

Page 1

SC 7000 and SC 9000XL Patient Monitors
Service Manual
E331.E539U.719.10.01.02
ASK-T898-03-7600
EM Guidelines, 1997 -04-02
Page 2
Page 3

SC 7000 and SC 9000XL Patient Monitors Service Manual
ADVISORY
Siemens is liable for the safety of its equipment only if maintenance, repair, and modifications are performed
by authorized personnel, and if components affecting the equipment's safety are replaced with Siemens
spare parts.
Any modification or repair not done by Siemens personnel must be documented. Such documentation must:
• be signed and dated
• contain the name of the company performing the work
• describe the changes made
• describe any equipment performance change s.
It is the responsibility of the user to contact Siemens to determine warranty status and/or liabilities if other
than an authorized Siemens technician repairs or makes modifications to medical devices.
ASK-T898-02-7600 Siemens Medical Systems, EM-PCS Danvers
apolotmfr5_5.advisory.fm/07-98/kaupp
Page 4

Service Manual SC 7000 and SC 9000XL Patient Monitors
Siemens Medical Systems, EM-PCS, Danvers ASK-T898-02-7600
apolotmfr5_5.Advisory.fm/07-98/kaupp
Page 5
7DEOH RI &RQWHQWV
ADVISORY
Chapter 1: General Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2 O v erview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2.1 R50 Recorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2.2 Infinity Docking Station . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2.3 Docking Station (Discontinued) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2.4 InfinityNet CPS (Discontinued) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.5 Remote Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.5.1 Passive Remote Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.5.2 Keypad . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.5.3 SC 9015 (Discontinued) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.6 PSL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
2.7 Interface Plate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
3 S ervice Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
4 Related Documentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
5 Cleaning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
6 Te chnical Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
7 Brief Operating Instructions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
7.1 SC 7000 and SC 9000XL Monitor Controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
8 P eripheral Device Controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
9 P asswords . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
9.1 Clinical Password . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
9.2 Service Password . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
10Menus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
10.1Main Menu . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
10.2Service Menu . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
10.3Install Monitoring Software . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
10.4Configuration Download Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
10.5Diagnostic Log Upload Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Chapter 2: Theory of Operation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Figure 2-1 SC 7000 / SC 9000XL Bus Structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1.1 Main Processor Bus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.2 Front End Bus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers i
7k9kXLSM.book.CD_ROMTOC.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 6

Service Manual SC 7000 and SC 9000XL Patient Monitors
1.3 REMOTE COMM Bus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Figure 2-2 REMOTE COMM Bus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.4 Error Handling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2 Main Unit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Figure 2-3 SC 7000 / SC 9000XL Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.1 Front Bezel Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.2 Cooling System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.3 Real Time Clock . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.4 Non-volatile Memory Battery Backup and Power Reset . . . . . . . . . . . . . . . . . . . . . . . . 10
2.5 MPC 860 Communication Channels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.6 Device CPS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.7 Infinity Docking Station . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.8 etCO2 cartridge . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.9 External Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.10Interfaces . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.10.1 Local Fixed Keys Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.10.2 Local Rotary Knob Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.10.3 SC 9015 Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.10.4 Fast Analog Output . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.10.5 HiFi Audible Alarm Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.10.6 LED/Statu s Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.10.7 QRS Sync Out Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.10.8 Local Alarm Out Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.10.9 Remote Alarm Out Interface for Nurse Call . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.11Recorder Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
2.12Backlight Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
2.13Serial EEPROMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3 G raphics Subsystem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 2-4 Graphics Subsystem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1 Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.2 Functional Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.3 Video Output . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
4 DSP Subsystem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Figure 2-5 DSP Subsystem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
5 P O D COM Subsystem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Figure 2-6 POD Communications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
ii Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM.book.CD_ROMTOC . fm/0 4-99/k aupp
Page 7

SC 7000 and SC 9000XL Patient Monitors Service Manual
5.1 Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
5.2 Outputs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
5.3 Error Handling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
6 P ow er Conversion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Figure 2-7 Power Conversion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
6.1 Power Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
6.1.1 Power Buss . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
6.1.2 Control and Load Sequencing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
6.1.3 Power On / Off . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
6.1.4 Power Source Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
6.1.5 Battery charging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
6.1.6 Indicator LEDs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Table 2-1Power and Charger LED Indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
6.1.7 Power Mode Indication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Table 2-2 Power Mode Table . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
6.1.8 Piezo Alarm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Table 2-3Piezo Alarm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
6.1.9 Fault Protection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
6.1.10 External Pod and Cartridge Overload Protection . . . . . . . . . . . . . . . . . . . . . . . 18
6.2 Electrical Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
6.2.1 Power Supply Input . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
6.3 System Power Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
6.3.1 Maximum Power Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
6.3.2 Main Battery Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
6.3.3 External Battery Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
7 Front Bezel Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
7.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
7.2 Functional Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
7.3 LCD Backlight Invertor Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
7.4 Ambient Light Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
7.5 Local Rotary Knob/fixed Keys Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
7.6 Battery/power LED Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
8 MultiMed Front End . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
8.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
8.2 Safety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Figure 2-8 MultiMed Front End . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers iii
7k9kXLSM.book.CD_ROMTOC.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 8

Service Manual SC 7000 and SC 9000XL Patient Monitors
8.3 Functional Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
8.3.1 ECG/Resp . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Table 2-4Parameter Sampling Table . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Figure 2-9 Lead Forming Network . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Figure 2-10 Respiration Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
8.3.2 Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Figure 2-11 Temperature Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
8.3.3 SpO2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Figure 2-12 SpO2 Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
9 NBP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Figure 2-13 NBP Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
9.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
9.2 Pneumatic Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
9.3 Transducers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
9.4 Pneumatic Controls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
9.5 Safety timer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
9.6 Logic gate array . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
9.7 Non-volatile memory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
9.8 Hose detection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
9.9 Watchdog Timer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
10HemoMed Front End . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Figure 2-14 HemoMed Front End . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
10.1Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
10.2Pressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
10.3Cardiac Output . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
11etCO2 Module . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Figure 2-15 etCO2 Sensing Process Functional Block Diagram . . . . . . . . . . . . . . . . . . . 29
11.1System Hardware . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 0
11.2System Memory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
11.3User Interface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
12HEMO 2/4 POD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
12.1Functional Description . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
12.2Pressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Figure 2-16 HEMO 2/4 POD Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Figure 2-17 IBP Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
12.2.1 Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
12.2.2 Cardiac Output . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
iv Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM.book.CD_ROMTOC . fm/0 4-99/k aupp
Page 9

SC 7000 and SC 9000XL Patient Monitors Service Manual
12.2.3 EEPROM Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32
12.2.4 LCD and Push Buttons . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32
12.2.5 Current Limiting the Voltage Reference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32
13Remote Comm Subsystem Hardware . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
13.1Connection Characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
14Infinity Network CPS and IDS (w/ Power Supply) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .33
14.1Network Board Hardware . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .33
Figure 2-18 Comm unications Functional Block Diagram . . . . . . . . . . . . . . . . . . . . . . . . . 33
14.2EEPROMs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .34
14.3CPS Power Supply . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .34
15Infinity Docking Station (IDS) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Chapter 3: Repair . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37
2 Service Policy and Replaceable Parts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37
2.1 Base Unit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37
2.2 R50 Recorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37
2.3 Modules, PODs, and Peripherals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
3 Safety Precautions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
4 Replaceable Parts and Subassemblies That DO NOT Require Opening the Monitor . . . .38
4.1 Replacing Rotary Knob . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38
4.2 Replacing Front Bezel Labels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38
4.2.1 Removing Existing Label . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
4.2.2 Installing Language Label . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .39
4.2.3 Installing SIEMENS Metal Logo Label . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .39
4.2.4 Installing Monitor Model Label . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .39
4.3 Replacing Foot Pads . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .39
4.4 Removing / Installing External Battery and Support Components . . . . . . . . . . . . . . . . 39
4.4.1 External Battery (optional) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .39
Figure 3-1 SC 7000 and SC 9000XL Rear View w/ Cover Removed . . . . . . . . . . . . . . . .40
Figure 3-2 Rear Housing Components/Subassemblies . . . . . . . . . . . . . . . . . . . . . . . . . .40
4.4.2 External Battery Compartment Door . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .41
4.4.3 Replacing External Battery Ejection Spring . . . . . . . . . . . . . . . . . . . . . . . . . . . .41
4.5 Removing / Installing Main Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .41
Figure 3-3 Battery Cable Ties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .42
4.6 Replacing Power Cable and Speaker Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . .42
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers v
7k9kXLSM.book.CD_ROMTOC.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 10
Service Manual SC 7000 and SC 9000XL Patient Monitors
0
4.7 NP Filters and Pump Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Figure 3-4 NP Subassembly in Rear Housing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
4.7.1 Replacing Manifold and Air Intake Filters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
4.7.2 Removing NP Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
4.7.3 Installing NP Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
4.7.4 NBP Characterization Preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
4.7.5 NBP Characterization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
4.8 Replacing Monitor Handle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
5 O pe ning Monitor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
5.1 Removing/Installing Side-Panels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
5.1.1 Removing Ejection Shaft Cover . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
5.1.2 Installing Ejection Shaft Cover . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
Figure 3-5 Removing Left and Right Side Panels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
5.1.3 Removing Right Side Panel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
5.1.4 Installing Right Side Panel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
5.1.5 Removing Left Side Panel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
5.1.6 Installing Left Side Panel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
5.2 Separating Front Bezel Subassembly and Rear Housing Subassembly . . . . . . . . . . . 47
Figure 3-6 Bottom Release Tabs for Front Bezel Subassembly . . . . . . . . . . . . . . . . . . 47
Figure 3-7 Security Clip
and Tape
0
@@ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Figure 3-8 Top Release Tabs for Front Bezel Subassembly . . . . . . . . . . . . . . . . . . . . . 48
6 Replacing Subassemblies in Rear Housing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
6.1 Removing/Installing Funnel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
6.2 Main Processor PCB Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
6.2.1 Removing Main Processor PCB Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . 49
6.2.2 Installing Main Processor PCB Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . 49
6.3 Replacing Rear Housing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Figure 3-9 Main Subassemblies of SC 7000 and SC 9000XL Patient Monitors . . . . . . 50
Figure 3-10 Front Bezel Subassembly Components . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Figure 3-11 Front Bezel Subassembly - Interior View . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
7 Replacing Subassemblies in Front Bezel Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . 52
7.1 Front Bezel PC Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
7.1.1 Removing Front Bezel PCB . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Figure 3-12 Optical Encoder Subassembly. See Note in Figure 3-10 caption. . . . . . . . . 52
7.1.2 Installing Front Bezel PC Board . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
7.2 Optical Encoder Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
vi Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM.book.CD_ROMTOC . fm/0 4-99/k aupp
Page 11

SC 7000 and SC 9000XL Patient Monitors Service Manual
Figure 3-13 Display Screen Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
7.3 Backlight Lamps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
7.4 Front Bezel/Lens Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
7.5 Front Bezel Subassembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
8 Closing Monitor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
Figure 3-14 SC 7000 / SC 9000XL Patient Monitor Bottom View . . . . . . . . . . . . . . . . . . . 56
Figure 3-15 Installing Security Clip and Tape . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Chapter 4: Functional Verification and Calibration . . . . . . . . . . . . . . . . . . . . . . . . . . . . .57
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
2 Recommended Tools and Test Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Table 4-1Recommended Tools and Test Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . 58
3 P ow er Circuits and Start-up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3.1 Power ON/OFF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3.2 Power-Up Sequence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3.3 Monitor Powered From External Source . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
4 Rotary Knob . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
5 LCD Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
6 Fix ed Keys . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
6.1 ON/OFF Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
6.2 Main Screen Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
6.3 Alarm Silence Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
6.4 Alarm Limits Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
6.5 All Alarms Off Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
6.6 Code Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
6.7 Record Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
6.8 Print Screen Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
6.9 NBP Start/Stop Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
6.10Zoom Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
6.11Help Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
6.12Mark Key . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
7 E CG /RESP Functions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 1
7.1 ECG/RESP Test Setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
7.2 Waveforms/Digital Readouts/Tones . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
7.3 Pacer Detection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
7.4 Lead-Off Indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
7.5 Alarm Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
7.6 Asystole . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers vii
7k9kXLSM.book.CD_ROMTOC.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 12

Service Manual SC 7000 and SC 9000XL Patient Monitors
8 S pO 2 Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
8.1 SpO2 Test Setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
8.2 Waveforms/Digital Readouts/Tones . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
8.3 Pulse Tone Generator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
8.4 SpO2 Limits Alarms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
9 Te m perature Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
9.1 Temperature Test Setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
9.2 Digital Readout . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
9.3 Temperature Calibration Check . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Table 4-2Resistance Value vs Temperature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
9.3.1 Recommended Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
9.3.2 Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
10Non-Invasive Blood Pressure Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Figure 4-1 NBP Calibration Check / Calibration Test Setup . . . . . . . . . . . . . . . . . . . . . . 65
10.1System Setup and Pneumatics Leakage Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
10.2Calibration Check . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
10.3NBP Calibration Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
10.4Hardware Overpressure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
10.5Pump . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
10.6Interval Mode . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
10.7Safety Timer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
11etCO2 Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
12HemoMed Pod . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
12.1IBP Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
Figure 4-2 IBP Functional Verification Test Setup for HemoMed Pod . . . . . . . . . . . . . 68
12.1.1 IBP Test setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
12.1.2 Channel A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
12.1.3 Channel B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
12.1.4 Channel C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
12.1.5 Channel D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
12.2Cardiac Output Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
13HEMO POD2/4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
13.1IBP Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
13.1.1 IBP Test setup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
Figure 4-3 IBP Functional Verification Test Setup for HEMO2/4 PODs . . . . . . . . . . . . . 70
13.1.2 HEMO2/4 POD Channel A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
13.1.3 HEMO2/4 POD Channel B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
viii Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM.book.CD_ROMTOC . fm/0 4-99/k aupp
Page 13

SC 7000 and SC 9000XL Patient Monitors Service Manual
13.1.4 HEMO4 POD Channel C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
13.1.5 HEMO4 POD Channel D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
13.2Temperature Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
13.3Cardiac Output Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
14Memory Backup Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
15CPS/IDS Mode . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
16DirectNet Mode (requires ≥VC2-level installed software) . . . . . . . . . . . . . . . . . . . . . . . . . . 72
17Leakage Current Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
Figure 4-4 Leakage Current Test Setups . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
Table 4-3Leakage Current Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
18Battery Charger Circuit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
19Recorder Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
Chapter 5: Troubleshooting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .75
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
2 Recommended Tools and Test Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Table 5-1Recommended Tools and Test Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . 75
3 P ow er Problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
3.1 Monitor won’t power ON when connected to external power source . . . . . . . . . . . . . 76
Figure 5-1 Connector I/O PCB . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
3.2 Monitor won’t maintain monitor operations for prescribed time or power ON. . . . . . 77
3.3 With external battery installed, monitor fails to function for prescribed time. . . . . . . 78
3.4 ON/OFF control problem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
3.5 Internal or external (auxiliary) battery doesn’t charge . . . . . . . . . . . . . . . . . . . . . . . . . 79
3.6 Power-Up Sequence Fails to Complete Properly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
Table 5-2Power-up Process Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
4 Monitor Resets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
5 P ow er On/Off Piezo Tone Fails to Sound. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
Table 5-3Power-off Alarm Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
6 Rotary Knob Malfunction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
Table 5-4Rotary Knob Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
7 Fix ed Key Fails to Function. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
Table 5-5Fixed Key Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
8 LCD Display Malfunction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
Table 5-6LCD Display Malfunction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
9 Is olating Cable Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers ix
7k9kXLSM.book.CD_ROMTOC.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 14

Service Manual SC 7000 and SC 9000XL Patient Monitors
10Visible or Audible Alarm Reporting Failure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Table 5-7Alarm Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
11MultiMed POD - Parameter Signal Problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Table 5-8Parameter Signal Problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
12NBP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
12.1NBP Error Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
12.2NBP Troubleshooting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
Table 5-9NBP Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
13etCO2 Malfunction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
14HEMO2/4 Pod / HemoMed Pod . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
Table 5-10etCO2 Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
14.1Readings Missing or Inaccurate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
14.2IBP Malfunctions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
Table 5-11IBP Malfunctions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
15No Printout from Recorder. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
Table 5-12Recorder Problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
16Patient-Related Data Not Retained or Monitor Fails to Compute Trends . . . . . . . . . . . . . 90
17Software Loading Problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
18Difficulty acquiring export protocol data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
19Total or partial loss of network communications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
Appendix A: Replacement Parts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .93
Figure A-1 Major Subassemblies, w/ Funnel and Side Panels (Exploded View) . . . . . 94
Table A-1Major Replaceable Subassemblies, Funnel, Side Panels and Labels . . . . 94
Figure A-2 Front Bezel Subassembly - Replaceable Parts/Subassemblies . . . . . . . . . 95
Table A-2Front Bezel Subassembly - Replaceable Parts/Subassemblies . . . . . . . . . 95
Figure A-3 Rear Housing - Replaceable Parts/Subassemblies . . . . . . . . . . . . . . . . . . . 96
Table A-3SC 7000 Rear Housing Subassembly - Replaceable Parts/Subassemblies 96
Figure A-4 R50 Recorder - Replaceable Parts/Subassemblies . . . . . . . . . . . . . . . . . . . 97
Table A-4R50 Recorder Replaceable Parts/Subassemblies . . . . . . . . . . . . . . . . . . . . 97
Figure A-5 Security Clip H/W Rwk Kit (See Table A-5.) . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Figure A-6 NBP Filter Capacitor on Main PCB H/W Rwk Kit (See Table A-5.) . . . . . . . . 98
Table A-5Field Rework Kits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
Appendix B: Connector / Cable Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9 9
1 Docking Connectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 99
Figure B-1 Monitor Docking Connector (Refer to Table B-1.) . . . . . . . . . . . . . . . . . . . . . 99
Figure B-2 CPS/IDS, Interface Plate Docking Connector (Refer to Table B-1.) . . . . . . . 99
x Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM.book.CD_ROMTOC . fm/0 4-99/k aupp
Page 15

SC 7000 and SC 9000XL Patient Monitors Service Manual
Figure B-3 Docking Station Cable Connector (Refer to Table B-1.) . . . . . . . . . . . . . . . . 99
Table B-1Docking Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 99
2 Infinity Basic/Device CPS Connectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
Figure B-4 Basic / Device CPS Connectors - Infinity Network (Refer to Table B-2.) . 100
Table B-2Basic / Device CPS Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 00
3 Infinity Docking Station Connectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101
Figure B-5 Infinity Docking Station Connectors(Refer to Table B-3.) . . . . . . . . . . . . . 101
Table B-3Infinity Docking Station Connectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101
4 Interface Plate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
Figure B-6 )Interface Plate Connectors (Rear View (Refer to Table B-4.) . . . . . . . . . . 102
5 Recorder / Alarm Y Cable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
Figure B-7 Recorder / Alarm Y Cable (Accessory (Refer to Table B-5.)) . . . . . . . . . . . 102
Table B-4Interface Plate Connectors Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
Table B-5Recorder / Alarm Y Cable Connector Pinouts and Wire Color Code . . . . 102
6 MultiMed Pods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
6.1 MultiMed Pod . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Figure B-8 MultiMed Pod (Refer to Table B-6.) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Table B-6MultiMed Pod Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
6.2 MultiMed 12 Pod . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Figure B-9 MultiMed 12 Pod (Refer to Table B-7.) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Table B-7MultiMed 12 Pod Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
7 MultiMed Pod Cable Connector on SC 7000 / SC 9000XL . . . . . . . . . . . . . . . . . . . . . . . . 1 04
Figure B-10MultiMed Pod Cable Connector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
Table B-8MultiMed Pod Cable Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
8 HemoMed Pod Cable Connector on SC 7000 / SC 9000XL . . . . . . . . . . . . . . . . . . . . . . . . 104
Figure B-11HemoMed Pod Cable Connector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
Table B-9HemoMed Pod Cable Connector Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . . 104
9 S C 7000 / SC 9000XL Analog Output Connector, X10 . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
Figure B-12Analog Output Connector (refer to Table B-8) . . . . . . . . . . . . . . . . . . . . . . 105
Table B-10Analog Output Connector, X10, Pinouts . . . . . . . . . . . . . . . . . . . . . . . . . 105
10SC 7000 / SC 9000XL Network Connector (Requires ŠVC2 software) . . . . . . . . . . . . . . 105
Figure B-13Network Connector (Refer to Table B-11.) . . . . . . . . . . . . . . . . . . . . . . . . . . 105
Table B-11Network Connector Pins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
11SC 7000 / SC 9000XL RS-232, Keypad Input, Alarm Out Connector, X8 . . . . . . . . . . . . . 106
Figure B-14RS-232, Keypad Input, Alarm Out Connector (see Table B-12) . . . . . . . . . 106
Table B-12RS-232, Keypad Input, Alarm Out Connector Pinouts . . . . . . . . . . . . . . 106
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers xi
7k9kXLSM.book.CD_ROMTOC.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 16

Service Manual SC 7000 and SC 9000XL Patient Monitors
12Remote Alarm Cable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
Figure B-15Remote Alarm Cable - Unterminated (Refer toTable B-13) . . . . . . . . . . . . . 106
Table B-13Remote Alarm Cable Connector Pinouts and Wire Color Code . . . . . . . 106
13Analog Cable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
Figure B-16Analog Cable (Unterminated - Refer to Table B-14.) . . . . . . . . . . . . . . . . . . 107
Table B-14Analog Cable Color Code . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
14PSL Connector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
Figure B-17PSL Connector (Refer to Table B-15.) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
Table B -15PSL Connector Pins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
15Cardiac Output Intermediate Cable Wiring Diagram . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108
Figure B-18Cardiac Output Intermediate Cable Wiring Diagram . . . . . . . . . . . . . . . . . 108
16Input Connector on etCO2 Module . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 109
Figure B-19Input Connector on etCO2 Module (Refer to Table B-16.) . . . . . . . . . . . . . 109
Table B-16etCO2 Module Input Connector Pins . . . . . . . . . . . . . . . . . . . . . . . . . . . . 109
17SC 9015 Remote Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110
Figure B-20SC 9015 Remote Display - Rear View (Refer to Table B-17.) . . . . . . . . . . . 110
Table B-17SC9015 Remote Display Connector Pins . . . . . . . . . . . . . . . . . . . . . . . . . 110
18HEMO Pod . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 11
Figure B-21HEMO Pod Connectors (Refer to Table B-18.) . . . . . . . . . . . . . . . . . . . . . . 111
Figure B-22Press Adapter Input (Refer to Table B-19.) . . . . . . . . . . . . . . . . . . . . . . . . . 111
Table B-18HEMO Pod Connector Signals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111
Table B-19PRESS Input Connector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111
Appendix C: Diagnostic/Error Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .113
1 O v erview of Diagnostic Messages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113
Table C-1Diagnostic Log Codes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113
Appendix D: Functional Verification Checklist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .135
Clinical Site Report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .138
Appendix E: Service Setup Instructions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .139
xii Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM.book.CD_ROMTOC . fm/0 4-99/k aupp
Page 17

Chapter 1: General Information
1Introduction
2 Overview
This Manual is intended to serve as a source of technical information for
qualified personnel to use in servicing SC 7000 and SC 9000XL Monitors
and associated peripheral devices. In light of the state-of-the-art technology
used in the manufacture of Siemens' equipment, proprietary nature of the
software, and specialized equipment required for replacement of most
individual parts, Siemens policy (see Section 3) is for SC 7000 and SC
9000XL monitors, and peripheral modules specifically related to the SC
7000 or SC 9000XL, to be serviced only to the field-replaceable
subassembly level. Replacement of components other than those listed in
“Appendix A: Replacement Parts”, should be performed only at Siemens
service depots.
SC 7000 and SC 9000XL patient monitors have been designed to function
as a portable or a stationary monitor with equal ease. Each has an internal
main battery, as well as provision f or an additional exte rn al (aux iliary )
battery for extended operation as a portable monitor. For stationary
operation near a bedside, the monitor is placed on a specially designed
docking station attached to a shelf, wall, or IV pole that securely locks it into
place. While on the docking station, the monitor is powered by an external
power supply that also charges the monitor's main battery and external
battery (if installed). In addition, the docking station provides audio, video
and data signal connection to the local network as well as a variety of locally
installed peripheral devices such as a remote display/controller, recorder,
MIB converter, and Surgical Display Controller or SDC (sometimes referred
to as the Independent Surgeon Display or ISD). NBP is included as an
integral function. For airway and sidestream CO
cartridge can be installed on a slide mount on the back of the SC 7000.
Employing the "pick-and-go" concept, the monitor is simply picked up off of
the docking station to return it to portable operation, with no interruption in
patient monitoring.
monitoring, an etCO2
2
2.1 R50 Recorder
2.2 I
NFINITY
Docking
Station
2.3 Docking Station (Discontinued)
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 1
7k9kXLSM.c1.CD_ROM.fm/04-99/kaupp
An R50 Recorder connects to the SC 7000 and SC 9000XL via a CPS or
IDS. The recorder may be either a network or local recorder, depending on
configuration of a CPS. If plugged directly into an IDS, the recorder
functions as only a local recorder for any monitor mounted on the IDS. For
standalone portable operation, an interface plate can be used to provide
recorder connection. The R50 Recorder prints on 50mm wide paper, and
has three control keys -- Start Cont., Alternate Speed, and Stop.
NFINITY
The I
power supply it replaces the discontinued Basic I
Docking Station combination (see Sections 2.3 and 2.4). As a docking
station, it serves as a secure mount for SC 7000 and SC 9000XL (and also
for SC 9000, SC 6000P and SC 6002) Monitors in “Pick-and-Go”
operations. When equipped with a MIB Option, an IDS provides the
combined functionality of a Device CPS and Breakout Box.
A docking station is a passive device that provides a sturdy mount for the
SC 7000 or SC 9000XL while supporting the "pick and go" concept. The
docking station mounts near a bedside, attached to a shelf, wall, or an IV
pole, and provides pass-through to a CPS for the signals from a SC 7000
or SC 9000XL. A second docking station supports peripheral devices such
as the R50 Recorder.
NOT A CONTROLLE D DOCUMENT
Docking Station (IDS) is an active device. With its separate
NFINITYNET
CPS and
Page 18

Service Manual SC 7000 and SC 9000XL Patient Monitors
NFINITY
NFINITYNET
Network connectivity
CPS (Communication/Power Supply)
2.4 I
NFINITYNET
(D
ISCONTINUED
CPS
)
A Basic or Device I
connects to an SC 7000 or SC 9000XL via a Docking Station, and performs
the following functions:
• powers the SC 7000 or SC 9000XL from an AC power source
• provides power to charge both main and external battery (if installed)
• provides I
• provides ALARM OUT
• provides remote display connectivity via AV cable
• provides connection capability to R50 Recorder(s)
• provides MIB and CANBUS connectivity
2.5 Remote Display
2.5.1 Passive Remote Display The passive remote display unit connects to a CPS or IDS via an A V cable,
and with the hand-held keypad, replaces the SC 9015 Remote Display/
Cpontrol unit (see Sections 2.5.2 and 2.5.3). It is powered separately from
the CPS/IDS by its own line cord, and includes the following hardware:
• 15” color VGA 640 x 480 screen or SVGA 800 X 600 screen (driven by
graphics hardware in the Monitor)
• power LED
2.5.2 Keypad The hand-held keypad provides for control of the monitor via the Passive Remote display and manual entry of calculation data from the bedside.
2.5.3 SC 9015 (Discontinued) The SC 9015 Remote Display/Control unit connects to the CPS or IDS via an AV cable. It is powered separately from the CPS/IDS by its own line cord, and includes the following hardware:
• 15” color VGA 640 x 480 screen (driven by graphics hardware in the
base unit)
• ambient light sensor (for controlling screen intensity)
• speaker (driven by an audio tone generator on the base unit)
• fixed keys and a rotary knob for user input
• power LED
2.6 PSL
2.7 Interface Plate
3 Service Policy
The PSL power supply plugs directly into the PSL connector on the back of
the SC 7000 or SC 9000XL, and is used for operating the monitor in a
stand-alone configuration. The PSL provides the following:
• powers the SC 7000 or SC 9000XL from an AC power source
• provides power to charge both main and external batteries
The Interface Plate provides connectivity to an R50 Recorder, remote
alarm out, SC 9015 Remote Display/Control (or Passive Remote Display)
when the monitor is in a standalone configuration powered by a PSL.
The design of the SC 7000 and SC 9000XL facilitates repair to the
replaceable subassembly (e.g., PCB, module) or selected component (e.g.,
rotary knob, battery) level in the field. PC Boards are NOT field repairable.
The repair philosophy for any unit is to replace specified subassemblies. A
listing of replaceable items is given in “Chapter 3: Repair” and “Appendix A:
Replacement Parts”.
2 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c1. CD_ROM . fm/0 4-99/ kaupp
Page 19

SC 7000 and SC 9000XL Patient Monitors Service Manual
4 Re lat ed
Documentation
5 Cleaning
6 Technical Data 7 Brief Operating
Instructions
7.1 SC 7000 and SC 9000XL Monitor Controls
• User Guide for the installed software version
• Hardware and Software Installation instructions
• Service Setup Instructions
Contact with chlorine bleach, Cidex, or body fluids does not damage or
cause discoloration of any component case of an SC 7000 or SC 9000XL
installation. Clean Base Unit, pods, cartridges, and cables using a 95%
solution of isopropyl alcohol. If contaminants enter the chimney (slot in
middle of unit), flush chimney with one cup of water not under pressure.
Note: Bac solution mars the finish of the monitor case.
A complete set of technical data is given in the Operating Instructions (User
Guide) for the installed software version.
This section provides a brief overview of SC 7000 and SC 9000XL monitor
controls to assist technical personnel in servicing and testing procedures. For
detailed operating instructions and additional information, consult the monitor’s
User Guide and supplements for the installed software version.
Control of al l S C 7000 and SC 9000XL func tions is via fixed keys that have
tactile f eedback, and a rot ary knob for s electing from on-screen menus.
Turning the rotary kno b locates differe nt menu item s, and pressing the knob
in selects the item. Depe nding on the item selected , pressing the knob in may
either bri ng up anothe r menu or init iate an ac tion. “Gho sted” it ems cannot be
selected.
8 Peripheral Device
Controls
9 Passwords
9.1 Clinical Password
9.2 Service Password
10Menus
10.1Main Menu
The Remote Keypad has an identical set of keys and a display knob, that
mimic the action of those on the SC 7000 or SC 9000XL Base Unit. Except
for the ON/OFF key, the monitors can be operated from either the base unit
or the Remo te Key pad.
Individual cartridges, pods, and peripheral devices (such as the recorder)
also have fixed keys that control specific aspects of their operation. Refer
to the monitor’s User Guide for specific key functions.
SC 7000 and SC 9000XL systems have two kinds of basic password
protection -- clinical password, and service password. Clinical and service
passwords are entered via selections on a keypad that appears whenever
a password-protected function is selected. To enter a password, turn the
rotary knob to highlight a number and then press in on the knob to enter the
number. When all numbers of the password have been entered, turn the
knob to highlight “Accept,” and press in on the knob.
The clinical password is available to authorized supervisory personnel at
the clinical site as well as to service personnel.
The service password is available to only authorized service personnel.
The Main Menu uses a three column layout for menu navigation: Level 1 =
main selection list, Level 2 = workspace A, and Level 3 = workspace B.
Selecting any function category on Level 1 of the Main Menu brings up a
list of selectable related functions and menus in Level 2. Selecting a
function in Level 2 produces a similar result in Level 3.
Press MENU fixed-key to display
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 3
7k9kXLSM.c1.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
MAIN
screen with overlay of Main Menu.
Page 20

Service Manual SC 7000 and SC 9000XL Patient Monitors
10.2Service Menu
10.3Install Monitoring Software
The Service Menu is accessed via the Monitor Options selection under the
Monitor Setup function on the Main Menu. To access the Service menu and
related functions, do the following:
1) Select Monitor Setup on Level 1, then select Biomed on Level 2, and
then select Service on Level 3.
2) Input the service password (
Note: In general, the Service Menu provides access to the following
(may vary with software version):
• Language selection
• Regulation
• Alarm So unds
• Network control
• Network Configuration (requires installed SW version ≥VC2)
• Transport Brightness
• Line frequenc y setting
• Restore factory defaults
• Copy setups to card
• Copy setups to monitor
• I n s tall So ft ware
• Locked Options
• Wav eform Simu lator
Software and languages for SC 7000 and SC 9000XL Monitors are installed
from a memory card via the monitor’s memory card reader. If the software
loading process fails to complete properly, and/or the monitor sounds a
steady tone (other than the Piezo), repeat the procedure. If the process fails
a second time, either the card or the Monitor is defective. Troubleshoot and
repair or replace as necessary.
4712
).
Note: In an I
with <VC2 software, or ≥VC2 software and configured for CPS/IDS
mode, be sure that the CPS or IDS is equipped with compatibile
software . R efe r to the Softw ar e C o mpatibility C ha r t fo r th e C PS / ID S
software version required for compatibility with a specific SC 7000 or
SC 9000XL software version
1) With Monitor switched off, insert and firmly seat PCMCIA card into
memory card slot. Do NOT remove PCMCIA card until instructed to do
so.
Note: The card can be seated in only one orientation because of
keyed channels on the end of the card. If the card can not be easily
seated, remove card, turn card over, reinsert, and firmly seat. Do NOT
attempt to forceably seat the card.
2) Power Monitor ON to initiate download process.
Note: During the download process, the pick and go icon (running
man) and the SIEMENS logo appear on the screen. The icon initially
displays as green and changes to white. The logo toggles between
green and white,and finally displays as green on a white background.
The newly installed software version appears under the logo.
3) After a single alert tone sounds and a message regarding patient data
loss appears, select “Continue” and then select YES for new patient.
NFINITY NETWORK
environment, if the monitor is equipped
4 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c1. CD_ROM . fm/0 4-99/ kaupp
Page 21

SC 7000 and SC 9000XL Patient Monitors Service Manual
4) Access Beds ide Setup , and verify that settings of Language,
Regulation, Alarm Sounds, Transport Brightness, and Line Frequency
are approrpriate for customer site. Also, assure that Waveform
Simulator is set to OFF.
5) Remove PCMCIA card.
6)• If SW version <VC2, or ≥VC2 and monitor to be mounted on a docking
station or IDS, set Monitor on active docking station and then set
Network Mode for CPS/IDS. Select “Save ALL” and then go to step 7.
Note: Monitor power-cycles automatically when “Save ALL” is
selected, if Network Mode is changed.
10.4 Configuration Download Procedure
•If SW version ≥VC2, and monitor to be directly connected to I
ETWORK
N
, refer to procedure in Software Installation Instructions or
NFINITY
Service Setup Instructions to set Network Mode for DirectNet and
configure monitor. Then go to step 9.
7) Affix new software version label (supplied) over existing software
version label near top of memory card slot on right side panel.
8) Verify that monitor returns to MAIN screen, after timeout.
9) Recycle PCMCIA card when it is of no further use.
The configuration download procedure (-- not to be confused with monitor
configuration procedure required for DirectNet functioning; see “Appendix
E: Service Setup Instructions”) is applicable only to monitors set for use
with a docking station or IDS. In general, the procedure is to completely set
up one monitor, save the setup to the CPS or IDS, and then transfer the
setup to a Data Card. The configuration stored in the Data Card can then
be used to setup monitor configurations in other CPS/IDSs.
1) With no Data Card inserted and monitor on docking station, adjust
settings for monitor exactly as required by customer.
2) Review configuration with appropriate customer personnel before
proceeding.
3) Press Menu key, and select Sav e/R estore → Save Setup.
4) Enter clinical passw ord,
, and select Accept.
375
5) Highlight setup to be saved, and press rotary knob in to save selection
to CPS/IDS.
6) Only the Default configuration supports “Pick and Go.”
7) Wait for message “New Setup Saved.”
8) Repeat steps 1 through 7 for optional setups as required, and select
Rename Setup in Biomed menu to name each setup in accordance
with site requirements.
9) With
MAIN
screen displayed on monitor, insert and firmly seat Data
Card into memory slot.
Note: The card can be fully inserted in only one orientation, because
of keyed channels on the end of the card, and can be damaged if
forced into the slot. Insert the card firmly, but
force the card.
Be sure that Write Protect on the card is OFF.
do NOT attempt to
10) P res s Menu key, and select Monitor Setup → Bio med → Service.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 5
7k9kXLSM.c1.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 22

Service Manual SC 7000 and SC 9000XL Patient Monitors
11) Enter Service password, 4712, and select Ac cept.
12) Select More → “Copy Setups to Card.”
13) Select “Copy All.”
14) Wait for message “Memory Card Tansfer Complete.” Then press Main
Screen key and remove Data Card from monitor.
15) Insert card into monitor connected to next CPS to be identically
configured.
16) P res s Menu key, and select Monitor Setup → Bio med → Service
17) E nter Service password, 4712, and select Accept.
18) Select More → “Copy Setups to Monitor.”
Note: In actuality, this copies the setups to the CPS or IDS, which in
turn reconfigures the setup of the monitor when “Restore Setups”
function is invoked.
19) Select “Replace All.”
20) Wait for message “Memory Card Tansfer Complete.” Then press Main
Screen key and remove Data Card from monitor.
10.5Diagn ostic Log Uploa d Procedur e
21) P res s Menu key, and select Save/ Res tore → Restore Setup.
22) Select “Default” → “Patient and Monitor Settings.”
23) Repeat steps 15 through 22 until all CPSs/IDSs to be identically
configured have been set up.
The monitor is constantly checking its performance during monitoring. If
errors occur, they are logged in the unit and stored in non-volatile memory.
The logs are useful in diagnosing problems remotely at the factory. The
following procedure can upload the diagnostic logs from approximately 10
to 16 monitors to a Data Card, depending on the size of the individual logs.
Assure that Write/Protect switch on Data Card is set to Write position.
1) With
2) Press Menu key, and select M onitor Setup → Biome d → Logs
3) Select “Copy All Logs.”
4) Remove Data Card from mon itor, and repeat steps 1, 2 and 3 for next
5) After all required diagnost ic logs have been upl oaded to the Dat a Card,
MAIN
screen displayed on monitor, insert and firmly seat Data
Card into memory slot.
monitor from which logs are to be uploaded.
send the Card (in its pr eaddressed return case when possible) t o:
Siemens Medical Systems, Inc.
EM-PCS
16 Electronics Avenue
Danvers, MA 01923 U.S.A.
Att: SC 7000 / SC 9000XL Project Manager
Note: The battery in the Data Card must be recharged for a period of
12 hours approximately every six months. Any SC 7000 or SC
9000XL Monitor powered by a CPS, IDS, or PSL can be used to
recharge the Data Card. Insert the card into the Monitor, and allow it
to remain in the monitor for 12 hours.
6 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c1. CD_ROM . fm/0 4-99/ kaupp
Page 23
Chapter 2: Theory of Operation
1Introduction
The SC 7000 and SC 9000XL are high-end single-board patient monitors.
The board provides the following parameters; 6 lead ECG, Respiration, two
Temperatures, SpO
connector for an etCO
, NBP, four IBPs, Cardiac Output, an interface
2
cartridge, and two onboard 5 watt patient isolated
2
ports for additional parameters. It has connectors for flat panel display,
simultaneous CRT, user interface, audio, batteries, NBP pneumatic
assembly, chart recorder, analog out, defib sync, memory card, Uarts, and
"Pick & Go" docking connector. The board contains the computer, power
supply and patient isolated front ends.
Computer Archictecture Hardware architecture of the monitors is based on a dual processor design
using two Motorola MPC860s with onboard cache. The main processor is
responsible for graphics and communications, while the second processor
is dedicated to data acquisition and algorithm processing. A DSP
subsystem preprocesses the front end data.
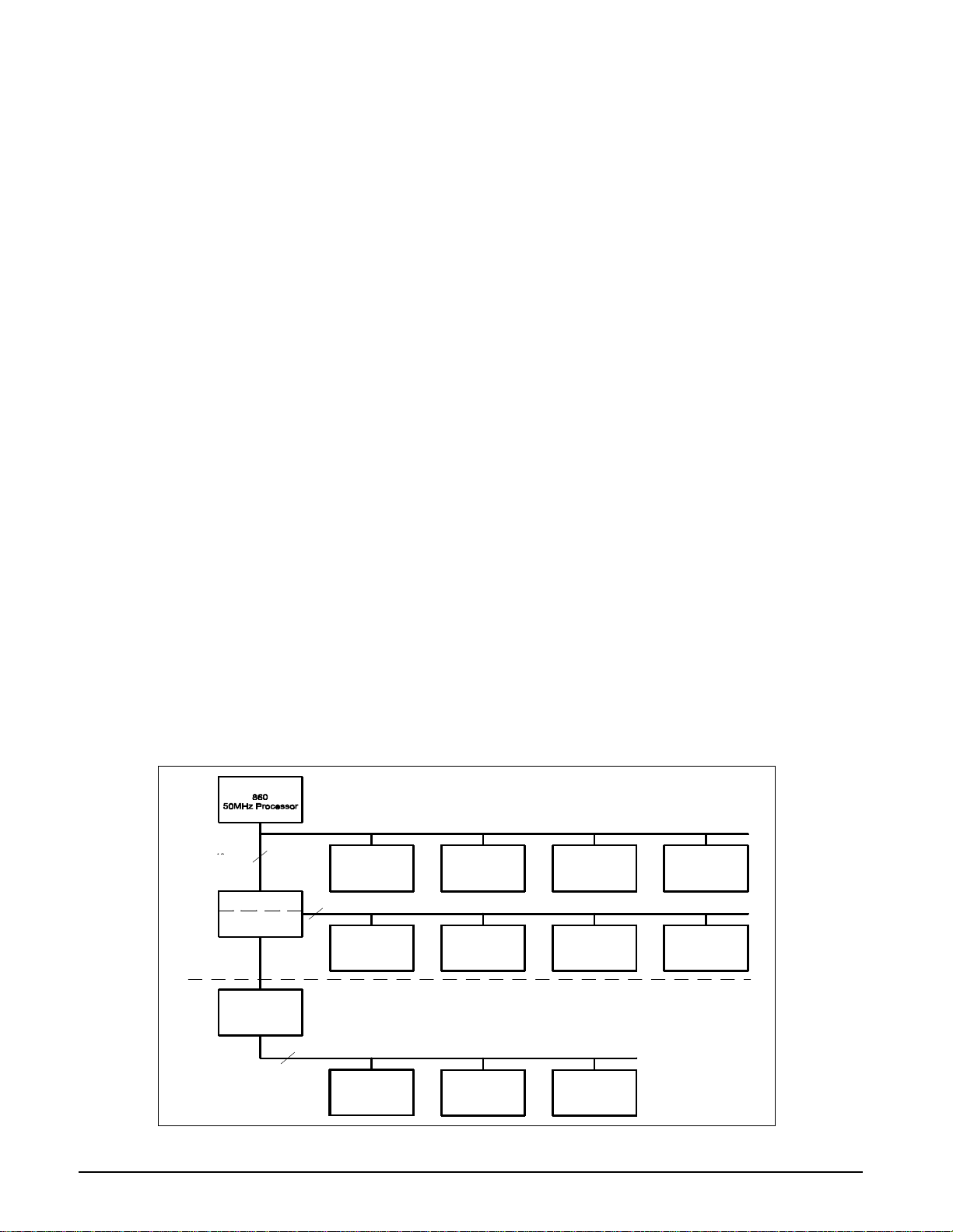
There are three major bus structures within the system; MAIN processor
bus, FRONT END bus, and REMOTE COMM bus (see Figure 2-1). The
buses operate at different speeds and efficiency. The FRONT END bus and
REMOTE COMM bus have multiple bus masters and common memory to
allow exchange between I/O devices.
The REMOTE COMM bus is special in that it may be connected and
disconnected without causing a monitor fault. This patented connect and
disconnect function of the monitor is advertised as "Pick and Go". This
allows monitors to be moved to different locations within the hospital and to
connect to multiple REMOTE COMM links without interruption of
monitoring. The traditional central station alarm function of alarming when
the patient monitor is suddenly disconnected from the network is modified
in this system by ensuring that a disconnect is intentional. A redundant
signal is used to verify a true “pick-and-go” such that a single fault does not
prevent an alarm by imitating a “pick-and-go.”
MAIN BUS
48
40
Megabytes/sec
SC 7000 /
SC 9000XL
IPS
3
Megabytes/sec
32
Processor Bridge
Remote Comm.
Transmitter
Remote Comm
Receiver
16
Local Memory
32
860
50MHz Processor
Common
Memory
48 Megabytes/sec
40
REMOTE COMM BUS
Memory
Expansion
FRONT END BUS
Common Memory DSP Pod I/O
Processor
Graphics I/O
Network
Adapter
Figure 2-1SC 7000 / SC 9000XL Bus Structure
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 7
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 24
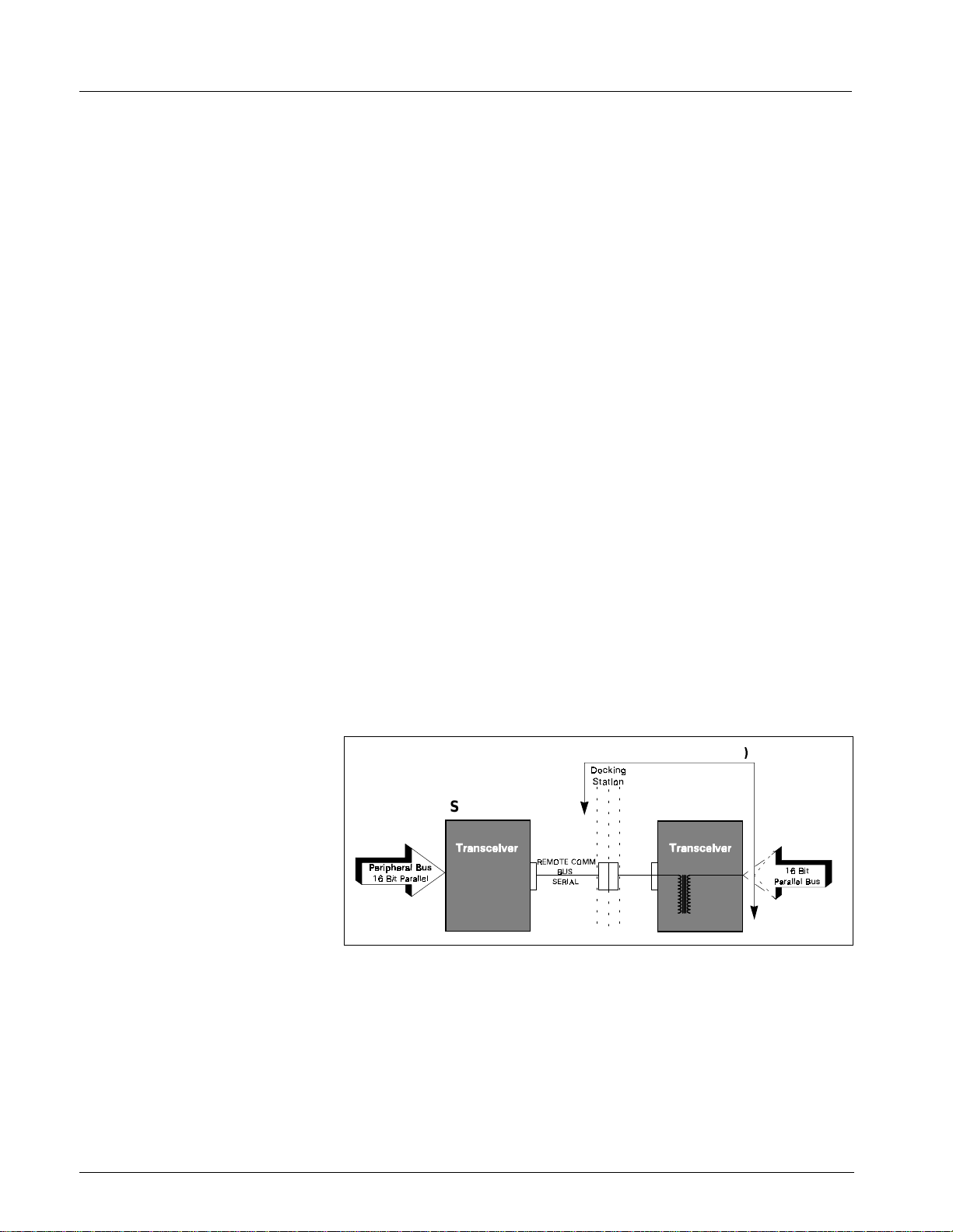
Service Manual SC 7000 and SC 9000XL Patient Monitors
L
1.1 Main Processo r Bus
1.2 Front End Bus
The Main processor bus is a 32 bit data bus connecting the MPC860 to its
main bank of 16 meg DRAM memory. The Program for the monitor is stored
in 8 meg Flash memory and uploaded to DRAM during initialization. The
DRAM is optimized for multiple word transfers allowing efficient cache fills.
This bus has an optional daughter card connector allowing expansion of the
main memory space. The graphics controller is connected to this bus to
allow high bandwidth access to video memory. The bus has a max
bandwidth of 40 megbytes/sec.
This bus also has an I/O space implemented in an FPGA. These functions
include audio, chart recorder interface, keypad and rotary knob interface,
and EEPROM. The EEPROM con tains serial #’s, calib ration const ants and
configurations. The I/O space also includes the Bridge to the FRONT END
bus and a port to the REMOTE COMM bus. The Bridge to the FRONT END
bus is unidirectional. This means that the Main processor may read and
write to the FRONT END bus, but the Front end processor can not access
the MAIN bus.
The Front End bus is a 32 bit data bus connecting the second MPC860 to
its main bank of 4 meg DRAM memory. The program for this processor is
downloaded from the main processor during initialization. The DRAM is
optimized for multiple word transfers allowing efficient cache fills. Both
processors contain 512K of battery-backed SRAM for trend and other
patient data storage. Data is exchanged through the common memory.
This bus has multiple bus masters that include the following:
1.3 REMOTE COMM Bus
• Front End 860
• Main 860
• DSP DMA
• POD Comm DMA (a POD is a configured front end)
• DRAM Refresh
IDS (= Dk. Sta. + XCVR
SC 7000/
SC 9000X
Figure 2-2 REMOTE COMM Bus
The R EMOTE COMM b us ( Figure 2-2) is a bus extender used to extend the
main bus to a second chassis. The parallel address bus and data bus are
serialized using high speed FDDI transceivers, allowing virtual parallel
access to a remote parallel bus. The parallel bus is located in the CPS
communication power supply module or in the Iinfinity Docking Station
(IDS). This bus interfaces to a network controller and other local serial
buses including MIB, lGraphics, Gas Monitoring, and other peripherals. The
host is stalled until completion of all read operations, but is released after a
write is latched to be serialized.
CPS
8 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 25
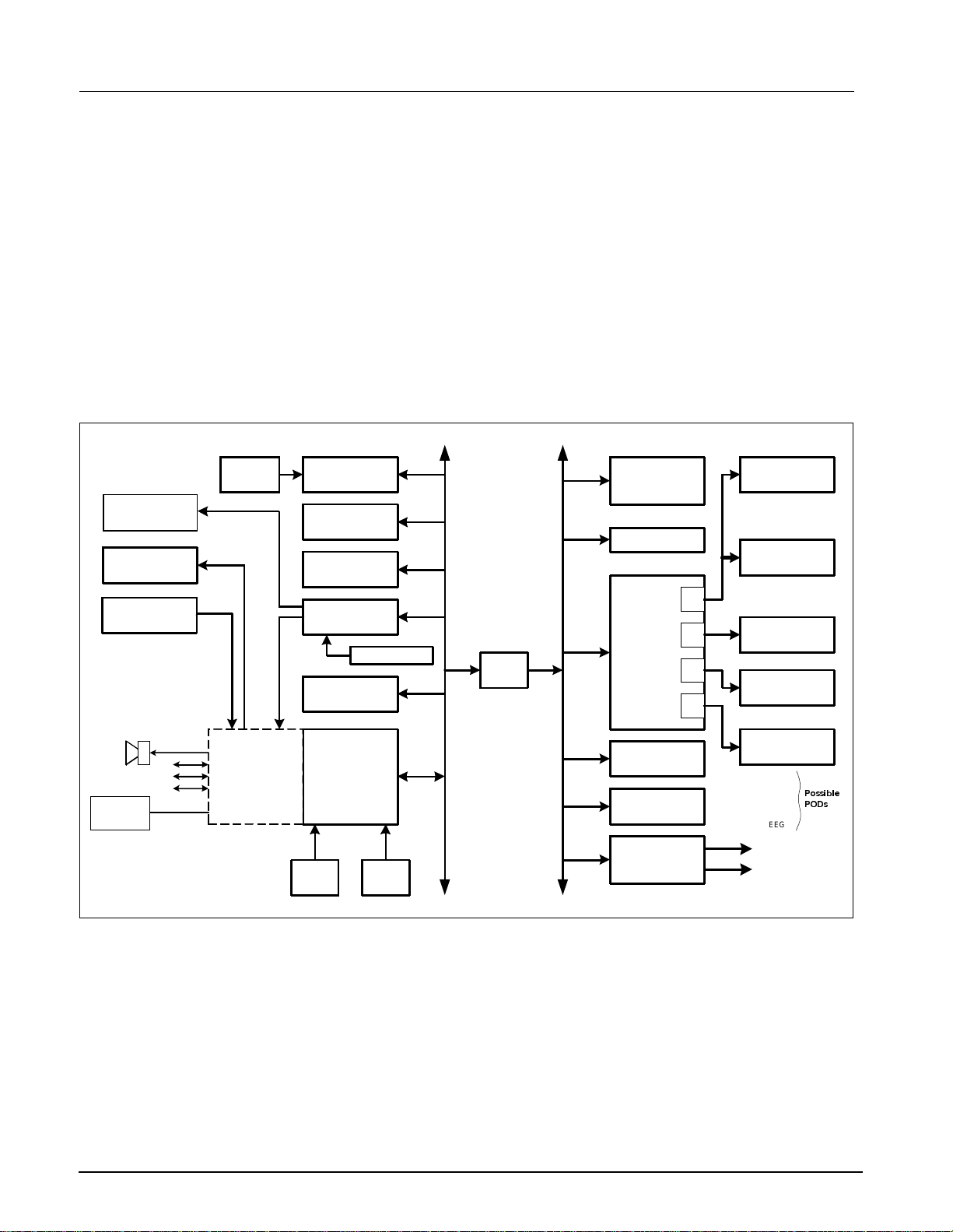
SC 7000 and SC 9000XL Patient Monitors Service Manual
1.4 Error Handling
Memory
CRT
LCD Display
Front Panel
Controls
Card
The hardware provides several cir cuits for error detection, error recovery,
and safety. The main proce ssor bus, f ront end pr ocessor bus, and REMOTE
COMM bus both have timeouts implemented w ith the arb iter to pre vent a lock
up of the sy st em . T he RE M O T E C OMM bus al so contain s a C RC for serial
transmis sion to and from t he CPS or IDS. I f a b ad CRC is detected an
interrupt is sent to the mai n 860. The main 860 and the Front End 860 are
both protec ted with watchdog t imers. I f a timer expi res, the system i nitiate s a
reset and restarts the monitor.
The power supply is also monitored with a piezo alarm that sounds during
power up (for test) and power down. This is to alert the user that the monitor
has turned off. The piezo alarm does not sound during a "Pick and Go"
since the monitor switched to battery operation without interruption. The
piezo is also sounded continuously if the monitor does not reset properly
after a watchdog timer has expired and the computer has halted.
860
Main Processor
RAM Memory
Flash Memory
VGA Graphics
Remote Comm
RAM Memory
Bridge
860
Front End
Processor
RAM Memory
POD
Com
MultiMed Pod
ECG/Resp
Temp
SpO
HemoMed Pod
Press
A
B
C
D
C.O.
etCO2 Cartridge
Pod 1
2
Chart
Recorder
Front Panel
Audio
Uart & Comm
Alarm Out
Keypad
RT Clock
Recorder
External
Battery
I/O Interfaces
Internal
Battery
2181 DSP
NBP
I/O Interface
Pod 2
HEMO2
HEMO4
12 Lead
tcpO
2
EEG
Analog Out
QRS Sync
3RVVLEOH
32'V
Figure 2-3 SC 7000 / SC 9000XL Block Diagram
2Main Unit
Both monitors are designed to be lightweight and portable. The division of
the REMOTE COMM bus and internal buses are a direct mapping of what
is needed during transport and what can be left in the patient’s room. The
REMOTE COMM bus is connected and disconnected via a docking station
which has a locating feature for the monitor as well as a locking latch. The
main unit has been designed as a single board computer. In addition to the
main board there is a front bezel board to interface to a flat panel display,
and a connector board used as a cable harness in the rear chassis. The
main processor board contains three sections (see Figure 2-3): processor,
power conversion, and front end. Each section is shielded from the others.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 9
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 26

Service Manual SC 7000 and SC 9000XL Patient Monitors
Processor Section The processor section co nt ai ns all compute r f unctions of t he m onitor. It
contains t wo M P C 860 processors, a VGA graph ics controll er, and a 2181
DSP. All of t hese devices co mmunicate using one large FPGA (field
programmable gate array) that is downloaded at init ial ization. The F P GA
contains all custom circuitry used in t he computer, including the processor
bridge, remote comm transmitter, pod com DMA, DSP interface, NBP
interfac e, and I/O interface s for both processors. Configur at i on of the FP GA
may be updat ed with the Software throu gh t he m em ory card adapter.
Power Conversion Section The power conversion section operates on a DC input from +11 to +15
volts. It switches between the external supply, the external battery and the
internal battery for the proper power source, and generates all necessary
dc voltages for the unit. It charges and maintains the internal and external
battery. This section also contains the patient isolation for the two internal
front ends as well as two general pod comm ports. It also has the power
control for the NBP pneumatics.
Front End Section The front en d cont ain s Multi Med and HemoM ed circ uit ry. T he M utiM ed fro nt
end provid es the following parameters ; 6-lead ECG, Respi ration, Puls e
Oximetry , and Temp erature . The NBP pressur e transd ucer is al so con tained
in this front end. The fr ont end is based on a si ngle 16 bit over sampling
converte r. Oversampling allows for a reduction i n anti-aliasing anal og
circuit ry while maintaini ng superior noise r ej ec tion. The HemoMed front end
provides four invasi ve pressures and Thermal Dilution Cardiac Output.
2.1 Front Bezel Board
2.2 Cooling System
2.3 Real Time Clock
2.4 Non-volatile Memory Battery Backup and Power Reset
The front bezel board is an interface board used to adapt a particular LCD
panel to the processor board. It also interfaces the front bezel rotary knob
and keypad to the processor. The front bezel board contains the backlight
invertor with a PWM input to allow for LCD brightness control in order to
save power.
The cooling system for the main monitor is convection based and uses a
patented chimney approach. The chimney is comprised of a heatsink which
cools the electronics and a plate which cools the LCD backlight. The
chimney is in the middle of the monitor and therefore is vented on top and
bottom. These vents should remain unobstructed for proper operation. The
chimney is waterproof and accidental liquid entering the chimney is safe.
CARE should be taken to operate the monitor below 45° C and store the
monitor below 60° C, since damage to the LCD can occur at 70° C. If the
internal temperature of the circuit board exceeds 80° C the monitor shuts
down to prevent damage to the electronics. The monitor does not restart
until the temperature is below the shut off value.
The Real Time Clo ck fu n ction is implemented with the EPSON- SEIKO
RTC4513 device, and is synchronized by the Central Station.
The shared RAM and real time clock are provided with a lithium battery
backup circuit to prevent corruption of this non-volatile memory during a
power loss condition (both primary and battery power are lost). Note that
the battery used for non-volatile memory backup should not be confused
with the internal and external batteries that are used to provide power to the
monitor base unit when primary power is lost. Non-volatile memory lithium
battery backup is controlled by a power supervisory device that provides a
power reset during a power loss condition.
Note: No provisions have been made to recharge this non-volatile
memory backup battery. Eventually (≈10 years), the battery must be
replaced.
10 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 27

SC 7000 and SC 9000XL Patient Monitors Service Manual
2.5 MPC 860 Communication Channels
Main Processor SCC1 Ethernet 10 Mbits/sec (future option)
Front End Processor SCC3 serial pod data
2.6 Device CPS
MPC 860 has an embedded communicat ions proces sor capable of
executing several protocols such as UART or Ethernet. The 860
communications channels are used as follows:
SCC2 SC 9015 UART selectable baud
SCC3 MVP-1 UART selectable baud
SCC4 MVP-2 UART selectable baud
SMC1 main diag UART 19.2 Kbaud
SPI a/d (power monitor)
SCC4 serial pod data
SMC1 front end diag UART
An additional UART implemented in the FPGA contains a large FIFO and
interfaces to the chart recorder.
A CPS (communication, power supply) has three boards -- power supply,
network board, and connector board, and allows for connection to an
INFINITY network as well as MIB and CAN. The FPGA and main program
memory are downloadable by the SC 7000 and SC 9000XL. The power
supply is a medical grade universal supply operating from 88 to 264 vac.
The Docking Station is a passive device that serves as a sturdy mount for
SC 7000 and SC 9000XL (as well as SC 9000 and SC 6000 series patient
monitors), in support of the P
through signals between the monitor and the CPS.
ICK-AND-GO
concept, and provides pass-
2.7 Infinity Docking Station
2.8 etCO2 cartridge
2.9 External Battery
The Infinity Docking Station base unit (IDS) with its separate power supply,
replaces the CPS and Docking Station combination in an I
ETWORK
N
monitors, as above, and also provides the network and peripheral device
connectivity of a Basic CPS. When equipped with a MIB 1-2 Option, it
provides the functionality of a Device CPS and Breakout Box.
The etCO2 cartridge is a hardware component attached to the back of the
SC7000 or SC 9000XL. The cartridge is a self contained computer capable
of mainstream and side stream measurements.
The external battery is a low cost lead acid battery and may be charged in
either the monitor or with an external charger. The external battery may be
hot-swapped to extend battery life during transport.
. As a docking station, it serves as a secure mount for the patient
NFINITY
2.10Interfaces
2.10.1 Local Fixed Keys Interface There are twelve fixed function keys on the monitor base unit, and a fixed
key dedicated as a power on/off switch. The power on/off switch is unique
in that it is not directly available via a status read command. The on/off
switch is input to the power supply subsystem interface, where the switch
state is detected and processed. Detection of a power off condition causes
an interrupt to the host processor.
2.10.2 Local Rotary Knob Interface The rotary knob is a 16 detent rotary knob. Each detent position indicates
a "click" clockwise or counter-clockwise. The change in detent position is
detected via a 2 bit quadrature code that changes value every time the
rotary knob is moved into a detent position. Also included in the rotary knob
is a push button switch that is operated by a press/release action. This
switch is used to select menu items on the screen.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 11
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 28

Service Manual SC 7000 and SC 9000XL Patient Monitors
2.10.3 SC 9015 Interface The SC 9015 Interface is implemented in the main processor
communication channels. SCC2 has been dedicated as the channel
between the remote monitor and the base unit, and provides a full duplex
transmit/receive channel from/to the remote monitor. This interface enables
the fixed keys and rotary knob on the remote display to control the main
unit, in parallel with controls on the main unit.
2.10.4 Fast Analog Output The ANALOG OUT interface consists of two identical channels. Each
ANALOG OUT channel provides a 12 bit D/A function. The design uses a
dual DAC to produce the D/A conversion. The sampled analog data is then
passed through a 2 pole low pass filter. The analog output has a maximum
delay of 20ms, and can be used for a defibrillator or balloon pump.
Separate Pacer Spike generation circuits for analog outputs 1 and 2 are
provided.
2.10.5 HiFi Audible Alarm Interface The Audible alarm interface consists of an FM synthesis and Audio DAC
chip set. There is also power amplifier drive circuitry for the two speaker
interfaces: the internal speaker located in the base unit and the speaker
located in the remote CRT. Circuitry has been included to provide a
mechanism for automatically generating an error tone when a watchdog
failure occurs via the piezo alarm (see Section 6.1.8)).
The chip is loaded with tone frequency, pitch, harmonics, and volume
information by the host processor, which controls the duration of the tone.
The audio DAC converts the received sampled tone data and produces a
sampled analog representation of the tone data.
The local speaker interface (also designated as main speaker interface) is
designed for an 8 ohm speaker load. This local speaker interface produces
1 watt of power into an 8 ohm load, and has thermal shutdown capability.
The remote speaker interface is designed to produce a 1Vrms maximum
signal into a 1 kohm load, and provides an ac coupled output.
2.10.6 LED/Status Interface Fi ve LEDs provide information in the present SC 7000 and SC 9000XL
configurations. Two are dedicated to the front end processor, to the DSP,
and two to the main processor.
2.10.7 QRS Sync Out Interface A QRS sync output is provided. The QRS SYNC OUTPUT is an open
collector type output driver that is pulled up to +12 volts (active HIGH). The
output is initialized to Gnd on reset or power on.
This QRS signal is available via an external connector mounted on the main
PC board. High level = +6V min (10KΩ load), +12.6V (no load); Low level
(no QRS) = 1V @ 5ma.
2.10.8 Local Alarm Out Interface A Local Alarm output is provided. This Local Alarm Output is an open
collector type output driver that is pulled up to +12 volts. The output is
initialized to ground (0 volts) on reset or power on (active HIGH).
Loopback status is available via a status read command.
The Local Alarm Out signal is available via an external connector mounted
on the main PC board.
2.10.9 Remote Alarm Out Interface
for Nurse Call
The Remote Alarm Output Interface is located in the CPS/IDS subsystem.
This output is an open collector output with a +12V pullup resistor, fed from
the monitor. The Remote Alarm Output is silenced when a monitor is
undocked.
12 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 29
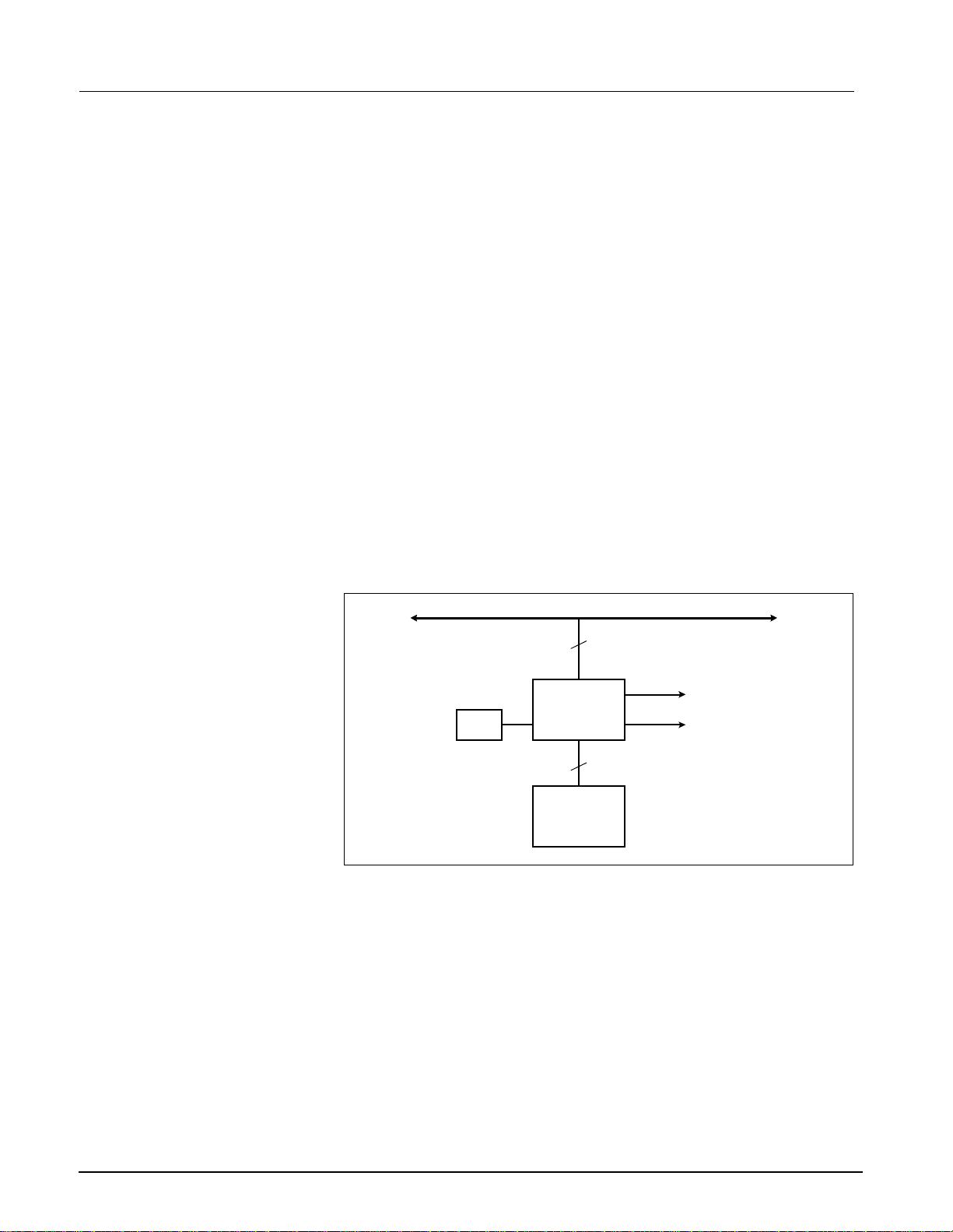
SC 7000 and SC 9000XL Patient Monitors Service Manual
2.11Recorder Interface
2.12Backlig ht Cont rol
2.13Serial EEPROMS
The Recorder interface has been designed to connect to an external
recorder via the base unit docking station connector. The recorder interface
provides all of the necessary control, data and power supply signals
required to drive an external recorder. The interface consists of current
limited DC power and a UART with handshake signals. The UART is
implemented in the main processor FPGA to allow for an extended FIFO.
SC 7000 and SC 9000XL displays require a fluorescent backlight for visibility.
The backli ght in vertor is located o n the fr ont beze l board . Intens ity of th e lig ht
is control led by a variable power ac i nverter and i s bas ed on ambient l ight
detection as well a s operator se l ection. A 10 KH z 6 bi t PWM is implemented
in the main processor FPGA, and a filter on the front bezel b oard converts
this digital signal to an analog volt age to control t he backlight i ntensity.
Four serial EEPROM devices, which contain the Monitor serial number,
Ethernet address, NBP pneumatic characterization and calibration
constants, and monitor setups, are located on the connector I/O board and
are part of the rear housing. If the main processor board is replaced the
monitor will keep its set ups from the se serial EE PR OM s.
Two EEPROMs can be written only at the factory, and contain the Monitor
serial number and Ethernet ID address. The other devices are writable by
the main processor and are changed during service menu setups. These
devices are used for the monitor as well as network setups, device
compatibility, and software feature locks.
3Graphics Subsystem
3.1 Overview
MAIN BUS
32
CRT Interface
LCD Interface
Video
Crystal
VGA Controller
DRAM Video
Buffer
32
Figure 2-4 Graphics Subsystem
The Graphics Subsystem is based on a commercial VGA controller (see
Figure 2-4), and drives both a CRT and LCD display from a local memory
used to refresh the screen. It uses a special video crystal which enables it
to synchronize to most video standards. The graphics chip is capable of
running resolutions such as 800 x 600, when these displays are added to
the monitor. The standard resolution is set to 640 X 480.
3.2 Functional Description
The VGA subsystem is designed to optimize the Bitblit operation, which
allows for quick updates of the screen. This is accomplished by writing
images to non-viewable areas of video memory before they are needed and
copying them to the screen on demand. The copy function is performed by
the VGA controller.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 13
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 30
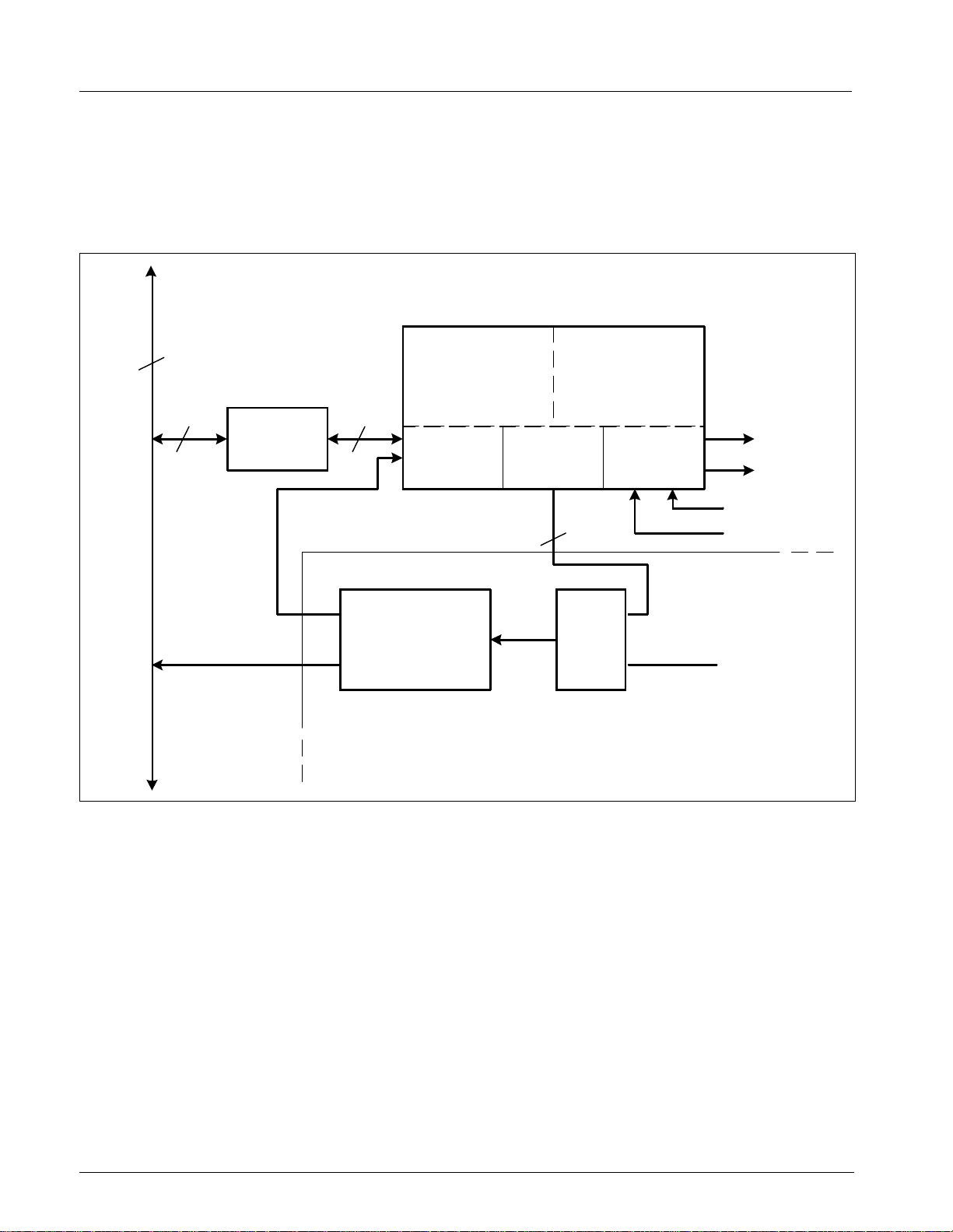
Service Manual SC 7000 and SC 9000XL Patient Monitors
3.3 Video Output
32
32 16
Front
End
Bus
Bus
Sizing
Control
The Graphics Subsystem provides output to an internal flat panel display,
while simultaneously providing the same output for a remote analog
display. The remote display signals are available on the docking station
connector and can drive a standard VGA monitor. The CRT interface uses
three 8 bit DACs for its three color outputs. The front bezel interface is
digital and contains 6 bits for each color.
2181 DSP
32 Kwords
8
SRAM
Serial
Ports
Front End
Processor
Pod Com C & D
Pod Com A & B
Main FPGA
Engine
IDMA
Port
DSP
I/O
Port
Memory
Address
Figure 2-5 DSP Subsystem
4 DSP Subsystem
DSP DMA
Controller
MUX
Main Processor
(Download)
The monitor uses a DSP for preprocessing of oversampled data (see
Figure 2-5). The DSP is a specialized microprocessor that executes high
speed repetitive functions such as digital filters. The DSP acquires data
from the incoming serial pod comm data streams. The data sent to the DSP
is selected by the control words in the pod com memory buffer. Typically
only high acquisition rate data is sent to the DSP.
The DSP has two other communication ports both of which can access the
internal 32Kword memory. The IDMA port is used to DMA data to and from
the common memory. Bus sizing logic converts the DSP 16 bit port to the
32 bit FRONT END bus. During initialization this path is used to download
code to the DSP. The main processor takes control of the DMA port during
this time. Once the system is operational the DSP takes control of the DMA
controller by using its I/O port. The I/O port is a dedicated 8 bit path into the
main FPGA, which allows the DSP access to the DSP DMA controller as
well as other internal FPGA registers, including analog out and QRS sync.
14 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 31

SC 7000 and SC 9000XL Patient Monitors Service Manual
d
d
d
d
Common RAM
Memory Buffers
Front
End
Bus
32
32
32
Channel A
Data In
Data Out
16
DSP
Serial
CH A & B
16
1616
DSP
Serial
CH C & D
16
M
U
X
M
U
X
Channel B
Data In
Data Out
Main FPGA
DMA
Channel A
DMA
Channel B
DMA
Channel C
DMA
Channel D
Channel C
Data In
Data Out
Pod
Com
Pod
Com
Pod
Com
Pod
Com
Channel D
Data In
Data Out
64K Samples/sec
64K Samples/sec
64K Samples/sec
64K Samples/sec
64K Samples/sec
64K Samples/sec
64K Samples/sec
64K Samples/sec
M
U
X
Pod Com
Isolation
Pod Com
Isolation
Cartridge
Interface
Pod Com
Isolation
Pod Com
Isolation
MultiMe
Front En
HemoMe
Front En
etCO
2
Cartridge
Pod 1
Pod 2
(16 bit Samples)
Figure 2-6 POD Communications
5 POD COM
Subsystem
A pod is a front end device that acquires data for a particular set of
parameters. A pod may contain a processor and return preprocessed data
or it may provide raw A/D samples.
Refer to Figure 2-6.
5.1 Overview
Data acquisition of the monitor is controlled by several DMA controllers that
operate on circular buffers residing in common memory on the FRONT
END bus. There are four channels, each allocated a 16 bit transmit buffer
and a 16 bit receive buffer. It takes four 32 bit transfers to update one
location in every buffer, since each access consists of high and low data
from different channels. The transmit buffer tells the pod either what sample
to take or to change a control setting. The receive buffer contains a/d
samples and status information from the pod. A control register in the FPGA
sets a mux to the DSP’s communication port and connects the selected pod
com channel.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 15
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 32

Service Manual SC 7000 and SC 9000XL Patient Monitors
y
+3.3V
Computer
Section
Docking Station
PSL
Auxiliary
Battery
MUX
V Buss
Enable
Switches
+5.0V
±12V
+40V
Batter
Charger
+12VDC
+40V
Battery
MultiMed
Power
HemoMed
Power
Main
Battery
Figure 2-7 Power Conversion
5.2 Outputs
5.3 Error Handling
Power
Conversion
ASIC
NBP Pump
Pod Com
Backlight
Cartridge
Recorder
Status ControlOn/Off
Main Processor
NBP Valves
The pod com subsystem has four channels. Channel A is dedicated to the
two internal front ends; the MultiMed and HemoMed. Channel B is
dedicated to the cartridge slot in the back of the unit. This connector does
not require patient isolation and has higher power than the pod com
connectors. Channels C and D are both used to communicate with external
pods. They have full patient isolation for both power and data.
The pod com channels provide error detection by performing CRC checks
on data in both directions. CRC errors are reported to the front end
processor through interrupts.
6 Power Conversion
Refer to Figure 2-7.
6.1 Power Control
6.1.1 Power Buss Most monitor loads are powered from a DC power buss, called VBUSS,
within the monitor. VBUSS powers the +3.3VDC, +5.0VDC, ±12VDC,
+40VDC and charger power converters. VBUSS also powers the external
pods, cartridge, strip recorder and backlight. The NBP pump and valves as
well as the internal multimed and hemomed front ends are powered from
the regulated +12V supply.
6.1.2 Control and Load
Sequencing
16 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
The switching of the VBUSS power inputs and the power converters is
managed by the power supply gate array. This gate array controls the
power on and power off of the monitor, and the battery charging process.
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 33

SC 7000 and SC 9000XL Patient Monitors Service Manual
It also provides a safety timer for the NBP pneumatics, which are controlled
by the main processor FPGA.
Logic circuits on the main gate array sequence the power to the Pods,
Cartridges, and Recorder to reduce power on load transients.
6.1.3 Power On / Off The monitor is normally switched on by the user pushing the On/Off button
for at least 1 second. (The monitor may switch on when the switch is
pushed for as short a time as 50 msec.)
The power down sequence may be initiated either by the user pushing the
on/off switch for at least 1 second or when the batteries are depleted. When
the power down sequence is initiated, the power conversion board control
logic generates an interrupt for the processor. 100 ms later, the power
supply shuts down. An immediate shutdown is initiated if a power fault
occurs (such as overvoltage).
6.1.4 Power Source Control Power for the monitor is provided by the Docking Station / PSL, External
(Auxiliary) Battery, or Main (Internal) Battery.
The PSL and Docking Station inputs are wired in parallel and are therefore
treated as a single power source. This input is monitored by a voltage
comparitor to determine that adequate voltage is present for Dock Power
operation. The main and external batteries also have voltage comparitors
indicating that their voltage is high enough to provide power.
Based on the information provided by the comparitors, a power source is
connected to VBUSS in the priority of docking station, external battery, and
then main battery.
6.1.5 Battery charging The battery charger is a two-level constant voltage charger with a fixed
current limit and temperature compensated voltage levels. When the
docking station power comes on, the main battery is fast charged at the
high voltage until the current drops below a specific threshold. Then the
charger switches to charge the auxiliary battery. When both have been
charged, the charger voltage drops to the lower “float” voltage and is time
multiplexed between the two batteries.
Since the presence of the auxiliary battery is established by the voltage
comparitor, a means for detecting that it has been unplugged during the
charging process is necessary. For this reason, the external battery voltage
comparitor is disabled during the battery’s ”float” charge interval. This
function is not needed during the fast charge interval since no current will
flow when the battery is disconnected and the fast charge m ode will be
exited automatically.
The fast charge cycle for the main battery is initiated every time the docking
station power comes on. The auxiliary battery will fast charge every time the
main battery finishes the fast charge or when the main battery is charged
and the auxiliary battery is plugged in.
6.1.6 Indicator LEDs Two green LED indicators on the front bezel of the monitor indicate power
and charger status, as given in Table 2-1.
Table 2-1 Power and Charger LED Indicators
LED CONDITION LED STATE
Power Processor power on on
processor power off off
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 17
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 34

Service Manual SC 7000 and SC 9000XL Patient Monitors
Table 2-1 Power and Charger LED Indicators (Continued)
LED CONDITION LED STATE
Charger Docking station power on on
Docking station power off off
*Battery or power fault off
* The charger LED is off if the main battery temperature is
excessive or if there is a power fault.
6.1.7 Power Mode Indication The source of power is indicated to the processor via the power mode bits,
as given in Table 2-2.
Table 2-2 Power Mode Table
MODE1 MODE0 INDICATION
1 X operating on dock power
0 0 o pe r ati n g o n au x iliary battery
0 1 operating on main battery
6.1.8 Piezo Alarm The piezo alarm activates at power up, power down, and if a software
watchdog is activated. At turn on, the software shuts the piezo off after two
seconds. The piezo functions are as indicated in Table 2-3.
Table 2-3 Piezo Alarm
Cause Du r ation
Turn on 2 seconds
Turn off >4 seconds, <10 seconds
Processor watchdog Continous (until sucessful reboot)
+5V Undervoltage >4 seconds, <10 seconds
+3.3V Undervoltage >4 seconds, < 10 seconds
6.1.9 Fault Protection Reverse polarity protection for the batteries and the PSL input are provided
by shunt diodes and fuses on the connector board. There is also a fuse in
series with the internal battery harness. +5V, +3.3V, and +12V supplies are
provided with overvoltage protection.
The main battery has a temperature sensor that is used to disable charge
or discharge of the battery if the temperature is excessive. The auxiliary
battery has a thermostat (65 ±5°C) built in to prevent operation or charging
if an overtemperature condition exists.
A temperature sensor in the power supply section of the main board will
shutdown the power system if the board temperature is excessive.
All power converters are fused to limit fault currents.
6.1.10 External Pod and Cartridge
Overload Protection
The external pods and cartridge current limit circuits are implemented in the
following manner:
When an overload occurs, the load is switched off after the 0.2 second
overload timeout. A retry occurs after 5 seconds.
18 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 35

SC 7000 and SC 9000XL Patient Monitors Service Manual
6.2 Electrical Specifications
6.2.1 Power Supply Input Docking Station, PSL Source (measured at monitor connectors)
The following speci fications indicate the desi gn limits of the power system
and do not relate to a present design configuration of the SC 7000 or SC
9000XL.
11.0 to 15 volts DC @ 6.0 Amps Max.
Buss Fault Detection <8.97 V±1%
Battery Source: 12V Lead Acid, 9.8 to 15 VDC @ 6.0 Amps Max.
Note: Due to the voltage measurement tolerance of the battery
comparitors, and resistive voltage drop, all VBUSS loads must
function to a minimum voltage of 9.4 volts. They must also ride
through a VBUSS dip of 0.4 volts for 25µsec.
6.3 System Power Specifications
6.3.1 Maximum Power Summary Total 68.2 Watts
Typical transport power = 19.4 watts (backlight = low, NBP = 15 min.
interval, no pods or cartridges, taxi and ethernet disabled, no alarms)
6.3.2 Main Battery Specifications Voltage 12V
Capacity 3.4 Ah
Discharge Time 75 minutes
Charge Time 4.5 hours
6.3.3 External Battery
Specifications
7 Front Bezel Board
7.1 Introduction
7.2 Functional Description
Voltage 12V
Capacity 2.3 Ah
Discharge Time 50 minutes
Charge Time 3.5 hours
The Front Bezel Board provides an interface to the various operator related
functions. The interface consists of circuitry and connectors that allow the
main processor to access all of the operator related functions.
The Front Bezel Board provides an interface between the main board and
the front bezel components. It is a cable harness for these components and
is unique in its construction. The front bezel board is made with a process
called "rigid - flex" allowing the board to act as a flex cable. This board may
be flexed for service, however CARE must be taken not to bend this
material at a sharp angle. This process allows direct connection to the LCD
assembly. The front end board mates to the main processor via a "floating"
44 pin high density D connector. This connector has a mechanical float to
allow the front and back of the unit to be snapped together without concern
for a cable between the two halves. The 44 pin D connector attaches to the
processor board with a flex cable.
The Front Bezel Board provides connectors and circuitry need for the
following functions:
• LCD display and Power Switch
• LCD Backlight Invertor
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 19
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 36

Service Manual SC 7000 and SC 9000XL Patient Monitors
• ambient light sensor
• base unit rotary knob and keypad interface
• battery and power LED's
• Jumper for selecting LCD power voltage (currently +5V)
7.3 LCD Backli ght Invertor Interface
7.4 Ambie nt Lig ht Interface
7.5 Local Rotary Knob/ fixed Keys Interface
7.6 Battery/power LED Interface
The Backlight circuitry for the LCD backlight is resident on the front bezel
board. The backlight inverter converts VBUSS power from the main board
to the high voltage ac power used by the backlight. The voltage may be
controlled by a digital PWM input supplied by the processor board.
The base unit's ambient light sensor is mounted on the front bezel board.
The ambient light sensor is a photocell that exhibits a logarithmic change
in resistance vs. light intensity. The ambient light sensor is connected in
series to a 2kΩ potentiometer which is used to calibrate the ambient light
sensor at the factory.
The SC 7000 and SC 9000X L base units eac h have twelve fix ed keys. An
additiona l ke y is dedi cat ed as t he power on/s tandb y swi tc h. The ro tary knob
interfac e prov ides a 2-bit encode r ou tput and also a ro tary knob pus h but ton
signal ou tput . A ll of t he ke y/r otary kno b signa ls are f ilt ered . Al l of th e key pad
switches hav e pul ldowns except the power on/standby switch . Thus, the
power switch signal output from the Fron t Bezel board is pulled up by the
power switch i nterface loc ated in the power supply sect ion.
The battery LED is turned on or off via the associated LED control signal
from the main board. The power LED is connected to +5V. Both the battery
and power led's are green when turned on.
The power and battery LED's have been integrated into the membrane
switch interface used for the fixed key and power on/standby switch. The
LED on/off control signals are provided by the base unit's power supply
section. Thus, the LED control signals originate in the power supply,
8 MultiMed Front End
8.1 Introduction
8.2 Safety
The MutiMed front end section of the main board combines 6-lead ECG, 2lead respiration, temperature, and saturated oxygen data gathered by the
MultiMed Pod from transducers at the patient and converts them to digital
form for transmission through isolators to the computer section of the main
board. This section also houses the NBP pressure transducer which uses
the same acquisition system. See Figure 2-8 on page 21.
The hardware design uses a single oversampling 16 bit converter to
measure all of the parameters. This allows bulky analog filters to be
replaced by software filters. Careful shielding and filters protect against
very high frequency interference from upsetting measurements.
• Patient isolation withstands 5kV during defib.
• Leakage currents are limited to safe values normally and during single
fault conditions.
• Patient is protected against electrosurgical burns at the electrodes.
• Defibrillation protection does not drain excessive current away from
the patient.
20 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 37

SC 7000 and SC 9000XL Patient Monitors Service Manual
g
Temp
ECG
Resp
SpO
Protection
2
MultiMed
Defib
ESU
NBP
Hose
RF Filter
Lead Off
Neutral
SW
Lead
Select
Modulator
Pressure
Transducer
Pre-
Amp
Modulator
Demodulator
LED Drive
Linearizer
Low-Pass
Filter
Bandpass
Filter
Current
Sources
Bandpass
Filter
Power Monitor
Amp
Amp
Amp
Amp
Temp
Temp Ref.
ECG
Pace
Amp
NBP
Resp
4
2
2
6
4
2
M
U
X
2
Converter
Control
16 Bit
A / D
Asic
Data Control
Differential
I/V
Converter
Ambient
Li
ht
Rejection
Demodulator
Cal Resistor
Red
I/R
Power
Pod Com
Figure 2-8 MultiMed Front End
• Specially shielded connectors and cables are used to provide
excellent immunity up to 1000MHz and can not be touched by patient
even when disconnected.
• Single cable from MultiMed Pod to main SC7000 or SC 9000XL unit
reduces clutter between bed and monitor.
8.3 Functional Description
Transducers gather physiological data at the patient and feed them into the
small MultiMed Pod at the bed. The MultiMed Pod in turn is connected via
a 3-meter cable to the MultiMed front end in the main unit where analog
ECG, Respiration, Temperature, and SpO
signals are converted to digital
2
form and sent through isolators for processing.
8.3.1 ECG/Resp The MultiMed Pod located close to the patient accepts a set of 3, 5 or 6 shielded ECG electrode leads, an SpO
(Nellcor) cable adapter, and a
2
temperature sensor. The ECG section contains RF filters, and overvoltage
clamps that include 1k series resistors to limit shunting of defi brillat or
current. The SpO
and temperature sections also contain RF filters.
2
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 21
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 38

Service Manual SC 7000 and SC 9000XL Patient Monitors
Impedance respiration is sensed through the ECG electodes. Void-free
potting and internal shielding enable compact containment of high voltage
defibrillator and electrosurgery pulses. The small interconnecting cable to
the main assembly is captive at the MultiMed POD but plugs into the
MultiMed front end via a specially shielded connector.
The front end accepts physiological signals from the MultiMed POD
connector and feeds temperature, respiration, and ECG signals via RF
filters, configuration multiplexers, and pre-amplifiers to a high-speed
multiplexer driving a 16-bit analog-to-digital (A/D) converter. The data
stream is sent to the Main Processor board via an opto-isolator. Control
commands from the Processor are sent out to the front end on a similar
isolating link. Isolated DC power is also provided.
The ECG signals are conducti vely coupl ed to the i solated ci rcuits via current limiting series resistors, whe reas the SpO
signals ar e optically is ol ated at
2
the trans duc er. Temperatu re s i gnals are doubl y insulated at t he patient by
disposab l e boots on the sen sor s. AC (40kHz) excitation currents f or
respiration monotoring are dc-isol at ed by high-vo ltage ceramic capacitors.
The A/D samples the following parameters:
Table 2-4 Parameter Sampling Table
Parame ter # of Channels
ECG 4
Pace 2
SpO
Red 1
2
SpO
IR 1
2
NBP 1
Resp 1
Temp 2
The pace signal samples are used directly by the DSP to detect pace
pulses. All other signals are decimated and filtered using digital signal
processing to the above specifications. Additional filtering is user selectable
and invokes additional digital signal processing in the computer section of
the board. The high oversampling rate is required to minimize the
requirements (and size) of the analog anti alias filters. Superior rejection to
ESU and other types of interference is achieved with this type of design.
ECG • Pacer pulses may be detectable by software on two lead-pairs.
• Bandwidth is set flexibly by software filters.
• Reconfigurable neutral selector can drive any electrode.
• Lead-on detection functions with even poor electrodes.
• Calibration voltages can be superimposed on patient wave-forms or
onto flat baselines.
See Figure 2-9. Composite electrocardiographic (ECG) signals generated
by the heart and by a pacemaker are filtered to reduce RF interference from
impedance respiration and electrosurgery and then injected with dc lead-off
detection currents. Over-voltage clamps protect the semiconduct ors from
the surges passing the sparkgaps in the MultiMed Pod and also reduce the
dc current applied to the patient due to a component fault.
22 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 39

SC 7000 and SC 9000XL Patient Monitors Service Manual
+ Clamp
RF Filter
RA
LL
LA
Chest
RF Filter
RF Filter
RF Filter
MUX
- Clamp
+ Clamp
- Clamp
+ Clamp
- Clamp
+ Clamp
- Clamp
+ Clamp
Wilson
Star
Demod
Augmented
Leads
RA
aVL, aVR,
aVF
LL
Ref
LA
Chest
Resp
RA
Normal Leads
RA
I
II
LA
V
W
Chest
III
LL
LA
aVLaVR
aVF
RF Filter
- Clamp
RLRL
Augmented Leads
LL
Figure 2-9 Lead Forming Network
The Wilson point, "W", the average of the LA, RA, and LL electrode
potentials, serves as the negative reference potential for the V and V' leadpairs and is also used as a measure of the common-mode potential of the
patient Figure 2-9. By driving the isolated comm on of the front end at the
same potential as the Wilson point, the common-mode voltage across the
electrodes is reduced nearly to zero and the effective common-mode
rejection is improved. As most of the common-mode current is now forced
through the neutral electrode, it becomes noisier and hence is not used as
part of another signal path. Switches are provided to select other electrodes
to be neutral if the RL electrode is off or missing. If the V' electrode is
present, then it can be selected to be neutral so that the three Einthoven
and the V lead pairs can stil l b e used. Howeve r, the V' lead-pair w ill be
corrupted due to neutral current noise. Similarly the V electrode can be
selected to be neutral. Now that the RL is disconnected from the neutral
driver, its potential can be monitored to determine whether it has been
reconnected to the patient and thus is able to be reselected to be neutral.
If only the three Einthoven (LA, RA, and LL) electrodes are connected, one
is selected as neutral leaving the remaining two electrodes to form one valid
lead-pair. The "W" now contains the neutral drive signal which bypasses
the neutral electrode and reduces the gain of the neutral driver amplifier. To
improve the resulting poor common-mode rejection, a Wilson Grounding
"WG" switch is activated to selectively disable the offending input to the
"W".
Respiration Refer to Figure 2-10 .
• Respiration is both ac- and dc-coupled in hardware. DC is used for
high Z sensing; ac is used for signal acquisition.
• Respiration may be monitored on leads I and II.
• Detection sensitivity has low dependence on base resistance or
electrode unbalance.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 23
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 40

Service Manual SC 7000 and SC 9000XL Patient Monitors
Figure 2-10 Respiration Functional Block Diagram
Impedance respiration is monitored by injecting a nominally 40kHz square
wave of current into one ECG electrode and removing it at another ECG
electrode. The resulting 40kHz voltage drop across those electrodes is
proportional to the impedance. Specially balanced true current sources do
not load the ECG electrodes or distort the ECG morphology. The waveform
of the current is preemphasized to reduce bypassing effects of cable
capacitance. The returning 40kHz differential voltage is amplified,
synchronously demodulated , and low-pass filtered. The resulting dccoupled waveform is converted to single-ended form, further low-pass
filtered, and passed to the A/D multiplexer. An ac-coupled stage with an
"autobloc" dc-restorer feeding a separate input to the A/D multiplexer also
provides additional gain.
Figure 2-11 Temperature Functional Block Diagram
8.3.2 Temperature Refer to Figur e 2-11 .
• Designed to meet the stringent German PTB requireme nts including
detection of marginal accuracy due to degradation of a single
component.
• A second temperature channel is also available.
Temperature is sensed at the patient by a non-linear negative-temperaturecoefficient thermistor. This is linearized with a precision resistor network
and excited by the same reference as the A/D converter to a produce
ratiometric digital output. An input multiplexer (MUX) selects among the
external signal and internal reference dividers simulating -5 and +50°C. The
dc amplifier matches the dynamic range of the A/D by combining,
amplifying, and precisely offsetting the small signal from the multiplexer.
Power supplies whose failure would invalidate temperature measurements
are also monitored and compared against the A/D reference.
24 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 41

SC 7000 and SC 9000XL Patient Monitors Service Manual
DAC
8.3.3 SpO
MUX
$'&
Figure 2-12 SpO2 Functional Block Diagram
2
Determination of the concentration of oxygen in the blood depends on the
principle that the absorption of red (R) light depends on the degree of
oxygenation of the blood, whereas the absorption of infrared (IR) radiation
is independent of oxygenation and causes only constant attenuation. Refer
to F igure 2-12. In the SpO
sensor, R and IR emitting leds are alternately
2
pulsed on at a 25% duty cycle. The intensity of light (inc lud i n g ambient )
transmitted through or scattered by the blood is converted to a current by a
photodiode in the sensor. The current that appears when both leds are off
depends mainly on the ambient light. This ambient contribution is later
subtracted to leave only the R or IR signal levels. The large dynamic range
of the light intensities requires constant automatic monitoring and
adjustment.
The intensities of the R and IR sources are independently controlled by two
digital-analog converters attenuating the 2.5V reference.
Attenuated radiation falling on the photodiode in the sensor is converted to
a current which passes through an RF filter balun in the HVPOD and enters
the current-to-voltage converters in the MultiMed front end. The resulting
unipolar stream of pulses is then ac-coupled to a controllable-gain
differential amplifier. The signal is then synchronously demodulated into
Red and IRed signals with ambient light subtracted. Additional gain control,
filtering, and signal offset are provided for each signal prior to A/D
conversion.
The calibration of each sensor is coded into the value of a precision resistor
built into the sensor. The value of this resistor is sensed by forming a
voltage divider. The value of the resistor ratio is read by a separate A/D
input, and out of range values are interpreted as “sensor unplugged.”
Communications The multiplexers and A/D are controlled by the Main Processor via a
Manchester-encoded serial communications chan nel (Pod Com) optically
coupled to the isolated front end. Most of the digital logic is contained in the
MultiMed FPGA. Outputs from the A/D are Manchester-encoded in the
MultiMed FPGA and fed to the opto-coupled data flow to the Main
Processor.
A power-on monitor resets the FPGA until both ±5V have risen to normal
range. The isolated dc-dc converters are synchronized to the data
acquisition sequence via the Main Processor FPGA. The A/D converter is
automatically calibrated after the power-on reset is cleared.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 25
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 42

Service Manual SC 7000 and SC 9000XL Patient Monitors
9 NBP
9.1 Introduction
9.2 Pneumatic Subassembly
Figure 2-13 NBP Functional Block Diagram
Refer to Figure 2-13.
The NBP design measures blood pressure non-invasively using an
inflatable cuff and the oscillometric method. The NBP algorithms are
performed in the front end processor. The NBP circuit contains two
pressure transducers which measure the hose pressure. The second
redundant pressure sensor is used to measure overpressure for safety.
This pressure transducer is mounted in the power section while the other
pressure transducer is mounted in the MultiMed front end. A plastic
manifold connects the two transducers together and to the pneumatic
assembly in the rear case. The MultiMed front end A/D samples the
pressure transducer.
The pneumatic subassembly cons ists of two modulating solenoi d valves
(V1, V2), a pump (P1), a filter, and a manifold. The manifold provides the
interconnection of the air passages between the individual components and
provides for their mechanical mounting. It also provides an acoustic
attenuation of the valve and pump noise. The filters prevent contamination
from entering the pneumatic system from the cuff hose or ambient air.
P1 provides the pressurized air to inflate the blood pressure cuff. V1 and
V2 are used to control the air flow during the de-flation phase of a blood
pressure measurement. V1 is a normally closed exhaust valve with a
relatively small orifice. V2 is a normally open exhaust valve with a
comparatively large orifice.
When a blood pressure measurement is initiated V2 is closed, P1 is turned
on and the rising cuff pressure is monitored via pressure transducers.
When the pressure has reached the target inflation pressure, P1 is turned
off. Neonate inflation cycles are identical exc ept that a speed control circuit
is used to reduce the pump output to approximately 15% of the adult mode.
After the inflation, there is a short delay after the pump stops to allow
26 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 43

SC 7000 and SC 9000XL Patient Monitors Service Manual
thermal transients to settle. Either V1 or V2 is now modulated to control the
deflation rate. The choice of V1 or V2 and the initial pulse width is made
based on the inflation cycle. The chosen valve is modulated and the pulse
width (open time) is continuously adjusted to provide a constant deflation
rate. If initial deflation was started with V1 the software may determine that
it needs to switch to V2 to maintain proper deflation. In any case when the
measurement cycle is complete, V2 is opened fully (de-energized) to allow
for rapid deflation.
9.3 Transduce rs
9.4 Pneumatic Controls
The measurement pressure transducer is DC coupled to a 16 bit A/D
converter so that cuff pressure is measured with adequate resolution to
detect blood pressure pulses.
The overpressure transducer has two threshold settings. The adult setting
is 300 ±30 mmHg and the nominal neonatal setting is 158 ±7 mmHg. Both
transducers share a common manifold and are mounted on the main PC
board.
The P1 control provides 3 functions.
• It limits current to the pump when the pump starts to prevent power
supply overload.
• It rapidly decelerates the pump when the pump is shut off, by applying
a low resistance across the motor.
• It provides a closed loop speed control for low speed neonatal operation.
A relatively high pulse voltage is used to drive V1 and V2 to get quick
response. This pulse lasts for approximately 2 milliseconds after which time
the valve voltage is lowered to a holding value. At the end of the valve "on"
time period, the valve voltage is allowed to reverse and the energy stored
in the solenoid inductance is rapidly released into a relatively high voltage
clamp circuit.
P1 and V2 are supplied by a redundant power switch so that, under fault
conditions, they can be de-energized.
9.5 Safety timer
9.6 Logic gate array
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 27
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
The software limits measurement time to 119 secs for adult mode, 89 secs
for neonatal mode and 59 secs for French neonatal mode. A safety timer
circuit monitors current in P1 and V2, and if due to some failure (hardware
or software), P1 or V2 remain activated for more than 120±1 seconds in
adult mode, 90±1 seconds for neonatal mode or 60±1 seconds in French
neonatal mode, the circuit latches on, causing the redundant power switch
to P1 and V2 to switch off. W hen the safety ti mer latch has b een se t, V1 is
opened as an additional safety feature. Only recycling the monitor resets
the safety timer latch. The safety timer circuit is functionally independent of
the logic gate array.
When the unit is powered up, the safety timer is de-activated until the pump
is started the first time. This feature allows service calibration without
triggering the safety timer. Once the pump has been activated the timer
circuit becomes functional.
The main FPGA provides the following control functions for the pneumatics
and the communications.
• Clock generation for safety timer
• 12 bit 20 Hz PWM and pulse control for V1 and V2
• Pump control
NOT A CONTROLLE D DOCUMENT
Page 44

Service Manual SC 7000 and SC 9000XL Patient Monitors
• Neonatal mode switching of pump and overpress ure
• Safety logic
9.7 Non-volatile memory
9.8 Hose detection
9.9 Watchdog Timer
Press
Transducers
HemoMed
Cardiac
Output
Keypad
A EEPROM stores pneumatic component flow factors. During calibration at
production system test and in the field, a 0.5 liter canister is connected to
the NBP input on the monitor. The monitor automatically measures the
pump and valve flow rates and determines their flow factors for the use in
the flow control algorithm.
An electromagnetic coil located at the hose connector detects the metal in
the hose connector when the connector is present.
A watchdog timer is implemented in the power conversion FPGA to monitor
the safety timer clock input from the main FPGA in case the main FPGA or
its crystal become damaged.
Keypad
Power Monitor
4
2
Linearization
Clamp and
Filter
Pressure
Excitation
Pressure
Sense Excitation
Reference
Temperature
Temperature
(Inj. blood, .7R)
4
Converter
Control
16 Bit
A / D
Asic
Data Control
M
U
X
2
3
Figure 2-14 HemoMed Front End
10HemoMed Front End
10.1Introduct ion
10.2Pressure
Power
Com
Pod
Refer to Figure 2-14. The HemoMed front end section of the monitor’s main
board takes invasive blood pressure, and thermal dilution cardiac output
data gathered by the HemoMed Pod from transducers at the patient and
converts them to digital form for transmission through isolators to the
computer section of the main board. The HemoMed front end may also be
used with a single or dual pressure cable instead of using the HemoMed.
The pressure data acquisition front end is designed to operate with resistive
strain gage pressure transducers having an output impedance of less than
3000 Ohms and an input impedance between 3000 and 200 Ohms.
Excitation voltage is applied in pairs. Press 1 and 3 share a driver as well
as Press 2 and 4. The output signals generated from the pressure sensors
are passed through filter and clamp networks which limit and filter RF noise.
The pressure excitations are monitored for fault detection.
28 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 45

SC 7000 and SC 9000XL Patient Monitors Service Manual
10.3Cardiac Output
The two thermistor signals are connected to a precision resistor network to
linearize voltage vs temp curve of the thermistor. The thermistor signals are
filtered and clamped before amplification. Two calibration voltages are also
sampled by the A/D converter to correct amplifier offset and gain errors.
The catheter also has a reference resistor which is read for calibration.
The front bezel switches on the HemoMed are converted to unique voltages
when pressed, allowing a voltage to be sent to the A/D converter, which can
be decoded by the front end processor into the corresponding switch
closure.
11 etCO2 Module
Figure 2-15 etCO
Sensing Process Functional Block Diagram
2
The etCO2module non-invasively monitors end-tidal CO2 using a technique
that relies on the selective absorption properties of the CO
to specific
2
frequencies of infra-red radiation. See Figure 2-15.
In the sensor a thick film infra-red source is pulsed at a rate of
approximately 87 Hz, generating a broad- band spectrum of IR. Selective
filtering separates this into two narrow regions, one inside and one outside
the band of CO
the band of CO
energy since the signal it receives is not affected by CO
baseline which serves as a Reference for the level of CO
absorption. The detector associated with the filter outside
2
absorption records the maximum level of the source
2
. It provides a
2
in the airway.
2
The other detector senses a filtered energy level modified by the presence
of CO
. As the level of CO2 increases, the CO2 gas molecules in the airway
2
absorb more of the light energy and less signal reaches the detector. This
signal, converted by the detector, is referred to as the Data signal. Current
through the thick-film source is bidirectional to offset the tendency of
particles within the source to migrate when exposed to a strong
unidirectional electric field caused by current flow only in one direction. This
keeps the structure of the source uniform and enhances system integrity
and life of the product.
To acquire a precise level of CO
sampled and the level of CO
, both channels are simultaneously
2
is determined from the ratio of the Data and
2
the Reference channels. The ratio is compared to a look-up table in
memory to establish the correct value in units of mmHg.
The module then sends the results to t he host system for f urther processing
and display.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 29
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 46

Service Manual SC 7000 and SC 9000XL Patient Monitors
11.1System Hardware
11.2System Memory
The module is a three-part system composed of a Digital Board, an Analog
Board, and an Accessory Assembly. The Digital Board has two major
functional areas: the power supply section and the bulk of the digital control
logic. The Analog Board provides for data acquisition and conversion, and
contains the servos for controlling the temperature of the case and detector
heaters, and the source pulser used to control the probe. The Accessory
Assembly contains the CO
calibration switches and calibrator EEPROM).
The system has three types of memory:
• PROM Programmable Read Only Memory
• SR AM Stati c Rand o m Acce ss Memo r y
• EEPROM Electrically Erasable Read Only Memory
PROM stores the module's program. Its contents remain intact even when
power is removed from the module. It has been socketed to allow for future
program updates, if required. Besides containing the module's program, it
also contains various look-up tables for calculating CO
the Interrupt Vector Table.
The system's Static RAM functions as a scratch pad to temporarily hold
various system variables until they are either no longer needed by the
system and are overwritten with new information, or power is removed from
the module and the RAM contents are lost.
sensor and the Calibrator (that contains the
2
parameters and
2
11.3User Interface
12HEMO 2/4 POD
12.1Functional Description
12.2Pressure
The EEPROM holds system parameter information that must be retained
when power is removed, but must also be modifiable by the processor. The
device contains multiple copies of system information such as calibration
factors, sensor serial number, and span cell number, to ensure data
integrity.
A Supervisor chip performs various monitoring tasks to ensure that the
microprocessor and system run properly.
The user interface provides capability for airway and adapter calibration,
and also compensation for effects of N
accessory assembly, switches inside the sensor, one for the Zero Cell and
one for the Span Cell, tell the processor when the assembly has been
placed on the proper cell for system calibration.
HEMO 2/4 PODs have provisions for monitoring either 2 or 4 invasive blood
pressures, 2 temperatures and cardiac output. See Figure 2-16
The pressure data acquisition front end is designed to operate with resistive
strain gage pressure transducers having an output impedance of less than
3000 Ohms and an input impedance between 3000 and 200 Ohms (see
Figure 2-17). Excitation voltage is applied, one at a time, to each resistive
strain gauge pressure transducers by a single, current limited voltage
reference circuit which is time-multiplexed across four pressure sensors.
The differential output signals generated by the pressure sensors are
passed through filter and clamp networks which limit the differential and
common mode voltage swings and filter out RF noise.
O and O2. When calibrating the
2
30 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 47

SC 7000 and SC 9000XL Patient Monitors Service Manual
ZERO
S1L
SWITCH TIMING BUS
S2L
S3L
S4L
PRESSURE SENSORS
TEMPERATURE SENSORS
O.7R
R?
T
1
1
BLOOD TEMP
T
21
P
A
2
P
A
2
P
A
21
P
A
T
T
INJECTATE TEMP
4 VOLTS
CLAMP AND
FILTERING
NETWORKS
+4.0 VOLTS
LINEARIZE
FILTER AND
CLAMP
A
A
A
CURRENT LIMITED
VOLTAGE
REFERENCE
DIFFERENTIAL TO
SINGLE-ENDED
CONVERTER AND
4 TO 1 MULTIPLEXER
(USING FLYING
CAPACITOR
TECHNIQUE)
I1L
I2L
I3L
VOLTAGE
REFERENCE
T1
T37
T10
CAL POINTS
T2
R_EDWARDS
GROUND
I4L
PA0
PA1
+5V OUTPUT
A
-5V OUTPUT
4PRESS
200 mmHg
0 mmHg
CALIBRATION CONSTANTS
TA1TA0
MUX
OFFSET
+
+
MUX
A
OFFSET
FIXED GAIN OF 10
+
+
+5V MONITOR
A
-5V MONITOR
FIXED GAIN OF 20
NON-ISOLATED
SWITCHING POWER
SUPPLY
MUX
4PRESSL
200mmHGL
ZEROL
+12V INPUT
200KHZ SYNC SIGNAL
FIXED GAIN OF 311
A
TCA1TCA0
MUX
FIXED GAIN OF 2
A
PUSH
CO START
BUTTONS
WEDGE
A
DATA AND CONTROL
LOGIC GATE ARRAY
D
16 BIT
LCD
CONTROLLER
LCD
DATA
CLOCK
DATA TRANSMITTER
DATA RECEIVER
PROTECTED
MANCHESTER
DATA OUT
MANCHESTER
DATA IN
EEPROM
WRITE
EEPROM
R/W
Figure 2-16 HEMO 2/4 POD Functional Block Diagram
Figure 2-17 IBP Functional Block Diagram
Next, the signals enter a functional block that converts the differential
signals into single ended signals which are then presented one at a time in
a time-multiplexed fashion to a fixed gain single ended amplifier.
Calibration voltages for zero and 200 mmHg are periodically switched into
the amplifier input to correct errors in amplifier offset and gain respectively.
An A/D converter samples the resulting output voltage. Timing is
coordinated by the logic gate array.
12.2.1 Temperatu re Each of two thermistors is connected to a functional block that consists of a precision resistor network to partially linearize the voltage verses temperature transfer curve of the thermistor. This functional block also consists of means for filtering RF noise and limiting the voltage swing. A 4.5 Volt reference is connected to power each linearization network.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 31
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 48

Service Manual SC 7000 and SC 9000XL Patient Monitors
A multiplexer selects one of the two temperatures or one of the two
calibration points and connects the voltage to the input of a fixed gain
amplifier. The two calibration points are used to correct gain and offset
errors in the amplifier circuits.
An offset is added to center the signal within the dynamic range of the A/D
converter. The signal is then further multiplexed with two power supply
voltage monitors and Cardiac Output. A fixed gain of two is finally applied
to match the signal range to the full scale range of the A/D converter.
12.2.2 Cardiac Output Cardiac output operates in much the same way as temperature. The thermistor signals are filtered and clamped then multiplexed to the input of a fixed gain amplifier. Two calibration voltages are also multiplexed in to correct amplifier offset and gain errors.
Next, a n of fset is added to t he signal to center i t to the dynami c range of the
A/D convert er. The amplified signal is t hen multiplex ed with temperature,
then throu gh a fixed gain of t wo and finally t o t he A/D converter.
12.2.3 EEPROM Storage Two EEPROM's are used fo r non-volatile information storage. One EEPROM is used for reading and writing data that changes during the operation of the POD, such as pressure offsets, the other stores more permanent information such as POD serial number and is therefore write protected. A state machine inside the logic gate array supports communications between the Host and the two EEPROM's. A mechanism is provided which allows service personnel to disable the write protection of the otherwise write protected EEPROM.
12.2.4 LCD and Push Buttons A total of 16 LCD characters are provided for use as pressure labels. Each pressure channel is allocated 4 LCD characters. The Logic Gate Array supports communication of controll between the Host and the LCD's.
Up to three push buttons are provided for user interface. There is one for
pressure zero, one for Cardiac Output Start and one spare. The interface
of the buttons to the Host is handled by the gate array.
12.2.5 Current Limiting the Voltage
Reference
13Remote Comm
Subsystem
Hardware
13.1Connection
Characteristics
In the event a defective pressure sensor presents a short circuit to the
excitation voltage source, the voltage source goes into current limit during
the bad transducer's time slot.
The main processor sees the Remote Bus interface to the CPS or IDS
Network as a slave device with a dedicated address space. The responding
devices, however, are in the CPS/IDS. Status bits indicate when the remote
device is connected and powered up, and signal validity on the
communication link. If a proper connect is established, a periodic poll is
sent to the CPS/IDS to up-date the interrupt status to the monitor every 8
microseconds.
Two mechan isms a re used to v erif y phy si cal a tta chme nt t o a do cking st ation.
• First, a hardwired signal between the monitor and CPS or IDS is
activated when a cable connection is achieved. This signal is valid
even if the CPS or IDS is powered off.
• Second, an opto-isolator is activated when a powered CPS or IDS is
attached to the monitor. A current loop is established by current
flowing thru the receive lines, opto-isolator and transmit lines.
A time filter is applied to both functions, such that the function must be valid
for a minimum of 100ms before activating. Deactivation is immediate.
32 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 49

SC 7000 and SC 9000XL Patient Monitors Service Manual
14 I
NFINITY
Network CPS
and IDS (w/ Power
Supply)
14.1Network Board Hardware
The SC 7000 a nd SC 9000 XL hav e been des igned t o functi on i n s tanda lone
mode or in an I
NFINITY NETWORK
The I
communications network controller and a power supply. The CPS/IDS
supplies power and communications interface for an SC 7000, SC 9000XL,
SC 9000, or SC6000 series patient monitor, and for peripheral devices
associated with the monitors. In addition they support two RS232 ports,
access to both CPS/IDS diagnostics and Host diagnostics, and support for
a passive remote display.
The major circuits include a high speed serial link to the Patient Monitor,
control and status registers to the 68302 and 8344 processors, and
miscellaneous functions. The serial link functions as a bus master on the
local bus. The 68302 performs bus arbitration (and provides a serial
channel for communication with an SC6000). The registers and
miscellaneous func-tions are slave devices on the bus and completely
accessible to the 68302.
NFINITY NETWORK
Basic and Device CPSs contain a data
. They are not compatible with SI RENET.
6&
6& ;/
RU
6&
&RQILJ
Figure 2-18 Communications Functional Block Diagram
Motorola 68302 CPU
The Motorola 68302 CPU serves as the processing engine for the
SC6000 serial port link. The 68302 CPU runs at a frequency of
20MHz, and is connected to the CPS Bus. It accesses the FLASH (its
code space) and the 68302 External RAM (its data space) via the
CPS/IDS Bus.
FLASH memory is used for storage and execution of the 68302
software, and also to store care unit specific setups. The 68302
executes its code directly out of the FLASH, and is accessible from the
Bus to provide the ability to program it with new software from an SC
7000, SC 9000XL, or SC 9000 monitor.
Serial Communication Controller - User Interface
Note: The SCC al so provides an SC 6000 series pati ent monitor s li nk.
“SCC3” of the Motorola 68302 CPU provides a diagnostic user
interface, to run embedded diagnostics on the CPS/IDS hardware
and trace operations during software analysis and debugging
sessions. “SCC3” is used with a UART baud rate of 19.2K.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 33
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 50

Service Manual SC 7000 and SC 9000XL Patient Monitors
External RAM is used for software downloader code, runtime stack,
SCC data buffers, monitor configuration data and error logs.
Monitor Connection Characteristics
The net wor k board com m uni cates wit h the att ached monitor by the high
speed serial link (or by the 68302 serial channel fo r an S C6000 series
monitor) . Because of the different characteristi cs of each type of link,
relays are used to select one or the other. (The default selection is t he
SC6000 lin k. ) If an SC 7000, SC 9000XL, or SC 9000 unit is detect ed,
the relays switch to the REMOTE COMM type link. A time filter is
applied to each signal, such that the func tion must be val i d f or a
minimum of 64 mi l liseconds before activati ng. Deactiv ation is
immediat e.
A hardwired signal between the monit or and CPS or IDS i s a ct i vated
when a cable connection is ac hi eved. This si gnal is valid even if the
monitor is powered off . For an SC 7000, SC 9000 XL, or SC 9000
onitor, a curr ent l oop i s es tablis hed by cur rent flow ing thr u t he tr ansmi t
M
lines, op t o-isolator and receive lines . A voltage compa rator activa t es
when the lo op i s sensed. The link is generated when a receive signal is
sensed by the T 1 receiver.
The connection state of the monitor is defined as
14.2EEPROMs
14.3CPS Power Supply
• Monitor docked
• No Monitor
•Error
• Transitional
Note: If the transitional state persists for greater than one second, a
faulty docking or error condition exits
The CPS and IDS contain SERIAL EEPROMs which are programmed in
the factory with various configuration parameters. One contains factoryprogrammed field service data and is read-only in the field. A second
EEPROM is field-programmable and contains various configuration
parameters.
The CPS power supply not only powers the network controller in the CPS
but also powers the docked patient monitor and up to two auxiliary units. It
is a line powered switching power supply capable of operating over the
range of international line voltages without having to be reconfigured.
Manual switching or fuse changing are not required.
The power supply provides a regulated +13 VDC at 7 amps to the monitor
via the docking station, and at 2.3 amps to each of 2 auxiliary docking
stations. The auxiliary docking station outputs are current limited for fault
isolation. A DC to DC converter connected to the +13 VDC output provides
a regulated +5 VDC and ±12 VDC for the network board. A fan speed
control circuit is also provided for cooling the CPS unit.
To eliminate ground potential difference resulting from the return current in
the docking station cable, the +13 VDC output has a 500 VRMS isolation
from earth ground. This isolation is maintained also in the DC to DC
converter for the +5V, ±12V outputs. An earth ground connection is made
to the monitor at the docking station for EMI suppression via the docking
station cable shield. The units connected to the auxiliary docking stations
have ground isolation in their DC to DC converters to eliminate ground
potential differences.
34 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 51

SC 7000 and SC 9000XL Patient Monitors Service Manual
The power supply uses a soft switching (quasi-resonant) square wave
forward converter topology operating at 500 Khz. No power factor
correction is provided.
Fuses (not user accessible) have the following approvals; UL recognized,
Semko approved, CB certified, BSI approved.
NFINITY
15I
NFINITY
Station (IDS)
Docking
An I
functions of a passive docking station with the networking and interface
functions of an I
replaces the Basic CPS and Docking Station combination. As a docking
station, it serves as a secure mount for Patient Monitors in Pick-and-Go
operations. When equipped with a MIB Option, it provides the functionality
of a Device CPS in combination with a Breakout Box.
The I
240Vac (auto-ranging) @ 50/60Hz, to supply 12VDC @ 10.8A to an Infinity
Docking Station, for powering Patient Monitors mounted on the docking
station. The Power Supply can also power an SC 7000, SC 9000XL. SC
9000, or SC6000 series monitor directly as a replacement for the AC Power
Adapter (PSL) in standalone installations.
Docking Station (IDS) is active device that combines the
NFINITY
NFINITY
Docking Station Power Supply operates from 100-120Vac or 200-
Network CPS. With its separate power supply, it
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 35
7k9kXLTM.c2.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 52

Service Manual SC 7000 and SC 9000XL Patient Monitors
This page intentionally blank.
36 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLTM.c2. CD_R OM .fm/0 4-99/ k aupp
Page 53

Chapter 3: Repair
1Introduction
2 Service Policy and
Replaceable Parts
2.1 Base Unit
This chapter describes how to disassemble SC 7000 and SC 9000XL
Patient Monitors, replace parts and subassemblies that Siemens has
identified as field-replaceable (see “Appendix A: Replacement Parts” ), and
reassemble the monitors. The structure of an SC7000 or an SC 9000XL
consists of a base unit with attachable modules and pods.
Warning
After replacing a part or subassembly, always functionally verify
proper operation of the monitor, before returning the monitor to
clinical service.
Qualified service personnel may replace the following specific items in the
field. Except for specified items, component-level repairs should not be
attempted and will void any warranty or exchange allowance for returned
subassemblies. A complete list of replaceable componen ts and part
numbers is given in Appendix A.
Front Bezel/Lens Subassembly
Language Label Set
LCD Backlight Lamps
Optical Encoder Subassembly
2.2 R50 Recorder
Rotary Knob
Front Bezel PC Board
Front Bezel Subassembly w/ Language Label Set
NP Pump Subass e mbly
NP Filters
Batteries (main and external)
Power Harness w/ Speaker
External Battery Compartment Door and Ejection Spring
Main Processor PCB Subassembly
Funnel
Monitor Handle
Rear Housing Side Panels w/ Label Set
Rear Housing / Connector I/O PCB
F1, F2, and F3 on Connector I/O PCB
Since an R50 Recorder operates in conjunction with the monitors,
replaceable subassemblies for the R50 are included in Appendix A.
Front bezel
Printer subassembly
A100 PC Board
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 37
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
Page 54

Service Manual SC 7000 and SC 9000XL Patient Monitors
2.3 Modules, PODs, and Peripherals
3 Safety Precautions
4 Re pl ace ab le P ar ts
and Subassemblies
That DO NOT
Require Opening the
Monito r
The following modules, PODs, and peripherals have no field-replaceable
parts or subassemblies.
• MultiMed and MultiMed 12 Pods, tcpO2/CO2 Pod, NeoMed Pod
•etCO
• CPS/IDS (except for dc power cable in IDS-PS, and MIB Options in
• Hemo4 Pod / Hemo2 Pod, HemoMed Pod
• Remote Display
• PCMCIA Card
Remove all power sources, attached modules and cables, before
attempting to replace any items or open the monitor case.
Module
2
IDS, which are field-replaceable)
&DXWLRQ
3
Open monitor only in a static-protected environment. Observe
standard precautions for protecting the equipment from static
electricity.
The following components and subassemblies can be replaced without
opening the monitor.
• rotary knob
• front bezel language and monitor model labels
• foot pads
• external battery (optional)
4.1 Replacing Rotary Knob
4.2 Replacing Front Bezel Labels
• external battery compartment door and battery ejector spring
• main battery
• power cable and speaker subassembly
• NP filters
• NP pump subassembly
• monitor handle
• rear housing side panels
The rotary knob (0 in Figure 3-10 on page 51) is press fitted onto the metal
shaft of the optical encoder subassembly. It must be removed very carefully
if it is to be reins t alle d.
To remove the knob, grip it
pull it straight out and off of the metal shaft. Avoid turning the knob.
Note: Placing a piece of cloth around the knob should prevent
scratching by the vise-grips, and allow the knob to be reused.
To install or reinstall a knob, align and firmly press knob onto shaft.
The Language Label kit ships with a set of language labels and SC 7000
and SC 9000XL model labels (see
SIEMENS metal logo label ships with the bezel (see
firmly with vise-grips or a similar tool, and
very
in Figure 3-10 on page 51). A
in Figure 3-10).
38 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
Page 55

SC 7000 and SC 9000XL Patient Monitors Service Manual
4.2.1 Removing Existing Label To remove existing label, carefully peel up one corner of label and pull it
towards opposite corner.
Caution
Use extreme care to not damage underlying membrane keypad
when replacing Language Label. If membrane keypad is damaged
the Front Bezel/Lens Subassembly must be replaced.
4.2.2 Installing Language Label 1) Peel protective covering from section of new label under function keys.
2) Position label on membrane keypad so that it fits squarely in label
depression allowance on front bezel, and using a sweeping or rolling
motion to prevent air bubbles from becoming trapped under label,
press on label to secure it to membrane keypad.
3) Remove protective co vering from remai nder of language label , and
with a similar motion affix label along bottom of bezel.
4.2.3 Installing SIEMENS Metal Logo Label
4.2.4 Installing Monitor Model Label
4.3 Replacing Foot Pads
Use this procedure if SIEMENS metal logo label not already installed on
front bezel.
1) Peel protective covering from new label.
2) Position in left rectangular depression in area near top left corner of
front bezel.
3) Press firmly, using a sweeping m otion to prevent air bubbles from
becoming trapped under label.
1) Peel protective covering from appropriate new monitor model label.
Discard other new label.
2) Position NEW label in rectangular depression to right of SIEMENS
metal logo label in area near top left corner of front bezel.
3) Press firmly, using a sweeping m otion to prevent air bubbles from
becoming trapped under label.
Two feet are on the bottom of the front bezel subassembly (see 3 in Figure
3-10 on page 51, and four are on the bottom of the rear housing (see
Figure 3-2 on page 40). Pads are secured in foot wells by adhesive.
1) Remove all remnants of existing pad and adhesive fro m foot well.
2) Remove protecti v e co vering from adhesive surface of replacement pad.
3) Position replacement pad in foot well, and press firmly on pad to
secure it in well.
7
in
4.4 Removing / Installing External Battery and Support Components
4.4.1 External Battery (optional) The external battery compartment door is hinged to the compartment
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 39
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
The external battery (7 in Figure 3-1) and main battery (0 in Figures 3-1
and 3-2) are contained in compartments on the rear of the monitor. It is
necessary to remove the back cover
housing on the right-hand end (facing the back of the monitor). The door
8
in Figure 3-2) has been designed to lift the battery as an assist to the
(
ejection spring (
when the battery is being removed. It also secures the battery in the
compartment and assures good electrical connection to the battery
connector when closed.
@
in Figure 3-2) at the opposite end of the compartment
6
only to replace the main battery.
Page 56

Service Manual SC 7000 and SC 9000XL Patient Monitors
6
2
X5
X3
X8
X7
4
7
a
5
a
8
Figure 3-1 SC 7000 and SC 9000XL Rear View w/ Cover Removed
9
9
4
5
10
1
9
3
10
2
6
2
1
1
3
7
4 pl
10
9
8
6
Figure 3-2 Rear Housing Components/Subassemblies (Left Side-Panel Removed) Note: Numbers in white
circles call out replaceable parts. Numbers in black circles are for text references.
40 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
Page 57

SC 7000 and SC 9000XL Patient Monitors Service Manual
Removing Battery To remove installed external battery, open hinged door to lift battery. An
ejector spring pushes the battery partially out of compartment, releasing it
from connector. Pull battery out to remove it from compartment.
Installing Battery To install external battery, open hinged door and insert battery (contact end
first, oriented with contacts toward rear of monitor) into compartment. Close
hinged door against battery to compress ejector spring and firmly seat
battery into battery connector. Assure that door latches securely.
4.4.2 External Battery
Compartment Door
Removing External
Compartment Door
Installing External
Compartment Door
4.4. 3 Replaci ng Ext ernal Batt ery
Ejection Spring
4.5 Removing / Installing Main Batte ry
The external battery compartment door is hinged to the compartment
housing on the right-hand end (facing the back of the monitor), and is held
in operating position by the rear cover. Do the following to replace the door:
1) Remove external battery (if installed).
2) Remov e and sa ve three Phillips-head screws (
securing back cover (
3) Slide battery compartment door (
4) Slide replacement battery compartment door into position in rear
housing, and reinstall rear cover.
5) Reinstall external battery contact end first, oriented with contacts
toward rear of monitor, (if previously installed), and close external
battery compartment door.
1) Remove external battery (if installed).
2) Remov e and sa ve three Phillips-head screws (
securing back cover (
3) Slide external battery ejection spring (
channel at the head of the external battery compartment.
4) Slide replacemen t ejection spring into channel at head of external
battery compartment, and reinstall back cover and external battery.
The main battery (0 in Figures 3-1 and 3-2) is in a compartment below the
external battery compartment behind the rear cover (
the following procedure to remove the main battery.
6
in Figure 3-2) to rear housing.
7
in Figure 3-2) out of rear housing.
6
in Figure 3-2) to rear housing.
@
=
in Figure 3-2)
=
in Figure 3-2)
in Figure 3-2) out of its
6
in Figure 3-2). Use
Caution
After removing the rear access panel,
securing the Main Battery to the rear housing. They have been
designed to be releaseable, and the monitor must be opened to
replace them. See Figure 3-3.
5HPRYLQJ %DWWHU\
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 41
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
1) Remove and save three Phillips-head screws (
page 40) securing rear cover
2) Using long nose pliers or similar tool, unplug two battery connectors
from main battery terminals.
(if installed). Note polarity of battery cable wires!
6
Be careful to NOT damage in-line fuse
do NO T cut the ty-wr a ps
=
in Figure 3-2 on
to rear housing, and remove panel.
Page 58

Service Manual SC 7000 and SC 9000XL Patient Monitors
Figure 3-3 Battery Cable Ties
3) Depress release tab on each ty-wrap lock (see Figure 3-3) and pull tywrap tongues out of locks to free battery.
4) Note routing of speaker cable, and slide battery out of compartment.
Installing Main Battery Reverse steps of removal procedure to install main battery. Route speaker
cable as noted in step 4 above before resecuring ty-wrap on main battery.
4.6 Replacing Power Cable and Speaker Subassembly
1) Remove external battery (if installed).
=
2) Remov e and sa ve three Phillips-head screws (
securing back cover
3) Using long nose pliers, unplug battery connectors from main battery.
Be careful to NOT damage in-line fuse (if installed). Note polarity
of battery cable wires! Red goes to +; Black goes to -.
4) Slide external battery connect or out of channel in battery
compartment.
Note: Do not remove ferrite filter (
subassembly. Note positioning of filter in connector compartment, and
locate in same position when installing new cable subassembly.
5) Using long-nose pliers, unplug speaker connector from X7 (see Figure 3-
1 on page 40) and power cable connector (
3-2) from Connector I/O PCB in connector ca vi ty (
remove power cable subassembly.
6) Depress release tab on each ty-wrap lock (see Figure 3-3) and pull tywrap tongues out of locks to permit removal of speaker cable. Note
routing of speaker cable for use in reassembly.
7) Slide speaker out of slots in rear housing, and remove power cable
and speaker subassembly.
8) Reverse procedure of steps 1 through 5 to install replacement power
cable and speaker subassembly.
6
on back of monitor, and remove cover.
H
in Figure 3-2) from cable
@
in Figure 3-2)
inFigur e 3-1 and in Figure
6
in Figure 3-1), and
Caution
Sandwich wires of power cable and speaker subassembly
between left side of housing and flat plastic cable guide (
Figure 3-1 on page 40) to prevent possible dama ge to harness whe n
installing rear housing screws.
42 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
in
Page 59

SC 7000 and SC 9000XL Patient Monitors Service Manual
4.7 NP Filters and Pump Subassembly
4.7.1 Replacing Manifold and Air
Intake Filters
1 2 3
7
10
Figure 3-4 NP Subassembly in Rear Housing
The NP subassembly, 4 in Figures 3-1 and 3-2, is housed in a
compartment above the external battery on the back of the monitor. Use the
following procedure to replace filters and/or the NP subassembly.
Refer to Figure 3-4. The manifold filter
mounted directly on the NP pump subassembly.
1) Remove and save three Phillips-head screws, = in Figure 3-2 on
page 40, securing back cover
cover.
8
0
6
on back of monitor, and remove
9
5
4
and air intake filter 6 are
6
2) Remove cap from holder of filter to be replaced.
Note: If replacing air intake filter, slide holder out of retainer plate
before removing cap.
3) Using long-nosed pliers or tweezers, remove and discard filter,
4) Insert replacement filter into holder. Observe following precaution.
Caution
The filter has a hole in one end. Insert the filter hole-end first, so
that the hole is at the internal end of the holder and the end
without the hole is at the cap end of the holder. This provides for
proper filtering with minimal restriction of air flow.
5) Reinstall cap on filter holder.
Note: If replacing air intake filter, slide holder back into slot in retainer
plate ➅ after reinstalling cap.
6) Reposition back cover on monitor, and reinstall three securing screws
removed in step 1.
4.7.2 Removing NP Subassembly 1) Remove and save three Phillips-head screws, = in Figure 3-2 on page
40, securi n g back co ver 6 on back of monitor, and remove cover.
2) Refer to Figure 3-4, and us ing long-nosed pliers, tweezers, or similar
tool, carefully pull transducer tubing @ off of mounting port on filter
housing 0, and back through slot in retainer plate 4. Observe the
following precaution.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 43
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
Page 60

Service Manual SC 7000 and SC 9000XL Patient Monitors
Caution
Be careful that the pliers or tweezers do NOT damage the tubing.
Also, do NOT put any tension on the other end of the tubing,
routed through the access hole in the back of the rear housing.
Routing of tubing inside the rear housing is critical.
3) Carefully pull cuff connector tubing (
connector on rear housing, observing precaution above.
4) Refer to Figure 3-1 on page 40. Using long-nosed pliers, unplug NP
subassembly cable connectors from X3 and X5 in connector cavity
Note: It may be necessary to slide ferrite filter on power cable
subassembly (H in Figure 3-2 on page 40) along the cable to permit
access to connectors in the connector cavity. Be sure to slide the filter
back into proper position after installing NP subassembly.
5) Note dress of cables through fer rite bead (
on NP subass em bly cables. Note also, that cable from NP coil sensor
5
(
in Figure 3-4 ) l oops through bead twice. Rem ov e and save bead.
6) Carefully cut ty-wrap bundling cuff connector ring filter cable (at
Figure 3-4) to NP subassembly cables.
7) Slide air intake filter holder
3-4) and move cuff connector filter cable out of slot.
8) Grasp pump mounting plate (
Figure 3-4), and pull NP subassembly straight out of NP compartment.
4.7.3 Installing NP Subassembl y 1) Slide NP subassem bly into compartme nt.
2) Perform steps 1 - 8 of Section 4.7.2 above in reverse order (including
re-securing of ferrite bead) to complete installation of replacement NP
subassembly. When installing new ty-wrap, be sure to secure near
7
plate (
in Figure 3-4) to keep cables in slot in plastic wall.
6
7
3
in Figure 3-4) off of cuff
out of slot in retainer plate (
in Figure 3-4) and retainer plate (4 in
8
in Figure 3-4 on p age 43)
4
in Figure
6
in
.
3) Perform an NBP characterization. Go on to section 4.7.4
4.7.4 NBP Characterization Preparation
)L[HG 9ROXPH /HDN DJH 7HVW
6\VWHP /HDNDJH 7HVW
44 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
Set up NBP Calibration assembly (kit Art. No. 28 77 855 EE54U) as
illustated in Figure 4-1 on page 65, and assure that fixed volume and
system pneumatic leakage are within specifications.
Note: For characterization, the Siemens-recommended Pressure
Transducer Tester or manometer can be used. Accuracy of ±0.3
mmHg is required for only NBP calibration procedure.
1) Pinch off hose attached to monitor (e.g., with a hemostat or clamp),
and using inflation bulb, increase pressure to 250 ±5 mmHg. Pinch off
hose at inflation bulb and let pressure stabilize for 1 minute.
2) Observe pressure drop for an additional 5 minutes. Drop should be <2
mmHg in 5 minutes. If not, tighten all connections and fittings, and
retest equipment for leakage. When leakage test OK, go on to step 3.
3) Remove hose clamps, and if necessary, use inflation bulb to assure
that pressure on manometer is 250mmHg.
4) Again pinch off hose at inflation bulb and observe pressure drop for an
additional minute. Pressure drop should be <4mmhg. If not, service
monitor’s internal pneumatics system and retest system for leakage.
When leakage test OK, remove clamp at inflation bulb and continue.
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
Page 61

SC 7000 and SC 9000XL Patient Monitors Service Manual
5) With monitor in Adult mode, power monitor ON and set following in
NBP parameter field menu:
• Inter val Time - OFF
• Continuous Mode - OFF
• Calibrate Mode - ON. (Obser ve “NBP Cal. = 0 mmHg” appears.)
6) Perform a calibration check. Refer to Section 10.2 on page 65 in
Chapter 4.
4.7.5 NBP Characterization Note: Always perform NBP calibration check before attempting characterization. Perform NBP calibration if NBP fails calibration check.
1) Disconnect calibration assembl y hose from caniste r, and using adult
hose, connect .5l pressure canister directly to monitor cuff connector.
2) Press Main Menu key, and select Monitor Setup → Biome d → Service.
3) Enter service password (4712) and select Accept.
4) Select Characterization → NBP Char.
5) Verify that “NBP Characterizing” displays in message field. When
message blanks, process has completed.
4.8 Replacing Monitor Handle
5 Opening Monitor
5.1 Removing/Installi ng Side-Panels
Note: (If characterization fails, refer to Section 12.2, “NBP
Troubleshooting” in Chapter 5.)
6) Press Main Screen key.
7) Functionally verify proper operation of monitor’s NBP function.
1) Remove left and right side panels from monitor. See Section 5.1.
A
2) Remove and save securing screws (
extract handle through top of monitor.
3) Install new handle through top of monitor, reinstall securing screws,
and reinstall left and right side panels.
Before attempting to open the monitor, always do the following:
• Remove all attached modules and unplug all cables from the monitor.
• Disconnect all external power sources, remove external battery (if
installed), and remove back cover and unplug cable from main battery.
• Assure that both you and the work area are properly protected against
static-electricity discharge.
The first step in opening the monitor is to remove the left and right side
panels, which are each secured to the monitor housing with several locking
tabs and two pressure-sensitive latches. Remove the panels as follows:
Note: Before the right-hand panel can be removed, it is necessary to
remove the cover from the PCMCIA card ejector shaft.
in Figure 3-2 on page 40), and
5.1.1 Removing Ejection Shaft Cover
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 45
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
1) Insert PCMCIA card into memory card slot on right-hand side of
monitor to force ejector button out.
2) Remove and save ejector shaft cover. To remove cover, grasp front
and back sides of cover between your thumb and forefinger, squeeze
cover slightly, and
shown at top left of next page.
carefully
rock cover off of shaft in direction of arrow
Page 62

Service Manual SC 7000 and SC 9000XL Patient Monitors
Caution
5.1.2 Installing Ejection Shaft Cover
The cover has nubs (see
in the top and bottom sides of the shaft. Grasping the cover by
1
the top and bottom sides tends to increase the effectiveness of
the nubs. The increased force required to remove it can pull the
shaft completely out of the ejector mechanism, requiring depot
repair of the monitor.
3) Push ejector shaft back in, and remove PCM CIA card.
Use the procedure of Section 5.1.1, reversing the action in step 2, to install
PCMCIA card ejector shaft cover.
Note: The button cover is not centered on the shaft, and can be
installed in only one orientation.
0
in illustration at left) that grip grooves
/HIW 5LJKW
Figure 3-5Removing Left and Right Side Panels (SC 7000 left side panel
shown in illus t r ati o n)
5.1.3 Removing Right Side Panel 1) Place monitor left side down on a smooth clean surface.
2) With PCMCIA card ejector shaft cover removed, press firmly on dots
below each side of sync output connector (see narrow arrows in Figure
3-5), to release latch.
3) While pressing on dots, slide panel downward (see broad arrows in
Figure 3-5) to release locking tabs, and then lift cover off of monitor.
5.1.4 Installing Right Side Panel 1) With monitor left side down on a smooth clean surface, pos ition s ide panel locking tabs into slots in monitor housing, and press inwards and upwards to lock side panel to monitor.
2) Reinstall PCMCIA card ejector shaft. See Section 5.1.2.
5.1.5 Removing Left Side Panel 1) Place monitor right side down on a smooth clean surface.
46 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
Page 63

SC 7000 and SC 9000XL Patient Monitors Service Manual
2) Press firmly on dots just below each side of IBP connector port shown
in Figure 3-5 (SC 7000 side panel used in illustration), to release latch.
3) While pressing on dots, slide panel downward to release locking tabs,
and then lift cover off of monitor.
5.1.6 Installing Left Side Panel With monitor right side down on a smooth clean surface, position side panel locking tabs into slots in monitor housing, and press inwards and upwards to lock side panel to monitor.
5.2 Separating F ront Bezel
Subassembly and
Rear Housing
Subassembly
Figure 3-6 Bottom Release Tabs for Front Bezel Subassembly
2
1
Figure 3-7 Security Clip
After left and right side panels have been removed, opening the monitor is
the process of separating the front bezel and rear housing subassemblies,
which are secured to each other by four locking tabs -- two on the top and
two on the bottom of the Front Bezel.
1) Turn the monitor backside down, with bottom of monitor facing you.
2) Remove tape and locking clips, if installed.
0
and Tape
@
Note: On some monitors, peel-and-stick tape (
covers locking clips (
release latches (one for each latch).
3) Press in firmly on thumb depressions on bottom of monitor to release
latches (see Figure 3-6), and slightly separate bottom of front bezel
subassembly from rear housing.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 47
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
0
in Figure 3-7) that prevent release of bottom
@
in Figure 3-7)
Page 64

Service Manual SC 7000 and SC 9000XL Patient Monitors
Figure 3-8 Top Release Tabs for Front Bezel Subassembly
4) Return monitor to its proper upright position, with back of monitor
facing you.
5) Insert tip of small screwdriver into each of two release slots on top of
monitor (see Figure 3-8), as you apply a slight tension between front
bezel subassembly and rear housing, to slightly separate top of front
bezel subassembly from rear housing.
6 Replacing
Subassemblies in
Rear Housing
6.1 Removing/Installi ng
Funnel
5HPRYLQJ )XQQHO
,QVWDOOLQJ )XQQHO
Note: It is helpful to lift the handle as shown in Figure 3-8 to access
the release slots.
6) Turn monitor around so that display screen is facing you.
7) Carefully pull Front Bezel Subassembly straight out from rear housing
to unplug interfacing connector on back right-hand side of Front Bezel
PCB from corresponding connector on Main Processing Board, and
separate the two subassemblies.
The only replaceable components contained in the rear housing, that
require the monitor to be opened, are the Main Processor PCB
Subassembly, the Funnel, and the Rear Housing Subassemb ly. Other
replaceable components and subassem bl ies, that do not require that the
monitor be opened, are discussed in Section 4 above.
Tabs on the top edge of the funnel located on the top of the heat sink on the
Main Processor PCB Subassembly lock the funnel into the rear housing.
1) After opening monitor, set rear housing subassembly bottomside down
so that Main Processor PCB Subassembly is facing you.
2) Using small common-blade screwdriver, depress locking tabs near left
and right sides of funnel through slots on top edge of rear housing (
in Figure 3-9 on page 50) to release funnel, and slide funnel out of rear
housing.
Reverse steps 1 and 2 to install funnel.
H
6.2 Main Processo r PCB
Subassembly
48 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
The Main Processor PCB Subassembly is secured in the rear housing as
follows:
• Tabs on the top edge of the funnel (
into slots in the top of the rear housing (
bottom edge of the funnel restrains the top edge of the heat sink and
holds the subassembly securely in the housing.
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
@
in Figure 3-9 on page 50) lock
H
in Figure 3- 9). The back
Page 65

SC 7000 and SC 9000XL Patient Monitors Service Manual
Caution
The funnel must be removed before attempting to remove the
Main Processor PCB Subassembly.
• The Front Bezel Subassembly, when installed, further locks the Main
Processor PCB Subassembly in place and comp letes mechani ca l
integration of the monitor’s several internal subassemblies.
6.2.1 Removing Main Processor PCB Subassembly
6.2.2 Installing Main Processor PCB Subassembly
1) After opening monitor, see Section 5, set rear housing subassembly
bottomside down on a clean flat surface.
2) Using long nose pliers, carefully pull NBP tubing off of transducer port
0
(
in Figure 3-9 on page 50) and out of its routing channel. Note
routing of NBP tubing. Use exactly same routing when
reassembling monito r. Save grommet for use in reassembly. Tuck
tubing temporarily under monitor handle on top of housing (to keep it
out of the w ay).
3) Using small common-blade screwdriver, depress locking tabs near left
and right sides of funnel through slots on top edge of rear housing (
in Figure 3-9) to release funnel, and slide funnel out of rear housing.
4) Reaching through rectangular slot on right hand side of rear housing,
apply pressure behind the 14-pin mini-champ connector housings on
main PCB to unplug Main Processor PCB Subassem bly from X4 on
the Connector I/O PC Board.
5) Grasp handle on Main Processor PCB support (
pull sub-assembly straight out from rear housing to slide connectors
on left side of main PCB out of channels in rear housing and remove
subassembly.
6) Place Main Processor PCB Subassembly in static-protected
environment.
Reverse procedure of Section 6.2.1 to install M ain P r oce ss or P C B
Subassembly.
3
in Figure 3-9), and
H
Note: Mati ng Ma in Processor PC B Subassembly into Rear Housi ng
Subassembly requires that Pod Com connectors (
align properly in chann el s (
$OVR EH YHU\ FDUHIXO WR OLPLW DQ\ H[FHVV SQHXPDWLF WXELQJ LQ WKH DUHD
EHWZHHQ WKH JURPPHW DQG WKH 1%3 SUHVVXUH WUDQVGXFHU WR PLQLPL]H
WKH SRVVLELOLW\ WKDW WKH WXELQJ FDQ EHFRPH SLQFKHG EHWZHHQ WKH KHDW
VLQN DQG IURQW SDQHO VXEDVVHPEO\ LQ WKH UHDVVHPEO\ SURFHVV
6.3 Replacing Rear Housing
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 49
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
Replacing the rear housing is a matter of removing subassemblies and
components (except the Connector I/O PCB) from the old rear housing, and
installing them in the new Rear Housing Subassembly in accordance with
procedures given in appropriate sections above. Perform the procedures in
the order given in the following steps:
N. B. The monitor’s serial number is electronically embedded in a chip
on the Connector I/O PCB and also printed on a label on back of the
rear housing. The replacement Rear Housing Subassembly must be
specially prepared at the factory, with an identical serial number,
<
in Figure 3-9) in lef t side of rear housing.
5
in Figure 3-9)
Page 66

Service Manual SC 7000 and SC 9000XL Patient Monitors
2
4
2
5
5
3
1
Rear Housing Subassembly
Main Processor PCB Subasse mbly
Front Bezel Subassembly
Figure 3-9 Main Subassemblies of SC 7000 and SC 9000XL Patient Monitors (left side panel not shown). Note:
Numbers in black circles relate to corresponding numbers in white circles. See text.
as a specific replacement for a defective housing or Connector I/O
PCB. The required serial number is embedded in the new Connector
I/O PCB installed in the replacement subassembly, and the proper
label is placed on the back of the housing. It is the responsibility of
the individual replacing a defective Rear Housing Subassembly to
ensure destruction and proper disposal of the subassembly replaced.
1) Open monitor. Transfer Main Pr ocessor PCB Subass em bl y and Funnel.
2) Transfer NP Subassem bly.
Note: Be sure to plug the NBP cuff connector sensor ring on new
housing into X8 on Connector I/O PCB. See Figure 3-1 on page 40.
3) Close monitor and transfer remaining components and subassemblies
into the compartments on back of monitor under rear cover.
4) Functionally verify proper operation of reassembled monitor.
50 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
Page 67

SC 7000 and SC 9000XL Patient Monitors Service Manual
10
11
8
8
(@ in Figure 3-11)
4
6
1
2
3
9
10
7
4
(3 in Figure 3-11)
Figure 3-10 Front Bezel Subassembly Components. Note: Numbers in white circles call out replaceable parts.
Numbers in black circles are referenced in text.
5
5
(0 in Figure 3-11)
1
4
5
2
3
Figure 3-11 Front Bezel Subassembly - Interior View
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 51
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
Page 68

Service Manual SC 7000 and SC 9000XL Patient Monitors
7 Replacing
Subassemblies in
Front B ezel
Subassembly
Replaceable subassemblies in the Front Bezel Subassembly are as
follows:
• Front Bezel PCB Subassembly (
• Optical Encoder Subassembly (
page 51, also see Figure 3-12 on page 52)
• Front Bezel/Lens Subassembly (
includes bezel w/ lens, display subassembly mounting frame, metal
logo, and feet)
• Backlight Lamps (see Figure 3-13 on page 54)
Note: The Front Bezel Subassembly, which includes all components
shown in Figure 3-9 on page 50, is also available for replacement as
a complete subassembly, (except for the language and model labels
which must be ordered as a separate kit).
4
in Figure 3-10 on page 51)
0, @, 3
in Figure 3-10 on pag e 51,
, and 5 in Figure 3-10 on
7.1 Front Bezel PC Board
7.1.1 Removing Front Bezel PCB It is necessary to remove the retainer plate, optical encoder subassembly, and display screen subassembly, to access and remove the Front Bezel PCB.
1) With front bezel subassembly laying face down on a smooth clean
surface, remove and save six se curi ng screws (see
on page 51) from retainer plate.
2) Move retainer plate slightly left to slide tabs on right hand side of plate
9
(
in Figure 3-10 and 5 in Figure 3-11 on page 51) out of tab slots
in side of front bezel frame.
0
in Figure 3-11
3) Lift bottom edge of retainer plate and slide plate out of tab slots (
Figure 3-11 on page 51) in top of front bezel frame.
4) Set retainer plate aside for use in reassembly.
Figure 3-12Optical Encoder Subassem bly. See Note in Figure 3-10
caption.
5) Remove rotary knob (
Note: Rotary knob is press fitted onto metal shaft of optical encoder
subassembly. It must be removed very carefully if it is to be
reinstalled. To remov e knob, grip it
similar tool, and pull it straight out and off of metal shaft. Avoid turning
knob. Placing a piece of cloth around knob should prevent scratching
by vise-grips, and allow knob to be reused.
0
in Figure 3-10 on page 51 and in Figure 3-12.
firmly with vise-grips or
very
4
in
52 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
Page 69

SC 7000 and SC 9000XL Patient Monitors Service Manual
6) Unplug optical encoder ribbon cable connector (< in Figure 3-10 on
page 51 and Figure 3-12 on page 52) from Front Bezel PCB.
7) Refer to Figure 3-10 or Figure 3 -12. Unscrew nut
encoder shaft in position in front bezel, and remove optical encoder
subassembly
positioning washer combination
8) Refer to Figure 3-10. Unplug membrane switch ribbon cable connector
@
and display backlight connectors ? from Front Bezel PCB, and
display screenflex cable connector
subassembly PC board.
9) Slide small screwdriver under tab near bottom on right hand side of
display subassembly, and carefully lift display subassembly (
Figure 3-10) out of front bezel frame. Set subassembly aside on a
clean flat surface for use in reassembly.
Note: Be very careful that no dust or other foreign matter gets on the
front bezel lens or on the display screen surface.
10) Rem ov e and save two screws (
securing Front Bezel PC Board interface connector to mounting tabs
on front bezel frame.
11) Rem ov e and save two remaining screws (
Figure 3-10) securing Front Bezel PC Board to front bezel frame.
12) Lift bott om right hand side of Front Bezel PC Board off of front bezel
frame, and slide board out from under interface connector mounting
tabs to remove board.
5
through back of panel. Save nut, and lock washer /
for use in reassembly.
9
;
from display screen
@
in Figure 3-11 on page 51)
3
H
securing optical
4
in
in Figure 3-11 and 8 in
7.1.2 I ns talling Front B e z el PC Board
1) With optical encoder and display screen subassemblies removed, and
front bezel subassembly laying face down on a smooth clean surface,
bottom facing you, slide Front Bezel PC Board into position on
mounting posts on front bezel frame, with interface connector housing
under front bezel frame connector mounting tabs.
Caution
The flex cable and connector on the right-hand side of the Front
Bezel PC Board can be easily damaged. Be particularly careful
when positioning the board in the front bezel subassembly or
reinstalling the display screen subassembly in step 5 below.
2) Install screws removed in step 10 above into interface connector
housing but do not tighten until step 4 below.
3) Install screws removed in step 11 above, and tighten to secure Front
Bezel PC Board to front bezel frame.
4) Tighten screws installed in step 2 to secure interface connector
housing to front bezel frame.
5) Locate display subassembly in front bezel frame and press to seat
subassembly into position.
Note: Be very careful that no dust, finger prints, or other foreign
matter is on the front bezel lens or on the display screen surface.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 53
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
Page 70

Service Manual SC 7000 and SC 9000XL Patient Monitors
6) Refer to Figure 3-10 on page 51. Plug display screen flex cable
connector
backlight connectors
@
into Front Bezel PC Board.
7) Dress display backlight cables into space between display
subassembly and front bezel PC board.
8) Slide optical encode r subassem bly shaft throug h hole in front bezel,
positioned such that keyway on shaft is toward top of panel.
9) Slide positioning washer removed in step 7 of Section 7.1.1 above
onto subassembly shaft so tab on hole in washer slides into keyway on
subassembly shaft and locking tab on washer is into hole in front bezel
above shaft.
Note: This assures that optical encoder subassembly is positioned so
that its ribbon cable connector plugs properly into the front bezel PC
board and the subassembly doesn’t rotate in subsequent use.
Note: Slide lockwasher and nut removed in step 7 of Sect ion 7.1.1
above onto subassembly shaft, and tighten to secure subassembly in
front bezel.
10) Plug optical encoder ribbon cable connector int o F ront Bezel PC Boa rd.
;
into display screen subassembly PC board, and display
?
and membrane switch ribbon cable connector
7.2 Optical Encoder Subassembly
11) Slide retainer plate tabs into tab slots (4 in Figure 3-11 on page 51) in
top of front bezel frame.
12) P ress down on plate and slide plate right to insert tabs on right hand
side of plate into tab slots on side of front bezel frame.
13) S ecure to frame using sc rews remov ed in step 1 of Section 7.1.1.
14) Reassemble monitor. Refer to Section Section 8.
Refer to steps step 1 through step 7 of Section 7.1.1 to remove Optical
Encoder Subassembly, and to steps step 8 through step 14 of Section 7.1.2
to install Optical Encoder Subassembly. Install new rotary knob. See
Section 4.1.
2
1
2
Figure 3-13 Display Screen Subassembly
54 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
Page 71

SC 7000 and SC 9000XL Patient Monitors Service Manual
7.3 Backlight Lamps
The backlight fluorescent lamps are located inside the display screen
subassembly (
1) With front bezel subassembl y separated from rear housing and laying
face down on a smooth clean surface, remove and save six screws
0
(
in Figure 3-11 on page 51) from retainer plate (6 in Figure 3-10).
2) Move retainer plate slightly left to slide tabs on right hand side of plate
9
(
in Figure 3-10 and 5 in Figure 3-11 on page 51) out of tab slots in
side of front bezel frame.
3) Lift bottom edge of retainer plate and slide plate out of tab slots (
Figure 3-11) in top of front bezel frame, and set aside for reassembly.
4) Unplug display screen flex cable connector (; in Figure 3-10) from
display screen subassembly PC board. Note pad that keeps connector
in place.
5) Unplug backlight connectors (
bezel PC board, and lift subassembly out of frame.
6) Using very small screwdriver, depress black nub on latch of each
backlight lamp holder (located at
and draw backlight lamps out of display screen subassembly in
direction of heavy arrows in Figure 3-13.
Note: As you remove backlight lamps, note that each has a small
on the side that faces up. Install the replacement lamps in the same
orientation as the lamps being removed. Always replace both lamps.
7
in Figure 3-10 on page 51). Replace lamps as follows:
0
in Figure 3-13 on page 54) from front
@
in Figure 3-13) to release latch,
4
in
7.4 Front Bezel/Lens Subassembly
7.5 Front Bezel Subassembly
8 Closing Monitor
7) Perform steps 1 through 6 in reverse order to install backlight lamps.
A replacement Front Bezel/Lens Subassembly ships with an installed lens,
mounting frame, Siemens Metal Logo, and feet. The Language Label Set
which includes SC 7000 and SC 9000XL Monitor Model Labels (see in
Figure 3-10 on page 51) must be ordered separately,
1) Install “SIEMENS” metal logo (if not already installed) and Monitor
Model labels on front bezel, using original bezel as a model.
2) Remove LCD display subassembly , optical encoder, Front Bezel PC
Board, and retainer plate from original Front Bezel and install in
replacement bezel. Refer to step 1 through step 5 of Section 7.3, and
also Sections 7.2 and 7.1.
A replacement Front Bezel Subassembly sh i ps with LCD display
subassembly, optical encoder, Front Bezel PC Board, and retainer plate
installed. Only the Language and Monitor Model labels (ordered separately
from replacement front bezel) need to be installed on the bezel before
closing the monitor. Refer to section S ect ion 4.2 to install labels, and then
go on to Section 8 to close monitor.
1) With open side of rear housing subassembly facing you, position front
bezel subassembly such that positioning guides on sides of
subassembly are partially inserted into guide-channels along sides of
rear housing subassembly.
2) Turn partially assembled monitor backside down.
3) Assuring that interfacing connectors are properly aligned, carefully
press two subassemblies together until four locking tabs on rear
housing (two on top and two on bottom) seat properly in front bezel
and lock the two subassemblies together.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 55
7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp NOT A CONTROLLED DOCUMENT
Page 72

Service Manual SC 7000 and SC 9000XL Patient Monitors
4) Turn monitor bottoms ide up. See Figure 3-14.
0
5) Insert small screwdriver or similar tool (
15) into slot in tab (
6) Apply slight pressure in direction illustrated by heavy arrow in Figure 315 to assure tab of rear housing is securely engaged in front bezel.
2
1
Figure 3-14 SC 7000 / SC 9000XL Patient Monitor Bottom View
7) Keeping pressure on lever (
security clip (
and end of locking tabs in rectangular cutouts in bezel.
@
in Figure 3-14) to use as a lever.
0
in Figure 3-15) , insert offset tongues of
@
in Figure 3-15) vertically into space between bezel
in Figure 3-14 and Figure 3-
8) Rotate clip (hinge-like) so that offset tongues angle up under locking
tabs (to prevent tabs from being depressed) and surface of clip lies flat
on bezel.
9) Align peel-and-stick label (
tab slots (along line
to secure clip to bezel.
Note: Do NOT attempt to depress locking tabs for at least 24 hours.
Tape requires +24 hours to develop full adhesive strength.
1
Figure 3-15Installing Security Clip and Tape
10) Rem ov e lever, and repeat steps 3 through 7 for other set of locking
tabs on bottom of bezel.
3
in Figure 3-15) along edge of rectangular
4
in Figure 3-15), and press down firmly on tape
2
3
4
11) Reinstall left and right side panels (see Sections 5.1.4 and 5.1.6), and
ejector shaft cover (see section Section 5.1.2).
12) Reconnect battery power and reinstall rear cover.
13) Functionally verify proper operation of the monitor before returning the
monitor to clinical service. Refer to “Chapter 4: Functional Verification
and Calibration” .
56 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLED DOCUMENT 7k9kXLSM.c3.CD_ROM.fm/04-99/kaupp
Page 73

Chapter 4: Functional Verification and Calibration
1Introduction
Calibration required for proper operation of SC 7000 and SC 9000XL
Patient Monitors have been programmed into the software for the monitor.
An adjustment potentiometer, however, permits calibration of the NBP
transducer in the field, if required following a calibration check. Specific
calibration and adjustment procedures needed in routine operations of the
monitor are detailed in the User Guide for the installed software version,
and are required to be performed only when directed to do so by a message
in the message field on the monitor display.
If specific reading of a patient parameter is suspect, Siemens recommends
functional verification for that function. Siemens recommends a full
functional verification for all patient parameters, including an NBP
calibration check, a pneumatic leakage check, a Temperature calibration
check and a leakage current check be performed in accordance with local
regulations or at least annually. In addition, re-characterization should be
performed at least every two years. Refer to Section 4.7.4 in Chapter 3.
Note: Re-characterization and calibration checks for NBP and
Temperature should be performed by only qualified personnel with the
necessary equipment.
may place specific requirements on who may perfor m these
functions
This chapter describes functional verification procedures, calibration check
procedures, and NBP calibration procedures for monitors in the field. The
procedures assure proper operation of the monitor, using industry-standard
patient simulators and test equipment, to verify that the monitor properly
processes and reports patient physiological parameter signal inputs.
Record results of functional verification testing in a copy of “Appendix D:
Functional Verification Checklist”.
Regulations in some national jurisdictions
2 Recommended
Tools and Test
Equipment
Software and certain of the monitor’s hardware components are continually
checked, first during power-up and later during on-line self-tests. All
monitor functions that are tested are performing in accordance with design
specifications if no error messages exhibit.
Perform all functional verification and calibration procedures with the main
battery installed, and the monitor off-line if mounted on a docking station
and powered by a CPS or IDS. Disconnect all patient parameter signal
inputs from the monitor, and plug in signal inputs from patient simulators
and industry-standard test equipment only as instructed to do so.
assure that the monitor is off-line, unplug network cable from, IDS,
CPS, or monitor (if monitor functioning in DirectNet mode).
If the monitor fails to perform as indicated for any specific function during
functional verification procedures, troubleshoot the monitor using
procedures in “Chapter 5: Troubleshooting” of this Manual and remedy the
malfunction before attempting to complete functional verification.
Use specified recommended tools and test equipment given in Table 4-1
below, or a known equivalent, when performing functional verification tests.
Substitutions are approved only if an equivalent is listed. Use of other test
equipment and/or accessories could result in inconclusive tests or damage
to system components.
To
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 57
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 74

Service Manual SC 7000 and SC 9000XL Patient Monitors
Table 4-1Recommended Tools and Test Equipment
Tools & Test Equipment Description
ECG/Resp:
Patient ECG/Resp simulator DNI Medsim 300B or equivalent
Leads: T hree-lead grabb er set, or IEC color code 1
IEC color code 2
Five-lead grabber set IEC color code 1
IEC color code 2
SpO
2
Art. No. 33 75 230 E530U
Art. No. 33 75 248 E530U
Art. No. 33 75 255 E530U
Art. No. 33 75 263 E530U
Patient SpO2 simulat or , or Nellcor PT2500 or equivalent
Reusable SpO
sensor: Durasensor Adult Art. No. 45 34 475 EH50U
2
Non-Invasive Blood Pressure:
*NBP simulator (calibrated) or Dynatech CuffLink, or Veri-Cal
Pressure Transducer Tester, or
equivalent
*Mercury manometer with hand bulb Baumanometer, 0-300 mmHg
NBP Calibration Assembly Art. No. 28 77 855 EE54U
NBP connection hose, 3.7 m Art. No. 12 75 275 EH40U
etCO
2
5.00 ±0.03% CO2, balance N2, Calibration Gas Cylinder Art. No. 28 68 532 EE54U
Calibration Gas Regulator, with elbow fitting Art. No. 28 68 540 EE54U
Mercury barometer with mm grade
Invasive blood pressure:
IBP simulator w/ test cable DNI Medsim 300B or equivalent
Cardiac Output
SHP ACC C.O. INTERMEDIATE CABEL Art. No. 33 68 458 E530U
Temperature
Temperature simulator w/ test cable (2 cables req’d) DNI Medsim 300B or equivalent
Temperature Y Cable Art. No. 55 92 154 E530U
SHP ACC TEMP ADPT CBL 1/4” JACK (2 req’d) Art. No. 51 98 333 E530U
Leakage
Leakage Tester Bender µP-Safety Tester 601/751,
or equivalent
Output Cables:
Recorder ÷ Interface Plate or CPS/IDS Art. No. 47 21 770 E530U
IDS (or equivalent CPS), unless Monitor used only in DirectNet mode Art. No. 52 60 110 E5460
*For functional verification and calibration check. For calibration, Paroscientific Pressure Meter, Model 740-
12D, or equivalent, is recommended. An equivalent must be accurate to ±0.3 mmHg from 0 to 330 mmHg.
58 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 75

SC 7000 and SC 9000XL Patient Monitors Service Manual
3 Power Circuits and
Start-up
3.1 Power ON/OFF
3.2 Power-Up Sequence
The following procedures check the monitor’s power circuits, power-up
sequence, and power off indicator. Begin this procedure with the monitor
turned off and powered only by fully charged main battery.
Note: If the monitor is mounted on a docking station, be sure that the
locking lever is in the unlocked position.
1) Press ON/OFF switch on front panel and verify that power LED in ON/
OFF key turns on.
2) Press and hold ON/O FF key for approximately two sec onds.
3) Verify that high pitched piezo tone sounds briefly and power LED in
ON/OFF key turns off.
Press ON/OFF key and verify following sequence of events:
• Power LED in ON/OFF key turns on.
• Display illuminates briefly, monitor beeps, high-pitched piezo tone
sounds briefly, and Battery charger LED illuminates briefly.
• After a few moments, during which display is NOT illuminated,
monitor sounds a chime.
• After a few more moments, New Patient prompt displays.
• Select NO, and press rotary knob in to clear prompt.
Note: With all patient inputs removed from the monitor, only
MAIN
“adult” and “ALL Alarms OFF” appear on
• Battery charge level bar graph, date and time report in message
area at bottom of display.
screen.
3.3 Monitor Powered From External Source
4 Rotary Knob
5 LCD Display
1) Move docking station lever to locked position.
2) Verify that Battery charger LED illuminates and battery charge level
bar graph disappears.
3) Remove monitor from docking station or move docking station lever to
unlocked position if additional functional verification procedures are to
be performed using only main battery power. Otherwise, continue.
The Rotary Knob in the lower right corner of the front panel controls an
optical encoder for pointing to and selecting display fields and functions.
1) Press Menu key, and verify that selected menu item changes for each
detent as knob is rotated one complete revolution in either direction.
2) Rotate knob until ← in upper left corner of Main Menu is selected.
3) Press knob in and verify that
The display is composed of an active-matrix LCD screen with backlight.
Test the LCD display as follows:
1) With
2) Press Menu key and select Monitor Setup → Display Options.
3) Select Brightness
4) Change setting of rotary knob and observe that brightness of display
MAIN
Screen displayed, verify that ≤17 Pixels are inoperative
(“st u ck” ON ) .
screen varies accordingly. (monitor must be on battery power)
MAIN
screen displays.
5) Set brightness for AUTO.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 59
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 76

Service Manual SC 7000 and SC 9000XL Patient Monitors
6) Verify that backlite provides sufficient and uniform background
illumination for LCD, while connected to external power source (CPS,
IDS, PSL).
7) Verify intensity change with change in ambient light.
6 Fixed Keys
6.1 ON/OFF Key
6.2 Main Screen Key
8) Press Main Screen key to return to
The following tests verify that membrane switches on the front panel are
functioning properly, and that the signal from the key is processed by the
Front Panel Control PCB. Functions controlled by the fixed keys are
individually verified elsewhere in this Chapter as required.
Note: Before beginning Key tests access Main menu. Select Monitor
Setup → Monitor Options → Speaker Volumes , and assure that
Attention Tone Volume is set to other than OFF.
The ON/OFF key initiates the power-on sequence if the monitor is powered
off, and powers-off the monitor, initiating a brief power-off piezo alarm, if the
monitor is powered-on.
Note: This test can be omitted if the procedure of section 3.1 has
already been performed.
1) Press and momentaril y hold ON/OFF key.
2) Verify that powered state of monitor changes.
3) Set monitor to powered-on state, if monitor powered off.
The Main Screen key sets the display to the
1) Press Menu key to display Main menu.
2) Press Main Screen key, and verify that Main menu extinguishes, and
display returns to
MAIN
screen.
MAIN
screen.
MAIN
screen.
6.3 Alarm Silence Key
6.4 Alarm Limits Key
6.5 All Alarms Off Key
6.6 Code Key
The Alarm Silence key silences an alarm tone for one minute.
1) Assure that HR alarm is enabled, and without any input applied to
MultiMed POD, plug MultiMed or MultiMed 12 cable into monitor.
Monitor should Alarm.
2) Press Alarm Silence key and verify that alarm ceases .
3) Turn off HR alarm in Alarm Limits Table before proceeding. See
section 6.4.
The Alarm Limits fixed key calls up a setup table on which upper and lower
alarm limits for physiologic parameters can be assigned, and alarms and
alarm recordings can be enabled or disabled.
1) With
2) Verify that Alarms Setup Table displays .
The All Alarms Off key silences all alarms for a period of 2 minutes.
1) Press All Alarms Off key.
2) Verify that 2 minute countdow n field appears at top center of display.
The Code key can perform any of several functions, depending on other
parameter settings entered into the monitor. Refer to operating instructions
in the User Guide for more detailed information. The following procedure
verifies only that the monitor responds to a key press.
MAIN
screen displayed, press Alarm Limits fixed key.
60 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 77

SC 7000 and SC 9000XL Patient Monitors Service Manual
1) Press the key and verify that a change occurs in the display.
2) Double-click key to return display to former status.
6.7 Record Key
6.8 Print Screen Key
6.9 NBP Start/Stop Key
6.10 Zoom Key
The Record key starts and stops a recording of limited duration when the
monitor is mounted on an IDS (or CPS).
1) With monitor mounted on IDS (or CPS) press Record key.
2) Verify that message “Recording Not Accepted” appears in message
field at bottom right-hand side of display.
Print Screen key initiates printing a copy of the display, on network printer.
1) Press Print Screen key twice.
2) Verify that message “Printer Unavailable, Waiting” appears in
message field at bottom right-hand side of display.
The NBP Start/Stop key initiates or terminates the inflation cycle for the
non-invasive blood pressure monitor function.
1) Press Menu key. Access Monitor Setup → Monitor Options → Speaker
Volumes, and set Attention Tone Volume to 50%.
2) Press NBP Start/S to p key.
3) Verify that monitor sounds a tone. (Cuff must not be plugged into cuff
connector.)
When a patient is being monitored, the Zoom key calls up a 1-hour trend
display for a quick overview of patient status.
1) Press Zoom key, and verify that “Fast Access Menu” displays.
6.11 Help Key
6.12 Mark Key
7 ECG/RESP
Functions
7.1 ECG/RESP Test Setup
2) Press Main Screen key to return.
1) Press Help key and observe that Main Help Menu appears on display.
2) Press Main Screen key to clear display.
The Mark key inserts parameter values with time and date stamp in the
tabular trends. Verify that Mark membrane switch is functional as follows:
1) Press Menu key and select Review → Trend Table.
2) Press Mark key and observe that time stamp on HR readout changes
from white to green and Mark symbol appears above stamp.
With the cable plugged into the monitor connect either a 3-lead, 5-lead, or
6-lead ECG cable from the Patient Simulator into the MultiMed POD.
1) Select HR parameter box and press rotary knob in to bring up ECG
menu.
• Set all ECG Lead settings at default values and remaining
parameters as follows:
-- ARR Monitoring Basic
-- RESP Monitoring ON
-- Pacer Detection ON
• QRS Sync Marker ON
• Pulse Tone Source ECG
• Pulse Tone Volume 10%
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 61
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 78

Service Manual SC 7000 and SC 9000XL Patient Monitors
2) Set simulator as follows:
• ECG = Norm al S inus
• HR = 80 beats per minute (bpm)
• amplitude = 1.0 mV
• RESPIRATION = Normal Rest.
• rate = 20 breaths per minute (BPM)
• ohms = 1.0
• LEAD SE L E C T = II/RA-LL
• BASELINE IMPEDANCE = 500
7.2 Waveforms/Digital Readouts/Tones
7.3 Pacer Detection
7.4 Lead-Off Indicators
1) Verify the following:
• Wavef orm and HR correspond to data provided by simulator.
♥
• Heart symbol (
• White spike present at each QRS complex.
• RESP and HR digital readout correspond to settings of simulator.
2) Vary Tone Volum e setting and verify that pulse tone volume changes .
3) Set Tone Volume to OFF, and verify that pulse tone stops.
1) Apply paced signal from simulator.
2) Verify that small “P” accompanies heart symbol (
detected, paced beat, blue spike appears for each paced signal, and
HR digital value agrees with pacer bpm setting.
3) Generate asystole condition in simulato r, with pacer output still active.
4) Verify that ASY appears in ARR parameter box, an asystole alarm
sounds, and waveform is flatline with pacer pulses.
5) Disable pacer signal, and return simulator to setup above (section
7.1).
1) One at a time, disconnect each ECG lead from simulator.
2)• For LL and RA electrodes, verify “Lead-Off” and “ECG Leads Invalid”
messages appear in message area, pulse tone ceases, *** replaces
digital heart rate in HR field.
) blinks and pulse tone sounds for each QRS complex.
P
♥
for every
)
• For V and RL electrodes, verify “Lead-Off” message, loss of V trace.
• For LA electrode, verify “Lead-Off” message only.
3) Reconne ct all leads to simulator.
7.5 Alarm Function
62 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
This procedure also tests that the alarm function of the monitor, as
applicable to all other patient parameters, is operational in the monitor.
1) In Alarm Limits Table, set HR alarm parameters as follows:
• Upper limit = 110 bpm
• Lower limit = 40 bpm
•Alarm = ON
2) Set emulator to HR = 120 bpm.
3) Verify that monitor responds with following Serious Alarm indications:
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 79

SC 7000 and SC 9000XL Patient Monitors Service Manual
• HR in parameter field = 120
• HR parameter field blinks and color changes.
• Ser ious A lar m tone sounds.
• Message HR > 110 appears in message area at bottom of display.
4) Reset simulator to HR = 80 bpm.
5) Verify the following:
• HR parameter field returns to nor m al color
• HR returns to 80
• Message area cont inues to report most recent alarm, HR >110.
6) Press Alarm Silence fixed key.
7) Verify that “HR > 110” ceases to be reported.
7.6 Asystole
8SpO2 Functi on
8.1 SpO2 Test Setup
8.2 Waveforms/Digital Readouts/Tones
Switch power to simulator OFF. Verify that HR parameter field reports ASY,
“Asystole” appears in message area at bottom of display, and monitor
responds with Life-Threatening alarm.
Switch power to simulat or ON.
The SC 7000 and SC 9000XL monitor oxygen saturation (SpO2) and pulse
rate using the spectrophotometric method. SpO
monitor power-up and also periodically while the monitor is in operation.
The SpO2 parameter box appears when an SpO2 input is applied to the
monitor through the MultiMed POD.
1) Select SpO
• Pulse Tone Source - SpO
• Pulse Tone Volume -10%
• Wavef orm Size - 10%
• Averaging - Normal
2) Do either of the following as appropriate:
a If using a variable SpO
pulse rate to 70 bpm, and plug simulator into SpO
cable to MultiMed POD.
b If using a Nellcor PT-2500 pocket tester or equivalent, plug tester
into SpO
1) Verify the following:
• Simulated SpO
(PLS) values correspond to simulator settings.
parameter box to access menu. Set parameters as follows:
2
2
simulator, set Sp O2 level to 98% and
2
input adapter cable to MultiMed POD.
2
waveform appears, and digital SpO2 and pulse rate
2
software is checked on
2
input adapter
2
♥
•
symbol blinks in SpO2 field, and pulse tone sounds synchronous
with appearance of
8.3 Pulse Tone Generator
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 63
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
1) Select Pulse Tone Volume in SpO2 menu.
2) Vary volume setting and verify that pulse tone volume changes.
3) Set Pulse Tone Volume to OFF, and verify that tone stops. Then reset
pulse tone to ON.
NOT A CONTROLLE D DOCUMENT
♥
symbol.
Page 80

Service Manual SC 7000 and SC 9000XL Patient Monitors
4) Do either of the following as appropriate:
a If using variable simulator, change oxygen saturation value and
verify that pulse tone frequency (pitch) increases as SpO
increases, and decreases as SpO
b If using pocket tester or equivalent, replace tester with adult finger
sensor and place sensor on your finger. Your SpO2 reading should
be > reading obtained from tester, and frequency (pitch) of pulse
tone should increase.
level decreases.
2
level
2
8.4 SpO2 Limit s Alarms
9 Temperature Function
9.1 Temperature Test Setup
9.2 Digital Readout
9.3 Temperature Calibration Check
1) In Alarm Limits Table, set SpO2 upper limit to 100%, lower limit to
80%, and assure that alarm is ON.
2) Set simulator to an SpO
3) Verify that monitor responds with serious Alarm indication.
4) Reset simulator to value within alarm range. Verify that alarm ceases
Using the Temperature Y Cable input to the MultiMed Pod, set up the
patient simulator to supply a temperature input to Temp A.
Set the simulator for a standard 37°C.
1) Verify that monitor indicates temperature of 37±0.1° C.
2) Change simulator to temperature above and then below 37°C.
3) Verify that monitor readout agrees with simulator settings ±0.1°C.
4) Repeat procedure for Temp B input to Temperature Y Cable.
Use the following procedure to check temperature calibration. Record and
retain results in a copy of Table 4-2. Also record results in Appendix D.
Monitor must be returned to Siemens for repair if calibration check fails.
Table 4-2 Resistance Value vs Temperature
value outside of set limits.
2
Resistance
Setting
9045 -4.0 -4.1 to -3.9
3539 15.0 14.9 to 15.1
1355 37.0 36.9 to 37.1
843.2 49.0 48.9 to 49.1
9.3.1 Recommended Equipme nt Decade Resistor, ±0.1% accuracy (or fixed resistors with same accuracy) Siemens Temp Adapter Cable, Art. No. 51 98 333 E530U (Optional) Siemens “Y” Adapter, Art. No. 55 92 154 E530U
9.3.2 Procedure 1) Connect MultiMed cable to input of patient monitor.
2) Connect temp “Y” cable to temp input of MultiMed Pod.
3) Connect decade resistor to Temp A temperature input.
4) For each resistance value in Table 4-2, verify that monitor reports “Set
Temperature” value ±0.1°C.
5) Repeat procedure for Temp B input to Temperature Y Cable.
64 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
Set
Temperature
Reading On
Monitor
Tolerance Pass/
Fail
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 81

SC 7000 and SC 9000XL Patient Monitors Service Manual
10Non-Invasive Blood
Pressure Function
The SC 7000 and SC 9000XL measure non-invasive blood pressure (NBP)
according to the oscillometric method. Perform NBP characterization after
replacing the NBP Subassembly and also after replacing the Rear Housing
Subassembly (which includes the Connector I/O PCB). Use tools listed in
Table 4-1 on page 58 to check calibration of the pressure transducer. Note
pressure indicator required for NBP calibration.
1
2
Figure 4-1 NBP Calibration Check / Calibration Test Setup
10.1 System Setup and
Pneumatics Leakage
Test
Set up the NBP Calibration assembly (Art. No. 28 77 855 EE54U) as
illustated in Figure 4-1. Assure that pneumatic leakage is within
specifications before continuing to Section 10.2, Calibration Check.
1) Assure that patient category is set to Adult.
2) Set following in NBP parameter field menu:
• Interval Time - OFF
• Continuous Mod e - OFF
• Calibrate Mode - ON. (Observe “NBP Cal. = 0 mmHg” appears.)
3 Clamp pneumatic hose (with hemostat or clamp) between T-connector
and monitor (
pressure to 250 ±5 mmHg. Then clamp hose at inflation bulb (
Figure 4-1),and let pressure stabilize for 1 minute.
4) Observe pressure drop for an additional 5 minutes. Drop should be <2
mmHg in 5 minutes. If not, tighten all connections and fittings and
retest equipment for leakage. When leakage test OK, go on to step 5.
5) With both clamps remov ed, reinflate to 250±5 mmHg, if necessary,
and then reclamp hose at inflation bulb.
6) Observe pressure drop for 1 minute. Drop should be <4 mmHg. If not,
service monitor’s internal pneumatics system and retest system for
leakage. When leakage test OK, remove clamp at inflation bulb and go
on to Section 10.2.
0
in Figure 4-1), and using pressure bulb, increase
Do NOT run pump.
@
in
10.2 Calibration Check
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 65
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
Note: You may have only 2 min. to perform this test if the pump has
run since the monitor was powered on, before the H/W deflation error
initiates. If this happens, you will need to reset the monitor. If the
pump has not run, however, there is no time limit.
NOT A CONTROLLE D DOCUMENT
Page 82

Service Manual SC 7000 and SC 9000XL Patient Monitors
1) Return to Main menu. Using hand bulb, increase pressu re to 250 ±5
mmHg, if necessary, and allow it to stabilize fo r 1 minute.
2) Verify that pressure values displayed on monitor and pressure
indicator are within ±3 mmHg of each other.
3) Slowly release pressure in 50 mmHg increments. At pressures of 200,
150, 100, and 50 mmHg, verify that pressure values on monitor and
pressure indicator are within ±3 mmHg of each other at each level.
4) If NBP function fails calibration check, continue to Section 10.3.
Otherwise, if calibration check OK, go on to Section 10.4, Hardware
Overpressure.
10.3 NBP Calibration
Procedure
10.4 Hardware
Overpressure
Note: For NBP calibration, the Pressure Indicator must be accurate to
±0.3 mmHg from 0.0 mmHg to 330.0 mmHg, and must be calibrated.
The calibration must be traceable to National Standards.
1) Remove left side panel from monitor. Refer to Section 5.1, Removing/
Installing Side-Panels, in Chapter 3, for procedure.
2) With NBP Calibrate Mode in monitor set to ON, using inflation bulb,
increase pressure to 250 ±5 mmHg.
3) Clamp pneumatic hose (with hemostat or clamp) at inflation bulb.
4) Adjust R393 for monitor pressure indication that matches reading on
pressure indicator ±1mmHg.
Note: R393 is accessible through hole in rear housing below
MultiMed connector on left side of monitor.
5) Remove clamp and release pressure from system.
1) With monitor still in calibration mode, slowly increase pressure. while
observing pressure rise on monitor’s screen.
Note: Pressure indicator accuracy of ±0.3 mmHg is not required for
hardware overpressure and subsequent NBP tests.
2) Verify that pressure suddenly drops at 300 ±30 mmH g.
3) Release all remaining pressure before proceeding.
4) Set patient category to neonat al and repeat steps 4 through 6, using
pressure limit of 157±8 mmHg for step 5.
10.5 Pump
10.6 Interval Mode
66 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
1) Set Calibrate Mode in NBP parameter field menu to OFF.
2) Press NBP Start/S to p key.
3) Verify the following:
• Pressure increases and then decreases.
• Inflation and deflation press ures reported in message field.
• Message “NBP No Pulsation” exhibits at end of deflation phase.
• All digital readouts in NBP field are ***.
1) With NBP Calibrate Mode set to OFF, set Interval Time to 1 min.
2) Verify the following:
• A one-minute countdown bar graph appears at bottom of NBP
par amete r bo x.
• NBP pum p starts immediately when rotary switch is pressed in.
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 83

SC 7000 and SC 9000XL Patient Monitors Service Manual
• NBP sequences through an inflation/deflation cycle and produces
“NBP No Pulsation” message at bottom of display.
• NBP pum p starts again when one-minute countdown bar resets to
initiate another cycle.
3) Press NBP Start/Stop key to stop cycle, and reset Interval Time to OFF.
10.7 Safety Timer
11 etCO2 Function
1) Assure that NBP Calibrate Mode is set to OFF.
2) Press NBP Start/Stop fixed key to start pump.
3) Press same key again to stop measurement.
4) Set NBP Calibrate Mode to ON, and press MAIN SCREEN key.
5) Press CODE key to start screen stopwatch. Observe monitor screen.
6) Press CODE key again to stop watch when “NBP Cuff Deflation Error”
message displays, indicating that safety timer has activated.
7) Verify that elapsed time is as follows:
• Adult 120 ±5 seconds.
• Neonatal 90 ±5 seconds
• French Homologation 60 ±5 seconds
8) Press NBP Start/Stop fixed key.
9) Verify that tone sounds and pump fails to start.
10) P ower-cycl e monitor to clear fault condition.
The etCO2 Module enables the SC 7000 or SC 9000XLto non-invasively
monitor end-tidal CO
absorption properties of CO
The module automatically compensates for variations in ambient
barometric pressure if set to automatic mode. Before beginning this
procedure, use a mercury column barometer or equivalent other device to
determine local atmospheric pressure. Record this value.
(etCO2) using a technique that relies on the selective
2
to specific frequencies of infrared radiation.
2
1) Plug accessory assembly into module.
Note: Observe that the parameter box appears on the monitor display
screen, and that “etCO2 Sensor Warming Up” followed by “etCO2
Place Sensor on Zero Cell” appears in the message field.
2) While sensor is warming up, select etCO2 parameter box.
3) Assure that Atmospheric Pressure is set to “Manual”, and is set to
value indicated by mercury column barometer.
4) Place sensor on Zero Cell.
5) Note that “etCO2 Calibrating Sensor” appears in message field,
followed by “etCO2 Place Sensor on Ref Cell”.
6) Place sensor on Reference Cell.
7) Verify that”etCO2 Verifying Sensor Cal” followed by “etCO2 Sensor
Cal Verified” appears in message area, and reading in etCO2
parameter box = 38 ±2mmHg.
8) Attach adult airway adapter to calibration gas cylinder. Do NOT open
valve on cylinder.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 67
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 84

Service Manual SC 7000 and SC 9000XL Patient Monitors
300
290
280
270
260
250
240
230
220
210
200
190
180
170
160
150
140
130
120
110
100
90
80
70
60
5
40
20
0
Manometer
Pressure
Transducer
Tester
Inflation
Stopcock
(Closed)
Bulb
12HemoMed Pod
Figure 4-2 IBP Functional Verification Test Setup for HemoMed Pod
Note: As CO
is heavier than room air, set up the airway adapter
2
such that the point where the gas exits from the adapter is higher in
elevation than the point where it enters.
9) Place sensor on adult airway adapter and note reading = 0 ±1 mmHg.
10) Turn valve on the cylinder until it is fully open.
11) Wai t for 30 seconds and reco rd displayed value.
12) Close valve and remo ve sensor from airway.
13) V erify that measured v alue is in range (0.05 x local pressure) ±3,
rounded to nearest integer.
14) Select etCO
parameter box and set Atmospheric Pressure to AUTO.
2
15) Repeat steps 4 through 12.
16) V erify that measured v alue = previously me asured value ±3, rounded
to nearest integer.
Refer to Figure 4-2 for test setup. Invasive blood pressure and cardiac
output functions of HEMO2/4 PODs are incorporated in the HemoMed Pod.
A single cable connects the Pod to the HemoMed 1input on the left side of
the SC 7000 or SC 9000XL. Pressure labels for HemoMed Pod channels
are set in the monitor.
12.1 IBP Function
12.1.1 IBP Test setup 1) With MultiMed cable and all other patient inputs unplugged from monitor, power-cycle monitor. Select NO to clear display.
2) Plug cable from HemoM ed Pod output into HemoMed 1 co nnecto r on
SC 7000 or SC 9000XL monitor. See Figure 4-2.
68 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 85

SC 7000 and SC 9000XL Patient Monitors Service Manual
12.1.2 Channel A 3) With
4) Set IBP simulator for a static pressure = 0 mmHg.
Monitor Zero Function 5) P ress Zero All key on HemoMed Pod.
6) Verify that a “Zero Accepted” message that changes to “Static
7) Select a pulsatile pressure on patient simulator.
8) Assure that Cal Factor and Manometer Cal are set to 100.
9) Verify that pressure reading on monitor agrees with values generated
If verifying only SC 7000, omit remaining steps in this section and go to
section 12.2. If also verifying HEMO POD, go on to step 10.
12.1.3 Channel B 10) Unplug BP adapter cable from channel A on HEMO POD and plug it
11) V erify that pressure reading on monitor agrees with values generated
12) Do either step a or step b as appropriate.
MAIN
screen displayed, connect BP output from simulator to first
input, channel A, on HEMO POD adapter.
Note: “Zero Required” message, appears on display.
Note: All four pressures are zeroed simultaneously in the monitor,
even if only channels A and B are to be used in the HemoMed Pod.
Pressure” appear in the message field.
by pressure signal from simulator.
into channel B.
by pressure signal from simulator.
a If HemoMed Pod has four channels, unplug the BP adapter cable
from channel B and plug it into channel C. then go on to step 13.
b If HemoMed Pod has only two channels, bypass remaining steps
of this section and go to section 12.2.
12.1.4 Channel C 13) Unplug BP adapter cable from channel B on HemoMed Pod and plug it into channel C.
14) V erify that pressure reading on monitor agrees with values generated
by pressure signal from simulator.
12.1.5 Channel D 15) Unplug BP adapter cable from channel C on HemoMed Pod and plug it into channel D.
16) V erify that pressure reading on monitor agrees with values generated
by pressure signal from simulator.
17) Unpl ug simulator input adapter cable from Hemo Med Pod, and go on
to section 12.2.
12.2 Cardiac Output Function
1) Plug C.O. output from simulator into C.O. test adapter cable, and plug
adapter cable into C.O input on HemoMed Pod.
2) When READY appears in CO parameter field verify that blood
temperature indication is 37±0.15°C.
3) Press C.O. START key on simulato r, and verify an Injectate
Temperature indication of 1±0.2°C.
13HEMO POD2/4
13.1 IBP Function
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 69
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
Refer to Figure 4-3 on page 70 for test setup.
IBP parameter boxes for up to two pressures for HEMO 2 POD or up to four
pressures for HEMO 4 POD display automatically when IBP signal from
POD is plugged into monitor, when Display Mode is set to automatic.
NOT A CONTROLLE D DOCUMENT
Page 86

Service Manual SC 7000 and SC 9000XL Patient Monitors
300
290
280
270
260
250
240
230
220
210
200
190
180
170
160
150
140
130
120
110
100
90
80
70
60
5
40
20
0
Manometer
Pressure
Transducer
Tester
Inflation
Stopcock
(Closed)
Bulb
Figure 4-3 IBP Functional Verification Test Setup for HEMO2/4 PODs
If verifying proper IVP functioning of only the Monitor, do sections 13.1.1
and 13.1.2, and then go on to section 13.2. If functionally verifying the
HEMO POD also complete sections 13.1.3, 13.1.4, and 13.1.5.
13.1.1 IBP Test setup 1) With MultiMed cable and all other patient inputs unplugged from monitor, power-cycle monitor. Select NO to clear display.
2) Plug cable from HEMO POD IBP SC 9000 output into Aux./Hemo 3
input on SC 7000 or SC 9000XL monitor.
13.1.2 HEMO2/4 POD Channel A 3) With
MAIN
screen displayed, connect BP output from simulator to first
input, channel A, on HEMO POD adapter.
4) Set IBP simulator for a static pressure = 0 mmHg.
Note: “Zero Required” message, identified by same pressure label is
shown in LCD window for channel A on front of HEMO POD appears
on display.
Monitor Zero Function 5) Press Zero All key on HEMO POD.
6) Verify that a “Zero Accepted” message that changes to “Static
Pressure”, both identified by the same pressure label, appear in the
message field.
7) Select a pulsatile pressure on patient simulator.
8) Assure that Cal Factor and Manometer Cal are set to 100.
9) Verify that pressure reading on monitor is in agreement with values
generated by pressure signal from simulator.
10) If monitor is an SC 9000XL, plug cable from HEMO POD IBP SC 9000
output into Aux./Hemo2 input and repeat steps 3 through 9. Otherwise,
continue.
11) If fun ctionally verifying only the SC 7000 or SC 9000X L, omit the
remaining steps in this section and go to Section 13.2. If also
functionally verifying HEMO POD, go on to step 12.
70 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 87

SC 7000 and SC 9000XL Patient Monitors Service Manual
13.1.3 HEMO2/4 POD Channel B 12) Unplug BP adapter cable from channel A on HEMO POD and plug it into channel B.
13) Obs erve th at pressure label change s to same pressure label as is
shown in LCD window for channel B on front of HEMO POD.
14) V erify that pressure reading on monitor is in agreement with values
generated by pressure signal from simulator.
15) Do either step a or step b as appropriate.
a If the HEMO POD has four channels, unplug the BP adapter cable
from channel B and plug it into channel C. then go on to step 16.
b If the HEMO POD has only two channels, bypass remaining steps
of this section and go to section 13.2.
13.1.4 HEMO4 POD Channel C 16) Unplug BP adapter cable from channel B on HEMO POD and plug it into channel C.
17) Obs erve th at pressure label change s to same pressure label as is
shown in LCD window for channel C on front of HEMO POD.
18) V erify that pressure reading on monitor is in agreement with values
generated by pressure signal from simulator.
13.1.5 HEMO4 POD Channe l D 19) Unplug BP adapter cable from channel C on HEMO POD and plug it into channel D.
13.2 Temperature Function
20) Obs erve th at pressure label change s to same pressure label as is
shown in LCD window for channel D on front of HEMO POD.
21) V erify that pressure reading on monitor is in agreement with values
generated by pressure signal from simulator.
22) Unpl ug simulator input adapter cable from HEMO POD, and go on to
section 13.2.
1) Plug fixed temperature (37°C) output from simulator into TEMP A
connector HEMO POD.
2) Plug selectable temperature output from simulator into TEMP B
connector HEMO POD, and set temperature for other than 37°C.
3) Verify the following:
• T field appears on
• T1a temperature = 37 ±0.1°C
• T1b temperature = simulator setting ±0.1°C.
4) Select Tem perature field, and acces s TEMP 1 menu .
5) Select TEMP Display and then select .
6) Verify that T1b changes to and reports temperature difference
between T1a and T1b ±0.2°C.
7) Reset TEMP Display in TEMP1 menu to T1b.
MAIN
screen
∆T1
∆T1
8) Press Main Screen key to clear table and return to
13.3 Cardiac Output Function
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 71
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
1) Plug C.O. output from simulator into C.O. test adapter cable, and plug
adapter cable into C.O./Temp B input on HEMO POD.
2) When READY appears in CO parameter field verify that blood
temperature indication is 37±0.15°C.
NOT A CONTROLLE D DOCUMENT
MAIN
Screen.
Page 88

Service Manual SC 7000 and SC 9000XL Patient Monitors
3) Press C.O. START key on simulato r, and verify an Injectate
Temperature indication of 1±0.2°C.
14Memory Backup
Functi on
15CPS/IDS Mode
The monitor retains patient-related data, such as alarm limits, trends, and
stored alarm recordings when it is powered off.
1) With monitor powered-up and no patient inputs applied, press Alarms
Limits fixed key and change limit for any parameter.
Note: Note time on Real Time Clock.
2) Power monitor off for approximately 2 minutes, and then power it back
on again.
3) After
4) Verify that new limit(s) you set in Step 1 have been retained, and that
This procedure tests that monitor communicates with a CPS or IDS. Omit
this test and go on to Section 16 if monitor used exclusively in DirectNet
mode.
1) With monitor mounted on docking station connected to a CPS, or on
2) Enter biomed password (
3) Select Network Setup → Network Config. → CPS/IDS → Save ALL.
4) Press Menu key and select Monitor Setup → Biomed → Logs
MAIN
screen displays, press Alarm Limits fixed key to call up
Alarm Limits Table.
clock has advanced the proper amount of time.
IDS press Menu key, and select Monitor Setup → Biome d → Service.
) and select “Accept.”
4712
Note: Monitor resets if Network Config. previously set for DirectNet.
16DirectNet Mo de
(requires ≥VC2-level
installed software)
5) Select Component Log → CPS/IDS.
6) Verify that Serial # of CPS or IDS appears on display.
This checks for proper configuration of a monitor set up for DirectNet
functioning, and for monitor communication via the I
this test if monitor used exclusively in CPS/IDS mode.
1) With monitor disconnected from doc king station, connec t monitor to
NFINITY NETWORK
I
Note: Remove label covering ethernet connector on right-hand side of
monitor, if necessary.
2) Press Menu key, and select M onitor Setup → Biome d → Service.
3) Enter biomed password (
4) Select Network Setup → Network Config. → DirectNet → Save ALL.
Note: Monitor resets if Network Config. previously set for CPS/IDS.
5) Setup monitor for simulated patent using external patient simulator.
6) Verify that waveforms display on MVWS.
Note: If I
function of another monitor on network to view waveforms. Then skip
step 7 and go to step 8.
7) Access
NFINITY NETWORK
netInfo
using ethernet connector on right side of monitor.
) and select “Accept.”
4712
not equipped with MVWS, use remote view
on MVWS and verify that monitor labels are unique.
NFINITY NETWORK
. Omit
8) Follow procedure in steps 2 through 4 to reset monitor to CPS/IDS
mode, if required.
72 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 89

SC 7000 and SC 9000XL Patient Monitors Service Manual
,'6
3RZHU
6XSSO\
,'6
3RZHU
6XSSO\
&36
36/
6XSSO\
3RZHU
,'6
LEAKAGE
TESTER
LEAKAGE
TESTER
LEAKAGE
TESTER
CPS
CPS
CPS
DOCKING
STATION
1),1,7<
,
DOCKING
'RFNLQJ
STATION
6WDWLRQ
DOCKING
25
STATION
MONITOR
MONITOR
MONITOR
17Leakage Current
Tests
.
Figure 4-4 Leakage Current Test Setups
Table 4-3 Leakage Current Tests
TEST Max. Curre nt
Combined Lead Leakage <10µA
Individual Lead Leakage <10µA
Paired Lead Leakage <10µA
Leakage with Line Voltage on Leads <50µA
SC 7000 and SC 9000XL monitors are battery operated devices,
functionally grounded through CPS or IDS power supply when operated
from a docking station. Leakage current tests assure that under both
normal and fault conditions, any leakage current does not exceed values
given inTable 4-3.
1) Perform leakage current tests with monitor on a docking station, and
CPS, IDS Power Supply, or PSL plugged into leakage tester. See
Figure 4-4.
2) Follow leakage tester manufacturer’s instructions to measure each of
leakage currents given in Table 4-3, for each of following conditions:
• open ground
• reversed polarity
• open ground reversed polarity
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 73
7k9kXLSM.c4.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 90

Service Manual SC 7000 and SC 9000XL Patient Monitors
3) Verify that current does not exceed values given in Table 4-3.
4) Record all values in monitor’s functional verification checklist.
18Battery Charger
Circuit
19Recorder Function
1) With a partially discharged main (internal) battery and no external
(auxiliary) battery installed, place monitor on powered docking station
and bring up
2) Slide lever on IDS to unlock position and note battery charge level.
3) Slide lever on IDS back to power position, and allow battery to charge
for ≈1 hr.
4) After 1 hr., verify that charge level on battery has increased.
5) With main battery at full charge and monitor on battery power, insert
external battery. Verify that battery charge level indicator at bottom of
MAIN
screen changes from internal indicator to external indicator.
The R50 Recorder connects to the monitor through the CPS or IDS, or
through an interface plate. The following procedure verifies that the monitor
is communicating with the Recorder.
1) Connect known good R50 Recorder to monitor, either through a CPS/
IDS or via an interface plate.
2) Press Menu key, and acce ss Monitor Setup → Biomed → Serv i c e
3) Enter Service password (
4) Select Bedside Setup, and set Waveform Simulator to ON.
5) After monitor cycles, bring up
6) Press Record fixed key.
MAIN
screen.
) and select Accept.
4712
MAIN
screen.
7) Verify that recorder begins to dispense waveform printout.
8) Press Stop key on recorder to stop paper flow.
9) Press Menu key, and acce ss Monit or Setup → Biomed → Service.
10) Enter Service password (
11) Select Bedside Setup, and set Waveform Simulator to OFF.
) and select Accept.
4712
74 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c4. CD_ROM . fm/0 4-99/ kaupp
Page 91

Chapter 5: Troubleshooting
1Introduction
Troubleshooting SC 7000 and SC 9000XL monitors is either a two- step or
three-step process.
Step 1) Determine whether the trouble is external, such as a
malfunctioning module, Pod, connector, or cable, or internal.
Step 2) Do either a or b as appropriate.
a If external, recalibrate or replace malfunctioning item.
b If internal, go on to step 3.
Step 3)Usual remedial action is to replace malfunctioning component
or subassembly. See “Appendix A: Replacement Parts” fo r
complete listing of replaceable system components and
subassemblies. After replacing an internal subassembly,
functionally verify all monitor functions before returning monitor
to clinical service.
SC 7000 and SC 9000XL monitoring system devices consist of the Base
Unit, and peripheral devices including the Docking Station, CPS, IDS w/
Power Supply, R50 Recorder, etCO
Pod, HEMO or HemoMed Pod, and Remote Display.
2 Recommended Tools and Test Equipme nt
Use the specified, recommended tools and test equipmen t, or a known
equivalent, when troubleshooting SC 7000 / SC 9000XL mo nitors and
peripheral equipment. Substitutions are approved only if an equivalent is
listed. Use of other test equipment and/or accessories could result in
inconclusive tests or damage to system components.
Module, MultiMed or MultiMed 12
2
Table 5-1 Recommended Tools and T est Equipment
Tools & Test Equipment Descri ption
Digital Multimeter (DMM), 4.5 digit Fluke, model 8050A (or equiv.)
Patient ECG/RESP, Temp, IBP simulator DNI Medsim 300B or equivalent
Leads:Three-lead grabber set, or IEC color code 1
IEC color code 2
Five-lead grabber set I EC color code 1
IEC color code 2
Patient SpO
Reusable SpO
sensor:
NBP simulator (calibrated) or DNI CuffLink
Mercury manometer with hand bulb, or Baumanometer, 0-300 mmHg
Electronic pressure indicator with handbulb Veri-Cal Pressure Transducer Tester, or
NBP Calibration Assembly Art. No. 28 77 855 EE54U
NBP connection hose 3.7 m Art. No. 12 75 275 EH40U
simulat or , or Nellcor P T2500 or equivalent
2
2
Durasensor, Adult Art. No. 45 34 475 EH50U
Art. No. 33 75 230 E530U
Art. No. 33 75 248 E530U
Art. No. 33 75 255 E530U
Art. No. 33 75 263 E530U
equivalent
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 75
7k9kXLSM.c5.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 92

Service Manual SC 7000 and SC 9000XL Patient Monitors
3 Power Problems
Before troubleshooting power problems, keep in mind that fuses are used
to protect delicate circuits from potentially harmful currents. Replacement
of a fuse may provide only a temporary solution and may not remove the
source of the fault. Never replace a fuse with other than what is specified.
3.1 Monitor won’t power
ON when co nnected to
exte rnal po wer source
(CPS, IDS, IDS Power
Supply, or PSL)
11 12
Docking Connector on CPS or IDS
BAT
EXT
F2
PSL
1) Is external AC power present?
Yes: Continue.
No: Troubleshoot line.
2) If monitor being powered by a CPS or IDS, depress curved docking
connector cover door on docking station to access docking connector,
and measure output voltage across pins 11 and 12 of connector (see
illustration at left),
if monitor being powered by an IDS Power
or
Supply or PSL, measure output voltage.
3) Is voltage = 11.6 to 13.8 VDC?
Yes: Cont inue .
No: Replace CPS/IDS or IDS Power Supply.
C19
C20
C18
C24
C25
C21
C22
C26
C27
C17
C16
C10
F2
F1
External Connector Side
Figure 5-1 Connector I/O PCB
BAT
INT
F3
C6
C7
C4
C5
C14
R3
R4
R1
R2
1
X4
X4
Interior Side
4) Does Monitor power ON using battery power?
Yes: The n problem is either with main processor PCB or, if
powering monitor from PSL, fuse F1 may be open.
,I SRZHULQJ PRQLWRU IURP &36,'6 UHSODFH 0DLQ 3URFHVVRU
3&% 6XEDVVHPEO\ ,I SRZHULQJ PRQLWRU IURP 36/ FRQWLQXH
WR VWHS
No: Go to Section 3.4, Troubleshooting ON/OFF cont rol.
F3
C13
C11
C12
L2
L3
C15 J5 J4
J1
C29 C28
J3
R8
R7
R5
R6
R11
C8
C9
F1
J2
76 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c5. CD_ROM . fm/0 4-99/ kaupp
Page 93

SC 7000 and SC 9000XL Patient Monitors Service Manual
5) Open monitor and remove Main Processor PCB Subassembly from
rear housing to access Connector I/O PCB.
6) Check continuity of F1. See Figure 5-1 on page 76.
Note: It is not necessary to remove Connector I/O PCB from rear
housing or lift one side of fuse. With power sources unplugged from
monitor and nothing plugged into X1, continuity of F1 can be checked
from solder points on interior side of board.
Removing the Connector I/O PCB requires that the slide lock on the
etCO2 connector on back of the monitor be removed to release the
board. This damages the label above the connector. The damaged
label must be removed and a replacement label (supplied with
replacement fuses) installed.
7) Does F1 measure as open? (>5Ω)
Yes: Remove Connector I/O PCB, replace F1, reassemble
monitor, and perform monitor power-on check. If F1 opens a
second time, replace F1 and Main Processor PCB
Subassembly.
No: Replace Main Processor PCB Subassembly.
3.2 Using main battery as
power source, monitor
either doesn’t
maintain monitor
operations for
prescribed time, or
won’t power ON.
1) Does unit power ON while connected to an external power source?
Yes: Cont inue
No: Go to Section 3.4, Troubleshooting ON/OFF cont rol.
2) Remove all external power sources (including external battery if
installed), remove back cover, and unplug battery cable from main
battery.
3) Is voltage = 11.6 to 13.8 VDC present at battery terminals?
Yes: Continue to step 4.
No: Battery is not charged to 12VDC. Reconnect battery cable
to battery terminals, and go to Section 3.5.
4) Check in-line fuse in power harness (if installed), and check for <5Ω
between black wire battery terminal connector and pin 4 on connector
X1. See Figure 5-1 on page 76.
5) Is harness fuse OK, and resistance between black wire terminal
connector and pin 4 on connector X1 <5Ω?
Yes: Open monitor and remove Main Processor PCB
Subassembly from rear housing to access Connector I/O
PCB. Then continue to step 6.
No: Either fuse in battery power harness is open or there is
discontinuity between black wire terminal connector and pin
4 on X1. Replace harness, and perform monitor power-on
check. If fuse opens a second time, replace harness and
Main Processor PCB Subassembly.
6) Check continuity of F3. See Figure 5-1 on page 76.
Note: It is not necessary to remove Connector I/O PCB from rear
housing or lift one side of fuse. With power sources unplugged from
monitor and nothing plugged into X1, continuity of F3 can be checked
from solder points on interior side of board.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 77
7k9kXLSM.c5.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 94

Service Manual SC 7000 and SC 9000XL Patient Monitors
Removing the Connector I/O PCB requires that the slide lock on the
etCO
connector on back of the monitor be removed to release the
2
board. This damages the label above the connector. The damaged
label must then be removed and a replacement label (supplied with
replacement fuses) installed in its place. It is necessary to remove a
Connector I/O PCB only if a fuse needs to be replaced.
7) Is F3 open? (>5Ω)
Yes: Repl ace fuse, reassemble m onitor, and continue to step 8.
No: Replace Main Processor PCB Subassembly.
8) Does monitor power ON using only main battery as power source?
Yes: Return monitor to service after checkout.
No: Replace fuse and Main Processor PCB Subassembly.
3.3 With external battery installed, monitor fails to function on battery power for prescribed time.
1) Remove external battery and measure battery terminal voltage.
2) Is voltage = 11.6 to 13.8 VDC?
Yes: Continue to step 5.
No: Battery is not charged to 12VDC. Reinsert external battery
into monitor, and go to Section 3.5.
3) Remove back cover, and with external power plugged into monitor
check voltage between pins 1 and 2 of X1. See Figure 5-1 on page 76
4) Is voltage = 13.6 to 13.9 VDC?
Yes: Go to Section 3.2.
No: Continue to step 5.
5) Check continuity of F2. See Figure 5-1 on page 76.
Note: It is not necessary to remove Connector I/O PCB from rear
housing or lift one side of fuse. With power sources unplugged from
monitor and nothing plugged into X1, continuity of F2 can be checked
from solder points on interior side of board.
Removing the Connector I/O PCB requires that the slide lock on the
etCO2 connector on back of the monitor be removed to release the
board. This damages the label above the connector. The damaged
label must then be removed and a replacement label (supplied with
replacement fuses) installed in its place. It is necessary to remove a
Connector I/O PCB only if a fuse needs to be replaced.
6) Is F2 open? (>5Ω)
Yes: Repl ace fuse, reassemble m onitor, and continue to step 8.
No: Replace Main Processor PCB Subassembly.
7) Install charged external battery and unplug power harness from either
terminal of main battery.
8) Does monitor power ON using only external battery as power source?
Yes: Reconnect power harness cable to main battery, and return
monitor to service after checkout.
No: Replace fuse and Main Processor PCB Subassembly.
78 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c5. CD_ROM . fm/0 4-99/ kaupp
Page 95

SC 7000 and SC 9000XL Patient Monitors Service Manual
3.4 ON/OFF control problem
1) Open monitor and remove M ain Processor P CB Subass em bly from
rear housing to access Connector I/O PCB.
2) Check continuity of F1, F2, and F3. See Figure 5-1 on page 76.
Note: It is not necessary to remove Connector I/O PCB from rear
housing or lift one side of fuse. With power sources unplugged from
monitor and nothing plugged into X4, continuity of F1, F2, and F3 can
be checked from solder points on interior side of board.
Removing the Connector I/O PCB requires that the slide lock on the
etCO2 connector on back of the monitor be removed to release the
board. This damages the label above the connector. The damaged
label must then be removed and a replacement label (supplied with
replacement fuses) installed in its place.
3) Does F1, F2 or F3 measure as open?
Yes: Remove Connector I/O PCB, replace open fuse(s),
reassemble monitor, and perform monitor power-on check.
,I IXVHV R SHQV D VHFRQG WLPH UHSODFH IXVHV DQG 0DLQ
3URFHVVRU 3&% 6XED VVHPEO\
No: Inspect 44-pin connector for bent pin or misalignment. If OK,
replace Front Bezel.
4) Does replacement of Front Bezel remedy problem?
Yes: Fun ctionally verify proper operation of monitor and return
monitor to clinical service.
No: Replace Main Processor PCB Subassembly.
3.5 Internal or external (auxiliary) battery doesn’t charge
1) When monitor connected to external power source, does battery
charger LED illuminate?
Yes: Battery possibly defective, fuse on power harness open, or
fuse on connector I/O board open. Continue to step 2.
No: Replace battery. If problem persists, replace Main
Processor PCB Subassembly. If still no charge indication,
replace Front Panel Subassembly.
2) Remove battery/NBP compartment access door and unplug battery
power cable connector from X1. See F igure 5-1 on page 76.
3) Connect external power source to monitor.
1
2
3
4
4) Re f er to illustration at lef t .
• Measure voltage between pins 3 and 4 of X1 on Connector I/O board
to check charging voltage for main battery.
• Measure voltage between pins 1 and 2 of X1 on Connector I/O board
to check charging voltage for external battery.
5) Is voltage = 13.6 to 13.9 VDC?
Yes: For main battery, go on to step 6. For external battery, go on
to step 8.
No: Go to step 8.
6) Check continuity of in-line fuse in power cable harness.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 79
7k9kXLSM.c5.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 96

Service Manual SC 7000 and SC 9000XL Patient Monitors
7) Is resistance <5Ω?
Yes: Go on to step 8.
No: Replace power cable harness.
8) Plug power cable connector back into X1, unplug battery connectors
from battery terminals (main battery) or remove external battery, and
measure voltage at battery connectors on power cable.
9) Is voltage = 13.6 to 13.9 VDC?
Yes: Replace battery.
No: Replace power cable. If problem recurs, Replace Main
Processor PCB Subassembly.
10) Open monitor and remove Main Processor PCB Subassembly from
rear housing to access Connector I/O PCB.
11) Check continuity of F2 (if external battery problem) or F3 (if main
battery problem). See Figure 5-1 on page 76.
Note: It is not necessary to remove Connector I/O PCB from rear
housing. With power sources unplugged from monitor and nothing
plugged into X1, continuity of F2 and F3 can be checked from solder
points on interior side of board.
Removing the Connector I/O PCB requires that the slide lock on the
etCO2 connector on back of the monitor be removed to release the
board, which damages the label above the connector. The damaged
label must then be removed and a replacement label (supplied with
replacement fuses) installed.
12) Does F2 or F3 measure as open? (>5Ω)
Yes: Remove Connector I/O PCB, replace open fuse(s),
reassemble monitor, and perform monitor power-on check.
If fuse opens a second time, replace fuse and Main
Processor PCB Subassembly. Othe rwise, go on to step 13.
No: Replace Main Processor PCB.
13) Does battery charge after replacing harness, fuse(s) or battery?
Yes: Return monitor to service after checkout.
No: Replace Main Processor PCB Subassembly.
3.6 Power-Up Sequence Fails to Complete Properly
Table 5-2 Power-up Process Malfunction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Power inputs all OK but
monitor fails to
complete power-up
sequence, e.g., sounds
continuous tone or
powers itself down,
sounds two tones and
then a continuous tone,
continually resets .
Software program
corrupted
Main Processo r PCB
malfunction
1. If power ON LE D illuminates bu t monitor fails to
complete power-up sequence, check the following:
2. If monitor has been functioni ng properly and problem
occurred spontaneously, software may have becom e
corrupted. Try reinstalling software.
3. If problem persists, replace Main Processor PCB
Subassembly.
4. If problem persists, contact TSS in Solna or Danvers.
80 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c5. CD_ROM . fm/0 4-99/ kaupp
Page 97

SC 7000 and SC 9000XL Patient Monitors Service Manual
4 Monitor Resets
During startup and also during normal monitor operations, diagnostic
programs running in the background environment provide a constant
monitoring of critical hardware components and software functions.
In the event a critical component or software function is determined by the
software to be malfunctioning or there is no response to a requested task,
the diagnostics may force a full or partial main processor reset. Such events
can be identified by either a temporary loss of display or by a highly audible
watchdog alert tone. Monitor resets are typically recorded in the diagnostic
error log, which can be retrieved for interpretation and diagnosis by factory
trained experts.
Should a monitor exhibit symptoms of a reset, compare contents of the
diagnostic error log with the list of Error Messages and Diagnostic Codes
in Appendix C, for possible remedial action. Otherwise, record the
information on a copy of the “Problem Report” on page 91 at the end of this
Chapter, and forward it along with the diagnostic error log to your respective
TSS center.
5 Power On/Off Piezo Tone Fails to Sound.
Table 5-3 Power-off Alarm Malfunction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Piezo tone fails to
sound when monitor
powered ON or OFF,
or loses power.
Main Processor PCB
malfunction
1. Replace Main Processor PCB Subassem bly.
2. If problem persists, contact TSS in Solna or Danvers.
6 Rotary Knob Malfunction.
Table 5-4 Rotary Knob Malfunction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Rotary knob fails to
properly select fields,
or pressing the knob in
fails to activate a menu
or select a default.
Optical Encoder
malfunction
Front Bezel PC Board
malfunction
Main Processor PCB
malfunction
1. Replace Optical Encoder.
2. Replace Front Bezel PC Board.
3. If problem persists, replace Main Proc essor PCB
Subassembly.
4. If problem persists, contact TSS in Solna or Danvers.
7 Fixed Key Fails to Function.
Table 5-5 Fixed Key M alfun ction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
A Fixed Key fails to
initiate change
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 81
7k9kXLSM.c5.CD_ROM.fm/04-99/kaupp
Front Bezel Membrane
Switch or PC Boar d
malfunction
Main Processor PCB
malfunction
NOT A CONTROLLE D DOCUMENT
1. Replace Front Bezel/Lens Subassembly.
2. If problem persists, replace Fron t Bezel PC Board.
3. If problem persists, replace Main Processor PCB
Subassembly.
4. If problem persists, contact TSS in Solna or Danvers.
Page 98

Service Manual SC 7000 and SC 9000XL Patient Monitors
8 LCD Display Malfunction
Table 5-6 LCD Display Malfunction
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Display backlight
intensity does not v ary
with change in ambient
light
> 17 inoperative pixels
(“stuck” ON or OFF) .
Areas of display
missing or color
contaminated
Sensor malfunction
Front Bezel PC Board
malfunction
LCD screen malfunction Replace Front Bezel Subassembly.
LCD Display malfunction
Front Bezel PC Board
malfunction
Graphics Processor on
Main Processor PCB
malfunction
.
1. Assure that monitor is being powered by CPS/IDS or
PSL, and intensity control is set to “Auto” mode.
2. • If in brightly lighted environment, cover ambient
sensor on upper right corner of front bezel.
• If in dimly lighted environment, shine light source
directly on ambient sensor on upper right corner of
front bezel.
3. If no change in display intensity, replace Front Bezel
PC Board. If problem persists, replace Main
Processor PCB Subass emb ly.
4. If problem persists, contact TSS in Solna or Danvers.
1. Using VGA connection cable and interface plate,
connect external VGA display to X7 on interface
plate.
2. • If external display exhibits similar problem, replace
Main Processor PCB Subasse mbly.
• If external display OK, replace Front Bezel
Subassembly. If problem persists, replace Main
Processor PCB Subassembly.
Backlight fails to
provide sufficient and
consistent background
illumination for the
LCD display.
Backlight defective
Front Bezel PC Board
malfunction
Main Processor PCB
malfunction
9 Isolating Cable Malfunctions
In general, the troubleshooting and repair approach for cable malfunctions
is to use a known input signal for any given parameter, and then replace a
cable or sensor found to be malfunctioning. Cable malfunctions, including
those associated with connectors on the cables, generally fall into one of
three cagegories -- Open circuits, Short circuits, and Intermittent conditions
Open circuits and short circuits manifest themselves as a loss of signal.
Software in the Monitor senses the loss, and generates an error message
such as “ECG Leads Off” and “SpO2 Transparent.” Typically, short circuits
result in software resets.
An intermittent condition manifests itself as noise on the signal. The source
of the noise can often be isolated by removing the signal and shorting the
input(s) to the cable. Then flex along the cable, particularly at connectors,
while watching for noise indications on the monitor display.
3. If problem persists, contact TSS in Solna or Danvers.
1. Replace backlights.
2. If problem persists, replace Front Bezel PC Board.
3. If problem persists, replace Main Processor PCB
Subassembly.
4. If problem persists, contact TSS in Solna or Danvers.
82 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c5. CD_ROM . fm/0 4-99/ kaupp
Page 99

SC 7000 and SC 9000XL Patient Monitors Service Manual
10Visible or Audible Alarm Reporting Failure.
Table 5-7 Alarm Malfunctions
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Audible Alarm O.K.,
but Visible Alarm Fails.
Visiblel Alarm O.K.,
but Audible Alarm
Fails.
Software pr ob lem 1. Try re ins t a lling softwar e.
2. If problem persists, contact TSS in Solna or Danvers.
Speaker malfunction
Main Processor PCB
malfunction
1. Power-cycle monitor and listen for tone after icon
appears on power-up screen (not the piezo, which
sounds before the icon appears).
2. If tone fails to sound, remove rear cover and check
speaker cable plugged into X7 on Connector I/O
board.
3. If speaker cable plugged in OK, replace Speaker
Subassembly.
4. If problem persists, replace Main Processor PCB
Subassembly.
5. If problem persists, replace Rear Housing
Subassembly.
6. If problem persists, contact TSS in Solna or Danvers.
11MultiMed POD - Parameter Signal Problems
Table 5-8 Parameter Signal Problems
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
Failure to report lead-off
condition
ECG/Resp waveform
noise
MultiMed POD
malfunction
Main Processor PCB
malfunction
Incorrect setting of line
frequency for customer
site
Poor connection or
intermittent break
MultiMed POD
malfunction
Main Processor PCB
malfunction
1. Check MultiMed Pod contadct for possible contamination. Clean if required. If problem persists, replace Pod.
2. If problem persists, replace Main Processor PCB
Subassembly.
3. If problem persists, contact TSS in Solna or Danvers.
1. Access the Service Menu under Monitor Setup →
Biomed → Service in the Main menu.
2. Assure that the setting is proper for the frequency of the
power source at the customer site.
3. If problem persists, check cables, connections, and
MultiMed POD for intermittent breaks.
4. Connect grabber connectors of an ECG lead set to a
common conductor, such as the shank of a screwdriver
blade, to produce a flatline ECG waveform.
5. Watch for a distinct change in noise level, indicating the
source of the problem,
(particularly at connectors).
6. Replace a defective ECG lead, cable, or MultiMed POD
7. If no cable, connector, or POD problem, replace Main
Processor PCB Subassembly.
as you flex each lead and cable
8. If problem persists, contact TSS in Solna or Danvers.
ASK-T898-03-7600 Siemens Medical Systems, EM-PCS Danvers 83
7k9kXLSM.c5.CD_ROM.fm/04-99/kaupp
NOT A CONTROLLE D DOCUMENT
Page 100

Service Manual SC 7000 and SC 9000XL Patient Monitors
Table 5-8 Parameter Signal Problems (Continued)
Symptom(s) Possible Cause(s) Troubleshooting and Remedial Action
SpO
parameter box
2
fails to appear when
sensor plugged into
MultiMed POD, or SpO
readings missing
Sensor malfunction
Open cable or connector
MultiMed POD
malfunction
2
Main Processor PCB
malfunction
SpO
waveform noise P oo r connection or
2
intermittent break in cable
MultiMed POD
malfunction
Main Processor PCB
malfunction
1. Check illumination of red LED in the sensor.
2. • If LED not illuminated, replace sensor and continue
to step 3.
• If LED illu min ated , place sensor on your finger and
go on to step 3.
3. If problem persists, replace intermediate cable between
sensor and MultiMed POD.
4. If problem persists, replace MultiMed POD.
5. If problem persists, replace Main Processor PCB
Subassembly.
6. If problem persists, contact TSS in Solna or Danvers.
1. With the SpO
sensor on your finger, observe the
2
waveform while you flex the lead and cable, particularly
at the sensor, at connectors, and at the MultiMed POD.
2. Watch for a distinct change in the waveform (distinctly
different from artifact) as you flex along the length of the
cables as well as at the sensor and connectors.
3. Replace a defective sensor , cable or MultiMed POD.
4. If no cable, connector, or POD problem, replace Main
Processor PCB Subassembly.
Temp parameter box
fails to appear when
sensor plugged into
MultiMed POD, Temp
readings missing or
inaccurate
Sensor malfunction
Open cable or connector
MultiMed POD
malfunction
Main Processor Board
malfunction
12NBP
12.1NBP Error Messages
1%3 2SHQ /LQH
1%3 %ORFNHG /LQH
1%3 2YHUSUHVVXUH
1%3 &XII 'HIODWLRQ (UURU
5. If problem persists, contact TSS in Solna or Danvers.
1. Replace sensor
2. If problem persists, replace MultiMed POD.
3. If problem persists, replace Main Processor PCB
Subassembly.
4. If problem persists, contact TSS in Solna or Danvers.
Results if the NBP measurement circuit does not sense pressure changes
after initiating inflation. Possible causes include an open line out to the
patient, an open or occluded line on the pressure measurement line running
between the NBP assembly and the pressure transducer on the main
processor board, a leaky cuff or cuff connector, or a defective valve on the
NBP pump assembly.
Result of the NBP measurement circuit detecting an occlusion on the line
to the patient, or a neonatal cuff with monitor in adult mode.
Result attributable to hardware or software detecting overpressure.
Result of the two minute NBP measurement timer expiring. It is typically
triggered when an NBP measurement had been taken prior to placing the
unit in calibration mode. (When calibrating, power-cycle monitor and then
don’t run pump until after calibration.)
84 Siemens Medical Systems, EM-PCS, Danvers ASK-T898-03-7600
NOT A CONTROLLE D DOCUMENT
7k9kXLSM .c5. CD_ROM . fm/0 4-99/ kaupp
 Loading...
Loading...