Compression (hex3.5)***
Guide Wire Pusher
Trocar, Long***
Screw Gauge, Long
Screw Gauge (20-120mm)
Extraction Rod, Conical (Ø8mm)
Screw Scale, Long
Guide Wire Handle
Guide Wire Handle Chuck
Rigid Rea mer Ø12mm***
T2 Basic Long Inst rument Tray
T2 Basic Long Inst rument Set,
Completely f illed
702429
703165
1806- 0 022
1806- 0 032
180 6-0 041
180 6 -0110
1806- 0125
1806- 013 0
1806- 0135
1806- 015 0
1806-0170
1806- 0185
1806- 0203
1806- 0215
1806- 0227
1806- 0233
1806- 0268
1806- 0271
180 6 - 0315
1806- 0325
180 6 - 0331
1806- 0350
1806- 0365
180 6 -1095
180 6 -1096
180 6 -2014
1806-9900
1806-9901
37
Page 38

Ordering Information – Instruments
180 6 -310 0
180 6-3101
1806-3005
1806-3010
1806-3015
1806-3026S
1806-3030S
180 6-30 31S
1806-3035
1806-3040
1806-3041
1806-3045
1806-3050
1806-3055
1806-3057
1806-3060
1806-3070
1806-3090
1806- 0294
1806-4290S
1806- 4260 S
1806- 4270S
1806- 8018S
Target Device
Knob for Target Device
Nail Holding Screw, Recon
One Step Conical Reamer Ø13, Recon
One Step Conical Reamer Ø15, Recon
Solid Stepdri ll for Lag Screw*
Recon K-Wire, Recon*
K-Wire, Recon, CoCr
Lag Screw Gauge, Recon
K-Wire Sleeve, Recon
Dril l Sleeve for Solid Stepdri ll
Tissue Protection Sleeve, Recon
Screwdriver Sha ft, Recon
Multihole Trocar
Protection Sleeve, Antegrade
Screwdriver, Recon
K-Wire Inserter
Screwdriver Sha ft, AO, Ball Tip
Screwdriver Sha ft, Self holding, 3.5 × 85mm
Dril l Ø4.2 × 230 mm, AO*
Dril l Ø4.2 × 34 0mm, AO*
Dril l Ø4.2 × 180m m, AO*
Drill Ø4.2 × 250mm , oblique AO*
* For non-sterile, leave “S” off the REF number
when ordering.
REF Description
T2ReconInstruments
38
Page 39

REF Description
Optional Instruments
REF Description
Spare Parts
Ordering Information – Instruments
1806-0040
1806-3025
1806-0240
1806- 0292
1806-0480
1806-9993
1806-9992
1806-9995
1806-9996
1320-5375
Awl, Cu r ved
Stepdrill for Lag Screw, Recon
Screw Capture Sleeve, Long
Screwdriver Sha ft, 3.5 x 85mm
Screw Gauge, Femur
T2 Recon Instrument Tray Insert
T2 Recon Silicone Mat Free Space
T2 Recon Drill Rack
T2 Recon Insert for Reamer Heads****
DTS Tray Calibration Stand
* For non-sterile, leave “S” off the REF number
when ordering.
**Caution:
The coupling of Elastosil handles contains
a mechanism with one or multiple ba ll
bearings. In case of applied a xial stress on
the Elastosil handle, those components
are pressed into t he surrounding cyl inder
resulting in a complete blockage of t he
device and possible bending.
To help avoid intra- operative complications and promote long-term functionality, we mandate that Elastosi l handles be
usedonlyfortheirintendeduse.DONOT
HITthem.
**** Bixcut Modular Head 9, 10, 11, 12, 13, 14,
15, 16, 17 and 2 additional Modular Heads
can be stored. See page 37 for details.
1213-3010
702628
1806-3065
1806- 0085S
1806-3047
1806-3048
1806-3080
1806-9990
1806-9991
One Shot Device
T-Handle, AO Medium Coupling**
Extraction Screwdriver
Guide Wire, Ball Tip, Ø3 × 1000mm, steri le*
T2 Paddle Trocar Recon Mode
T2 Paddle Trocar Antegrade Mode
X-Ray Template, Recon
T2 Recon Instrument Tray
T2 Recon Instrument Set,
completely f illed
REF Description
T2ReconInstruments
39
Page 40

Complete range of modular and
fixed-head reamers to match
surgeon preference and optimize
O.R.efficiency,presentedinfully
sterilizable cases.
Studies
1
have demonstrated that
the pressures developed within
the medullary cavity through the
introduction of unreamed IMnails can
be far greater than those devel oped
during reaming − but this depends
very much upon the design of the
reamer.
After a three year development study2
involving several universities, the
factors that determine the pressures
and temperatures developed during
reaming were clearly established.
These factors were applied to the de velopment of advanced reamers that
demonstrate significantly better per form ance than the best of previous
designs3.
1
Ja n Paul M. Frolke, e t al. ;
Intramedullary Pressure in Rea med Femor al
Nail ing with Two Different Rea mer Designs.,
Eur. J. of Trauma, 2001 #5
2
Medhi Moussavi, et al.;
Pressure Changes Duri ng Reaming w ith Di fferent
Parameters a nd Reamer Designs,
Clinical Orthopaedics a nd Related Research
Number 373, pp. 295-303, 2000
3 Andrea s Speit ling;
Intra medul lar y Reamers, commented slides of
internal test repor t, Sep 1999
Large c learance rate resulting f rom reduced number
of reamer blades coupled with reduced length of
reamer head to allow for ef fect ive relief of pressure
and effi cient removal of materia l
3
.
Cutti ng fl ute geometry optimized to lower pressure
generation
3
.
Forwa rd- and side-cut ting face combination produces
effi cient material removal and rapid clearance
3
.
Double-wound shaf t tra nsmits torque effectively a nd
with h igh reliabi lity. Low-fric tion surface fi nish aids
rapid debris clea ranc e
3
.
Smal ler, 6 and 8mm shaf t diameters a re designed to
reduce IM pressure.
Typical Standard
Ream erØ14 mm
Clea ra nc e are a :
32% of cross section
Bixcut
Ream erØ14 mm
Clea ra nc e are a :
59% of cross sec tion
Ordering Information – Instruments
Bixcut
Bixcut
40
Page 41

REF Description Diameter
mm
BIXCUT MODULAR HEAD
REF Diameter Length
mm mm
BIXCUT FIXED HEAD − AO FITTING**
REF Description Length
mm
BIXCUT SHAFTS (STERILE)
1,2, 3, 4
REF Description
SHAFT ACCESSORIES
REF Description
BIXCUT TRAYS EMPTY
Ordering Information – Instruments
REF Description
OPTIONAL INSTRUMENTS
0227- 0060 Hand Reamer 6 mm
w/Mod Trinkle connection
0227-0070 Hand Reamer 7 mm
w/Mod Trinkle connection
0227-0080 Hand Reamer 8 mm
w/Mod Trinkle connection
0227-0090 Hand Reamer 9 mm
w/Mod Trinkle connection
1806-6520 Curved Reduction Rod 8.5 mm
w/Mod Trinkle connection
1806- 6500 T-Handle w/Mod Trink le connection
0226-3090
0226-3095
0226 -3100
0226-3105
0226 -3110
0226 -3115
0226 -3120
0226 -3125
0226 -3130
0226-3135
0226 -3140
0226 -3145
0226 -3150
0226-3155
0226 -3160
0226 -3165
0226 -3170
0226 -3175
0226 -3180
022 6-4185
0226 -4190
0226 -4195
0226-4200
0226-4205
0226- 4210
0226- 4215
0226-4220
0226-4225
0226-4230
0226-4235
0226-4240
0226-4245
0226-4250
0226-4255
0226-4260
0226-4265
0226-4270
0226-4275
0226-4280
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
Bixcut Head
9.0
9.5
10.0
10.5
11.0
11.5
12.0
12.5
13.0
13.5
14.0
14. 5
15.0
15.5
16.0
16.5
17.0
17. 5
18.0
18.5
19.0
19.5
20.0
20.5
21.0
21.5
22.0
22.5
23.0
23.5
24.0
24.5
25.0
25.5
26.0
26.5
27. 0
27. 5
28.0
0227-8240S Mod. Trink le 284
0227-3000S Mod. Trink le 448
0227-8 510S Mod. Tri n k le 510
0227-8885S Mod. Trinkle 885
0226-8240S AO 284
0226-3000S AO 448
0225-6000 Tray, Modular Head
(up to size 22.0mm)
0225-6001 Tray, Modular Head
(up to size 28.0mm)
0225-8000 Tray, Fixed Head
(up to size 18.0mm)
0225-6040 Mini Trauma Tray
(for modular heads 9-18)
0225-6050 Mini Revision Tray
(for modular heads 9-28)
0225-5060
0225-5065
0225-5070
0225- 6075
0225-6080
0225-6085
0225-6090
0225-6095
0225- 6100
0225-6105
0225 -6110
0225 -8115
022 5-8120
0225-8125
022 5-813 0
0225-8135
0225 -8140
0225 -8145
022 5-815 0
0225-8155
0225-8160
0225-8165
022 5-8170
022 5-8175
022 5-8180
6.0*
6.5*
7.0 *
7.5
8.0
8.5
9.0
9.5
10.0
10.5
11.0
11.5
12.0
12.5
13.0
13.5
14.0
14. 5
15.0
15.5
16.0
16.5
17.0
17. 5
18.0
400
400
400
480
480
480
480
480
480
480
480
480
480
480
480
480
480
480
480
480
480
480
480
480
480
3212-0-210 Grommet (pack of 25)
3212-0-220 Grommet inserter/extractor
0225-6010 Grommet Case
Note:
Bixcut Fi xedHead−ModiedTrinkletting available in same diameters and leng th as the
AOFitting(REFNo :0227-xxxx)
* Use with 2.2mm × 800mm Smooth Tip and 2.5mm × 800mm Ball Tip Guide Wires only.
**
Use with Stryker power equipment.
1. Non-Sterile shafts supplied without Grommet. Use new Grommet for each surgery. See shaft
accessories.
2. Sterile shafts supplied with grommet pre-assembled.
3. For non-sterile leave “S” off the REF Number when ordering (510 and 885mm available only sterile
Modified Trinkle Fitting).
4. non-sterile, AO Fitting Shafts in 510 and 885mm are available as build to order items:
• CM810921 AO Fitting Shaft, length 510mm
• CM810923 AO Fitting Shaft, length 885mm.
41
Page 42

Notes
42
Page 43

Notes
43
Page 44

Manufactured by:
Stryker Trauma GmbH
Prof.-Küntscher-Strasse 1-5
D-24232 Schönkirchen
Germany
www.osteosynthesis.stryker.com
This document is intended solely for the use of healthca re professional s. A surgeon must a lways rely on his or her own
professional cl inical judg ment when deciding whether to use a par ticular product when treating a particular patient .
Stryker does not dispense medica l advice and recommend s that surgeon‘s be trained in the use of any part icular
product before usi ng it in surgery. The information presented in this brochure is intended to demonstrate a Str yker
product. Alway s refer to the package ins ert, product label and /or user inst ructions includi ng the instr uctions for
Clean ing and Steri lization (if applicable) before u sing any Stryker products. Product s may not be available in a ll
markets. Product ava ilabilit y is subject to the regulatory or medical prac tices that govern ind ividual markets. Please
contact your Stryker representative if you have question s about the avai lability of St ryker products in you r area.
Stryker Cor poration or its divisions or other corporate af filiated ent ities own, use or have applied for the followi ng
trademarks or serv ice marks : Bixcut, Gam ma, Gamma3, Stryker, T2. A ll other trademark s are trademarks of their
respec tive owners or holders.
The produc ts listed above are CE ma rked.
Literat u re Num be r : B1000 084Re v1
1/11
Copyright © 2011 Stryker
 Loading...
Loading...