

Page 1
Page 2

The purpose of this booklet is to acquaint
the reader with the need and procedure for
examining the Larynx and Nasopharynx areas.
It will reveal the true nature of hoarseness,
and when regularly employed, the physician
can confidently diagnose and advise treatment or consultation early in the course of
a laryngeal disease. The early recognition of
laryngeal abnormalities permits conservative
therapy with maximum preservation of laryngeal tissue and the patient’s voice.
Indirect nasopharyngoscopy can also be sat-
isfactorily accomplished. It examines the back
of the nose, including the eustachian tubes,
for possible infections, blockages, tumors,
and adenoid tissue in children.
We wish to express our sincere appreciation to
Dr. Edwin W.
Department of Otolaryngology and
Surgery, University of Tennessee Center for the
Health Sciences, Memphis, Tennessee, for his
valuable assistance in the preparation of this
instructional booklet.
Cocke,
Jr., M.D., Clinical Professor,
Maxillofacial
Page 3
I
“I
advantages of the head mirror system and
may be employed with minimum difficulty.
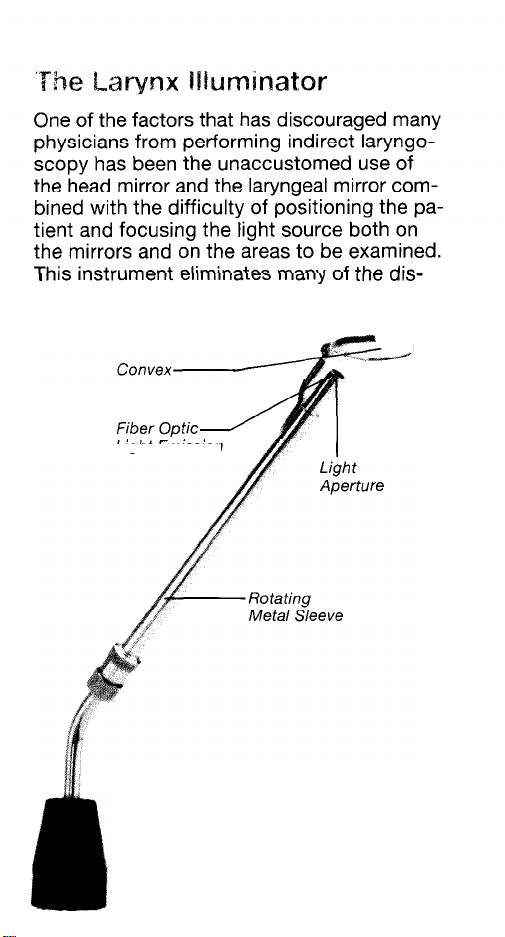
Mirror
Light Emission
Figure 1
Halogen Larynx Illuminator Light
passing through the aperture will
illuminate the palate and pharynx
to
assist in positioning the mirror.
The metal sleeve and mirror are
removable for sterilization.
Page 4
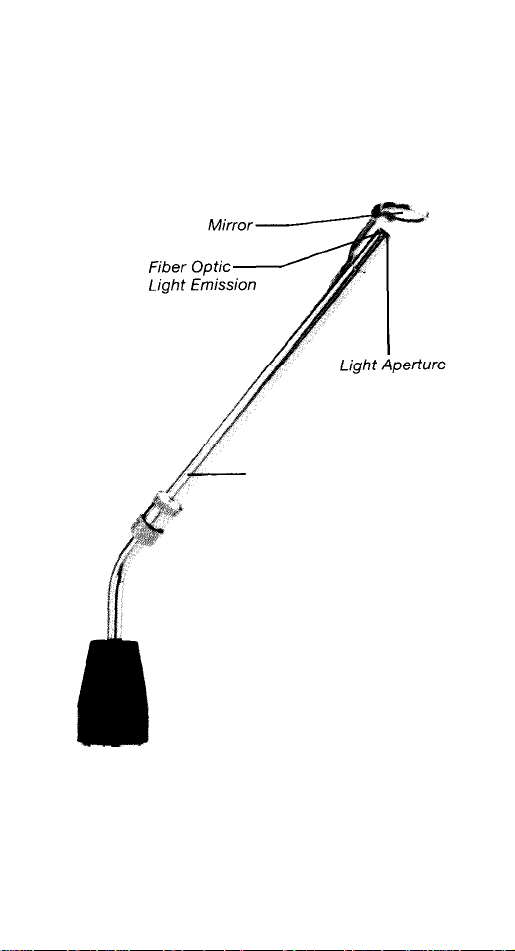
The Nasopharynx Illuminator
The nasopharyngeal mirror is identical to the
laryngeal mirror except that it is round and
smaller.
Rotating
Metal
Sleeve
Figure 2
Halogen Nasophatynx
Illuminator
Page 5

Laryngopharynx
(Hypopharynx)
Esophagus
Superior
turbinate
Sphenoid
Adenoids
Opening of
nasal
I
sinus
Figure 3
The pharynx has three divisions: the nasopharynx located between the base of the skull and the palate;
the oropharynx between the palate and base of the
tongue; and the laryngopharynx between the base
of the tongue and the esophagus.
Page 6

To successfully examine the laryngopharynx
with the illuminated Welch Allyn mirror, it is
desirable for the light in the examining area
to be subdued. The patient is reassured and
asked to breathe though his mouth. Sedation
may be required in apprehensive patients or
topical anesthesia to the palate and pharynx
in patients whose gag reflex is excessive.
The physician must employ the instrument
frequently enough to become proficient, to
establish a routine, to gain confidence, and
to become familiar with the normal anatomy
of the laryngopharynx. The following steps
will produce satisfactory results:
The examiner should sit to one side
1.
(patient’s left) or in front of the patient
to be examined.
The patient sits in a straight back chair
2.
with his hips firmly against the back rest,
trunk forward, head back, chin extended,
mouth open, and his tongue extended.
The Welch Allyn hand piece with attached
3.
laryngeal mirror is held in the examiner’s
right hand. The light switch is turned on
to illuminate the fiber optic light source.
A gauze square wrapped about the patient’s
4.
tongue facilitates holding it between thumb
and middle finger of the left hand while
the index finger elevates the upper lip. The
patient may be requested to hold his own
tongue while the examiner depresses it
with a tongue blade held in his left hand.
Page 7

5. The mirror is inserted into the mouth. Light
passing through the light aperture facili-
tates positioning the mirror so it passes
between the tonsils and elevates the soft
palate. The patient is encouraged to breathe
deeply through his mouth and relax. A topical anesthetic may be applied should there
be excessive gagging.
6. The reflected light in the mirror now illuminates the base of the tongue and the
laryngopharynx. A minor degree of rotation of the
laryngeal mirror assists in illuminating and
examining the various anatomical structures.
7. Variations in color, contour and motion of
each side of the larynx when compared
with identical structures of the opposite
side should arouse suspicion that an ab-
normality exists.
Figure 4
Reflected light in the mirror will illuminate the base of
the tongue and laryngopharynx
Page 8

of the right and left false vocal
vocal cords, anterior and posterior commissures. The mobility of each true cord
is then evaluated.
cords, true
Page 9

Indirect Nasopharyngoscopy
Indirect nasopharyngoscopy (posterior rhinoscopy)
is accomplished with the Nasopharynx
Illuminator. Of interest is the “vault” of the
nasopharynx and eustachian tubes, adenoid
tissue, polyps and tumors.
The following steps will produce satisfactory
examination results:
1.
The examiner should sit to one side (pa-
tient’s left) or in front of the patient to be
examined.
2. The Welch
nasopharyngeal mirror is held in the examiner’s right hand. The light switch is turned
on to illuminate the fiber optic light source.
3. Following depression of the tongue with a
tongue blade held in the left hand, the patient is asked to breathe simultaneously
through his nose and mouth. This relaxes
the soft palate.
4. The mirror is passed into the mouth along
the surface of the tongue blade, coming to
rest between the soft palate and the
ryngeal wall. Care should be taken to avoid
touching the tongue, pharynx or palate
with the mirror.
5. The handle of the mirror is depressed and
rotated from side to side so that succes-
sive parts of the nasopharynx may be
viewed.
6. Should excessive gagging ensue, topical
anesthesia should be applied.
Allyn
hand piece with attached
pha-
Page 10

Figure 5
Reflected light in the mirror
nose and nasopharynx.
will
illuminate the posterior
7. Should the space between the palate
and pharyngeal wall be too narrow for
examination, a soft palate retractor may
be required.
8. Variations in color and contour of each
side of the nasopharynx when compared
with identical structures of the opposite
side should arouse suspicion that an ab-
normality exists.
9. The various anatomical structures that may
be viewed include the eustachian tube
orifice, torus tubarius, fossa of
Rosen-
muller, adenoid, middle turbinate, inferior
turbinate and nasal septum.
Page 11

The instructions given in this manual are presented as a guide to successful laryngeal
and nasopharyngeal examinations. These
examinations should always be included in
a complete physical examination. In addition
to revealing the true nature of hoarseness,
the physician can confidently diagnose and
advise treatment or consultation in the earliest stages of disease. Early recognition of
abnormalities permits conservative therapy
with maximum preservation of tissue. When
used regularly and correctly, the Larynx Illuminator and Nasopharynx Illuminator can
serve as one of the physician’s most effective pieces of diagnostic equipment.
Page 12

 Loading...
Loading...