

Page 1
Instructions for Use
Avalon Fetal Monitor
FM20/30, FM40/50
Release G.0 with Software Revision G.02.xx
Patient Monitoring
Page 2

Page 3
1Table of Contents
1 Introduction 9
Who this Book is For 9
Confirm Fetal Life Before Using the Monitor 10
Introducing the Avalon Family of Fetal Monitors 11
2 Installation 13
Installation Checklist 13
Unpacking and Checking the Shipment 14
Mounting the Monitor 15
Mounting the External Power Supply (M8023A) 15
Connecting the Monitor to AC Mains 16
How and When to Carry Out the Test Blocks 17
Safety Tests 18
3 Basic Operation 19
Supported Measurements 19
Avalon FM20 and FM30 20
Avalon FM40 and FM50 21
Cordless Monitoring 22
Getting to Know Your Avalon FM20/FM30 23
Getting to Know Your Avalon FM40/FM50 24
Operating and Navigating 27
Operating Modes 32
Automatic Screen Layouts 33
Settings 33
Checking Your Monitor Revision 35
Preparing to Monitor 35
Starting Monitoring 53
Switching the Monitor to Standby 54
After Monitoring 54
Disconnecting from Power 54
Troubleshooting 55
4 Using Batteries (with FM20/30 Battery Option) 57
External Power Supply M8023A 58
Battery Power Indicators 58
Battery Status Window 60
Optimizing Battery Performance 61
3
Page 4
5 Alarms 63
Alarm Mode 63
Visual Alarm Indicators 64
Audible Alarm Indicators 64
Acknowledging Alarms 66
Acknowledging Disconnect INOPs 66
Pausing or Switching Off Alarms 66
Alarm Limits 68
Reviewing Alarms 68
Latching Alarms 69
Testing Alarms 71
Alarm Behavior at Power On 71
6 Patient Alarms and INOPs 73
Alarm Messages 73
Technical Alarm Messages (INOPs) 76
7 Admitting and Discharging 83
Admit/Discharge on the Monitor 83
New Patient Check 84
OB TraceVue: via LAN 85
OB TraceVue: via RS232 85
8 Non-Stress Test Timer 87
Setting NST Autostart/Autostop 87
Viewing the NST Timer 87
Timer Expiry Notification 87
Accessing the NST Setup Pop-up Keys 88
9 Non-Stress Test Report 91
Setting Up an NST Report 91
NST Report Status Window 92
NST Reassurance Criteria 94
Non-Reassuring Report 94
Non-Reactive NST Test 94
10 Monitoring FHR and FMP Using Ultrasound 95
Technical Description 95
Limitations of the Technology 96
Misidentification of MHR as FHR 96
Cross-Channel Verification 97
What You Need 97
Cordless Monitoring - Important Considerations 97
Preparing to Monitor 98
Selecting Fetal Heart Sound 99
Changing the Fetal Heart Sound Volume 99
4
Page 5
Fetal Movement Profile 100
Troubleshooting 102
Additional Information 103
Testing Ultrasound Transducers 112
11 Monitoring Twin FHRs 113
Important Considerations 113
Monitoring Twins Externally 114
Monitoring Twins Internally 115
Cross-Channel Verification 115
Separating FHR Traces 116
Troubleshooting 119
12 Monitoring Triple FHRs 121
Important Considerations 121
Monitoring Triplets 122
Cross-Channel Verification 122
Separating FHR Traces 123
"Standard" Separation Order 123
"Classic" Separation Order 123
When Trace Separation is Off 124
Troubleshooting 125
13 Fetal Heart Rate Alarms 127
Changing Alarm Settings 127
Changing Signal Loss Delay 128
14 Monitoring Uterine Activity Externally 129
What You Need 129
External Toco Monitoring 130
Toco Sensitivity 130
Troubleshooting 131
Testing Toco Transducers 132
15 Monitoring Uterine Activity Internally 133
What You Need 133
Internal (IUP) Monitoring 134
Troubleshooting 135
16 Monitoring FHR Using DECG 137
Misidentification of MHR as FHR 137
What You Need 137
Making Connections 139
Monitoring DECG 139
Suppressing Artifacts 140
Troubleshooting 141
5
Page 6
Testing DECG Mode 142
17 Monitoring Noninvasive Blood Pressure 143
Introducing the Oscillometric Noninvasive Blood Pressure Measurement 143
Preparing to Measure Noninvasive Blood Pressure 144
Starting and Stopping Measurements 146
Enabling Automatic Mode and Setting Repetition Time 146
Choosing the Alarm Source 147
Assisting Venous Puncture 147
Calibration 148
Troubleshooting 148
18 Monitoring SpO2 149
Selecting an SpO2 Sensor 149
Applying the Sensor 149
Connecting SpO2 Cables 150
Measuring SpO2 151
SpO2 Signal Quality Indicator 152
Assessing a Suspicious SpO2 Reading 152
Understanding SpO2 Alarms 152
Setting Up Tone Modulation 153
Setting the QRS Volume 153
19 Monitoring Maternal Heart / Pulse Rate 155
Priority for Maternal Heart / Pulse Rate 155
Cross-Channel Verification 155
MHR from MECG Electrodes 156
Monitoring MECG Wave 158
Pulse Rate from SpO2 159
Pulse Rate from Toco MP 159
Adjusting the Heart Rate / Pulse Alarm Limits 160
Average Pulse Rate from Noninvasive Blood Pressure 160
Troubleshooting 160
Testing MECG Mode 160
20 Printing the ECG Waveform 161
21 Paper Save Mode for Maternal Measurements 165
22 Recovering Data 167
Recovering Traces on Paper 167
Recovering Traces on an OB TraceVue System 168
Recording Stored Data 168
23 Care and Cleaning 171
General Points 171
6
Page 7
Cleaning and Disinfecting 172
Cleaning and Disinfecting Monitoring Accessories 173
Sterilizing 173
24 Maintenance 175
Inspecting the Equipment and Accessories 175
Inspecting the Cables and Cords 175
Maintenance Task and Test Schedule 176
Storing Recorder Paper 176
Cleaning the Printhead 177
Disposing of the Monitor 177
25 Accessories and Supplies 179
Information on Latex 179
Transducers 179
Fetal Accessories 180
DECG Accessories: Component Compatibility 181
MECG Accessories 181
Noninvasive Blood Pressure Accessories 181
SpO2 Accessories 183
Recorder Paper 187
26 Specifications and Standards Compliance 189
Environmental Specifications 189
Physical Specifications 190
Performance Specifications 191
Recorder Specifications 201
Battery Specifications 203
Alarm Defaults 204
Compatible External Displays: FM40/FM50 Only 204
Manufacturer's Information 205
Trademark Acknowledgement 205
Regulatory and Standards Compliance 205
Environment 212
Monitoring After a Loss of Power 212
ESU, MRI and Defibrillation 213
Cardiac Pacemakers and Electrical Stimulators 213
Fast Transients/Bursts 213
Symbols on the System 214
Index 217
7
Page 8

8
Page 9

1Introduction
Who this Book is For
This book is for trained healthcare professionals using the Avalon FM20, FM30, FM40 and FM50
fetal/maternal monitors. It describes how to set up and use the monitor and transducers. Familiarize
yourself with all instructions including warnings and cautions before starting to monitor patients. Read
and keep the Instructions for Use that come with any accessories, as these contain important
information about application and care and cleaning that is not repeated in this book.
You should be:
• Trained in the use of fetal heart rate (FHR) monitors.
• Trained in the interpretation of FHR traces.
• Familiar with using medical devices and with standard fetal monitoring procedures.
1
For information on how to configure and service the monitor, refer to the Service Guide, or contact your
authorized service provider.
Your monitor may not have all of the features and options described in this guide. The exact
appearance of the monitor may differ slightly from that shown in the illustrations.
In this guide:
•A warning alerts you to a potential serious outcome, adverse event or safety hazard. Failure to
observe a warning may result in death or serious injury to the user or patient.
•A caution alerts you to where special care is necessary for the safe and effective use of the
product. Failure to observe a caution may result in minor or moderate personal injury or damage
to the product or other property, and possibly in a remote risk of more serious injury.
• Monitor refers to the entire fetal/maternal monitor. Display refers to the physical display unit.
Screen refers to everything you see on the monitor's display, such as measurements, alarms,
patient data and so forth.
FM30 • Whenever a monitor’s identifier appears to the left of a heading or paragraph, it means that the
information applies to that monitor only. Where the information applies to all models, no
distinction is made.
9
Page 10

1Introduction
Confirm Fetal Life Before Using the Monitor
Fetal monitoring technology available today is not always able to differentiate a fetal heart rate (FHR)
signal source from a maternal heart rate (MHR) source in all situations. Therefore, you should confirm
fetal life by independent means before starting to use the fetal monitor, for example, by palpation of fetal
movement or auscultation of fetal heart sounds using a fetoscope, stethoscope, or Pinard stethoscope.
If you cannot hear the fetal heart sounds, and you cannot confirm fetal movement by palpation,
confirm fetal life using obstetric ultrasonography. Continue to confirm that the fetus is the signal
source for the FHR during monitoring.
Be aware that:
• a MHR trace can exhibit features that are very similar to those of a FHR trace, even including
accelerations and decelerations. Do not rely solely on trace pattern features to identify a fetal
source.
• Fetal Movement Profile (FMP) annotations on a fetal trace alone may not always indicate that the
fetus is alive. The body of a deceased fetus can move and cause the monitor to annotate fetal body
movements.
Here are some examples where the MHR can be misidentified as the FHR.
• When using an ultrasound transducer:
– It is possible to pick up maternal signal sources, such as the aorta or other large vessels.
– Misidentification may occur when the MHR is higher than normal (especially when it is over
100 bpm).
• When using a fetal scalp electrode:
– Electrical impulses from the maternal heart can sometimes be transmitted to the fetal monitor
through a recently deceased fetus via the spiral scalp electrode cable, appearing to be a fetal
signal source.
– The recorded MHR (and any artifact) can be misinterpreted as a FHR (especially when it is
over 100 bpm).
• When Fetal Movement Profile (FMP) is enabled:
FMP annotations in the absence of fetal life may be a result of:
– Movement of the deceased fetus during or following maternal movement.
– Movement of the deceased fetus during or following manual palpation of fetal movement
(especially if the pressure applied is too forceful).
– Movement of the ultrasound transducer.
– The ultrasound transducer detecting a maternal movement source, such as the mother
coughing.
See also the chapters “Monitoring FHR and FMP Using Ultrasound” on page 95 and “Monitoring
FHR Using DECG” on page 137.
To reduce the possibility of mistaking the MHR for FHR, it is recommended that you monitor both
maternal and fetal heart rates. The monitor's cross-channel verification (CCV) facility can help by
automatically detecting when a MHR coincides with a FHR. For further details, see “Cross-Channel
Verification” on page 97.
10
Page 11
1 Introduction
Introducing the Avalon Family of Fetal Monitors
The Avalon family of fetal monitors consists of the Avalon FM20, FM30, FM40 and FM50. While the
FM20/FM30 and the FM40/FM50 have different form factors, the method of operation is very
similar for all monitors. The Avalon fetal monitors also share the same transducers, accessories,
software, and are compatible with the Avalon CTS Cordless Fetal Transducer System (M2720A).
Intended Use
The Philips Avalon FM20 (M2702A), FM30 (M2703A), FM40 (M2704A) and FM50 (M2705A) Fetal/
Maternal Monitors are intended for:
• non-invasive monitoring of fetal heart rates and movements.
• non-invasive monitoring of maternal heart rates, maternal pulse rates, uterine activity, maternal
noninvasive blood pressure, and maternal oxygen saturation.
• invasive monitoring of fetal Direct ECG and intrauterine pressure and for displaying and
recording of fetal and maternal ECG waves. (FM30 and FM50 only)
• displaying, storing and recording patient data and parameter values and for generating alarms from
fetal and maternal parameters.
• transmitting patient data and parameter values to a patient information and surveillance system.
• use by trained health care professionals.
• use in antepartum testing areas, in labor and delivery rooms and during postpartum recovery in the
hospital environment. They are not intended for use in intensive care units or operating rooms.
• transport situations in healthcare facilities, for healthcare facilities outside hospitals, such as
doctors’ offices, and for use in private households. (FM20 and FM30 only)
WARNING
The fetal/maternal monitors are not intended for:
• use during defibrillation, electro-surgery, or magnetic resonance imaging (MRI).
• ECG measurements on patients connected to electrical stimulators or with cardiac pacemakers.
• use of the invasive measurements IUP and fetal DECG and use of the patient module (M2738A)
in domestic establishments and those connected directly to the public low-voltage supply network
that supplies buildings used for domestic purposes.
CAUTION
US federal law restricts this device to sale by, or on the order of, a physician.
11
Page 12

1Introduction
Indications for Use
Avalon Fetal/Maternal Monitor FM20:
Indicated for use by trained health care professionals whenever there is a need for monitoring of the
physiological parameters uterine activity, heart rate, oxygen saturation, non-invasive blood pressure,
pulse rate of pregnant women and the fetal heart rates of single fetuses, twins, and triplets in labor and
delivery rooms, in antepartum testing areas, in private households and during transports in healthcare
facilities.
Avalon Fetal/Maternal Monitor FM30:
Indicated for use by trained health care professionals whenever there is a need for monitoring of the
physiological parameters uterine activity, heart rate, ECG, oxygen saturation, non-invasive blood
pressure, and pulse rate of pregnant women and the fetal heart rates of single fetuses, twins, and
triplets in labor and delivery rooms, in antepartum testing areas, in private households and during
transports in healthcare facilities.
Avalon Fetal/Maternal Monitor FM40:
Indicated for use by trained health care professionals whenever there is a need for monitoring of the
physiological parameters uterine activity, heart rate, oxygen saturation, non-invasive blood pressure,
and pulse rate of pregnant women and the fetal heart rates of single fetuses, twins, and triplets in labor
and delivery rooms and in antepartum testing areas.
Avalon Fetal/Maternal Monitor FM50:
Indicated for use by trained health care professionals whenever there is a need for monitoring of the
physiological parameters uterine activity, heart rate, ECG, oxygen saturation, non-invasive blood
pressure, and pulse rate of pregnant women and the fetal heart rates of single fetuses, twins, and
triplets in labor and delivery rooms and in antepartum testing areas.
12
Page 13
2Installation
Installation should be carried out by qualified service personnel, either by the hospital's biomedical
department, or by Philips Support.
As the first step in preparing the monitor for use, follow the installation instructions given in
this chapter.
For a list of conventions used in this guide, see “Basic Operation” on page 19.
Not all accessories and supplies may be available in all geographies. Please contact your local Philips
sales representative for details of availability.
Installation Checklist
Use this checklist to document your installation.
2
Step Task Check Box
when Task
Done
1 Perform initial inspection of delivery, unpack and check the shipment
(see “Unpacking and Checking the Shipment” on page 14)
2 Mount the monitor as appropriate for your installation (see “Mounting
the Monitor” on page 15)
3 Connect the fetal monitor to AC mains using the supplied power cord.
This configuration varies, depending whether an external power
supply/battery option is used. (see “External Power Supply M8023A”
on page 58)
4 Perform Safety Tests (see “Safety Tests” on page 18)
5 Check that default settings (including the line frequency) are
appropriate for your institution
6 Check/set the paper scale (see “Checking/Setting Paper Scale” on
page 42)
7 Load paper into the recorder (see “Loading Paper: FM20/FM30” on
page 44 or “Loading Paper: FM40/FM50” on page 45, depending on
your monitor)
8 Check/set the time and date (see “Setting the Date and Time” on
page 35)
13
Page 14
2 Installation
Step Task Check Box
9 Check/set paper speed (see “Choosing Paper Speed” on page 48)
10 Perform System Test as necessary (see the Service Guide)
11 For monitors with the battery option (#E25) chosen, confirm that the
battery can be charged, and that the monitor can be powered by the
battery.
12 Test Transducers (see “Testing Ultrasound Transducers” on page 112
and “Testing Toco Transducers” on page 132)
Unpacking and Checking the Shipment
The monitor and any supporting options ordered are supplied packed in protective shipping cartons.
Initial Inspection
Before unpacking, visually check the packaging and ensure that there are no signs of mishandling or
damage.
when Task
Done
Open the package carefully and remove the instrument and accessories.
Check that the contents are complete and that the correct options and accessories have been delivered.
System Components, Accessories and Supplies FM20 FM30 FM40 FM50
Toco+ Transducer (with belt clip) - optional - optional
Toco MP Transducer (with belt clip) 1111
US Transducer (with belt clip) 1111
Patient Module for DECG/MECG/IUP optional
DECG Reusable Legplate Adapter Cable - 1 - 1
MECG Adapter Cable - 1 - 1
IUP Adapter Cable
External Power Supply and MSL Cable optional optional - -
Event Marker optional optional optional optional
Fetal Paper Pack (country-specific, installed) 1111
Powercord 1111
Printed Instructions for Use 1111
Documentation DVD: includes FM20/30 Service Guide,
FM40/50 Service Guide, Instructions for Use (including
localized versions), and Training Guide
2
1
optional optional
- optional - optional
1111
1
optional
14
1
For assessment of maternal heart rate only.
2
Ships with Patient Module (K03).
Page 15
2 Installation
Claims for Damage
If the shipping cartons are damaged, contact the carrier.
If any of the equipment is damaged, contact both the carrier and your local Philips service organization
for repair or replacement arrangements.
Repacking
Retain the original packing carton and material, in case you need to return equipment to Philips for
service. If you no longer have the original packing materials, Philips can advise you on alternatives.
Mounting the Monitor
FM20/30 The monitor can be rested on a flat surface, set at an angle using the built-in stand, or mounted on a
wall, on a cart or on a rollstand. See the Service Guide for details.
FM40/50 The monitor can be rested on a flat surface, or on a cart. See your monitor's Service Guide for details.
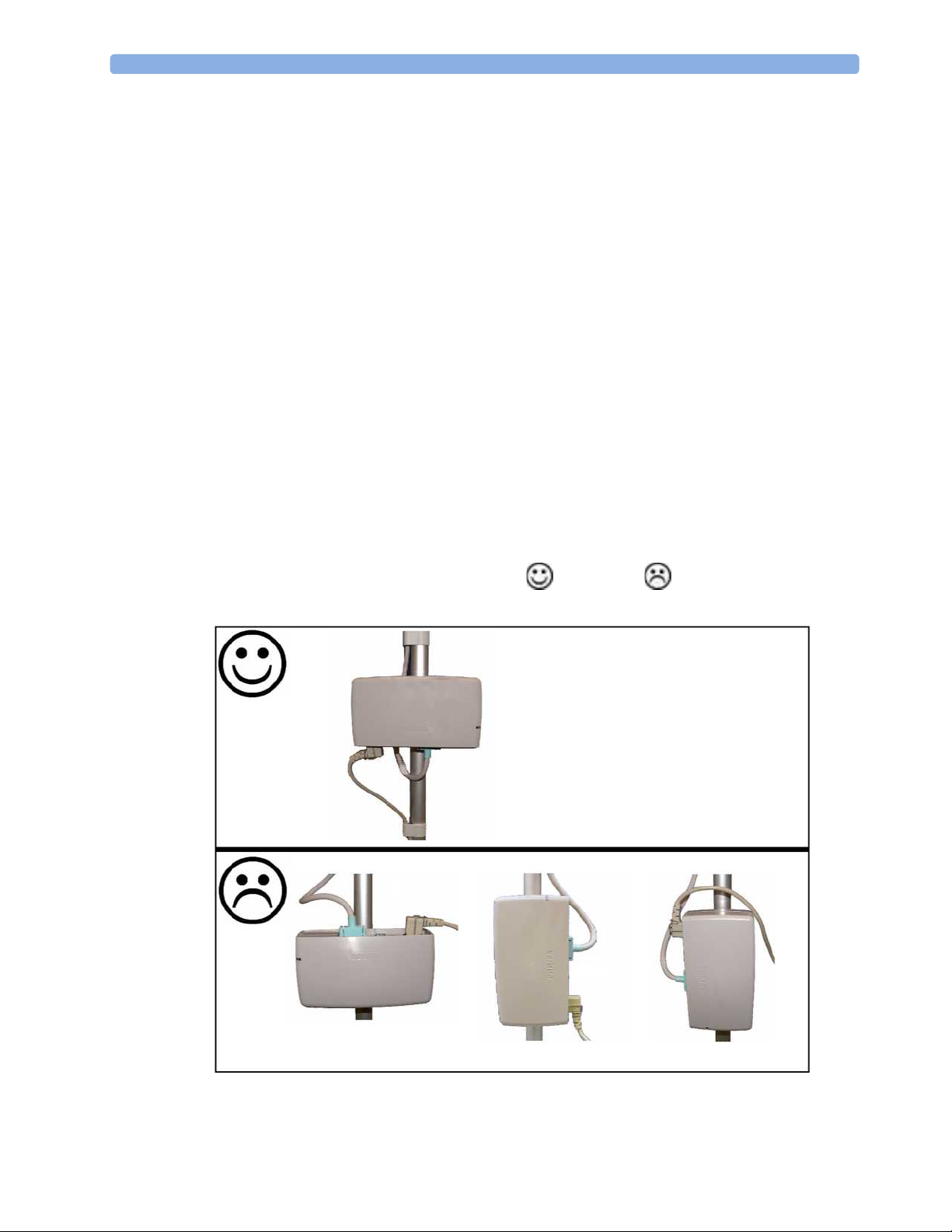
Mounting the External Power Supply (M8023A)
The external power supply (M8023A option #E25) can be rested on its rubber feet on a flat, level
surface, or mounted as described in the Service Guide.
The following pictures show examples of correct and incorrect ways to mount the power
supply.
15
Page 16
2 Installation
Connecting the Monitor to AC Mains
FM20/30 The monitor is an electrical Class II device in which the protection against electric shock does not rely
on basic insulation and a protective earth conductor but on double and/or reinforced insulation.
FM40/50 The monitor is an electrical Class I device. Protection against electric shock is provided by a protective
earth conductor.
The monitor has a wide-range power supply that allows you to operate the monitor from an AC
(alternating current) power source of 100 V to 240 V (± 10%) and 50 or 60 Hz (± 5%).
WARNING
• Always use the supplied power cord with the earthed mains plug to connect the monitor to an
earthed AC mains socket. Never adapt the mains plug from the power supply to fit an unearthed
AC mains socket.
• Check that the line frequency is correctly set for your institution (50 Hz or 60 Hz) before putting
the monitor into service.
• FM20/FM30 only: The protective earth conductor is required for EMC purposes. It has no
protective function against electric shock! The protection against electric shock in this device is
provided by double and/or reinforced insulation.
• Do not use AC mains extension cords or multiple portable socket-outlets.
16
Page 17
2 Installation
How and When to Carry Out the Test Blocks
The following table defines which test and inspection blocks need to be performed, and when they are
required.
Test Blo ck Test or Inspection to be Performed Test Blo ck R equire d fo r
Which Events?
Visual Inspect the monitor, transducers and cables for any
damage.
Are they free of damage?
Power On Power on the monitor. Does it boot up successfully without
errors? After boot up the monitor sounds a tone, and can
you see the monitoring main screen.
If recorder power-on auto-start is configured to On, does
the recorder print
“Switching the Recorder On and Off ” on page 49 for
details.)
Functionality Test FM20/30 with Battery Option #E25 Only
After power up, touch the battery status indicator in the
bottom right of the screen. The battery status window
should open. Check to see if there is an exclamation mark
flashing in the gauge. Press the
the window and return to the main screen.
Safety Tests (1) to (4) Perform safety tests (1) to (4), as described in your
monitor's Service Guide, for standalone devices if required by
local regulations, and each time you combine equipment to
form a system, or exchange system components.
Performance Test the transducers (see “Testing Ultrasound Transducers”
on page 112 and “Testing Toco Transducers” on page 132).
System Perform the system test according to IEC/EN 60601-1-1/
IEC/EN 62353, if applicable, after combining equipment
to form a system (see your monitor's Service Guide).
Selftest: OK across the trace paper? (See
Main Screen key to close
Installation
Preventive Maintenance
Installation
Preventive Maintenance
Installation
Preventive Maintenance
Installation
Preventive Maintenance
Installation
Preventive Maintenance
Combining system
components
For test and inspection information regarding repairs, upgrades and all other service events, refer to
your monitor's Service Guide.
17
Page 18
2 Installation
Safety Tests
Details of the safety tests and procedures required after an installation or an exchange of system
components are described in your monitor's Service Guide. These safety tests are derived from
international standards but may not be sufficient to meet local requirements.
WARNING
• Do not use additional AC mains extension cords or multiple portable socket-outlets. If a multiple
portable socket-outlet is used, the resulting system must be compliant with IEC/EN 60601-1-1.
• Do not connect any devices that are not supported as part of a system.
• Do not use a device in the patient vicinity if it does not comply with IEC/EN 60601-1. The whole
installation, including devices outside of the patient vicinity, must comply with IEC/EN 60601-1-
1. Any non-medical device, including a PC running an OB TraceVue system, placed and operated
in the patient's vicinity must be powered via a separating transformer (compliant with IEC/EN
60601-1-1) that ensures mechanical fixing of the power cords and covering of any unused power
outlets.
18
Page 19
3Basic Operation
This chapter gives you an overview of the monitor and its functions. It tells you how to perform tasks
that are common to all measurements (such as entering data, switching a measurement on, changing
some monitor settings, and setting up the recorder). The alarms section gives an overview of alarms.
The remaining sections tell you how to perform individual measurements, and how to care for and
maintain the equipment.
3
Supported Measurements
The following Fetal Measurements are supported:
Fetal Monitor
or Model
FM20 Standard Optional Standard - -
FM30 Standard Optional Standard Standard Standard
FM40 Standard Optional Standard - -
FM50 Standard Optional Standard Standard Standard
Fetal Heart Rate
(FHR) via US
(including Twins)
Triple FHR via
US
Toco FHR via Direct
ECG (DECG)
Intrauterine
Pressure (IUP)
19
Page 20
3 Basic Operation
The following Maternal Measurements are supported:
Fetal Monitor
or Model
FM20 Standard - Standard Optional -
FM30 Standard Standard Standard Optional Optional
FM40 Standard - Standard Standard Standard
FM50 Standard Standard Standard Standard Standard
Maternal
Heart Rate
(MHR) via
Maternal ECG
Electrodes
Maternal
ECG
(MECG)
Maternal Pulse
from Toco
Non-invasive Blood
Pressure with Pulse
Rate
Pulse Oximetry
(Maternal SpO
with Pulse Rate
Avalon FM20 and FM30
This section outlines the capabilities of your monitor.
)
2
Avalon FM20
The Avalon FM20 fetal/maternal monitor provides a solution for external fetal monitoring
applications, and optional non-invasive maternal vital signs.
You can monitor fetal heart rates (FHRs) externally using ultrasound, uterine activity and maternal
pulse using an external Toco transducer, and the maternal heart rate (MHR) via maternal ECG
electrodes, and optionally, non-invasive blood pressure.
Measurements are displayed on a 6.5-inch color display as numerics. The display is a touchscreen, and
you operate the monitor using this touchscreen interface. The integrated recorder documents fetal and
maternal measurements as well as user defined annotations.
You can connect the monitor to an OB TraceVue system via the RS232 connection, or over a LAN
connection (with OB TraceVue Revision E.00.00 and later).
20
Page 21

Avalon FM30
The Avalon FM30 fetal/maternal monitor offers a solution for both external and internal fetal
monitoring applications, and optional non-invasive maternal vital signs.
The Avalon FM30 shares all the features and capabilities of the Avalon FM20. In addition, you can
monitor one FHR internally via direct fetal electrocardiogram (DECG), uterine activity internally using
an intra-uterine pressure (IUP) catheter together with a Toco
optionally, maternal oxygen saturation (SpO
The Avalon FM30 carries the label, indicating that it is capable of intrapartum monitoring.
3 Basic Operation
+
transducer or patient module, and
).
2
FM20/30
Battery
Option
#E25 Only
The battery option for the FM20/30 provides support for the in-transport monitoring of all
measurements when disconnected from a power supply. Existing data storage is automatically
with
uploaded to OB TraceVue after reconnecting to the system. Trace printing during transport is also
possible.
Avalon FM40 and FM50
This section outlines the capabilities of your monitor.
Avalon FM40
The Avalon FM40 fetal/maternal monitor provides a solution for external fetal monitoring
applications, and non-invasive maternal vital signs.
You can monitor fetal heart rates (FHRs) externally using ultrasound, uterine activity using an external
Toco transducer, and the maternal heart rate (MHR) via maternal ECG electrodes, and non-invasive
blood pressure and maternal oxygen saturation (SpO
Measurements are displayed on a 6.5-inch color display as numerics. The display is a touchscreen, and
you operate the monitor using this touchscreen interface. The integrated recorder documents fetal and
maternal measurements as well as user defined annotations.
You can connect the monitor to an OB TraceVue obstetrical documentation and surveillance system
via the RS232 connection, or over a LAN connection (with OB TraceVue Revision E.00.00 and later).
).
2
21
Page 22
3 Basic Operation
Avalon FM50
The Avalon FM50 fetal/maternal monitor offers a solution for both external and internal fetal
monitoring applications, and non-invasive maternal vital signs.
The Avalon FM50 shares all the features and capabilities of the Avalon FM40. In addition, you can
monitor one FHR internally via direct fetal electrocardiogram (DECG), and uterine activity internally
using an intra-uterine pressure (IUP) catheter together with a Toco
The Avalon FM50 carries the label, indicating that it is capable of intrapartum monitoring.
Cordless Monitoring
All monitors are compatible with the Avalon CTS Cordless Fetal Transducer System (M2720A). Note
the following points regarding cordless monitoring:
• One Avalon CTS Cordless Fetal Transducer System can be connected to a monitor at a time.
• Monitoring multiple pregnancies using cordless transducers is not supported.
• Using a mixture of wired and cordless fetal transducers is not supported. You can use either wired
or cordless fetal transducers. If sufficient signal quality cannot be achieved using cordless fetal
transducers, then switching to wired transducers is recommended.
+
transducer or patient module.
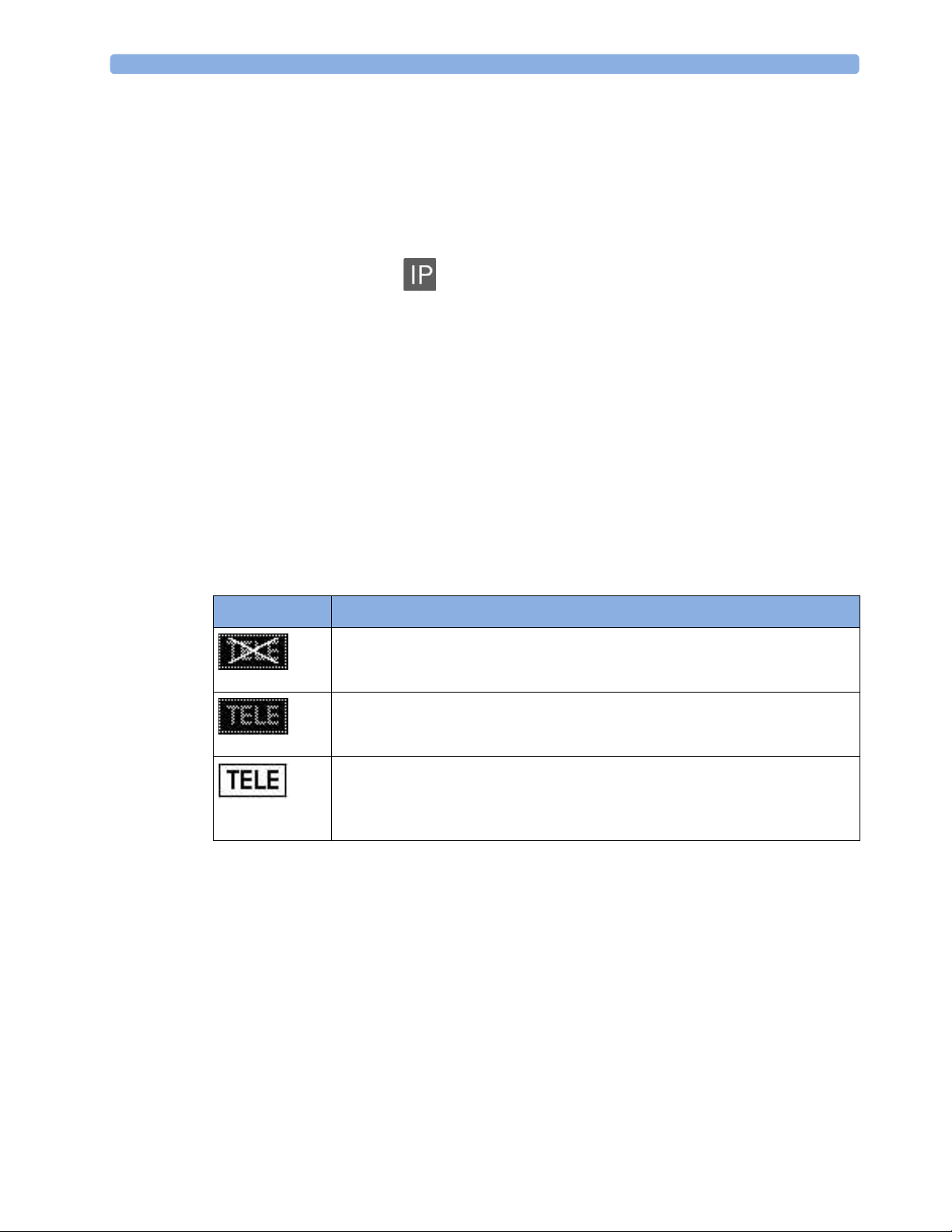
• When the monitor recognizes an Avalon CTS interface cable M2731-60001 (red connector) or
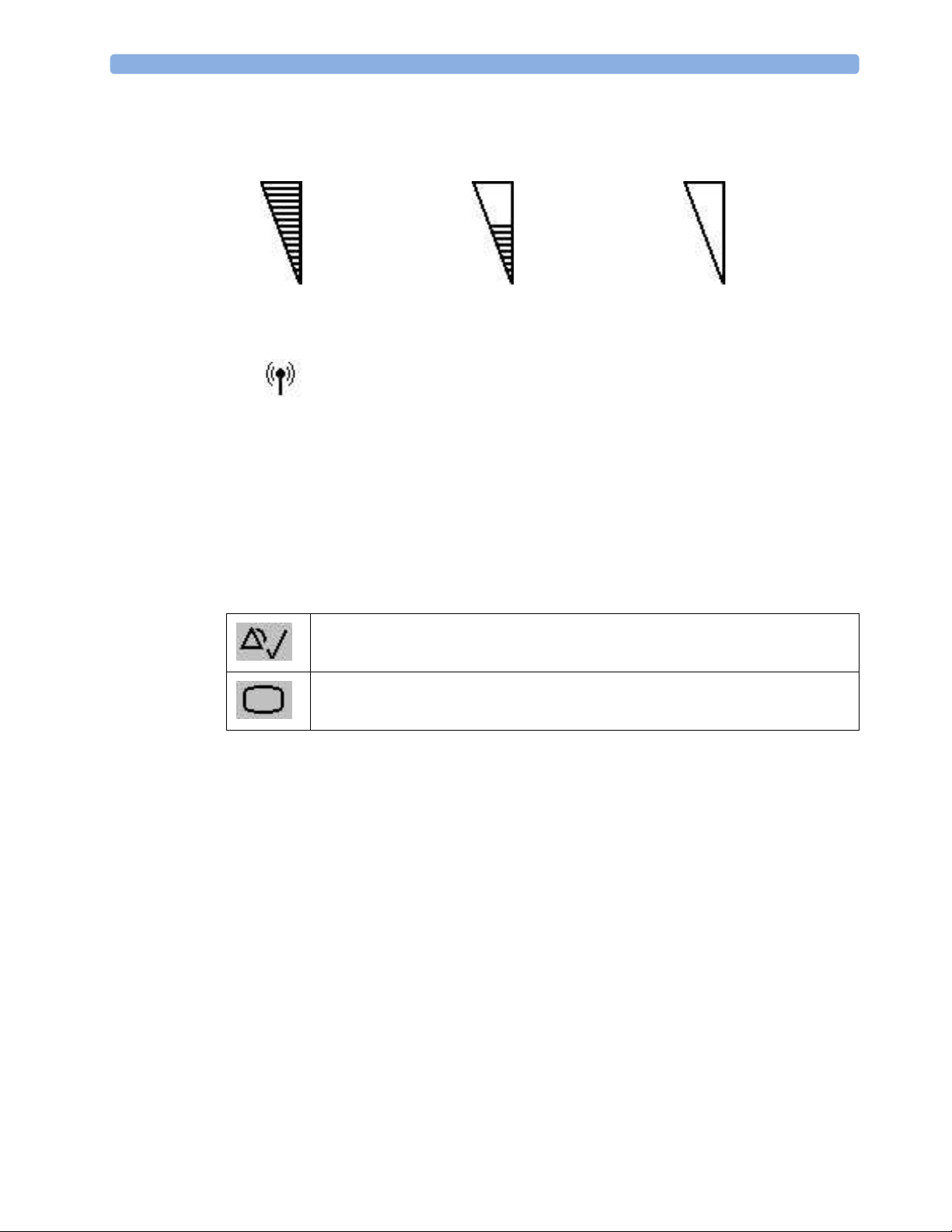
M2732-60001 (black connector, for rear connection on FM40/FM50 only), it gives confirmation
by showing the following status indicator in the lower right-hand corner of the screen:
Indicator Meaning
Avalon CTS interface cable is connected to the monitor, but the Avalon CTS base
station is not connected to the interface cable, disconnected from AC mains, or is
in Standby.
Avalon CTS interface cable is connected to the monitor, Avalon CTS base station
is connected, powered on, and cordless transducers are ready to use, but no
cordless transducers are currently active (all are still docked in the base station).
Avalon CTS interface cable is connected to the monitor, Avalon CTS base station
is connected, powered on, and at least one cordless transducer has been taken out
of the base station and is active. As cordless transducers have priority over wired
transducers, any connected wired transducers are disabled.
• Cordless transducers have priority over wired transducers. When an Avalon CTS base station is
connected via the appropriate interface cable to the fetal monitor, and there are also wired
transducers connected to the monitor, the wired transducers are disabled whenever a cordless
transducer is active. To change back to using wired transducers, dock the cordless transducers in
the Avalon CTS base station or switch the base station to Standby, and continue monitoring with
the wired transducers. Note that if a sufficient ultrasound signal quality cannot be achieved by
transducer repositioning, change to wired transducers.
22
• When using a cordless ultrasound transducer from an Avalon CTS system, the monitor
automatically sets the Fetal Movement Profile (
you wish, (see “Switching FMP On and Off ” on page 101), but you should refer to the sections
“Cordless Monitoring - Important Considerations” on page 97 and “Fetal Movement Profile” on
page 100.
FMP) to Off. You can enable the FMP again should
Page 23
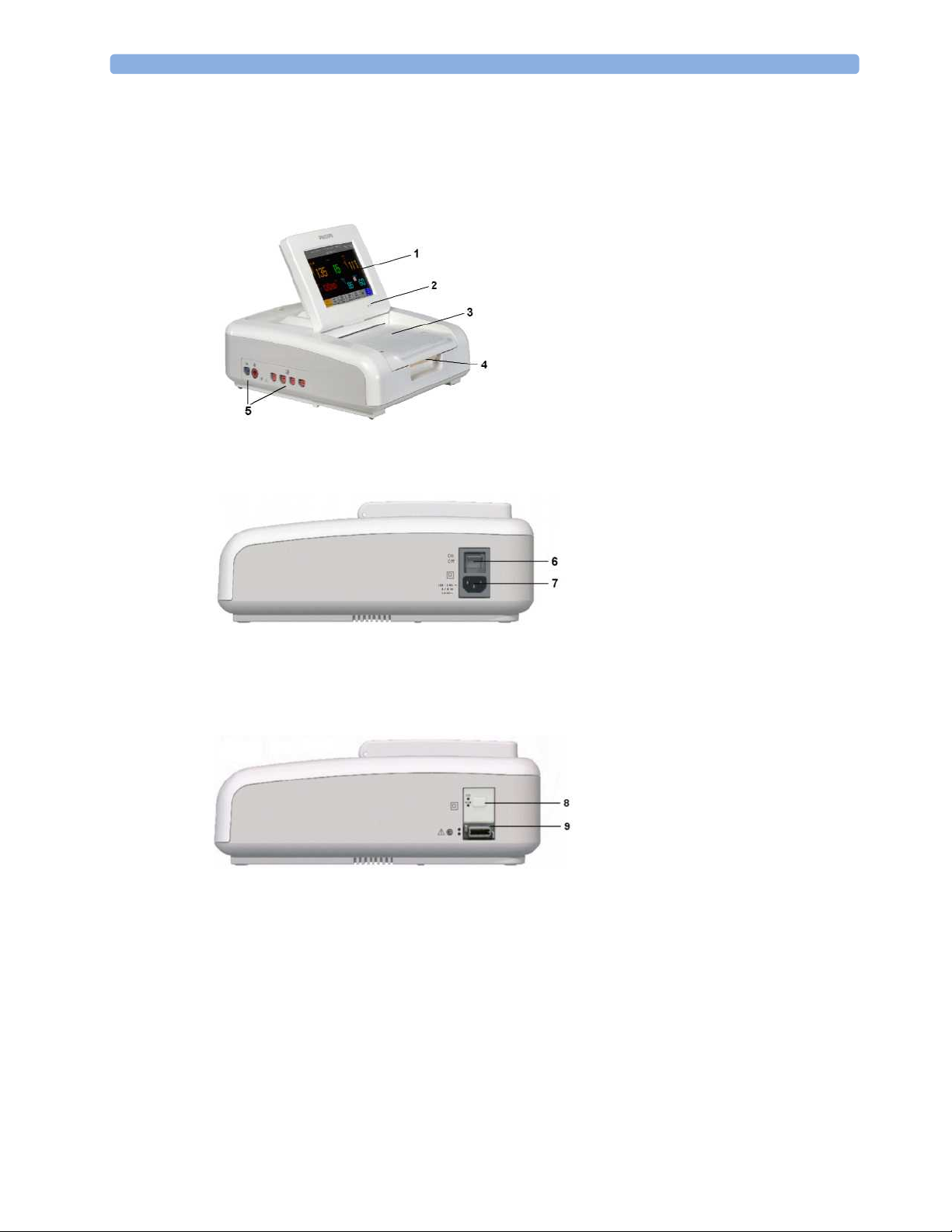
Getting to Know Your Avalon FM20/FM30
Overview
1 Touchscreen Display (tilt and
fold)
2 Power LED
3 Paper Drawer
4 Paper Drawer release
5 Connectors (see Left Side view)
Right Side
6 On/Off Switch
7 Power Connector
3 Basic Operation
with
Battery
Option
8 On/Standby Switch
9 MSL Connector
23
Page 24

3 Basic Operation
Rear
Left Side
10 Display Release
11 Carrying Handle
12 Built-in Stand
13 SpO
14 Noninvasive Blood Pressure
15 Fetal Sensor Sockets - each
Socket (optional)
2
Socket (optional)
socket accepts any fetal
transducer, an Avalon CTS
Cordless Fetal Transducer
System base station (connected
via the interface cable M2731-
60001), or event marker
Getting to Know Your Avalon FM40/FM50
Front
1 On/Standby Switch
2 Power LED
3 Recorder Paper Table
4 Touchscreen Color Display
5 Transparent Paper Guide with
tear-off edge
6 Paper Eject Button. Press to
open paper drawer. Press again
and hold when removing paper.
7 Fetal Sensor Sockets. Connect
any fetal sensor or patient
module here, including Avalon
CTS via M2731-60001 interface
cable (with red connector).
8 Noninvasive Blood Pressure
Socket
9 SpO
Socket
2
24
Page 25
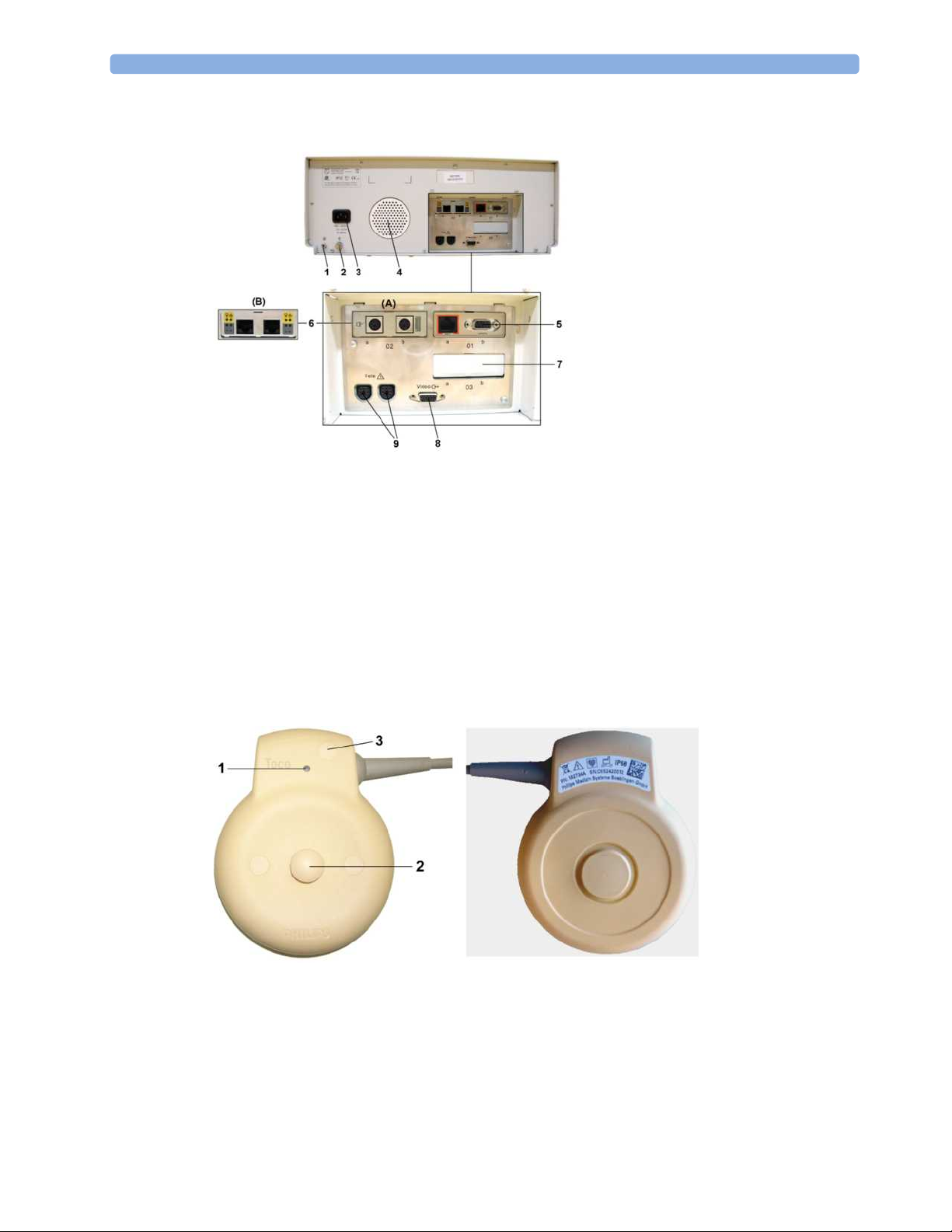
Rear
3 Basic Operation
1 Reserved for future use:
protective earth intended for use
in system installations.
2 Equipotential Grounding Point
3 Power Cord Connector
4 Loudspeaker
5 Slot 01 for optional LAN /
RS232 system interface (for
connection to an obstetrical
information and surveillance
system)
6 Slot 02 for optional interfaces:
Either dual PS/2 system
interface (A) for mouse and
keyboard connection)
Or MIB interface (B) for
external touch screen
connection
7 Slot 03 reserved for future use
8 Video Output (VGA)
9 Telemetry Interface. If not using
one of the fetal sensor sockets,
one Avalon CTS can be
connected at a time to either
socket using the M2732-60001
interface cable (with black
connector).
Transducers
Toco and Toco MP Transducer (M2734A, M2734B)
1 Transducer Finder LED - lights up on the transducer providing the measurement source.
2 Belt Button
3 "MP" for M2734B "Toco MP" transducers (additionally capable of providing the maternal pulse
measurement)
25
Page 26
3 Basic Operation
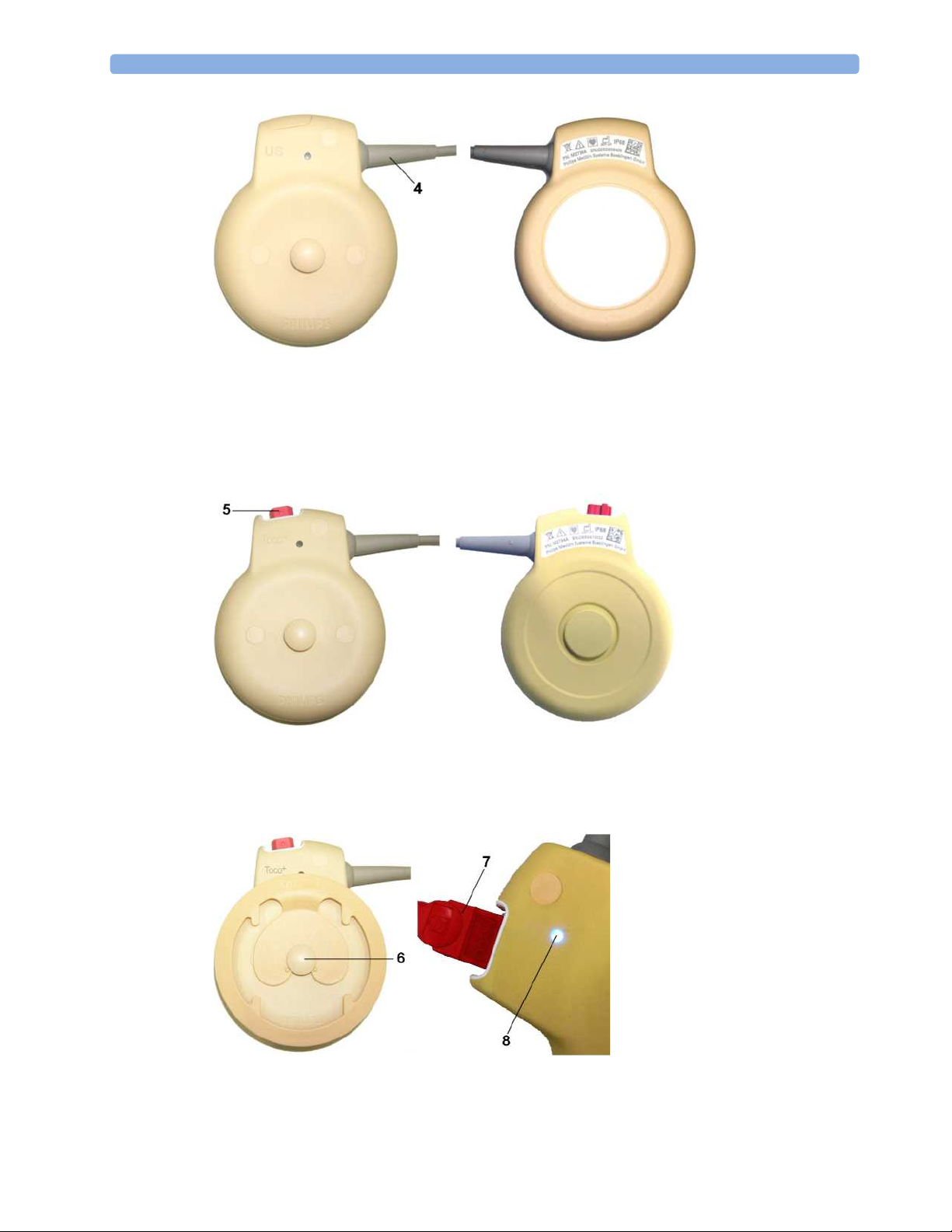
Ultrasound Transducer (M2736A)
4 Cable - connects to any of the four Fetal Sensor Sockets on the monitor
Note that the The M2736AA US transducer is identical to the M2736A US transducer,
including all specifications.
26
+
Transducer with ECG/IUP capability (M2735A)
Toco
5 Connector - for connecting ECG/IUP adapter cables (M2735A Toco
6 Butterfly Belt Clip (shown
fitted; for use with belts without
button holes)
7 Close-up of MECG adapter
cable connected to Toco
transducer
8 Close-up of active Finder LED
+
transducer only)
+
Page 27

3 Basic Operation
Patient Module for ECG/IUP (M2738A)
+
9 Connector - for connecting ECG/IUP adapter cables (same as for Toco
10 Cable - connects to any of the four Fetal Sensor Sockets on the monitor
transducer)
Operating and Navigating
Your monitor has a touchscreen. Everything you need to operate the monitor, other than to turn it on
and off, is contained on its screen. Most screen elements are interactive. Screen elements include
measurement numerics, screen keys, information fields, status indicators, alarms fields and menus.
FM40/50 If an optional external touch display with a MIB interface board are connected to the monitor, you can
operate the monitor using the external touch display.
Screen Elements
Monitor Information Line
1 INOP and alarm status area - shows active alert messages
2 LAN connection status indicator only. RS232 system connection is not indicated. Either the
Monitor is connected to OB TraceVue , the LAN cable is connected but no connection to
OB TraceVue ; or, if no indicator is shown, there is no network connection.
3 Patient identification
27
Page 28

3 Basic Operation
4
5 Bed label (when connected to a Philips OB TraceVue system)
6 Fetal heart sound volume adjust/indicator
7 Alarm volume adjust/indicator
8 Numeric/measurement values
9 Fetal Trace Recorder - status indicator
Date and time
Fetal recorder is On
Fetal recorder is Off (when Paper Save Mode is off )
Fetal recorder is Off (when Paper Save Mode is on)
There is a Recorder problem that can be solved by the user (for example, paper out, paper jam,
wrong paper scale set)
Fetal recorder is defective: call service.
10 Avalon CTS System - status indicator:
Avalon CTS interface cable is connected to the monitor, but Avalon CTS base station is not
connected to the interface cable, disconnected from AC mains, or is in Standby.
Avalon CTS interface cable is connected to the monitor, Avalon CTS base station is connected,
powered on, and cordless transducers are ready to use, but no cordless transducers are currently
active (all are still docked in the base station).
Avalon CTS interface cable is connected to the monitor, Avalon CTS base station is connected,
powered on, and at least one cordless transducer has been taken out of the base station and is
active. Any connected wired transducers are disabled.
11 Close all open menus and windows and return to main screen
12 Battery Status Indicator
28
13 Scroll to display more SmartKeys
14 SmartKeys - these can vary according to your monitor's configuration
15 Silence - key which acknowledges all active alarms by switching off audible alarm indicators
Page 29
Keys
3 Basic Operation
Status line - shows status and prompt messages
16
17 Signal quality indicator
Good / full acceptable / medium Poor / no signal
18 Measurement label (a cordless measurement from a connected Avalon CTS system is indicated by
the symbol)
19 NST timer, if configured (default is Off)
The monitor has three different types of keys.
Permanent Keys
A permanent key is a graphical key that remains permanently on the screen, giving you fast access to
functions.
Silence - acknowledges all active alarms by switching off audible alarm indicators.
Main Screen - closes all open menus and windows and returns to the main screen.
29
Page 30
3 Basic Operation
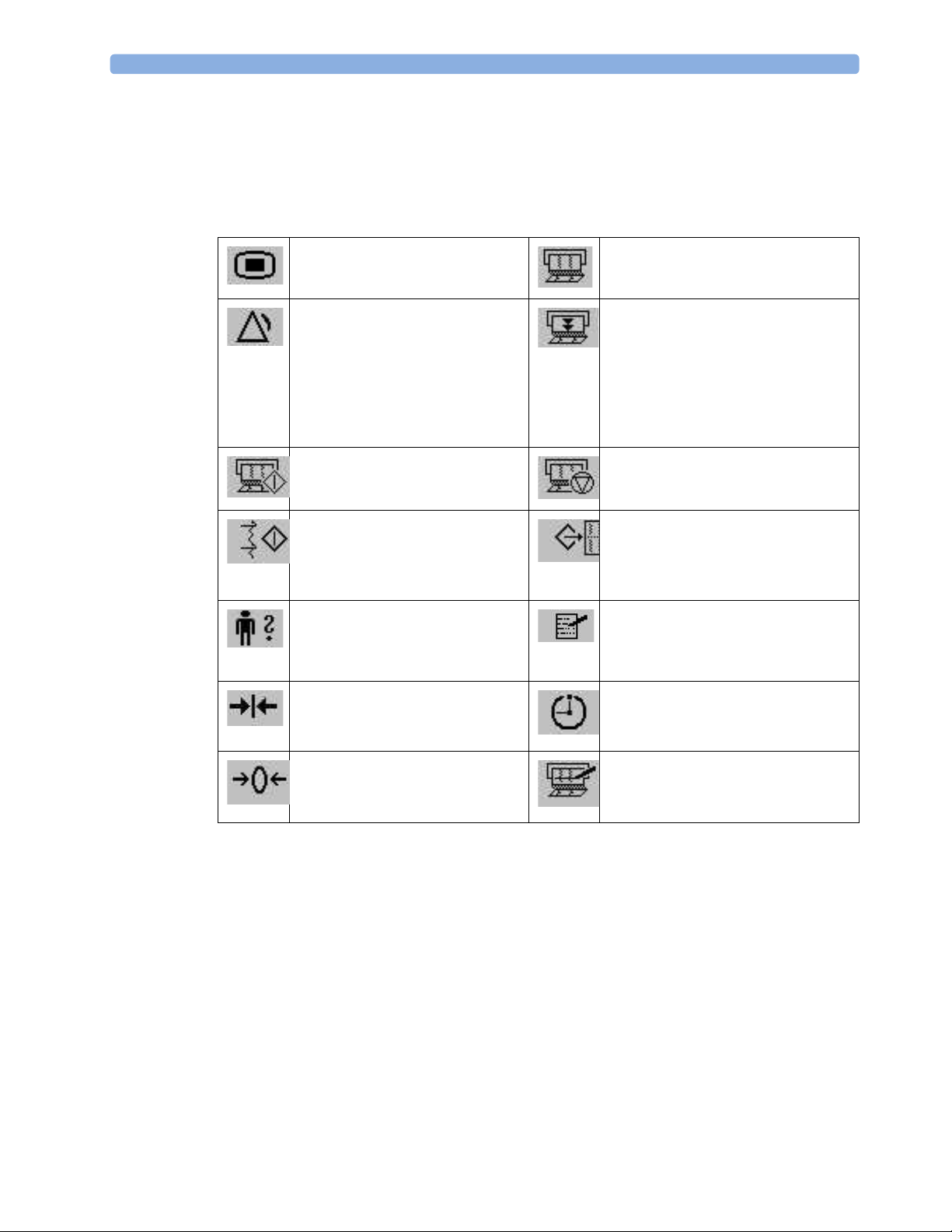
SmartKeys
SmartKeys are configurable graphical keys, located at the bottom of the main screen. They give you
fast access to functions. The selection of SmartKeys available on your monitor depends on your
monitor configuration and on the options purchased.
Main Setup - enter main setup
menu.
Pause Alarms - pauses alarm
indicators. Pause duration depends
on monitor configuration. If pause
duration is infinite, this key is
labeled
Alarms Off.
Select again to immediately reenable alarm indicators.
Start Recordng - turn the trace
recorder on.
Start ECG- start printing the
MECG, DECG or both waves,
when both are available.
Admit/ Dischrge - enter patient
identification menu to admit/
discharge
Toco Baseline - reset Toco
baseline/whichever is available
(see below)
Recorder Start/ Stop - turn the trace
recorder on or off.
Paper Advance - advance the paper
automatically to the next fold.
Stop Recordng - turn the trace
recorder off.
Stored Data Rec - print trace data
from the monitor's memory.
Enter Notes - enter notes
Timer - enters NST timer window
30
Zero IUP - zero IUP
measurement/whichever is
available (see above)
Set Marker - mark an event
Page 31

3 Basic Operation
Start/ Stop:
- start/stop manual noninvasive
blood pressure measurement
- start auto series
- stop current automatic
measurement within series
Start NBP:
- start manual noninvasive blood
pressure measurement
- start auto series
Repeat Time - set the time interval
between two noninvasive blood
pressure measurements
Sound Vol. Up - increases the
Fetal Heart Rate volume
Monitor Standby - enter Standby
mode, suspends monitoring. All
numerics and waves disappear
from the display. All settings and
patient data information are
retained.
Stop All - stop all noninvasive blood
pressure measurements
Stop NBP:
- stop manual noninvasive blood
pressure measurement
- stop current automatic measurement
within series
Defaults - load User Default
Sound Vol. Down - decreases the
Fetal Heart Rate volume
NST Report - initiate an NST trace
interpretation and obtain a NonStress Test (NST) Report
Pop-Up Keys
Pop-up keys are context-sensitive graphical keys that appear automatically on the monitor screen when
required. For example, the
Confirm pop-up key appears when you need to confirm a change.
Using the Touchscreen
Select screen elements by pressing them directly on the monitor's screen.
Disabling Touchscreen Operation
To temporarily disable touchscreen operation of the monitor, press and hold the Main Screen
permanent key for about three seconds. A red padlock will blink on the
Press and hold the
touchscreen operation.
Main Screen permanent key again for about three seconds to re-enable the
Main Screen permanent key.
31
Page 32

3 Basic Operation
Selecting Screen Elements
Select a screen element to tell the monitor to carry out the actions linked to the element.
You access most screen elements by touching that element directly. For example, select the FHR1
numeric to call up the
trace recorder.
However, some smaller screen elements are grouped together at the top of the screen in the
information area. To access one of these elements, touch anywhere in the information area, and select
the element from the selection list that appears. For example, to view alarm messages:
1 Touch the alarm status field, or anywhere else in the information area at the top of the screen. The
window with the selection list opens.
2 Select Alarm Messages from the list. This opens the Alarm Messages window, from where you
proceed to view the alarm messages.
Setup FHR1 menu, or select the Start/ Stop SmartKey to start or stop the fetal
Operating Modes
When you switch the monitor on, it starts up in monitoring mode. To change to a different mode:
1 Select the Main Setup menu.
2 Select Operating Modes and choose the mode you require.
Your monitor has four operating modes. Some are passcode protected.
• Monitoring Mode: This is the normal mode for monitoring patients. You can change elements
such as alarm limits, and so forth. When you discharge the patient, these elements return to their
default values. Changes can be stored permanently in Configuration Mode. You may see items,
such as some menu options, that are visible but "grayed out" so that you can neither select nor
change them. These are for your information and can be changed in Configuration Mode.
• Demo Mode: Passcode protected, this is for demonstration and training purposes. You must not
change into Demonstration Mode during monitoring. When transducers are connected to the
monitor and the recorder is on, a demo trace is recorded, but this is not transmitted to an
information and surveillance system such as OB TraceVue.
• Configuration Mode: Passcode protected, this is for personnel trained in configuration tasks.
These tasks are described in the Service Guide. During installation the monitor is configured for use
in your environment. This configuration defines the default settings you work with when you
switch on.
• Service Mode: Passcode protected, this is for trained service personnel.
When the monitor is in Demonstration Mode, Configuration Mode, or Service Mode, this is indicated
by a box containing the mode name. Select this field to change to a different mode.
32
Page 33

Automatic Screen Layouts
Your monitor's preconfigured screen layouts define how measurement information is arranged on
screen. The monitor automatically applies the correct screen layout for the measurements you are
monitoring. No user action is required.
Connecting or disconnecting transducers, or switching the noninvasive blood pressure measurement
on or off, results in an automatic adjustment of the screen layout. When a measurement is off, its
numerics are removed from the monitor's screen. The monitor stops acquiring data and generating
alarms for this measurement. If you disconnect a transducer while it is performing a measurement, the
monitor issues a disconnect INOP (and in the case of SpO
question marks).
Settings
This section describes the various settings available on the monitor.
Active Settings
What the monitor displays, and the way it operates, is controlled by its settings. They determine screen
content, layout, high and low alarm limits and so forth.
3 Basic Operation
, replaces the measurement numeric with
2
The "active settings" are the current settings the monitor uses, including any adjustments made by the
last user. Active settings are not permanent, but are retained after a loss of mains power.
There are also two preconfigured default settings:
•User Default
•Factory Default
User Default
The User Default is a complete configuration stored in the monitor's long-term memory. You can
change individual settings and store them in the User Default. In other words, you can store the active
settings, modified to your preference, in the User Default (in configuration mode).
In monitoring mode, you can load the User Default settings to return to your preferred settings:
1 Select the Defaults SmartKey .
2 Select Confirm in the dialog box to load the User Default.
To reload the user default settings select Confirm Confirm Cancel
Factory Default
The Factory Default is a complete configuration pre-defined at the factory. You cannot modify it. In
configuration mode, you can load the Factory Default as the active settings.
33
Page 34

3 Basic Operation
CAUTION
This resets all settings to factory defined values, but be aware that some values will differ from those
with which the monitor was originally shipped from the factory (recorder speed and paper scale type
will need to be corrected, for instance). After loading the Factory Default, please check the settings
and, if necessary, change them to the settings you normally use.
You can use the Factory Default as the basis for producing your User Default. See the Service Guide for
details.
Global Settings
General monitor configuration settings are stored in the Global Settings. These include settings for line
frequency, QRS type and whether the monitor is automatically reset to the User Default after a power
interruption of more than one minute. You can change the Global Settings in Configuration Mode.
Changing Measurement Settings
Each measurement has a setup menu in which you can adjust all of its settings. You can enter a setup
menu:
• via the measurement numeric - select the measurement numeric on the screen to enter its setup
menu. For example, to enter the
•via the
This guide always describes the entry method using the measurement's setup menu. You can use the
method you prefer.
Main Setup SmartKey - if you want to setup a measurement when the measurement is
switched off, use the
measurement name from the pop-up list. With this SmartKey you can access any setup menu in
the monitor.
Main Setup SmartKey and select Measurements. Then select the
Setup FHR1 menu, select the FHR1 (fetal heart rate 1) numeric.
Switching the Noninvasive Blood Pressure Measurement On and Off
The noninvasive blood pressure measurement is the only measurement for which you can manually
switch on and off. To do this:
1 Enter the noninvasive blood pressure measurement's setup menu.
2 Select NBP to toggle between on and off. The screen display indicates the active setting.
Changing Monitor Settings
To change monitor settings such as brightness, or touch tone volume:
1 Enter the Main Setup menu by selecting the SmartKey .
34
2 Select the setting you want to change, or select User Interface to enter a submenu where you can
change user interface settings.
Page 35

Adjusting the Screen Brightness
1 Enter the Main Setup menu by selecting the SmartKey .
2 Select User Interface.
3 Select Brightness.
4 Select the appropriate setting for the screen brightness. 10 is the brightest, 1 is the least bright.
Optimum is suitable for most situations.
Adjusting Touch Tone Volume
The touch tone volume is the tone you hear when you select any field on the monitor screen. To adjust
the touch tone volume,
1 Enter the Main Setup menu by selecting the SmartKey .
2 Select User Interface.
3 Select Touch ToneVolume, then select the appropriate setting for the touch tone volume: 10 is the
loudest and 1 is the quietest. Selecting zero switches the touch tone volume off.
3 Basic Operation
Setting the Date and Time
1 Select the date and time screen element from the monitor's info line to enter the Date, Time
menu.
2 Select, in turn, the Year, Month, Day, Hour (in 24 hour format) and Minute, as necessary.
3 Select Store Date, Time to change the date and time.
If connected to a Philips OB TraceVue system, the monitor uses the OB TraceVue system date and
time, including daylight saving time changes.
WARNING
Changing the date and time while the monitor is connected to an OB TraceVue system can result in a
mismatch in the time and date between the monitor and the OB TraceVue system.
When disconnected from AC power, the monitor retains the date and time setting for at least two
months.
Checking Your Monitor Revision
1 Select Main Setup -> Revisions to open the Monitor Revision menu.
2 From the Monitor Revision menu, select the monitor component for which you need revision
information.
Preparing to Monitor
Confirm fetal life before you begin fetal monitoring. Familiarize yourself with the basic operation
principles before you start to monitor.
35
Page 36

3 Basic Operation
Switching On: FM20/FM30
FM20/30 • Connect the monitor to AC mains and switch the monitor on.
• The green power-on LED comes on.
• The monitor performs a self-test as it starts up.
Selftest: OK, the serial number, and revisions for
the software and firmware are printed on the fetal trace paper (if recorder
On).
to
• The monitor display comes on.
• There is a start-up tone from the loudspeaker.
FM20/30
(with
Battery
Option)
• If this option has been chosen, the green power-on LED on both the External Power Supply and
the Battery LED indicator will come on.
Switching On: FM40/FM50
FM40/50 • Connect the monitor to AC mains. The green LED comes on.
• Press the On/Standby switch.
• The monitor performs a self-test as it starts up.
the software and firmware are printed on the fetal trace paper (if recorder
to
On).
• The monitor display comes on.
• There is a start-up tone from the loudspeaker.
Selftest: OK, the serial number, and revisions for
Auto Start is configured
Auto Start is configured
Adjusting the Display Angle (FM20/FM30)
FM20/30 You can tilt the display on the FM20 and FM30 to one of five different positions, or you can fold it
completely down. The tilt/fold mechanism works on a one-way ratchet system. You hear a click as
each of the five positions is reached. The screen can be folded back down only after tilting the display
forwards as far as it will go.
To tilt the display from the folded position:
1 Unlock the display by releasing the catch.
36
Page 37

3 Basic Operation
Lift the display forwards. You hear a click as the first position engages. If you want to tilt the
2
display further, lift the display further forwards until you reach the desired angle.
To fold the display:
1 Pull the display forwards as far as it will go.
2 Then push it all the way back until it clicks shut.
If your monitor is wall-mounted, the display should be folded flat.
37
Page 38

3 Basic Operation
Fastening Belts and Transducers
You can use more than one belt if, for example, you are monitoring uterine activity and FHR
simultaneously. There are two basic ways to fasten belts and transducers:
• Belts with button fixings.
• Velcro belts together with the butterfly belt clip.
Using Belts with Button Fixings
1 Place the transducer belt across the bed, ensuring that the fixing button will face away from the
mother when it is fastened.
2 Lie the patient on the bed and arrange the belt around her until it is tight but still comfortable.
3 Fasten the belt by pushing the fixing button through the overlapping section of the belt. Ensure
that the fixing button and the loose ends of the belt are at the patient's side.
4 When you have positioned a transducer satisfactorily, you can attach it to the belt by pushing the
belt button on the transducer through one of the holes in the belt.
Alternatively, attach the butterfly belt clip to the transducer belt button and use this to attach the
transducer to the belt. The clip allows you to slide the transducer for easy repositioning.
38
Page 39

Using Belt with Velcro Fixings
Insert one end of the belt between the belt guides on one side of the butterfly belt clip, and secure with
the velcro fixing. Insert the other end of the belt between the belt guides on the other side of the
butterfly belt clip, adjust for the correct tension, then secure with the velcro fixing.
3 Basic Operation
1 Fasten one end with velcro fixing
2 Belt guides
3 Pull the other end through, adjust for tension, and secure with velcro fixing
WARNING
When connecting devices for acquiring measurements, always position cables and NBP tubing
carefully to avoid entanglement or potential strangulation.
39
Page 40

3 Basic Operation
Connecting a Transducer to the Monitor
1 SpO
socket
2
2 Noninvasive blood pressure
socket
3 Fetal sensor sockets
You can plug a fetal transducer, a ECG/IUP patient module, an Avalon CTS Cordless Fetal
Transducer System interface cable (M2731-60001, red connector), or an external event marker into any
of the four fetal sensor sockets marked or "Fetal Sensors" (depending on geography). For
measuring maternal SpO
, connect the sensor to the socket marked or "SpO2" (depending on
2
geography), and for maternal non-invasive blood pressure, connect the cuff to the socket marked
or "NBP" (depending on geography).
40
For the FM40 and FM50, you can connect an Avalon CTS Cordless Fetal Transducer System interface
cable (M2732-60001, black connector) to one of the two dedicated black sockets marked "Tele" at the
rear of the monitor, as an alternative to using one of the fetal sensor sockets at the front.
1 M2732-60001 interface cable to
Avalon CTS Cordless Fetal
Transducer System.
2 Connect the black connector to
one of the two black sockets
(marked "Tele") on the rear of
the monitor.
Page 41

3 Basic Operation
When you connect a transducer or sensor:
• The appropriate measurement is shown on the display. For fetal measurements using an Avalon
CTS system, the symbol appears additionally next to the measurement label, indicating that
the measurement is being made by a cordless transducer.
1 Measurement label
2 Cordless measurement symbol
• Fetal heart rate measurements are labeled in the order in which you plug in the transducers for
those measurements. It does not matter which fetal sensor socket you use, as the monitor allocates
a channel automatically. For instance, when monitoring triplets, the first transducer you connect is
automatically allocated a channel, and the measurement is labeled
third
FHR3. See also chapters “Monitoring Twin FHRs” on page 113 and “Monitoring Triple
FHR1, the second FHR2, and the
FHRs” on page 121.
• When you touch a measurement numeric on the screen, the setup menu for that measurement
opens. The fetal sensor socket to which the transducer for this measurement is connected is
identified by the transducer position indicator in the blue setup menu header:
for FM20/30;
for FM40/50.
• The blue Finder LED on a wired fetal transducer illuminates when you touch the measurement on
the screen, allowing you to identify the corresponding transducer.
1 Finder LED
41
Page 42

3 Basic Operation
• The recorder prints an annotation showing the date, time, paper speed, and monitoring mode. It
repeats this every 10 minutes.
Checking/Setting Paper Scale
You can check the paper Scale Type (US for USA, or Internat'l for other geographies) in the Fetal
Recorder
them. They can be changed in Configuration Mode.
1 Enter the Main Setup menu by selecting the SmartKey .
2 Select Fetal Recorder.
3 Check the current setting for Scale Type. If it is not appropriate, change it in the Fetal Recorder
menu. In Monitoring Mode, you can see these settings (grayed out), but you cannot change
menu in Configuration Mode:
Scale Type to toggle between US and Internat'l.
Select
Paper Guide: FM40/FM50
FM40/50 The recorder in the FM40 and FM50 features a transparent paper guide which:
• facilitates correct alignment of the paper, both during loading and while the recorder is running.
See “Loading Paper: FM40/FM50” on page 45.
• incorporates a tear-off edge, which not only allows you to tear off the trace paper where you like
(not necessarily at a fold), but also helps to avoid paper misalignment while doing so (see “Tearing
Off the Paper: FM40/FM50” on page 48).
• is removable (see “Removing the Paper Guide: FM40/FM50” on page 42).
Removing the Paper Guide: FM40/FM50
FM40/50 The paper guide is removable, and you can use the recorder without it. When not using the paper
guide, ALWAYS tear off the paper along the perforation to avoid possible paper misalignment (see
“Tearing Off the Paper: FM40/FM50” on page 48).
To remove the paper guide:
1 Press the paper eject button to open the paper drawer.
42
2 Hinge the transparent paper guide forward.
Page 43

A - Protrusion holds paper guide in closed position
3 Release the paper guide from one side of the holder...
3 Basic Operation
4 ....then remove the paper guide.
43
Page 44

3 Basic Operation
Refitting is a reversal of the removal procedure.
Loading Paper: FM20/FM30
CAUTION
Using recorder paper that is not approved by Philips can result in accelerated paper fading and can
damage the thermal line printhead. This type of damage is not covered by warranty.
FM20/30 To load a pack of paper:
1 If the recorder is on, press the recorder Start/ Stop SmartKey or the Stop Recordng
SmartKey to turn it off before loading a new pack of paper.
2 Press the paper table release to unlock the paper drawer and then pull the table forward to open it
fully.
44
3 Lift out any remaining paper from the tray.
4 Prepare to place the new pack of paper in the tray with the bottom side down. The bottom side is
indicated by the word STOP printed on the final page of the new pack.
5 Unfold the top page of the pack and position the uterine activity scale on the right.
6 Slide the pack into the tray.
7 Push the paper drawer back until it "clicks" closed.
Page 45

8
Press the recorder Start/ Stop SmartKey or the Start Recordng SmartKey to switch on
the recorder.
9 Annotations of trace information are printed on the trace paper (see “Switching the Recorder On
and Off ” on page 49 for details).
Loading Paper: FM40/FM50
3 Basic Operation
CAUTION
Using recorder paper that is not approved by Philips can result in accelerated paper fading and can
damage the thermal line printhead. This type of damage is not covered by warranty.
FM40/50 To load a pack of paper:
1 If the recorder is on, press the recorder Start/ Stop SmartKey or the Stop Recordng
SmartKey to turn it off before loading a new pack of paper.
2 Press the paper eject button to open the paper drawer.
3 Lift out any remaining paper from the tray. Press and hold the paper eject button to partially eject
the paper, thus making it easier to remove.
4 Hinge the transparent paper guide forward. It is held in the closed position by a small protrusion
on each side of the holder.
45
Page 46

3 Basic Operation
5 Prepare to place the new pack of paper in the tray with the bottom side down. The bottom side is
6 Unfold the top page of the pack and position the uterine activity scale on the right.
7 Slide the pack into the tray.
A - Protrusion holds paper guide in closed position
indicated by the word STOP printed on the final page of the new pack.
46
8 Feed the paper evenly through the paper guide. Do not close the paper guide yet.
9 Close the paper drawer.
Page 47

10
Now close the paper guide.
3 Basic Operation
11 Press the recorder Start/ Stop SmartKey or the Start Recordng SmartKey to switch on
the recorder.
12 Annotations of trace information are printed on the trace paper (see “Switching the Recorder On
and Off ” on page 49 for details).
Paper-Out Indication
Each pack of paper has 150 pages. The monitor issues a paper-out warning in the status line at the
bottom of the screen, when there are five pages to go. If you switch on the recorder or press the paper
advance key when there are fewer than five pages remaining, it may take two pages before the alert is
activated. Load a new pack in time.
If the recorder runs out of paper, an audible paper-out alert is sounded, if so configured.
Fetal traces continue to be recorded into the monitor's backup memory, and can be retrieved and
printed completely if new paper is loaded within one hour, when the
enabled in Configuration Mode. See “Recovering Traces on Paper” on page 167 for further
information.
Bridge Paperout setting is
47
Page 48

3 Basic Operation
Choosing Paper Speed
You can choose a paper speed of 1, 2, or 3 centimeters per minute (cm/min). The default setting is 3
cm/min.
The ACOG technical bulletin on FHR monitoring states that "accurate pattern recognition is difficult if not
impossible at 1 cm/min and that 1 cm/min is only recommended for more economic screening. When FHR
abnormalities arise, the faster paper speeds will enhance FHR pattern recognition".
Additionally, because a change in paper speed results in a change in the appearance of an FHR trace,
you are advised to ensure ALL monitors in your institution are set to the same speed.
To set the paper speed (in Configuration Mode):
1 Enter the Main Setup menu using the SmartKey .
2 Select Fetal Recorder.
3 In the Fetal Recorder menu, you can see the current speed setting. Select Recorder Speed (only
visible in monitoring mode).
4 Select the desired speed from the given choices: 1, 2 or 3 cm/min.
Tearing Off the Paper: FM20/FM30
CAUTION
NEVER pull on the paper to advance it, as this can cause misalignment of the paper. ALWAYS tear
off the paper along the perforation.
To tear off the trace paper after monitoring:
1 If the recorder is running (the "recorder on" status indicator is displayed), turn off the
recorder by selecting the fetal recorder Start/ Stop SmartKey or the Stop Recordng
SmartKey.
2 Select the Paper Advance SmartKey . This advances the paper automatically to the next
perforation.
3 When the paper stops advancing, tear off the trace paper along the perforation.
Tearing Off the Paper: FM40/FM50
CAUTION
NEVER pull on the paper to advance it, as this can cause misalignment of the paper.
48
The recorder's paper guide incorporates a tear-off edge, allowing you to tear off the trace paper cleanly
where you like (not necessarily at a fold). When not using the paper guide, ALWAYS tear off the paper
along the perforation.
Page 49

Using the Paper Guide
To tear off the trace paper after monitoring using the paper guide:
1 If the recorder is running (the "recorder on" status indicator is displayed), turn off the
recorder by selecting the fetal recorder Start/ Stop SmartKey or the Stop Recordng
SmartKey.
2 Tear off the paper as shown in the pictures. To ensure a clean tear, always tear in an upwards
motion, as indicated by the arrows. You can start tearing from the left or right (right-handed user
shown).
3 Basic Operation
If you wish to tear off the paper at a fold, select the
the paper to stop, then tear off.
Without the Paper Guide
To tear off the trace paper after monitoring without using the paper guide:
1 If the recorder is running (the "recorder on" status indicator is displayed), turn off the
recorder by selecting the fetal recorder Start/ Stop SmartKey or the Stop Recordng
SmartKey.
2 Select the Paper Advance SmartKey . This advances the paper automatically to the next
perforation.
3 When the paper stops advancing, tear off the trace paper along the perforation.
Switching the Recorder On and Off
Note that in addition to the normal recording of real-time traces, you will sometimes see a trace
recovery printout from the monitor's internal backup memory at high speed when the recorder is
started. For details, see “Recovering Traces on Paper” on page 167.
Paper Advance SmartKey , wait for
For an explanation of the various symbols that can appear on the trace recording, see “Recorder
Specifications” on page 201.
To switch the recorder on, select
SmartKeys: fetal recorder Start/ Stop or Start Recordng .
Start/Stop from the Fetal Recorder menu, or press one of the
49
Page 50

3 Basic Operation
When you switch on:
• The "recorder on" status indicator is displayed in the bottom right-hand corner of the
• The paper advances quickly for 2 cm and then returns to the set speed.
• Whenever the recorder is switched on, a trace header is printed vertically on the trace paper,
screen.
containing the following:
Selftest: OK: confirmation that the monitor's self-test completed successfully, and that it is
–
ready to use.
– the software revision and firmware revision
–the serial number
–the time
–the date
– patient name and medical record number (if entered)
– the paper speed
1 Fetal heart rate label
2 Uterine activity label
50
• The current monitoring modes (if any transducers are connected to the monitor) are printed.
• Whenever a transducer's mode is changed the following are printed:
–the time
–the date
– trace identification symbols
– the paper speed
Page 51

3 Basic Operation
The monitor prints the time, date, paper speed and monitoring modes in the trace header when first
switched on, in a periodic time stamp every ten minutes after, and if the monitoring modes change.
The time stamp begins with the symbol.
1 Time stamp printed every ten
minutes
Maternal parameters are also annotated on the trace. In the case of noninvasive blood pressure, the
annotation is made at the end of the measurement. If the noninvasive blood pressure measurement
repetition time is short, the noninvasive blood pressure numeric may not always be printed.
The recording of notes (see “Entering Notes” on page 52) or time/date information may be
interrupted by connecting or unplugging a transducer or by a change in measurement-related setting
(for example, artifact suppression, Toco sensitivity, or alarm settings).
A new patient admission or a change to the paper scale setting stops all annotations, and prompts a
new vertical trace header to be printed.
To switch the recorder off:
• Either select
• Or press one of the SmartKeys (depending on configuration): fetal recorder Start/ Stop
or
Stop Recordng .
If your recorder is configured with
to confirm that you want to stop the recorder, before it will stop.
When the recorder is off, the "recorder off" status indicator is displayed in the bottom right-hand
corner of the screen: when Paper Save Mode is off, and when Paper Save Mode is on.
Start/Stop from the Fetal Recorder menu.
Advancing the Paper
You can advance the paper automatically to the next fold by pressing the Paper Advance SmartKey
at any time except during a stored data recording. This is also possible using the
Recorder
menu.
Confirmed Stop On (a Configuration Mode setting), you will need
Fetal
Marking an Event
You can record significant events on the trace paper (for example, when pain medication is
administered or when the mother changes position). The mother can use the remote event marker to
mark events herself. You connect the remote event marker to any free fetal sensor socket.
51
Page 52

3 Basic Operation
To mark an event on the trace paper you can:
• Either select the Set Marker SmartKey .
• Or press the button on the remote event marker. The remote event marker is connected to the
A small arrow is printed on the heart rate scale on the trace paper. This reflects exactly when the
marker button was first pressed; keeping the button pressed has no influence on the annotation.
monitor via any fetal transducer socket.
Entering Notes
Your monitor has a set of 15 factory pre-configured notes (see below). The maximum length of one
single note is 30 characters. It is possible to edit the notes in Configuration Mode (please refer to the
Service Guide).
To enter a note:
♦ Press the Enter Notes SmartKey to open the Enter Note menu.
♦ Scroll if necessary, then select the note you wish to enter. A confirmation dialog box opens:
To store and record the note select Confirm. Select
Cancel to reject the current note.
♦ Select Confirm to enter the note. The note is then shown in the status line of the display, and is
annotated on the fetal trace if the fetal recorder is on.
By default, notes are printed lengthwise in the direction of the trace, in the space between the FHR
grid and the uterine activity grid. If you prefer, you can configure the recorder to print across the trace.
You can change this in Configuration Mode by changing the
Recorder
The following are the pre-configured notes from which to choose:
1 Patient Repositioned
Confirm Cancel
Notes Recording setting in the Fetal
menu from Along (default) to Across (notes print widthwise across the trace).
52
2 Vaginal Examination
Page 53

3 Basic Operation
MD Notified
3
4 Sitting
5 On Back
6 Left Lateral
7 Ambulating
8 Tocolytic Given
9 Membranes Ruptured
10 Amniotomy
11 Amniotic Fluid Clear
12 Amniotic Fluid Not Clear
13 Oxytocin
14 Urinary Catheter
15 Micro Blood Analysis
Up to two notes can be printed directly, and the monitor can temporarily store up to a further two
notes, and these are printed after the first two have been recorded. Any further notes are discarded.
For example, if you enter six notes in quick succession, the first two notes you entered are recorded
right away, the next two are stored in memory and then printed when the first two have been recorded,
and the last two are discarded.
If the printing of two notes happens to coincide with the regular recording of the time stamp that takes
place once every ten minutes, the time stamp is delayed until the notes have finished printing.
Signal Quality
During monitoring, if the fetal heart rate signal quality fluctuates, and becomes poor, it does not
necessarily mean that the transducer needs repositioning. The fluctuation may be caused by fetal
movement. Allow time for the signal to stabilize before deciding whether to reposition the transducer
(ultrasound) or apply a new electrode (ECG). For the best trace quality, the signal quality indicator
should be full, indicating good signal quality, even though it may be possible to make traces at a lower
signal quality level.
Starting Monitoring
Confirm fetal life before you begin fetal monitoring.
After you switch on the monitor:
1 Check that you have the correct patient cables and transducers plugged in for the measurement
you want to monitor.
2 Admit your patient to the monitor (see “Admitting a Patient” on page 83).
3 Check that the alarm limits, alarm and fetal heart rate volumes, patient category and so forth are
appropriate for your patient. Change them if necessary.
4 Refer to the appropriate measurement section for details of how to perform the measurements
you require.
53
Page 54

3 Basic Operation
Switching the Monitor to Standby
To switch the monitor to Standby:
Either
Select the
Or
1 Enter the Main Setup menu using the SmartKey .
2 Select Monitor Standby.
Pressing any key or selecting any field on the screen will resume monitoring.
Monitor Standby SmartKey .
After Monitoring
1 Discharge the patient.
2 Remove the transducer from the patient and, using a soft tissue, remove any gel from it. Then
clean the transducer.
3 Tear off the paper at the fold. To avoid misalignment of the recorder mechanism, NEVER pull on
the paper to advance it, or try to tear it other than at a fold (unless using the paper guide with the
FM40/FM50).
4 Switch off the monitor.
Disconnecting from Power
FM20/30 To disconnect the monitor from AC power, switch the monitor off using the On/Off switch located
on the right side of the device, or unplug the power cord from the AC mains socket.
FM20/30
(with
Battery
Option)
FM40/50
and FM20/
30 with
Battery
Option
54
To disconnect from Battery power, switch the monitor off using the On/Standby switch located on
the right side of the device.
The On/Standby switch does not disconnect the monitor from the AC power source. To disconnect,
unplug the power cord from the AC mains socket. Note that if the power cord is unplugged from the
AC mains socket before the monitor is put into Standby, a beeper is activated. The beeper warns you if
the monitor is accidentally disconnected from AC mains.
Page 55

3 Basic Operation
Troubleshooting
Problem Possible Causes Solutions
Light or no trace. Wrong paper. Use recommended paper.
Dirty printhead. Clean printhead. See “Cleaning the
Printhead” on page 177.
FM20/30 only: Paper misaligned due to
drawer not being correctly shut.
End of paper noted when
pack not finished.
CHECK PAPER INOP is displayed. See “Patient Alarms and INOPs” on
FetRec EQUIP MALF INOP is displayed.
PAPER END INOP is displayed.
WRONG PAPER SCALE INOP is displayed.
Bad paper feed or wrong paper. Check paper feed and use recommended
Shut the drawer fully, pushing evenly with
both hands.
paper.
page 73.
55
Page 56

3 Basic Operation
56
Page 57

4Using Batteries (with FM20/30
Battery Option)
You can switch between battery-powered and mains-powered (AC) operation without interrupting
monitoring.
The monitor is connected to the AC mains power via the external power supply.
4
NOTE
The Battery Option is not available for the FM40/FM50.
57
Page 58

4 Using Batteries (with FM20/30 Battery Option)
External Power Supply M8023A
The external power supply M8023A (option #E25) allows you to operate the fetal monitor from an
AC (alternating current) power source of 100 V to 240 V (± 10%) and 50/60 Hz (± 5%). If this option
is used, then the M8023A (option #E25) power supply is included for FM20/30.
WARNING
• Always use the supplied power cord with the earthed mains plug to connect the external power
supply M8023A (option #E25) to an earthed AC mains socket. Never adapt the mains plug from
the power supply to fit an unearthed AC mains socket.
1 AC power cord. Connect to AC
mains socket.
2 Measurement Link (MSL) cable.
Supplies power to the monitor
for operation and for battery
charging.
3 Power-on LED. The green light
is on when the external power
supply is connected to AC
mains.
• Do not use AC mains extension cords or multiple portable socket-outlets. If a multiple portable
socket-outlet without an approved isolation transformer is used, the interruption of its protective
earthing may result in enclosure leakage currents equal to the sum of the individual earth leakage
currents, so exceeding allowable limits.
• Do not connect any devices that are not supported as part of a system.
• Any non-medical device placed and operated in the patient’s vicinity must be powered via an
approved isolation transformer that ensures mechanical fixing of the power cords and covering of
any unused power outlets.
Battery Power Indicators
The battery LED and battery status information on the Main Screen, in combination with INOP
messages and prompts, help you keep track of the battery power status. The indicators always show
the remaining capacity in relation to the battery's actual maximum capacity, which may lessen as the
battery ages. You can see the actual capacity in the
Battery LED
The battery LED on the right side of the monitor is indicated below.
Battery Status window.
58
Page 59

4 Using Batteries (with FM20/30 Battery Option)
Battery LED Colors If the monitor is connected to
mains power, this means
Green
Yellow
Red, flashing
Red, flashes intermittently
battery power is > 90%
battery charging (battery power
< 90%)
battery or charger malfunction battery malfunction
Battery Status on the Main Screen
Battery status information is permanently displayed on all screens. It shows the status of the battery,
with the battery power remaining, with an estimate of the monitoring time this represents.
Battery power gauge: This shows the remaining battery power. It is divided into sections, each
representing 20% of the total power. If three sections are filled, as in this example, this indicates that
60% battery power remains. If no data is available from the battery, a question mark is shown in the
gauge.
If the monitor is running on
battery power, this means
less than 10 minutes power
remaining
Monitoring Time Available: Below the battery power gauge a time is displayed. This is the estimated
monitoring time available with the current battery power. Note that this time fluctuates depending on
the system load (the display brightness, the recorder configuration, and how many measurements you
carry out).
Battery malfunction symbols: Normal battery function is indicated by the battery power gauge,
together with the remaining operating time, on the Main Screen. You are informed of problems or
changes in the status of the battery by the battery status/malfunction indicator. This consists of a blank
battery gauge containing a "!" symbol. If the symbol is red, this indicates a critical situation. You can
check the specific cause of the problem by looking at the symbol(s) displayed in the
window.
Battery Status
59
Page 60

4 Using Batteries (with FM20/30 Battery Option)
Battery Status Indicator Battery Malfunction Indicator
Alternates with the battery gauge on the
Main Screen.
Check in the Battery Status window
to see which status symbol is displayed to
identify the cause.
Checking Battery Charge
To check the charge status of a battery, refer to the battery power gauge on the screen or open the
Battery Status window.
When Battery Lifetime is Expired
When the Lithium Ion battery is aged, either after 3 years from manufacturing date or after 500
charge/discharge cycles, it is recommended to replace the battery. To remind you of this a Battery has
aged, replacement is strongly recommended message will appear in the
This message will only be displayed at the correct time when the date and time on the monitor is
correct. Contact your service personnel.
The red ! flashes. Critical battery
situation or malfunction. Check
in the Battery Statuswindow
to see which malfunction
indicator is displayed, or refer to
the INOP, to identify the cause.
Battery Status window.
Battery Status Window
♦ To access the Battery Status window and its associated pop-up keys, select the battery status
information on the Screen, or select
Capacity, remaining tells you how much power is left in the battery.
Capacity, fullCharge tells you how much power the battery can hold when fully charged.
TimeToEmpty tells you approximately how long you can continue to use the monitor without an AC
connection. Note that this time fluctuates depending on the system load (the display brightness and
how many measurements you carry out), and the remaining capacity of the battery.
TimeToFull is shown in place of TimeToEmpty if the monitor is connected to a power supply, and
tells you how much time is left until the battery is charged to 90%. If >10 hrs is shown here, the
battery may not charge completely when the monitor is in use.
Battery status/malfunction symbols: If a problem is detected with the battery, an INOP may be
issued, and the following symbols are displayed in the Battery Status window, where they may be
accompanied by a status message providing more details.
Symbols indicating critical situations are colored red.
Main Setup -> Battery.
60
Page 61

4 Using Batteries (with FM20/30 Battery Option)
Battery status symbols Battery malfunction symbols
battery is empty (red) incompatible battery
battery not charging as the temperature
is above or below the specified range
battery requires maintenance (red) battery has no power left
charging stopped to protect the battery (red) battery temperature too high
Optimizing Battery Performance
The performance of rechargeable batteries may deteriorate over time. Battery maintenance as
recommended here can help to slow down this process.
Display Brightness Setting
In the Main Setup menu, select User Interface, Brightness, then Optimum. This selects a level of
brightness suitable for most monitoring locations that uses less battery power than brighter settings.
(red) battery malfunction
(red) battery is missing, insert battery
Ensure that the current level of brightness is suitable for your monitoring location.
Charging the Battery
To charge the battery,
1 Connect the monitor to the external power supply (M8023A).
2 Charge the battery until it is full, the battery LED is green, and the battery power gauge is filled.
In certain situations, where many measurements are in use (plus the recorder), the load on the monitor
may be so high that the battery will not charge. In this case you must reduce the load by removing
measurements, reducing the screen brightness or stopping the recorder. Internal temperature
conditions could also cause the battery to not charge. This is necessary to protect the battery from
damage and does not indicate a malfunction. Keep the monitor at room temperature and move it away
from heat sources or out of direct sunlight. The battery will resume charging when the temperature is
within range again. Note that the battery will charge more quickly when the monitor is switched off.
Storing the Battery
The battery should not remain inside the monitor if it is not used for a longer period of time. Batteries
should be charged to a maximum of 50% for storage. For battery removal or exchange, contact your
service personnel.
61
Page 62

4 Using Batteries (with FM20/30 Battery Option)
NOTE
The battery will discharge over time in a monitor that is not connected to AC via the external power
supply (M8023A). The reported values for "remaining capacity" and "runtime" will become less
accurate when the battery is stored in this way for a longer period of time (that is, several weeks).
Conditioning the Battery
You must condition the battery when the "battery requires maintenance" symbol shows on the Screen.
Do not interrupt the charge or discharge cycle during conditioning.
CAUTION
Do not use a monitor currently being used in order to condition batteries. The monitor switches off
automatically when there is no battery power left.
To condition the battery,
1 Charge the battery until it is completely full. Open the Battery Status window and check that the
Batt Fully Charged message is displayed.
2 Disconnect the monitor from mains power, and let the monitor run until there is no battery power
left and the monitor switches itself off.
3 Reconnect the monitor to mains power and charge the battery until it is full for use or charge to
50% for storage.
Battery Safety Information
WARNING
Use only Philips batteries part number M4605A. Use of a different battery may present a risk of fire
or explosion.
Do not open batteries, or dispose of them in fire, or cause them to short circuit. They may ignite,
explode, leak or heat up, causing personal injury.
If battery leakage should occur, avoid contact with skin. Refer to qualified service personnel.
Dispose of used batteries promptly and in an environmentally-responsible manner. Do not dispose
of the battery in normal waste containers. Consult your hospital administrator to find out about local
arrangements.
CAUTION
Do not disassemble, heat above 100°C (212°F) or incinerate the batteries, to avoid the risk of fire and
burns. Keep batteries out of the reach of children and in their original package until you are ready to
use them.
62
If battery leakage should occur, use caution in removing the battery. Avoid contact with skin. Refer to
qualified service personnel.
Page 63

5Alarms
The alarm information here applies to all measurements. Measurement-specific alarm information is
contained in the sections on individual measurements.
The fetal monitor has three alarm levels: red, yellow, and INOP.
Red and yellow alarms are patient alarms. A red alarm indicates high priority, such as a potentially life
threatening situation (for example, SpO
a lower priority alarm (for example, a fetal heart rate alarm limit violation).
INOPs are technical alarms. They indicate that the monitor cannot measure and therefore not detect
critical conditions reliably. If an INOP interrupts monitoring and alarm detection (for example,
LEADS OFF
audible tone. INOPs without this tone indicate that there may be a problem with the reliability of the
data, but that monitoring is not interrupted.
5
below the desaturation alarm limit). A yellow alarm indicates
2
MECG
), the monitor places a question mark in place of the measurement numeric and sounds an
Alarms are indicated after the specified alarm delay time. This is made up of the system delay time plus
the trigger delay time for the individual measurement. See the Specifications section for details.
If more than one alarm is active, the alarm messages are shown in the alarm status area in succession.
An arrow symbol next to the alarm message informs you that more than one message is active.
The monitor sounds an audible indicator for the highest priority alarm. If more than one alarm
condition is active in the same measurement, the monitor announces the most severe.
WARNING
Alarm systems of the monitor and those of the connected OB system are independent and not
synchronized.
Alarm Mode
You can configure the alarm mode for your fetal monitor. There are two possible modes:
All: alarms and INOPs are enabled, with all audible and visual indicators active.
•
INOP Only only INOPs are enabled, with audible and visual indication active. This is the default
•
alarm mode.
63
Page 64

5 Alarms
WARNING
In INOP Only mode, no fetal/maternal patient alarms are enabled or indicated.
The alarm status area for yellow and red alarms shows the INOP only indication in conjunction with
the "Alarms Off" symbol. No alarm limits or alarm off icons are displayed. No fetal/maternal patient
alarm settings are available in the setup menus.
Visual Alarm Indicators
Alarm message: An alarm message appears in the alarm status area on the second line at the top of the
screen indicating the source of the alarm. If more than one measurement is in an alarm condition, the
message changes every two seconds, and has an arrow at the side. The background color of the alarm
message matches the alarm priority: red for red alarms, yellow for yellow alarms, and light blue for
INOPs. The asterisk symbols (*) beside the alarm message match the alarm priority: *** for red alarms,
** for yellow alarms. INOPs are displayed without asterisks.
Depending on how your monitor is configured, it may display alarm limit violation messages:
• in text form, for example
• in numeric form, for example
alarm limit, and the first number shows the value at which that alarm limit was violated by the
widest margin.
Flashing numeric: The numeric of the measurement in alarm flashes.
Bright alarm limits: If the alarm was triggered by an alarm limit violation, the corresponding alarm limit
on the monitor screen is shown more brightly.
** FHR1 LOW or
**FHR1 94<110, where the second number shows the currently set
Audible Alarm Indicators
The audible alarm indicators configured for your fetal monitor depend on which alarm standard
applies in your hospital. Audible alarm indicator patterns are repeated until you acknowledge the alarm
by switching it off or pausing it, or until the alarm condition ceases (if audible alarm indication is set to
non-latching).
WARNING
Do not rely exclusively on the audible alarm system for fetal monitoring. Adjustment of alarm volume
to a low level or off during monitoring may result in a dangerous situation. Remember that the most
reliable method of fetal monitoring combines close personal surveillance with correct operation of
monitoring equipment.
Alarm Tone Configuration
The audible alarm indicators of your monitor are configurable. In the monitor's Configuration Mode,
you can change the alarm sound to suit the different alarm standards valid in different countries.
Standard Philips Alarms
• Red alarms: A high pitched sound is repeated once a second.
64
Page 65

• Yellow alarms: A lower pitched sound is repeated every two seconds.
• INOPs: an INOP tone is repeated every two seconds.
ISO/IEC Standard 9703-2 Audible Alarms
• Red alarms: A high pitched tone is repeated five times, followed by a pause.
• Yellow alarms: A lower pitched tone is repeated three times, followed by a pause.
• INOPs: a lower pitched tone is repeated twice, followed by a pause.
Changing the Alarm Tone Volume
The alarm volume symbol at the top right of the monitor screen gives you an indication of the current
volume. To change the volume:
1 Select the volume symbol . The volume scale pops up.
2 Select the required volume from the volume scale.
5 Alarms
1 Alarm Volume
When the alarm volume is set to zero (
alarm volume off, you will not get any audible indication of alarm conditions.
Power Loss Tone
FM40/50
and FM20/
30 with
Battery
Option
When power is lost - no power is available from the AC power source or from the battery - before the
monitor is put into Standby, a beeper will sound. The tone can be silenced by pressing the On/Standby
switch.
Off), the alarm volume symbol shows this. If you switch the
65
Page 66

5 Alarms
Acknowledging Alarms
To acknowledge all active alarms and INOPs, select the Silence key . This switches off the
audible alarm indicators.
A check mark beside the alarm message indicates that the alarm has been acknowledged.
If the condition that triggered the alarm is still present after the alarm has been acknowledged, the
alarm message stays on the screen with a check mark symbol beside it.
If the alarm condition is no longer present, all alarm indicators stop and the alarm is reset.
Switching off the alarms for the measurement in alarm, or switching off the measurement itself, also
stops alarm indication.
Acknowledging Disconnect INOPs
Acknowledging an INOP that results from a disconnected transducer switches off the associated
measurement.
Pausing or Switching Off Alarms
If you want to temporarily prevent alarms from sounding, for example while you are moving a patient,
you can pause alarms. Depending on your fetal monitor configuration, alarms are paused for one, two,
or three minutes, or infinitely.
To view the alarm pause setting chosen for your unit:
1 Select Main Setup -> Alarms -> Alarm Settings.
2 Check the Alarms Off setting.
This setting can be changed in Configuration Mode.
To Pause All Alarms
If you have configured alarms to be paused for one, two or three minutes, the SmartKey is labeled
Pause Alarms.
Select the
Or
1 Select Main Setup.
2 SelectAlarms.
Pause Alarms SmartKey to pause all alarms.
3 Select Pause Alarms.
To Switch All Alarms Off
You can switch alarms off permanently if your monitor is configured to allow infinite alarms pause and
the SmartKey is labeled
66
Alarms Off.
Page 67

Select the Alarms Off SmartKey.
Or
1 Select Main Setup.
2 Select Alarms.
3 Select Alarms Off.
To Switch Individual Measurement Alarms On or Off
This applies to alarm mode All.
1 Select the measurement numeric to enter its setup menu.
2 Select Alarms to toggle between On and Off.
5 Alarms
The alarms off symbol is shown beside the measurement numeric.
While Alarms are Paused or Off
• In the alarm field, the monitor displays the message Alarms Paused or Alarms Off, together with
the alarms paused symbol and the remaining pause time in minutes and seconds, or
alarms off symbol .
• No alarms are sounded and no alarm messages are shown.
• INOP messages are shown but no INOP tones are sounded.
The following INOPs are the only exceptions:
NBP CUFF OVERPRESS, Batt EMPTY and Batt MALFUNCTION (these INOPs are issued even if alarms
are paused or off).
If a disconnect INOP is present and alarms are paused or switched off, the measurement in question is
switched off.
Restarting Paused Alarms
To manually switch on alarm indication again after a pause, select the SmartKey Pause Alarms (or
Alarms Off) again.
Alarm indication starts again automatically after the pause period expires. If the monitor is configured
to stay paused infinitely, you must select
Alarms Off again to restart alarm indication.
67
Page 68

5 Alarms
Alarm Limits
The alarm limits you set determine the conditions that trigger yellow and red limit alarms.
WARNING
Be aware that the monitors in your care area may each have different alarm settings, to suit different
scenarios. Always check that the alarm settings are appropriate before you start monitoring.
Viewing Individual Alarm Limits (Alarm Mode "All" Only)
1 Alarm Limits
2 Audio source symbol
You can usually see the alarm limits set for each measurement next to the measurement numeric on
the main screen.
If your monitor is not configured to show the alarm limits next to the numeric, you can see them in the
appropriate measurement setup menu. Select the measurement numeric to enter the menu and check
the limits.
Changing Alarm Limits
To change individual measurement alarm limits using the measurement's Setup Menu:
1 In the measurement's Setup Menu, select the alarm limit you want to change. This calls up a list of
available values for the alarm limit.
2 Select a value from the list to adjust the alarm limit.
Reviewing Alarms
To review the currently active alarms and INOPs, select any of the alarm status areas on the fetal
monitor screen. The
monitor's alarm history when you discharge a patient, or if you enter Demonstration Mode.
Alarm Messages Window
The Alarm Messages window shows all the currently active alarms and INOPs in chronological order,
beginning at the top with the most recent. INOPs are shown on the left hand side and alarms are
shown on the right hand side. Any active red alarms are shown first, followed by yellow alarms.
Acknowledged alarms or INOPs are shown with the check mark symbol.
Alarm Messages window pops up . All alarms and INOPs are erased from the
68
Alarm Messages window pop-up keys appear when the window is opened. Selecting the Review
The
pop-up key opens the Review Alarms window.
Alarms
Page 69

Review Alarms Window
The Review Alarms window contains a list of up to 300 of the most recent alarms and INOPs with
date and time information. If configured to do so, each alarm is shown with the alarm limit active
when the alarm was triggered and the maximum value measured beyond this limit. The
window also shows any changes made to the Alarms On/Off or Silence status. Note that only main
alarms On/Off transitions are logged in the alarm history, and On/Off alarm transitions for individual
measurements are not logged.
5 Alarms
Alarms On
SpO₂ NON-PULSAT.
Alarms Silenced
** FHR1 HIGH
** SpO₂ LOW
Review Alarms
The information in the
Review Alarms window pop-up keys appear when the window is opened. Selecting the Active
The
pop-up key opens the Alarm Messages window.
Alarms
Review Alarms window is deleted when a patient is discharged.
Latching Alarms
The alarm latching setting for your monitor defines how the alarm indicators behave when you do not
acknowledge them. When alarms are set to non-latching, their indicators end when the alarm condition
ends. Switching alarm latching on means that visual and/or audible alarm indications are still displayed
or announced by the monitor after the alarm condition ends. The indication lasts until you
acknowledge the alarm.
Viewing the Alarm Latching Settings
To see the alarm latching setting for your monitor:
1 In the monitor's Main Setup menu, select Alarms.
2 Select Alarm Settings, and see the Visual Latching and Audible Latching settings.
This setting can be changed in Configuration Mode. You should be aware of the settings chosen for
your unit. There are three possible choices each for visual and audible latching: Red, Red and Yellow,
and Off. The audible latching configuration can never be configured to a higher level than that
configured for the visual latching. In other words, the audible latching setting is always the same level,
or lower, than the visual latching setting. For example, if visual latching is configured to
Red Only,
69
Page 70

5 Alarms
then audible latching can only be set to Red or Off. The following table shows the possible
combinations for latching settings:
Possible Combinations for Alarm Latching Settings
Visual Latching Setting Audible Latching Setting
Red and Yellow Red and Yellow
Red and Yellow Red
Red and Yellow Off
Red Red
Red Off
Off Off
Alarm Latching Behavior
Alarm Condition Red and Yellow Measurement Alarms
Acknowledgment Presence Non-latching alarms Visual and audible
latching
Alarm has not been
acknowledged.
Alarm has been
acknowledged.
Alarm condition still
present.
Alarm condition no
longer present.
Alarm condition still
present.
Alarm condition no
longer present.
Alarm tone on. Alarm
message.
All audible and visual
alarm indicators
automatically stop.
Alarm tone off. Alarm
message.
Audible and visual alarm
indicators automatically
stop.
Alarm tone on. Alarm
message. Flashing numerics.
Alarm tone on.
Alarm message.
Flashing numerics.
Alarm tone off. Alarm
message. Flashing numerics.
Audible and visual alarm
indicators automatically
stop.
All INOPs except the "unplugged" INOPs are non-latching.
Visual latching,
audible non-latching
Alarm tone on. Alarm
message. Flashing numerics.
Alarm message. Flashing
numerics.
Audible alarm indicators
automatically stop.
Alarm tone off. Alarm
message. Flashing numerics.
Audible and visual alarm
indicators automatically
stop.
70
Page 71

Testing Alarms
In general, to test the functioning of visible and audible alarms, do the following:
1 Enable the alarm.
2 Set the alarm limits.
3 Measure or simulate the parameter that is out of range, or signal loss.
4 Verify that the visible and audible alarms are working.
As an example, to test the FHR alarms:
1 Connect the US transducer to a fetal sensor socket.
2 Enable the FHR alerting (see “Turning Alarms On or Off ” on page 127).
3 Set the high alert limit and delay to 150 bpm and 60 seconds respectively, and the low alert limit
and delay to 110 bpm and 60 seconds respectively (see “Changing Alarm Limits” on page 127).
4 Generate a fetal heart rate of approximately 180 bpm (3 beats per second) for more that one
minute.
5 Verify the functioning of the visible and audible alarm.
5 Alarms
Alarm Behavior at Power On
Selecting AlarmsOffAtStart will cause alarms to be initially suspended or off the next time the monitor
is switched on (depending on the setting for Alarms Off). The Alarms Off as Infinite behaves in the
same manner as when Alarm Mode equals INOP Only.
In order for alarms to be suspended or switched off initially, the monitor must be switched off for
more than one minute, the last main alarm state was set to off or suspended.
The exception to this condition is when the alarms off state has been set to Infinite, and the new active
setting is set to Infinite.
71
Page 72

5 Alarms
72
Page 73

6Patient Alarms and INOPs
This chapter lists alarms and technical alarms (INOPs) for the fetal monitors, alphabetically,
irrespective of their priority. INOPs start “Technical Alarm Messages (INOPs)” on page 76.
Alarm Messages
Fetal alarms are identified by either "FHR" or "DFHR". All other alarms without these identifiers refer
to maternal parameters.
Alarm Message From Condition Indication
6
*** BRADY (Pulse)
***BRADY xxx < yyy
*** DESAT
*** DESAT xx < yy
** DFHR1 HIGH
** DFHR2 HIGH
** DFHR3 HIGH
**DFHR1 xxx>yyy
**DFHR2 xxx>yyy
**DFHR3 xxx>yyy
** DFHR1 LOW
** DFHR2 LOW
** DFHR3 LOW
**DFHR1 xxx<yyy
**DFHR2 xxx<yyy
**DFHR3 xxx<yyy
SpO
2
The heart rate from the Pulse signal
has fallen below the bradycardia
limit. xxx denotes the lowest
measured value; yyy is the
bradycardia limit.
SpO
2
The SpO2 value has fallen below the
desaturation alarm limit. xx denotes
the lowest measured value, and yy is
the desaturation limit.
FHR (DECG) The fetal heart rate obtained from
DECG has risen above the high
alarm limit.
xxx denotes the highest measured
value, and yyy is the high alarm limit.
FHR (DECG) The fetal heart rate obtained from
DECG has fallen below the low
alarm limit.
xxx denotes the lowest measured
value, and yyy is the low alarm limit.
Numeric flashes and alarm
limit is highlighted, red alarm
message, alarm tone.
Numeric flashes, red alarm
message, alarm tone.
Numeric flashes and high
limit is highlighted, yellow
alarm message, alarm tone.
Numeric flashes and low limit
is highlighted, yellow alarm
message, alarm tone.
73
Page 74

6 Patient Alarms and INOPs
Alarm Message From Condition Indication
*** EXTREME BRADY
***BRADY xxx < yyy
*** EXTREME TACHY
***TACHY xxx > yy
** FHR1 HIGH
** FHR2 HIGH
** FHR3 HIGH
**FHR1 xxx>yyy
**FHR2 xxx>yyy
**FHR3 xxx>yyy
** FHR1 LOW
** FHR2 LOW
** FHR3 LOW
**FHR1 xxx<yyy
**FHR2 xxx<yyy
**FHR3 xxx<yyy
** HR HIGH
**HR xxx>yyy
** HR LOW
**HR xxx<yyy
** NBPs HIGH
** NBPd HIGH
** NBPm HIGH
** NBPs LOW
** NBPd LOW
** NBPm LOW
MECG The maternal heart rate obtained
from the maternal ECG has fallen
below the extreme bradycardia limit.
xxx denotes the lowest measured
value, and yyy is the extreme
bradycardia limit.
MECG The maternal heart rate obtained
from the maternal ECG has risen
above the extreme tachycardia limit.
xxx denotes the highest measured
value, and yy is the extreme
tachycardia limit.
FHR (ultrasound) The fetal heart rate obtained from
ultrasound has risen above the high
alarm limit.
xxx denotes the highest measured
value, and yyy is the high alarm limit.
FHR (ultrasound) The fetal heart rate obtained from
ultrasound has fallen below the low
alarm limit.
xxx denotes the lowest measured
value, and yyy is the low alarm limit.
MECG The maternal heart rate obtained
from the maternal ECG has risen
above the high alarm limit.
xxx denotes the highest measured
value, and yyy is the high alarm limit.
MECG The maternal heart rate obtained
from the maternal ECG has fallen
below the low alarm limit.
xxx denotes the lowest measured
value, and yyy is the low alarm limit.
Noninvasive
blood pressure
The measured noninvasive blood
pressure value is above the high
alarm limit.
s, d, or m after the label indicates
whether the systolic, diastolic or
mean pressure has crossed the limit.
Noninvasive
blood pressure
The measured noninvasive blood
pressure value is below the low alarm
limit.
s, d, or m after the label indicates
whether the systolic, diastolic or
mean pressure has crossed the limit.
Numeric flashes, red alarm
message, alarm tone.
Numeric flashes, red alarm
message, alarm tone.
Numeric flashes and high
limit is highlighted, yellow
alarm message, alarm tone.
Numeric flashes and low limit
is highlighted, yellow alarm
message, alarm tone.
Numeric flashes and high
limit is highlighted, yellow
alarm message, alarm tone.
Numeric flashes and low limit
is highlighted, yellow alarm
message, alarm tone.
Numeric flashes and high
limit is highlighted, yellow
alarm message, alarm tone.
Numeric flashes and low limit
is highlighted, yellow alarm
message, alarm tone.
74
Page 75

6 Patient Alarms and INOPs
Alarm Message From Condition Indication
** Pulse HIGH SpO
** Pulse LOW SpO
** SpO₂ HIGH SpO
** SpO₂ LOW SpO
*** TACHY (Pulse)
***TACHY/P xxx>yy
SpO
2
The pulse rate has exceeded the high
alarm limit.
Numeric flashes and high
limit is highlighted, yellow
alarm message, alarm tone.
2
The pulse rate has dropped below
the low alarm limit.
Numeric flashes and low limit
is highlighted, yellow alarm
message, alarm tone.
2
The arterial oxygen saturation has
exceeded the high alarm limit.
Numeric flashes and high
limit is highlighted, yellow
alarm message, alarm tone.
2
The arterial oxygen saturation has
fallen below the low alarm limit.
Numeric flashes and low limit
is highlighted, yellow alarm
message, alarm tone.
2
The heart rate from the Pulse signal
has exceeded the tachycardia limit.
xxx denotes the highest measured
Numeric flashes, alarm limit is
highlighted, red alarm
message, alarm tone.
value, and yyy is the tachycardia limit.
75
Page 76

6 Patient Alarms and INOPs
Technical Alarm Messages (INOPs)
INOP Message, Indication Source What to do
Batt EMPTY
INOP tone, battery LED flashes
during this INOP, alarms cannot
be paused or switched off.
Battery The estimated remaining battery-powered operating time is less
than 10 minutes. Connect the monitor to AC immediately.
If the condition persists and the monitor is not connected to
mains power, this INOP is re-issued two minutes after you
acknowledge it.
Batt INCOMPAT.
INOP tone
Batt LOW
INOP tone
Batt MALFUNCTION
INOP tone, battery LED flashes
during this INOP, alarms cannot
be paused or switched off unless
Battery The battery cannot be used with this monitor. Replace with the
correct battery.
Battery The estimated battery-powered operating time remaining is less
than 20 minutes.
Battery The monitor cannot determine the battery status. If this INOP
persists, replace the faulty battery. If the condition persists and
the monitor is not connected to mains power, this INOP is
reissued two minutes after you acknowledge it.
the monitor is connected to
mains power.
Batt MISSING Battery No battery found in FM20/30. Contact your service personnel.
BUS MASTER MALFUNC Monitor There is a problem with the monitor's hardware. Contact your
service personnel.
CHARGER MALFUNC.
INOP tone, battery LED may
flash
CHECK BATT TEMP Battery The temperature of the battery is too high. Check that the
Battery There is a problem with the battery charger in the monitor.
Connect the monitor to mains power and contact your service
personnel.
monitor is not exposed to heat.
Check Flex Texts
INOP tone
Monitor If this INOP appears, check the monitor and patient settings
before you resume monitoring. If the settings are unexpected,
there may be a problem with the monitor software. Contact your
service personnel.
Check Monitor Func
INOP tone
Check Keyboard
INOP tone
Check Mouse Device
INOP tone
CHECK PAPER
INOP tone
Check Settings
INOP tone
Monitor A potential internal problem with the monitor has been
detected. Contact your service personnel.
Monitor Perform a visual and functional check of the keyboard. Contact
your service personnel.
Monitor Perform a visual and functional check of the mouse input
device. Contact your service personnel.
Recorder Check that there is no paper jam, that the print drawer is
properly shut, that the paper is loaded with the grid facing
upwards, and that the correct Philips paper is being used.
Monitor If this INOP appears, check the monitor and patient settings
before you resume monitoring. If the settings are unexpected,
there may be a problem with the monitor software. Contact your
service personnel.
76
Page 77

6 Patient Alarms and INOPs
INOP Message, Indication Source What to do
CHECK TI CONFIG Monitor If this INOP appears, the monitor can be used normally, except
for the Trace Interpretation feature. Contact your service
personnel.
Check Touch Input Monitor Perform a visual and functional check of the touch input device.
Contact your service personnel.
COINCIDENCE Monitor One or more fetal/maternal heart rates/pulse rates persistently
coincide with each other (see “Cross-Channel Verification” on
page 97).
CUFF NOT DEFLATED
Numeric is replaced by a -?INOP tone.
During this INOP, alarms
cannot be paused or switched
Noninvasive
blood pressure
Remove the cuff from the patient. Make sure that the tubing is
not kinked or twisted. Try restarting the measurement. You can
silence the INOP, but the INOP message remains visible until
the next measurement is started or the
Stop All SmartKey is
selected.
off.
DFHR1 EQUIP MALF
DFHR2 EQUIP MALF
DFHR3 EQUIP MALF
DECG There is a problem with the DECG hardware. Contact your
service personnel.
INOP tone
DFHR1 LEADS OFF
DFHR2 LEADS OFF
DFHR3 LEADS OFF
Numeric is replaced by a -?INOP tone.
DFHR1 SIGNAL LOSS
DFHR2 SIGNAL LOSS
DFHR3 SIGNAL LOSS
DFHR1 UNPLUGGED
DFHR2 UNPLUGGED
DFHR3 UNPLUGGED
INOP tone
MECG EQUIP MALF
INOP tone
MECG LEADS OFF
Numeric is replaced by a -?INOP tone.
MECG UNPLUGGED
INOP tone
FetRec EQUIP MALF
INOP tone
DECG One or more DECG lead is not attached. Make sure that all
required leads are attached, and no electrodes have been
displaced. Check all connections are sound, and that the legplate
attachment electrode is properly attached. If the INOP persists,
try using another adapter cable, or legplate attachment electrode.
If the INOP still persists, contact your service personnel.
DECG The input signal quality is not sufficient to process the
measurement. Reapply the fetal scalp electrode.
DECG Reconnect the DECG transducer to the monitor. Check all
connections are sound.
MECG There is a problem with the MECG hardware. Contact your
service personnel.
MECG One or more MECG lead is not attached. Make sure that all
required leads are attached, and no electrodes have been
displaced. Check all connections are sound. If the INOP
persists, try using another adapter cable. If the INOP still
persists, contact your service personnel.
MECG Reconnect the MECG transducer to the monitor. Check all
connections are sound.
Recorder There is a problem with the fetal recorder hardware. Contact
your service personnel.
77
Page 78

6 Patient Alarms and INOPs
INOP Message, Indication Source What to do
FetRec CHK CONF.
INOP tone
FHR1 EQUIP MALF
FHR2 EQUIP MALF
FHR3 EQUIP MALF
INOP tone
FHR1 SIGNAL LOSS
FHR2 SIGNAL LOSS
FHR3 SIGNAL LOSS
FHR1 UNPLUGGED
FHR2 UNPLUGGED
FHR3 UNPLUGGED
INOP tone
Internal.Comm.Malf
INOP tone
IUP EQUIP MALF
INOP tone
IUP UNPLUGGED
INOP tone
NBP CUFF OVERPRESS
Numeric replaced by a -?INOP tone.
During this INOP, alarms
cannot be paused or switched
off.
NBP EQUIP MALF
Numeric is replaced by a -?INOP tone.
NBP INTERRUPTED
Numeric is replaced by a -?INOP tone.
Recorder
Recorder Speed and/or Scale Type settings are set to
"Unknown" and need to be set to the correct values in
Configuration Mode before the recorder can be operated.
FHR
(ultrasound)
FHR
(ultrasound)
There is a problem with the FHR hardware. Contact your
service personnel.
The input signal quality is not sufficient to process the
measurement. Adjust the position of the transducer to obtain a
better signal.
FHR
(ultrasound)
Reconnect the FHR transducer to the monitor. Check all
connections are sound.
Monitor There is a problem with I2C Bus communication in the monitor.
Contact your service personnel.
IUP There is a problem with the IUP hardware. Contact your service
personnel.
IUP Reconnect the IUP transducer to the monitor. Check all
connections are sound.
Noninvasive
blood pressure
The cuff pressure exceeds the overpressure safety limits.
Remove the cuff from the patient. Make sure that the tubing is
not kinked or twisted and that the correct patient category is
selected. Try restarting the measurement.
You can silence this INOP, but the INOP message remains
visible until the next measurement is started or the
Stop All
SmartKey is selected.
Noninvasive
blood pressure
Remove the cuff from the patient. The noninvasive blood
pressure hardware is faulty. Contact your service personnel.
You can silence this INOP, but the INOP message remains
visible until the next measurement is started or the
Stop All
SmartKey is selected.
Noninvasive
blood pressure
Check the tubing and cuff for leakages or kinks. Check that you
are using the correct cuff size and placement, and that the
correct patient category is selected. Try restarting the
measurement.
If the INOP occurs repeatedly, contact your service personnel.
You can silence this INOP, but the INOP message remains
visible until the next measurement is started or the
Stop All
SmartKey is selected.
This INOP arises when the measurement needed longer than
the maximum time for inflation, deflation or the total
measurement.
78
Page 79

INOP Message, Indication Source What to do
6 Patient Alarms and INOPs
NBP MEASURE FAILED
Numeric is replaced by a -?INOP tone.
Noninvasive
blood pressure
Check that you are using the correct cuff size and placement,
and that the correct patient category is selected. Try restarting
the measurement.
You can silence this INOP, but the INOP message remains
visible until the next measurement is started or the
Stop All
SmartKey is selected.
Check the condition and suitability of the patient for
noninvasive blood pressure monitoring. Use another cuff to
continue measuring.
No Central Monit.
INOP tone
Monitor There is a problem with the communication to the network.
Central monitoring is currently not possible (no patient alarms
or information). Check the connection. Contact your service
personnel.
PAPER END Monitor The end of the paper pack is detected. Insert a new pack of
paper.
PRINTHEAD OVERHEAT
INOP tone
Recorder The printhead is too hot. The recorder stops, the recorder
key is disabled, and remains so until the printhead cools
Stop
down sufficiently. Wait for the printhead to cool down, then
press the recorder
Start/ Stop key or the Silence key to clear the
Start/
INOP.
Pulse(Toco) MALF Toc o MP
Maternal Pulse
There is a problem with the Toco MP transducer hardware.
Contact your service personnel.
Measurement
Settings Malfunc.
INOP tone
Speaker Malfunct.
INOP tone
SpO₂ EQUIP MALF
INOP tone
SpO₂ ERRATIC
Numeric is replaced by a -?-
Monitor The monitor cannot use the predefined settings for monitoring.
Contact your service personnel.
Monitor Contact your service personnel to check the speaker and the
connection to the speaker.
SpO
2
There is a problem with the SpO2 hardware. Contact your
service personnel.
SpO
2
Check the sensor placement. Try another adapter cable and
sensor. If the INOP persists, contact your service personnel.
INOP tone.
SpO₂ EXTD.UPDATE
Label is preceded by a
?(questionable numeric)
SpO₂ INTERFERNCE
Numeric is replaced by a -?INOP tone.
SpO
SpO
2
2
The update period of displayed values is extended due to a
noninvasive blood pressure measurement on the same limb or
an excessively noisy signal.
There is too much interference, caused by a high level of
ambient light and/or electrical interference. Cover the sensor to
minimize ambient light. If the INOP persists, make sure that the
sensor cable is not damaged or positioned too close to power
cables.
SpO₂ LOW PERF
Label is preceded by a
?(questionable numeric)
SpO
2
Accuracy may be compromised due to very low perfusion.
Stimulate circulation at sensor site. If INOP persists, change the
measurement site.
79
Page 80

6 Patient Alarms and INOPs
INOP Message, Indication Source What to do
SpO₂ NOISY SIGN.
Numeric is replaced by a -?INOP tone.
SpO₂ NON-PULSAT.
Numeric is replaced by a -?INOP tone.
SpO₂ NO SENSOR
Numeric is replaced by a -?INOP tone.
SpO₂ POOR SIGNAL
Label is preceded by a
SpO
SpO
SpO
SpO
2
Excessive patient movement or electrical interference is causing
irregular pulse patterns. Try to reduce patient movement or to
relieve the cable strain on the sensor.
2
Check the perfusion at measurement site. If necessary, stimulate
circulation or change measurement site. If the INOP is due to
noninvasive blood pressure measurement on the same limb, wait
until the measurement is finished.
2
Make sure the SpO2 sensor is connected. If the INOP persists,
try another adapter cable and sensor. If you silence this INOP,
the measurement will be switched off.
2
The signal condition of the SpO2 measurement is poor and
measurement accuracy may be compromised.
?(questionable numeric)
SpO₂ PULSE?
Numeric is replaced by a -?-
SpO
2
The detectable pulsations of the SpO2 signal are outside the
specified pulse rate range.
INOP tone.
SpO₂ SEARCHING
Numeric unavailable
SpO₂ SENSOR MALF
Numeric is replaced by a -?INOP tone.
SpO₂ SENSOR OFF
Numeric is replaced by -?INOP tone.
SpO₂ UNKN.SENSOR
Numeric is replaced by a -?-
SpO₂ UPGRADE
Label is replaced by a -?-, or
SpO
SpO
SpO
SpO
SpO
2
SpO2 is analyzing the patient signal to derive Pulse, and SpO2
values. Please wait until the search analysis is complete.
2
The SpO2 sensor or adapter cable is faulty. Try another adapter
cable and sensor. If the INOP persists, contact your service
personnel.
2
The SpO2 sensor is not properly applied to the patient. Apply
the sensor following the instructions supplied by the
manufacturer.
2
2
The connected sensor or adapter cable is not supported by the
SpO
measurement. Use only specified sensors and cables.
2
The SpO2 measurement is currently in UPGRADE mode.
Monitoring is not possible in this mode.
numeric is unavailable.
TimeExpired:NST Monitor The time has expired for the NST timer. Clearing the timer
clears the INOP.
Toco EQUIP MALF
INOP tone
Toco There is a problem with the Toco hardware. Contact your
service personnel.
80
Page 81

INOP Message, Indication Source What to do
6 Patient Alarms and INOPs
Toco UNPLUGGED
INOP tone
Unsupported LAN
INOP tone
User I/F Malfunct.
INOP tone
WRONG PAPER SCALE
INOP tone
Toco Reconnect the Toco transducer to the monitor. Check all
connections are sound.
Monitor There is a problem with the communication to the network and
central monitoring is currently not possible. Check the
connection.If the INOP persists, switch off the monitor and
contact your service personnel.
Monitor Perform a visual and functional check of all the monitor input
devices. Contact your service personnel.
Recorder The grid scale of the paper in the monitor does not match the
grid scale configured in the monitor. Make sure that you use the
correct paper and scale for your institution:
pre-printed: 30-240 in US and Canada, 50-210 in other
geographies.
81
Page 82

6 Patient Alarms and INOPs
82
Page 83

7Admitting and Discharging
The fetal monitor can store basic patient demographic information used to identify patients.
Admit/Discharge on the Monitor
This section describes how you admit and discharge patients when using the monitor as a stand-alone
device (that is, when not used with a obstetrical information and surveillance system such as OB
TraceVue).
Admitting a Patient
The fetal monitor displays physiological data as soon as a patient is connected. This lets you monitor a
patient who is not yet admitted. It is however important to admit patients properly so that you can
identify your patient on recordings.
7
Use the
patients.
To admit a patient,
1 Select the patient name field or select the Admit/ Dischrge SmartKey to open the Patient
2 Clear any previous patient data by selecting Dischrge Patient and then Confirm.
3 Select Admit Patient.
4 Enter the patient information: select each field and use the on-screen keyboard.
5 Select Confirm. The patient status changes to admitted. If the recorder is running, the recorder
Patient Demographics window and its associated pop-up keys to admit and discharge
Demographics
If you do not discharge the previous patient, you will not be able to distinguish data from the
previous and current patients, for example, on the recording.
If a conventional keyboard is connected to the monitor you can use this to enter patient
information:
Last Name: Enter the patient's last name (family name), for example Doe.
–
–
First Name: Enter the patient's first name, for example Jane.
MRN: Enter the patient's medical record number (MRN), for example 12345678.
–
stops and immediately restarts to annotate the new patient data.
window.
83
Page 84

7 Admitting and Discharging
Editing Patient Information
To edit the patient information after a patient has been admitted, select the patient name field on the
main screen of the fetal monitor to open the
changes.
Discharging a Patient
You should always perform a discharge even if your previous patient was not admitted. A discharge:
Patient Demographics window, and make the required
– clears the information in the
– resets all monitor settings to the settings defined in the User Default.
– advances the paper automatically if the recorder is running.
– stops the fetal recorder.
When a patient is discharged from the monitor, all patient demographic data is deleted (trace data is
not affected).
To discharge a patient,
1 Select the patient name field to display the Patient Demographics window and associated pop-up
keys.
2 Select the pop-up key for Dischrge Patient.
3 Select Confirm to discharge the patient.
CAUTION
In order to ensure that the settings are reset to user defaults for a new patient, always discharge the
previous patient from the fetal monitor.
NOTE
In order to ensure a continuous record, it is recommended to discharge the patient before performing
a new patient admission in OB TraceVue.
Patient Demographics window.
New Patient Check
The fetal monitor can be configured to ask you in certain situations:
• after a specified power-off period
• after a specified standby period
whether a new patient is now being monitored. The pop-up window is entitled
84
The monitor offers a
No key to continue monitoring with the current patient data and settings.
a
The time periods for the two conditions can be configured independently.
Yes key to discharge the previous patient and begin monitoring a new patient and
Is This A New Patient?
Page 85

OB TraceVue: via LAN
Both the monitor from which you are transferring a patient and the monitor to which you are
transferring her must be switched on and connected to the OB TraceVue network during the patient
transfer.
When the monitor is connected to an OB TraceVue system over a LAN connection, the OB TraceVue
system acts as the "master" over patient demographic data. All patient and location-related data that is
visible on the monitor is set, overwritten or updated by the OB TraceVue system. See the OB
TraceVue Instructions for Use for details.
OB TraceVue: via RS232
In contrast to a LAN connection, when the monitor is connected to an OB TraceVue system over an
RS232 connection, the OB TraceVue system has no control over the monitor's patient admission and
discharge functions.
7 Admitting and Discharging
Depending on how OB TraceVue is configured, either the
just the bed label alone, are taken from the OB TraceVue system. See the OB TraceVue Instructions for
Use for details.
Last Name, First Name and the bed label, or
85
Page 86

7 Admitting and Discharging
86
Page 87

8Non-Stress Test Timer
The non-stress test (NST) timer shows the elapsed time for the non-stress test. The timer counts up to
the time you set for the NST.
Setting NST Autostart/Autostop
You can set the recorder so that it starts automatically (NST Autostart) when the NST timer is started,
and stops automatically (
elapsed). As default,
NST Autostop) when the NST is complete (when the set run time has
NST Autostart is On, and NST Autostop is Off.
Viewing the NST Timer
8
You can configure the timer notification symbol ( ), the NST label, a progress bar and the
elapsed time to be displayed in the top left-hand corner of the screen. By default, the NST timer is not
displayed on the screen.
Alternatively, you can view the timer in the
To open the
Either
a. Press the
Or
b. Access the NST pop-up keys (see “Accessing the NST Setup Pop-up Keys” on page 88), and press
the
Timers window:
Timer SmartKey .
Timers key.
Timer Expiry Notification
When the timer expires, the color changes from blue to green, you hear a single tone, and a message
appears in the status line on the Main Screen.
The volume of the tone can be set in Configuration Mode.
Timers window.
87
Page 88

8 Non-Stress Test Timer
Accessing the NST Setup Pop-up Keys
You control and set up the NST timer (for example, start, stop, or clear the timer, and set the run time)
using a selection of pop-up keys that you access via any one of three possible routes:
•Via the
•Via the
• Via the NST menu entry in the menu that pops-up when you touch the top left-hand corner of the
screen (Route 3).
Timer SmartKey (Route 1).
Main Setup SmartKey (Route 2).
Via the Timer SmartKey (Route 1)
Press the Timer SmartKey . The Timers window opens, and the pop-up keys for
controlling/setting up the NST timer appear (see “Pop-up Keys for NST Timer Setup” on
page 88).
Via the Main Setup SmartKey (Route 2)
1 Enter the Main Setup menu using the SmartKey .
2 Select NST to enter the Setup NST menu. At the same time, the pop-up keys for controlling/
setting up the NST timer appear (see “Pop-up Keys for NST Timer Setup” on page 88).
Via the NST Field (Route 3)
Select the NST field displayed in the top left-hand corner of the screen (when so configured). The
pop-up keys for controlling/setting up the NST timer appear (see “Pop-up Keys for NST Timer
Setup” on page 88).
Pop-up Keys for NST Timer Setup
Pop-Up Keys Selecting this pop-up key lets you.... Comments
Start start the timer
Stop stop the timer, allowing either restarting after a pause
Start) or clearing (Clear key).
(
Setup NST enter the Setup NST menu. From here you can set the
run time.
Timer return to the Timers window. This pop-up key is not available with
88
This pop-up key is not available with
Route 2, as the
already open.
Route 1, as the
already open.
Setup NST menu is
Timers window is
Page 89

Run Time
8 Non-Stress Test Timer
The run time can be set from 10 to 60 minutes. To set the run time, you first need to enter the Setup
menu:
NST
1 To enter the Setup NST menu:
Either
a. Enter the
Main Setup menu using the SmartKey . Then select NST.
Or
b. Access the NST pop-up keys (see “Accessing the NST Setup Pop-up Keys” on page 88), and
press the
2 Select Run Time.
Setup NST key.
89
Page 90

8 Non-Stress Test Timer
90
Page 91

9Non-Stress Test Report
It is generally accepted that a non stress test (NST) allows you to assess fetal well-being. The monitor's
NST report process uses fetal ultrasound (but not DECG) heart rate traces and the Maternal Toco
Trace, generating a printed report when criteria are met and the test can be considered reassuring. The
American term Non Stress Test (NST) is used for antepartum testing. The interpretation algorithm
and ruleset are equivalent to those implemented in OB TraceVue Revision F.xx, and are based on the
2008 NICHD guidelines.
An NST report is a diagnostic aid, but it does not replace the clinician’s judgment. The interpretation
and the appropriate clinical response remain with the clinician.
A fetus normally produces characteristic heart rate patterns. Average baseline variability and
acceleration of the FHR in response to fetal movement are considered reassuring signs. This test does
not take into account any form of external fetal stimulation.
For every active ultrasound fetal heart rate measurement, one NST report can reside in the monitor’s
memory. The reports are cleared when you discharge a patient and when you start a new NST report.
9
When the NST Report option is available and the "NST Report" feature is "on", the NST status for all
available ultrasound fetal heart rate measurements is displayed as a permanent element within the
application area on the resting display.
The minimum displayed information is:
• NST identification (by FHR number: 1, 2, 3)
• Current NST status (by color: inverse for "not started yet", white for "running", yellow for
"stopped", green for "finished")
Setting Up an NST Report
To setup NST Report functionality:
1 Enter the Main Setup menu and select the NST Report or
2 Select the NST Report SmartKey.
3 Press the "Setup" pop-up key.
4 Set your configuration options.
Select from:
NST Analysis. Choose from On or Off.
•
This switches the report feature on or off. This is linked to the NST timer. Both must be set to
for the NST report to function.
On
91
Page 92

9 Non-Stress Test Report
• Report Recording. Choose from:
–
Manual - press the Record Report pop up key to trigger a manual request.
After Recorder Stop - report is recorded as soon as recorder becomes idle
–
Immediately - If a realtime recording is running, the monitor pauses it. The recording is
–
continued after the report has been recorded.
Average short term variability (STV) value is documented in [bpm] and [ms] if STV is configured as
part of the NST Report. This parameter is not considered as reassuring criteria.
NST Report Status Window
The NST Report window displays a detailed overview of the current NST status for any available
ultrasound fetal heart rate measurement. You can see:
• NST Status - whether it is ready, ongoing, or the time and date at which it was stopped, or at which
it finished.
• Runtime - the time that has elapsed since the NST began.
• Accelerations - the number of FHR accelerations detected so far.
• Baseline - the average baseline value.
• Variability - the average variability value.
• Short Term Variability - the current short term variability (STV) value.
• Decelerations - the number of FHR decelerations detected so far.
• FHR Availability - current statistical FHR availability value.
• Sinusoidal - the current status of sinusoidal rhythm detection.
For criteria not yet met, a white arrow symbol marks the overall status on the top line, and also appear
against every criterion not yet met. A yellow symbol indicates detection of severe or prolonged
decelerations.
The pop-up keys let you perform the following actions:
FHR1, FHR2, FHR3 - switch to the window showing the current NST status for the fetal heart rate.
•
Record Report - prints the NST Report on paper.
•
Record Trace - records the trace episode that belongs to the current report. Depending on device
•
usage, the trace recording might be incomplete.
Setup - opens the Setup NST Report window.
•
92
Page 93

Example NST Report
Field Field Content
9 Non-Stress Test Report
Report Title, with FHR
label and date
Product Information Product DE53102345 G.01.70, OB A.04.24,
Patient Information Rogers, Alice
Start time, end time,
NST duration, Reporting
Period
Overall one-line NST
result summary
Title Trace Interpretation Summary
Result Accelerations Accelerations: 2
Result: Contractions Contractions: 3
Result: Baseline and
Variability
NST Report for FHR1 on 12 Oct 2009
Toco DE52401090, FHR1 DE00002345 A.05.26
Age: 27
Gestational Age: Week 34, Day 5
Time: 11:34 - 12:06
Runtime: 32 minutes
Reporting Period: 20 minutes
NST Criteria*: not met
at: 11:59 12:02
at: 11:57 12:00 12:04
Baseline: 125 bpm (Range: 118 bpm - 129 bpm)
Variability: 23 bpm (Range: 20 bpm - 24 bpm)
Short Term Var.: 0.9 bpm (3.8 msec)
Statistics: FHR
availability
Result: Decelerations Decelerations: 1
Result:
Sinusoidal Rhythm
detected
FHR available: 95%
at: 11:58
severe
prolonged
Sinusoidal: No
93
Page 94

9 Non-Stress Test Report
NST Reassurance Criteria
The patient is monitored for a user-definable period of time (10 - 60 minutes in steps of 5 minutes).
The test is considered reassuring when the following criteria are met:
• The fetal heart rate is valid at least 90% (this is configurable) of the specified time span.
• The FHR features a user-defined minimum number of accelerations.
• The FHR features a user-defined maximum number of tolerated decelerations, and does not
include severe or prolonged decelerations, which are never tolerated.
• The average baseline fetal heart rate lies within the user-defined limits for low heart rate and high
heart rate over the whole time span.
• The FHR exhibits a moderate variability (user-defined) for the specified time span.
An NST Report is generated when the reassuring criteria are met the first time in the current
monitoring phase. When performing NST with twins or triplets, a separate NST Report is generated
for each fetus.
In the printed report, the average short term variability (STV) value is shown in bpm and ms. This is
not part of the reassurance criteria.
After the reassurance criteria have been met, the clinician can print the NST Report and then turn the
fetal monitor off, or may continue fetal monitoring and print the report at any time.
Non-Reassuring Report
When the reassurance criteria are NOT met if the test has run for 90 minutes, or if you stop anytime
during the 90 minute period, then the test is stopped and a report is generated, stating the reassurance
criteria have not been met.
Non-Reactive NST Test
If a non-reactive test occurs and you then use acoustic stimulation, you must exercise caution in
interpreting the resulting traces, as artificial stimulation is not taken into account when calculating test
results.
94
Page 95

10Monitoring FHR and FMP
Using Ultrasound
To monitor a single FHR externally, you use an ultrasound transducer attached to a belt around the
mother's abdomen.The ultrasound transducer directs a low-energy ultrasound beam towards the fetal
heart and detects the reflected signal. Your monitor can also detect fetal movements and print the fetal
movement profile (
week of gestation for non-stress testing or routine fetal monitoring.
WARNING
Performing ultrasound imaging or Doppler flow measurements together with ultrasound fetal
monitoring may cause false FHR readings, and the trace recording may deteriorate.
FMP) on the trace. Monitoring using ultrasound is recommended from the 25th
10
Technical Description
Fetal monitors use the ultrasound Doppler method for externally monitoring the fetal heart rate. Using
the Doppler method, the transducer (in transmitter mode) sends sound waves into the body which are
then reflected by different tissues. These reflections (Doppler echoes) are picked up by the transducer
(in listening mode). These Doppler echoes are amplified and sent to the monitor’s speaker through
which the fetal heart signal can be heard. In parallel the Doppler echoes are processed through an
autocorrelation algorithm to determine the fetal heart rate (FHR). The FHR is displayed on the
monitor’s numeric display and on the recorded trace.
Properly representing the fetal heart rate using a device that derives heartbeats from motion is a
formidable task and the limitations of the technology will be discussed shortly. Basic fetal cardiac
physiology may contribute to difficulties in obtaining a reliable ultrasound signal. A heart rate pattern
of a fetus is capable of extraordinary variation, ranging from a quiet stable pattern with minimal
variation while the fetus is “asleep” to robust accelerations of 40-60 bpm above baseline rate over a
few seconds or exaggerated variability when the fetus is active. Decelerations of the rate 60-80 bpm
below baseline may develop even more abruptly than the accelerations. Beat-to-beat arrhythmias may
further exaggerate the amount of “variability” and be seen at the bottom of variable decelerations, or in
the presence of fetal breathing movements which also tend to lower the fetal heart rate. The
recognition of these normal variations in fetal heart rate patterns will greatly assist in the separation of
genuine fetal information from the artifact.
95
Page 96

10 Monitoring FHR and FMP Using Ultrasound
Limitations of the Technology
All tissues moving towards or away from the transducer generate Doppler echoes. Therefore, the
resulting signal that is provided to the monitor’s speaker, and for further fetal heart signal processing,
can contain components of the beating fetal heart wall or valves, fetal movements, fetal breathing or
hiccup, maternal movements such as breathing or position changes, and pulsating maternal arteries.
The fetal heart signal processing uses an autocorrelation algorithm to obtain periodic events such as
heart beats. If the signal is erratic such as from a fetal arrhythmia, the ultrasound device may have
trouble tracking the abrupt changes and may misrepresent the true FHR pattern. Signals such as those
from moving fetal limbs are usually very strong, thereby masking the fetal heart signal. During
prolonged movements where the fetal heart signal is masked, the FHR appears blank on the numeric
display and as a gap on the recorded trace. Fetal position changes, maternal position changes, or
uterine contractions can move the fetal heart partly or fully out of the ultrasound beam resulting in
signal loss or even picking up Doppler echoes from pulsating maternal arteries. In these cases a
maternal heart rate or sometimes even a rate resulting from the mixture of fetal and maternal signals
may be displayed on the monitor’s numeric display and on the recorded trace.
In contrast to the timely well-defined R-peak of an ECG signal obtained with a fetal scalp electrode,
the ultrasound Doppler signal from a fetal heart consists of multiple components from atria (diastole),
ventricles (systole), valves, and pulsating arteries. These components vary depending on fetal and
transducer position and angle, and are further modulated by factors such as fetal or maternal breathing.
These effects may produce what is called “artifact”. Optimal transducer positioning therefore is key to
minimizing these effects and thereby minimizing artifact.
Misidentification of MHR as FHR
FHR detection by the monitor may not always indicate that the fetus is alive. Confirm fetal life before
monitoring, and continue to confirm that the fetus is the signal source for the recorded heart rate (see
“Confirm Fetal Life Before Using the Monitor” on page 10).
Here are some examples where the MHR can be misidentified as the FHR.
• When using an ultrasound transducer:
– It is possible to pick up maternal signal sources, such as the maternal heart, aorta, or other
large vessels.
– Misidentification may occur when the maternal heart rate (MHR) is higher than normal
(especially when it is over 100 bpm).
NOTE
When an ultrasound transducer is connected to the monitor but not applied to the patient, the
measurement may generate unexpected intermittent FHR readings.
• When Fetal Movement Profile (FMP) is enabled:
The FMP annotations on a fetal trace alone may not always indicate that the fetus is alive. For
example, FMP annotations in the absence of fetal life may be a result of:
– Movement of the deceased fetus during or following maternal movement.
– Movement of the deceased fetus during or following manual palpation of fetal position
(especially if the pressure applied is too forceful).
– Movement of the ultrasound transducer.
96
Page 97

Cross-Channel Verification
To reduce the possibility of mistaking the MHR for FHR, it is recommended that you monitor both
maternal and fetal heart rates (see “Monitoring Maternal Heart / Pulse Rate” on page 155). The
monitor's cross-channel verification (CCV) facility can help by automatically detecting when the same
heart rate is being recorded by different transducers.
When the MHR and FHR are being monitored, CCV will alert you when the values are very similar or
the same. This may indicate fetal demise, and the transducer may be picking up a signal from a
maternal source. CCV can compare all monitored heart rates and indicate when any two channels are
picking up the same signal.
When CCV detects two heart rates that coincide, you are alerted within approximately one minute to
check the tracings and potentially to reposition the transducers.
In case of difficulties deriving a stable maternal pulse reading using the Toco MP transducer, it is
recommended to use SpO
SpO
, use MECG instead. Reasons to switch the method for deriving a maternal pulse or heart rate
2
include: motion artifacts, arrhythmia, and individual differences in pulse signal quality on the
abdominal skin (via Toco MP).
instead. In case of similar problems with the pulse measurement from
2
10 Monitoring FHR and FMP Using Ultrasound
What You Need
• Ultrasound transducer.
• Ultrasound gel.
• Transducer belt (and optional butterfly belt clip, if applicable).
Cordless Monitoring - Important Considerations
When using an Avalon CTS Cordless Fetal Transducer System (M2720A) with your monitor, please
note the following:
• Refer to “Cordless Monitoring” on page 22 for general rules regarding the use of cordless
transducers from an Avalon CTS Cordless Fetal Transducer System.
• When using a cordless ultrasound transducer from an Avalon CTS system to measure the fetal
heart rate, note that you cannot use any other ultrasound transducer (whether cordless or wired) at
the same time.
WARNING
To avoid interference on ultrasound channels: When changing from using cordless to wired
ultrasound transducers to measure the fetal heart rate, REMOVE the cordless ultrasound transducer
from the patient and dock it in the Avalon CTS basestation. Never use ultrasound transducers
connected to more than one fetal monitor on the same patient.
• When using an Avalon CTS Cordless fetal Transducer System (M2720A), the monitor
automatically sets the Fetal Movement Profile (FMP) to Off, due to the likelihood of generating
artifacts when the mother is mobile. You can enable FMP again manually should you wish, but you
should be aware that FMP is not recommended when the mother is likely to move, and you should
97
Page 98

10 Monitoring FHR and FMP Using Ultrasound
disable Fetal Movement Profile (FMP) on the fetal monitor (Fetal Movement Off) if the mother is
walking. See also “Fetal Movement Profile” on page 100.
• The symbol appears next to the measurement label, indicating that the measurement is being
made by a cordless transducer.
Preparing to Monitor
1 FHR1
2 Toco parameter
Prepare for ultrasound monitoring using the list below. The standard procedures in use in your facility
determine the sequence of actions.
• Determine fetal position.
• Fasten the belt around the patient.
• Switch on the monitor and the recorder.
• Connect the transducer to a free socket. Note that the signal quality indicator for the heart rate
initially displays an invalid signal.
• Apply a thin layer of ultrasound gel to the underside of the transducer.
CAUTION
Using ultrasound gel not approved by Philips may reduce signal quality and may damage the
transducer. This type of damage is not covered by warranty.
• Place the transducer on the abdomen, if possible over the fetal back or below the level of the
umbilicus in a full-term pregnancy of cephalic presentation, or above the level of the umbilicus in
a full-term pregnancy of breech presentation. Work the transducer in a circular motion to ensure
the gel layer makes good contact.
When the sensor is connected correctly and a good signal is being received, the signal quality
indicator should be full. If an inadequate signal is being produced, the signal quality indicator will
indicate a poor signal, and no numeric will appear on the screen.
98
• Adjust the audio volume of the monitor's loudspeaker to a clearly audible level, while moving the
transducer over the abdomen. When you have a good signal, secure the transducer in position
below the belt.
Page 99

10 Monitoring FHR and FMP Using Ultrasound
WARNING
Periodically compare the mother's pulse with the signal coming from the monitor's loudspeaker to
ensure that you are monitoring fetal heart rate. Do not mistake a doubled or elevated MHR for FHR.
Note that when applied to the patient, the ultrasound transducer may warm slightly (less than 1°C/
1.8°F above ambient temperature). When NOT applied, the transducer can reach a maximum
temperature of 44°C/112.2°F at an air temperature of 40°C/104°F.
Selecting Fetal Heart Sound
You can listen to the fetal heart sound from one ultrasound transducer at a time. When the fetal heart
sound is selected for a FHR channel, you see the audio source symbol next to the FHR numeric
label for that channel.
1 FHR1
2 Audio source symbol
To select the audio source for a FHR channel:
Enter the
Press
Setup FHR1 menu for the channel you want to hear (FHR1 used as an example).
Select Audio. It may take a few seconds for the audio source symbol to appear.
Changing the Fetal Heart Sound Volume
The FHR volume symbol at the top right of the Fetal Heart Sound Volume window gives you an
indication of the current volume. To change the volume:
1 Select the volume symbol . The volume scale pops up.
99
Page 100

10 Monitoring FHR and FMP Using Ultrasound
Select the required volume from the volume scale.
2
Fetal Movement Profile
The Fetal Movement Profile (FMP) parameter detects fetal movements via an ultrasound transducer
connected to the monitor. Only the fetus monitored on the FHR1 channel is monitored for FMP.
Once you have enabled FMP (see “Switching FMP On and Off” on page 101), it is triggered
automatically whenever:
Alarm Volume
1
• You connect an ultrasound transducer.
• A patient is discharged.
Be aware that when using an Avalon CTS Cordless fetal Transducer System (M2720A), the monitor
automatically sets the FMP to
When FMP is enabled, the ultrasound transducer detects gross fetal body movements. Eye movements
are not detected and movement of the feet and hands may not be detected. Positioning or
repositioning of the transducer is recorded as fetal movement. Maternal movement, excessive fetal
breathing or fetal hiccups may also be recorded as fetal movement. You can mark these artifacts on the
trace paper using either the remote event marker or the event marker key as described in “Marking an
Event” on page 51. Ignore these movements when you interpret the FMP. When monitoring twins or
triplets, only the fetus monitored on the FHR1 channel is monitored for movement, but be aware that
movements recorded for FHR1 may also be caused by movement of the second or third fetus.
The fetal movement profile (FMP) appears as "activity blocks" (see A below) along the top of the
Toco Scale, the length of each block showing the duration of the activity.
Off (see “Cordless Monitoring - Important Considerations” on page 97).
100
 Loading...
Loading...