

Page 1

Exclusively Distributed by 3M ESPE
Celara™ Denture System
Celara Denture System
Training Manual
Page 2

Table of Contents
Introduction: The Celara Denture System .....................................................................................3
Replacing a Patient’s Existing Denture ....................................................................................3–15
“Why Start from Scratch?” ....................................................................................................3
Making “Excellent” Final Impressions ................................................................................ 4–5
Suggestions When Using the Dentures as Trays for Final Impressions ....................................6
Evaluating “Records” from Impressions ..............................................................................7– 8
Boxing Impressions and Pouring Casts ............................................................................. 8 –11
Fabricating the Wax Pattern in the Dental Office ............................................................ 12–14
Sending the Container to the Laboratory to Have the Laboratory Inject the Wax Pattern ....... 15
Page 3
Introduction
Congratulations, and welcome to the Celara™ Denture System! The Celara System was developed to
help dental professionals to successfully treat the expanding population of denture patients.
Traditional denture techniques are lengthy, cumbersome and often lead to unpredictable results. In
addition, over the last several years, denture training is being de-emphasized in dental schools. The
bottom line is that fewer dentists would like to treat denture cases, while the demand for denture
treatment is increasing.
The Celara Denture System started with replacing a patient’s existing denture and has evolved
into many other applications; such as: New Dentures, Spare Dentures, and Implant Retained
Dentures. The Celara Denture System is your solution to your removable cases.
Replacing a Patient’s Existing Denture
“Why Start From Scratch?”
It is accepted practice that patients should have their complete dentures replaced every 5–7 years
to compensate for shrinkage of the ridges and the wear of the teeth. Making a new denture for
existing denture wearers can be one of the most challenging procedures dentists can perform.
Why? Patients often have trouble adapting and adjusting to the new denture — especially
when the dentist starts from scratch — when few, if any, attributes of the old dentures can be
adequately communicated to the laboratory. The Celara Denture Technique enables dentists to
routinely fabricate dentures in three simple appointments with better patient satisfaction and fewer
adjustments. This is all accomplished with precise communication between the patient, the doctor,
and the dental laboratory.
Figure 1: Celara Refill Kit.
Everything is conveniently packaged
and pre-measured.
• Rapid Repair Tabs —to extend the
borders or repair broken flanges
• Celara Disposable Container — for
boxing the impression
• Celara Extended Pour Alginate
• Celara Quick Setting Stone with
Water Measure
• Celara Laboratory Bag
3
Page 4
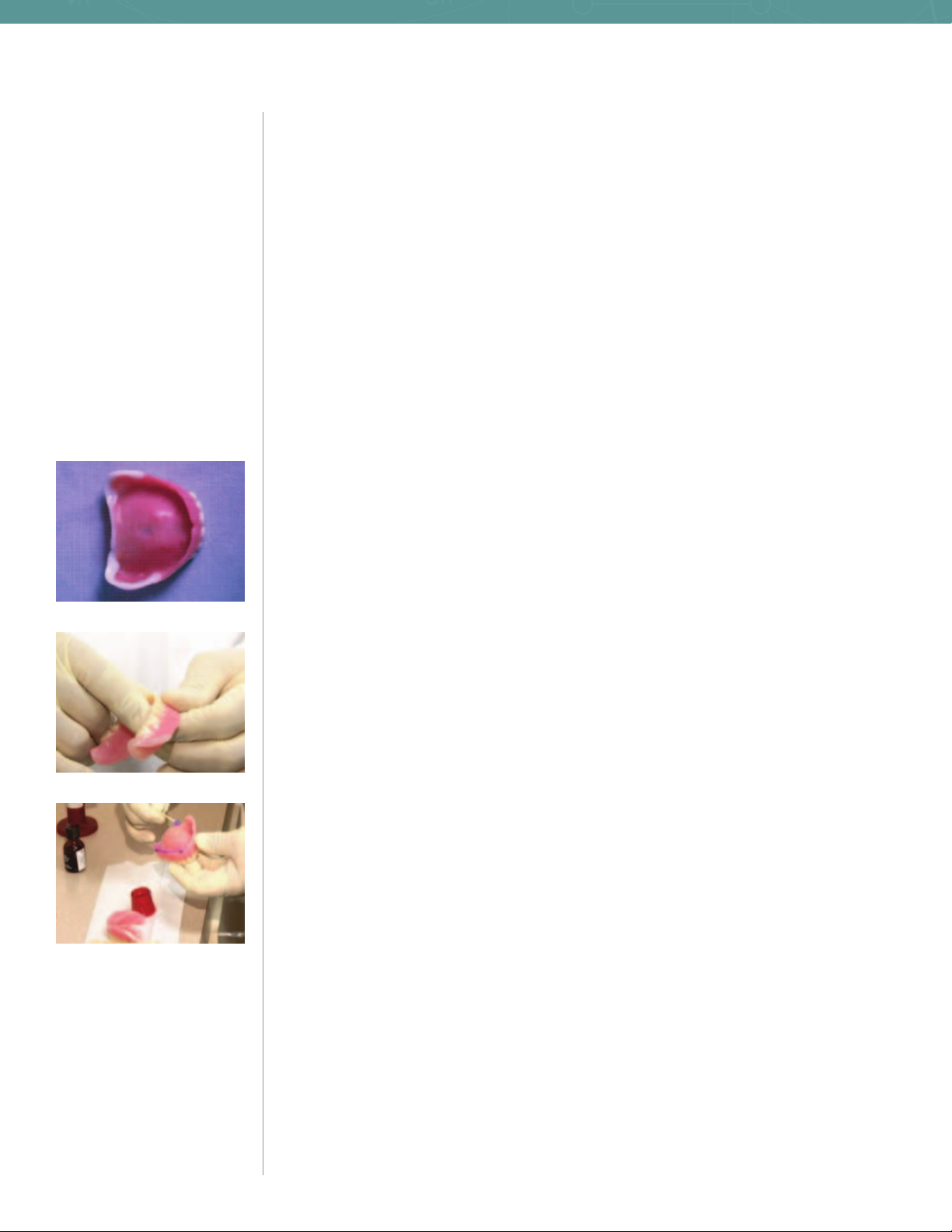
Figure 2A
Making “Excellent” Final Impressions
The Existing Denture Makes an Excellent Tray for the Final Impression
• It has borders which the patient is accustomed to
• The occlusion can help orient the tray back into the mouth correctly
• The old denture usually fits loosely, creating an even thickness of impression material
With today’s modern materials, it is not necessary to grind out undercuts or drill relief holes
through the old denture. With the Celara™ Denture Technique, doctors can use their preferred
impression material and techniques. The following two-stage impression technique is
strongly recommended:
Two Stage Impression Technique — Stage 1:
1. Scrub the denture with pumice and water.
2. Evaluate the border extensions —if the critical areas are short, they can be extended using
the Celara Rapid Repair Tabs. It is not recommended to use the Rapid Repaid Tabs over the
entire denture borders as is typically done with a custom tray. They are used only on the
borders which are critical to the fit — the posterior tuberosity areas and posterior border of the
maxillary denture and retromolar pad and buccal shelf of the mandibular denture (Figure 2A). It
is best to maintain the other borders of the denture as these borders are not critical to the fit,
and they are what the patient is used to. This is one of the strongest rationales for using the
denture as a custom tray. If the flange is broken, it is easily repaired using Celara Rapid Repair
Tab s (Figure 2B). Rapid Repair Tabs are not used in every case.
Figure 2B
Figure 3
3. Apply appropriate adhesive liberally around the borders only. It is not necessary
or recommended, to apply the adhesive around the entire tissue surface of the
denture (Figure 3).
It greatly expedites the clean up when adhesive is not applied over the entire tissue surface. Further,
in the event an impression is missed, the impression material over the palate or crest of the ridge
can easily be cut away with a dull knife, enabling a new impression to be made.
4. Apply heavy body polyvinylsiloxane around the borders of the denture, insert the denture in
the mouth and border mold.
4
Page 5
When fabricating upper and lower dentures, it is best to make the impressions simultaneously with
the teeth lightly in occlusion. Always insert the maxillary denture first, making sure it is completely
seated, and do an open-mouth border molding technique for the posterior border — picking up
the hannular notches and posterior tuberosity areas. Simply have the patient open very wide
and move the jaw side to side to establish the thickness of the posterior tuberosity areas. With
the mandibular denture, you want a “closed mouth” border molding technique; after you insert
the denture, have the patient lift his/her tongue to record the sublingual frenulum and sublingual
mylohyoid area— floor of the mouth.
Remove the dentures after the impression material sets and carefully trim away all impression
material which is on the tissue surfaces, leaving an established border (Figure 4).
Border molding with the heavy body first, accomplishes two things. It creates a seal and makes
a loose denture fit, and it lifts the denture off the tissue slightly— approximately 1/2mm, which
creates relief for the final wash. The heavy body polyvinylsiloxane is ideal for border molding an
existing denture as it will not overextend and will roll to the existing borders. This maintains the
length and thickness of these borders.
1. Have the patient rinse out with very cold water for 1–2 minutes.
The cold water will shrink the tissues and reduce inflammation making an impression with the
maxillary arch constricted. Often the maxillary arch will expand slightly to compensate for an
ill-fitting denture.
Figure 4
2. Dry the ridges.
3. Make the final impression with “extra light” or “light” body wash (Figure 5). Avoid overfilling
the anterior of the maxillary denture with impression material.
4. Always seat the maxillary denture prior to the mandibular denture when making the
impressions simultaneously. Completely seat the maxillary denture and have the patient
open wide, moving the jaw side to side. Insert the mandibular denture, and have the patient
lift the tongue and border mold. Have the patient hold his/her teeth lightly in occlusion while
the impression material sets.
Figure 5
5
Page 6

Figure 6
Suggestions When Using the Dentures as Trays
for Final Impressions
Single Stage Impression Technique
When using a one-stage impression technique — using a single phase impression material — use
a MEDIUM BODY VISCOSITY. Light body can result in too thin a layer of impression material and
undercuts can be an issue. Heavy body impression material can compress the tissues resulting in
excessive future adjustments.
Although border molding is recommended and extremely effective, some doctors may choose not to
border mold, and instead use a technique that has proven successful for them in the past.
Addressing Undercuts
Typically, severe undercuts are not present in patient’s wearing a denture that is 10+ years old.
Additionally, border molding with a heavy body impression material will help to relieve and insulate
against under cuts.
With that said, If severe undercuts exist within the ridge of the denture, it is advisable to relieve
the denture from the tissue using 3 small pieces of Celara Rapid Repair Tabs — acting as a tripod
of tissue stops (Figure 6). This can be easily accomplished by softening the tab and placing 3 small
pea-sized pieces on the tissue surfaces of the denture in three areas and having the patient bite
lightly into occlusion. This technique will lift the denture(s) off the tissue slightly, approximately
1mm per arch, assuring adequate thickness of impression material to enable the cast to come
out of the undercut without breaking — providing the impression is properly boxed. When doing
a two-stage impression technique, the heavy body material usually relieves the denture slightly.
If severe undercuts exist, the denture base can be relieved with Rapid Repair Tabs prior to
border molding.
Functional Impressions
When hyperplasia exists and it is necessary to heal the tissues prior to making the new denture, a
tissue conditioning treatment regime can be used. When a functional impression technique is used
as the final impression, and it becomes hard after being worn for several days, it is recommended
a final wash of polyvinylsiloxane be made over the functional impression as a final wash. These
functional impression materials can slump, resulting in an inaccurate impression, and the
functional impressions can become hard and non-resilient, resulting in possible fracturing of the
cast upon removal.
Occasionally, the hyperplasia occurs from the occlusion and must be treated after the new dentures
are fabricated.
6
Page 7

Evaluating “Records” from Impressions
After the impressions are carefully removed from the mouth and all excess impression material
removed from the facial surfaces of the dentures, the impressions are placed back into the mouth
and all aspects of the records are observed such as midline, vertical dimension, tooth positions,
planes of occlusion, esthetics, etc.
WHEN SIGNIGICANT CHANGES ARE NECESSARY— a wax pattern can be made in the dental office
or in the dental laboratory. A wax pattern is made and used similarly to a wax rim obtaining proper
vertical, tooth positions, planes of occlusion, and centric relations. When the wax pattern(s) is
fabricated in the dental office, the impression(s) is made, the wax pattern(s) is fabricated and all
patient records are obtained usually on the same sixty to ninety minute appointment.
WHEN MINOR CHANGES ARE NECESSARY — a wax pattern can be fabricated in the dental office
and used to obtain and verify all the records. Or alternatively, as is most commonly done, the
impression is boxed and a cast poured in the dental office. The containers are then sent to the
laboratory in a tightly sealed bag, along with the prescription, a bite registration, and the desired
mold and shade of the teeth. The laboratory can inject the pattern over a stabilized base and
provide a partial set-up (with the anterior teeth) or a complete set-up for the try-in on the second
appointment (Figure 7A, 7B).
Figure 7A: Partial Set-Up
Figure 7B: Complete Set-Up
7
Page 8

Troubleshooting— Using Existing Denture as Tray for Final Impression
• Avoid using Rapid Repair Tabs over entire borders of denture.
– This is usually not necessary, and you will likely throw off the occlusion.
• Avoid using only light body or extra-light body impression material in a single stage
technique without relieving denture off tissues with Rapid Repair Tabs — 3 small
pea-sized pieces, softened, acting as a tripod similar to tissue stops in a custom tray.
– This will result in undercut issues! An extremely thin wash of impression will result
without relieving the denture.
• Avoid using only heavy body impression material in a single stage technique.
– This will result in excessive compression of the tissues and excessive adjustments.
• Avoid using alginate as final impression inside denture.
– This material is too flimsy and the impression will distort when re-inserted into
the mouth.
Always use appropriate adhesive liberally around the borders in a two-stage impression.
If Impression is Missed
Cut away tissue surface, leaving the borders and remake impression. It takes the same time as
simply adding to missed area. This is one reason not to add adhesive over entire tissue surface of
denture in a two-stage impression.
Figure 8A
Figure 8A
Boxing Impressions and Pouring Casts
Typically the dental assistant performs the boxing of impressions and pouring the cast. The Celara
Refill Kit has everything necessary packaged and pre-measured for the dental assistant. The
procedure to box the impression and pour the cast is very simple and easy to perform, however,
the assistant should practice several times prior to doing an actual case.
Supplies Needed:
• 2 Mixing Bowls
• 2 Spatulas
• 1 Dull Knife
• Celara Refill Kit
• 1 Rubber band
To box the impression and pour the cast, the assistant will need the Celara container, which
consists of an upper and lower half. The lower half has an open top and a closed bottom, while the
upper half has an open bottom and top ( Figure 8A, 8B).
8
Page 9

Boxing the Impression
Empty the entire package of the pre-measured Celara™ alginate into a clean mixing bowl and
use the lower half of the container full of water for the measure of water. It is important that you
use the amount of alginate in the package with a full lower container of water. This consistency
produces a loose mix of alginate. Too thick a mix will result in the alginate rolling at the denture
borders exposing too much of the denture flange. This can result in the denture locking on the
cast. Too much water or too little alginate will result in too thin a mix, and can result in the denture
sinking into the alginate. The proper mix of alginate results in a thin mix which may be lumpy and
may contain bubbles having the consistency of oatmeal. It is okay to have a few lumps and a
few bubbles. We are using the alginate mainly to box the impression — alginate is just as
accurate an impression material if mixed thin or thick.
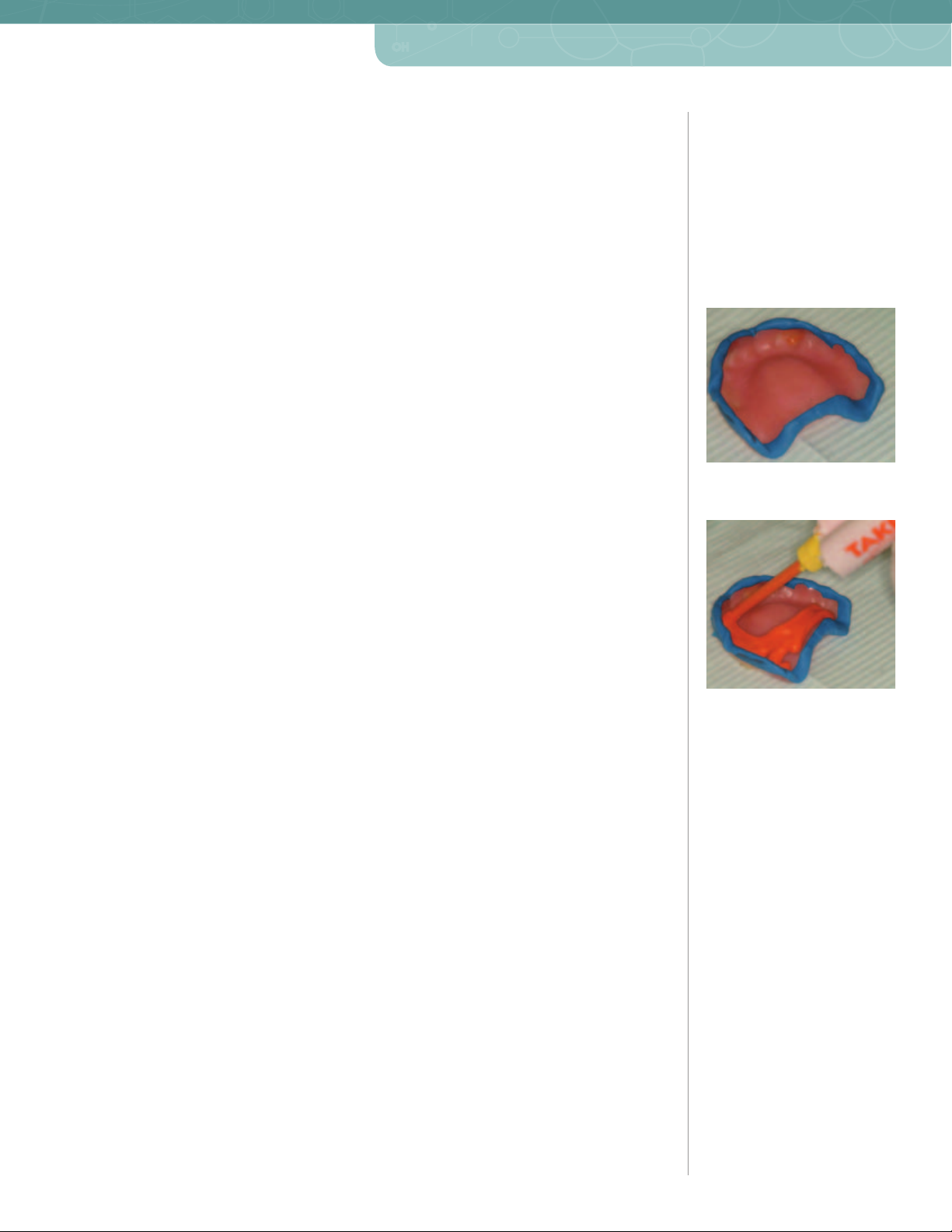
Pour the thin mix of alginate in the lower half of the container to within approximately 1/4" from
the top, or 7/8 full (Figure 9). This leaves enough room for the displacement of the denture when
submerged in the alginate. Cover the palate, occlusal, and incisal edges of the teeth with the
alginate and immerse the denture in the lower container filled with alginate teeth side down so that
1–2mm of the borders are above the alginate to prevent the denture from locking on the cast. It
is important that only 1–2mm of the borders are above the alginate to prevent the denture
from locking on the cast (Figure 10A).
The alginate may run onto the posterior surface of the impression and cause the anterior flanges
of the denture to rise above 1–2mm. If this occurs, you can tease the anterior border down in the
alginate by holding it with your fingers or even placing a pencil across the impression (Figure 10B).
Figure 9
Fig ure 10A
Fig ure 10B
After the alginate sets — approximately 2 minutes— ALL THE ALGINATE MUST BE REMOVED
FROM THE IMPRESSED SURFACES OF THE IMPRESSION. It is extremely critical that all the
impressed surfaces of the impression be exposed by removing all alginate which is over
the impression. The alginate can be easily removed by trimming it away with a dull knife
(Figure 11A, 11B). It is recommended that the alginate at the heals of the impression be removed by
cutting it away on a bevel. This places excess stone behind the heal of the cast — strengthening the
heals of the cast which is where most casts fracture.
When boxing the mandibular impression, the posterior heals of the impression will be immersed in
the alginate and all the alginate covering these areas of the impression must be removed prior to
pouring a cast. This is easily accomplished cutting the alginate away with a dull knife. When
the alginate covers the posterior heals of the mandibular impression, the alginate can only be
removed to the edge of the impression and therefore 1–2mm of these borders will not be above the
alginate. (Figure 12).
If any of the alginate ran out over the rim of the container, it is easily removed with a dull
knife. This assures the upper and lower containers have a positive seat.
Fi g u re 11A
Fi g u re 11B
Figure 12
9
Page 10

Figure 13
Pouring the Cast
Place the upper half of the container over the lower half — making sure the serrated top is punched
out. The upper and lower halves will seat, but will not snap or lock. Make sure the upper and lower
ledges are seated correctly.
Empty a complete package of Celara™ stone in a clean mixing bowl and add a full measuring cup
(provided) of water. The proper amount of water for stone powder is 43 mL. Too much water which
produces a thin, runny mix, can cause the stone to over expand — possibly resulting in an ill-fitting
denture. If a vibrator is used to pour the stone cast the containers must be secured tightly with a
rubber band to prevent the stone from running out between the containers (Figure 13).
Cover the entire surface of the impression with stone, placing the stone in the posterior of the
impression and forcing the stone forward thus preventing trapping air. It will be noted that the stone
will not completely fill the top half of the container.
The Celara stone will completely set in 5–7 minutes and is formulated to have the ideal expansion
and hardness for dentures. It is not desirable to have a cast which is too hard. The acrylic of the
denture can fracture upon deflasking if the cast is too hard. It is desirable to have a very slight
expansion of the cast — enabling a thin layer of moisture between the denture and the ridge.
Troubleshooting— Boxing Impressions and Pouring Casts
• Avoid adding the alginate powder to water.
– This is too difficult to mix. Add the water to the alginate powder.
• Avoid leaving alginate powder in the bag when dispensing into mixing bowl.
– This can lead to too thin a mix.
• Avoid not measuring the water.
– To use alginate to box an impression, you want a thinner mix than is typically done
for using alginate to make an impression. With the Celara Refill Kit, everything is
pre-measured. USE THE LOWER CONTAINER FULL OF WATER AS THE WATER
MEASURE FOR A FULL PACKAGE OF ALGINATE. This will produce the correct
consistency for boxing the impression.
• Avoid filling the lower container full before immersing the denture.
– This will lead to excess alginate running over the ledge of the lower container.
• Avoid trapping air.
– Smear alginate over the palate and teeth prior to immersing in the alginate. Immerse the
maxillary denture by rotating it from the anterior to the posterior.
• Avoid leaving any alginate over the impressed surfaces of the impression.
– This will affect the cast and ADVERSELY AFFECT THE FIT OF THE DENTURE, especially
alginate in the posterior of the impression.
10
• Avoid mixing the stone too thin.
– This can result in the stone over-expanding and the cast being too soft.
Page 11

Opening Container
After the stone completely sets (5–7 minutes), carefully open the container, using a laboratory
knife. Typically the denture will remain on the stone cast in the upper half of the container and an
alginate impression of the external surface of the denture will be in the lower half of the container.
Occasionally, the denture will come off the cast and be in the alginate —this is not a problem.
Simply remove the denture from the alginate.
Rarely the alginate will come out of the lower container. If this occurs, simply separate the alginate
from the stone and place the alginate back into the lower container. This usually occurs when the
lower container is not filled adequately with alginate, or excess water is on the bottom of the lower
container prior to filling it with alginate.
Removing Denture from Cast
Remove the denture carefully from the cast. Use a laboratory knife along the sides of the
posterior edges and carefully tease the denture impression off the cast. Avoid prying with
the knife on the heals of the maxillary and mandibular denture, as often these posterior
areas are worn thin and may easily fracture.
Cleaning the Patient’s Denture
Before giving the denture back to the patient, be sure to remove residual Orange Solvent using
standard cleaning practices; i.e., steam cleaning or ultrasonic cleaning.
With the Celara™ Denture Technique, the patient is never without their denture. The whole
procedure, when mastered, should routinely take approximately 30–45 minutes, or 1–1 1/2 hours
when fabricating the wax pattern in the dental office.
11
Page 12

Fi gur e 14
Fig ure 15A
Fig ure 15B
Figure 15C
Fabricating the Wax Pattern in the Dental Office
A wax injector enables the ability to fabricate the wax pattern in the dental office and modify
this custom occlusal rim and take all the patient records on the same appointment as the
impression. (Figure 14).
The optimum injecting temperature is 170–190°F. This temperature is typically reached by setting
the injector at the Medium/High position. It will take about 20 minutes to reach this temperature
from a "solid" state. Experiment with your injector to find the optimum position for injecting. Mark
this position on your machine for future reference.
Spruing The Alginate Lower Container
Entrance Sprue Hole: Using a thin tapered bur, approximately 1/8" in diameter (determine the
size bur that works best for you), drill a hole through the anterior of the container entering the
void created by the denture. The sprue hole should be started approximately in the middle of the
container, not near the containers ledge, and enter the void above the ANTERIOR TEETH IN THE
ANTERIOR FLANGE (Figure 165, 165, 15C).
Do not have the sprue hole enter the midline of the anterior teeth as the anterior teeth need to be
accurately represented in the wax pattern. The hole can also be made using a cork boring tool or
small 3/16" thin straw, once a small hole is cut through the container (Figure 16).
Exit Sprue Hole(s): The exit sprue for the maxillary arch can be made similarly as the entrance
sprue and should exit the distal end of the impression void. The exit hole should be directly opposite
the entrance hole for the maxillary arch. If you prefer, you can make 2 exit holes in the maxillary
arch — one at one at each distal end of the maxillary denture. Be sure to make these holes at the
“highest point” of the void when held vertically, as to allow the wax to fill the entire void before
exiting. In the mandibular arch there is one entrance sprue hole and two exit holes — one at each
distal end of the mandibular denture, exiting the distal retromolar area (Figure 17). Note: Be careful
not to make the exit holes in an area where the stone cast will cover the holes. These holes must be
made in the void itself.
12
Figure 16
Fi g u re 17
Page 13

Injecting the Wax Pattern
At the proper temperature, the wax will flow easily and be clear. If it is cloudy, it is too cool. If you
hear it cracking in the pot, it is too hot.
When using the wax injector for the first time, melt 8–10 Celara™ Wax rods in the injector, and
bleed the air out of the pump by pumping 4 or 5 times until wax begins to come out. Going forward,
add 1–2 rods of wax per arch being fabricated.
Lubricate the stone cast with an appropriate model release agent. DO NOT FORGET TO LUBRICATE
THE STONE CAST. The wax will stick to the stone if separating agent is not used.
Secure the container tightly together with a rubber band. Test the wax injector— PUMP
SLOWLY— to make sure the wax is flowing. Prior to injecting the wax, make sure the alginate is
dry and free of excess moisture. The alginate can be carefully dried with air immediately prior to
injecting. Excessive moisture, especially in the anterior teeth, will cause the incisal edges to be
misrepresented in the wax pattern. Carefully place the inlet sprue hole over the inlet of the wax
injector and pump very slowly until the wax extrudes through the exit sprue(s).
In the case of the mandibular denture, the wax may extrude through one exit hole first. Place
your finger over this exit hole and force the wax through the second hole. This will assure a
complete pattern.
DO NOT REMOVE THE CONTAINER IMMEDIATELY. Keep the container on the inlet of the
injector long enough for the wax to solidify in the inlet sprue hole. This will prevent the wax
from running out when the container is lifted off (Figure 18). If the wax runs out, this will
create voids in the “distal” end of the wax pattern.
Immediately place the container in a cold water bath to allow the wax to adequately
harden—approximately 5 minutes. It is important for the wax to harden completely while
securely on the cast, as this will ensure an accurate fit at try-in.
After the wax hardens, open the container and trim the wax pattern on the cast.
Occasionally, the wax pattern will come off the cast and it will be in the alginate. If this occurs, cut
through the sprue before removing the wax from the alginate.
The Celara wax pattern is a replica of the denture over the cast. The wax is a special formulation
which is rigid enough to obtain records in the mouth without distorting. If the wax pattern breaks or
distorts upon removal from the cast, it usually means there are significant undercuts in the cast. If
the wax pattern breaks or distorts, check the cast for undercuts and block them out with soft utility
wax and re-inject a new wax pattern.
Fig ure 18
13
Page 14

The wax pattern is ideal for obtaining records, as it was injected directly over the cast, and
therefore will fit (Figure 19). If the dentist desires, a post dam can be cut into the cast prior to
injecting. The wax pattern is also familiar and comfortable for the patient and provides a reference
to communicate to the laboratory, from which any and all changes are made predictably. The Celara
wax pattern is handled just like a wax rim. Base plate wax can be added to it, or it can be marked
and trimmed similar to a traditional rim.
Fig ure 19
Troubleshooting— Fabricating the Wax Pattern
• Avoid injecting too cool a temperature.
– This will result in a wavy wax pattern.
• Avoid injecting the wax too hot.
– This can result in excess shrinkage of the wax pattern.
• Avoid having the sprue hole too large.
– It will not make a seal in the inlet of the injector and the pattern may not fill with wax.
• Avoid having the inlet sprue hole too close to the ledge of the container.
– This will make it very difficult to place the container on the inlet of the wax injector.
• Avoid having the inlet sprue into the anterior teeth.
– The inlet sprue should enter the void above the anterior teeth in the anterior flange
of the denture. The anterior teeth and midline must be accurately represented in
the wax-pattern.
• Avoid injecting the alginate wet. Dry the alginate before injecting.
– The incisal edges of the anterior teeth will not be represented accurately if excessive
moisture is in the alginate.
• Avoid pumping the wax injector too vigorously — Pump very slowly and easily.
– This can shoot the wax out the exit sprue, which will make a mess and possibly
cause injury.
14
• Avoid removing the container from the inlet sprue of the container too quickly.
– Allow the wax to harden in the sprue before lifting the container off the inlet of the wax
injector. This prevents the wax from running out and creating a void in the pattern. The
resulting void will be in the distal of the pattern.
• Allow the wax pattern to adequately harden before removing it from the cast and
trimming to prevent distortion of the wax pattern.
Page 15

Sending the Container to the Laboratory to Have
the Laboratory Inject the Wax Pattern
In the event that only minor changes are necessary, the Celara™ Denture System enables the
dentist to send the container with the cast and the alginate to the laboratory for fabrication of the
wax pattern.
Make sure to seal the wax pattern to the cast when sending the Celara case to the laboratory.
Also include the alginate container in a tightly sealed bag. This gives the laboratory the option to
re-inject if they elect.
A small wet towel must be placed between the alginate and stone halves of the containers.
The containers must be secured together and placed in a tightly sealed bag. The Celara
alginate is specially formulated so that it will not shrink or distort for up to 96 hours if these
instructions are followed correctly.
If cleaning and disinfection of the alginate is required, use a disinfection process and technique
which does not cause distortion. Immediately after disinfection procedures, place the alginate
container back in a sealed bag. Celara alginate will not distort in a sealed bag, but will distort if left
out unsealed.
Figure 20: Pattern Only
You can request the laboratory to provide back a Celara Wax Pattern over a stabilized hard base, to
be used as a typical base plate and rim (Figure 20). Alternatively, you can request a complete setup for try-in over a stabilized hard base, providing the lab receives a bite from the impressions in
the mouth along with the mold and shade of the teeth (Figure 21. A partial set-up with anterior teeth
only can also be requested from the laboratory (Figure 22).
Figure 21: Complete Set-Up
Figure 22: Partial Set-Up
15
Page 16

Dental Products
49836
3M Center
Building 275-2SE-03
St. Paul, MN 55144-1000
U.S.A.
1-800-634-2249
Customer Care Center: 1-800-634-2249 www.3MESPE.com
Please recycle. Printed in U.S.A.
© 3M 2011. All rights reserved.
44-0007-4983-6-A
3M and ESPE are trademarks
of 3M or 3M ESPE AG.
Celara is a trademark of
Dentovations, Inc.
Manufactured by Dentovations Inc.
Boston, MA 02109 U.S.A.
 Loading...
Loading...