



AV-S Ventilator
Remote Display Module and Interface
for use with A200SPAbsorber
Service Manual
Partnership for Life
THE IMPORTANCE OF PATIENT MONITORING
WARNING
Anaesthetic systems have the capability to deliver mixtures of gases and vapours to the patient which could cause injury or death unless controlled by a qualified anaesthetist.
There can be considerable variation in the effect of anaesthetic drugs on individual patients so that the setting and observation of control levels on the anaesthesia systems does not in itself ensure total patient safety.
Anaesthesia system monitors and patient monitors are very desirable aids for the anaesthetist but are not true clinical monitors as the condition of the patient is also dependent on his respiration and the functioning of his cardio-vascular system.
IT IS ESSENTIAL THAT THESE ELEMENTS ARE MONITORED FREQUENTLY AND REGULARLY AND THAT ANY OBSERVATIONS ARE GIVEN PRECEDENCE OVER MACHINE CONTROL PARAMETERS IN JUDGING THE STATE OF A CLINICAL PROCEDURE.

IMPORTANT
Servicing and Repairs
In order to ensure the full operational life of this ventilator, servicing by a Penlon-trained engineer should be undertaken periodically.
The ventilator must be serviced to the following schedule:
(a)Six monthly service - inspection and function testing.
(b)Annual / two year / four year services - inspection and function testing, and component replacement.
Details of these operations are given in this Manual for the AV-S, available only for Penlon trained engineers.
For any enquiry regarding the servicing or repair of this product, contact the nearest accredited Penlon agent:
or communicate directly with:
Technical Support
Penlon Limited
Abingdon Science Park
Barton Lane
Abingdon
OX14 3PH
UK
Tel: |
44 (0) 1235 547076 |
Fax: |
44 (0) 1235 547062 |
E-mail: technicalsupport@penlon.co.uk
Always give as much of the following information as possible:
1.Type of equipment
2.Product name
3.Serial number
4.Approximate date of purchase
5.Apparent fault
(i)

FOREWORD
This manual has been produced to provide authorised personnel with information on the function, routine performance, service and maintenance applicable to the AV-S Anaesthesia Ventilator.
Information contained in this manual is correct at the date of publication.
The policy of Penlon Limited is one of continued improvement to its products.
Because of this policy, Penlon Limited reserves the right to make any changes which may affect instructions in this manual, without giving prior notice.
Personnel must make themselves familiar with the contents of this manual and the machine’s function before servicing the apparatus.
Copyright © Penlon Limited, 2008.
All rights reserved.
(ii)

CONTENTS
|
|
Page No. |
|
USER RESPONSIBILITY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
1 |
1. |
WARNINGS AND CAUTIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
2 |
2. |
PURPOSE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
7 |
3.DESCRIPTION
3.1 |
General . . . . . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
8 |
3.2 |
Ventilation Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . |
10 |
|
3.3 |
Pneumatic System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
13 |
|
3.3.1 |
System Operation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . |
13 |
|
3.4 |
Electrical System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
14 |
|
3.5 |
Control Panel |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
15 |
3.5.1 |
Touchscreen Operation and Navigator wheel / push-button . . . . . . . . |
. . . . |
15 |
|
3.5.2 |
User Adjustable Parameters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . |
16 |
|
3.5.3 |
Operational capability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
17 |
|
3.5.4 |
Output Compensation Functions . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
18 |
|
3.6 |
Interface with Prima SP and A200SP . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
19 |
|
3.7 |
Ventilation Modes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . |
20 |
|
3.7.1 |
Standby Mode . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . |
20 |
3.7.2 |
Volume Mode . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . |
21 |
3.7.3 |
Pressure Mode |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
22 |
3.7.4 |
Spontaneous Mode . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . |
23 |
|
3.7.5 |
Advanced Spontaneous Breathing Modes . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
24 |
|
3.7.5.1 |
SIMV (Synchronised Intermittent Mandatory Ventilation) . . . . . . . . . |
. . . . |
24 |
|
3.7.5.2 |
SMMV (Synchronised Mandatory Minute Ventilation) . . . . . . . . . . . |
. |
25 |
|
3.7.5.3 |
PSV (Pressure Supported Ventilation) . . . . . . . . . . . . . . . . . . . . |
. . |
26 |
|
3.7.5.4 PEEP ( Positive End Expiratory Pressure) . . . . . . . . . . . . . . . . . . . . |
. . |
27 |
||
3.8 |
On-screen Menus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . . |
28 |
|
3.9 |
Spirometry . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
29 |
3.10 |
Display Waveforms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
29 |
|
3.11 |
Alarms . . . . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
30 |
|
3.12 |
Oxygen Monitor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
31 |
|
3.13.1 |
System Operation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . |
31 |
|
3.12.2 |
The MOX-3 Oxygen Sensor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
31 |
|
3.12.3 |
Menus . . . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
32 |
3.12.4 |
Display . . . . . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
33 |
|
3.12.5 |
Alarms . . . . . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
33 |
|
3.12.6 |
Alarm Mute. . . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
33 |
|
4. |
SPECIFICATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
34 |
|
|
Ventilator . . . . |
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . |
34 |
|
Oxygen Monitor . |
.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
37 |
(iii)

CONTENTS
5.PRE-OPERATION PROCEDURES
5.1 |
Ventilator Set-up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
39 |
5.1.1 |
Mounting the Ventilator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
39 |
5.1.2 |
Electrical Power Connections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
39 |
5.1.3 |
Ventilator Gas Supply . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
39 |
5.1.4 |
Breathing System Schematic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
39 |
5.1.5 |
Bellows Drive Gas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
43 |
5.1.6 |
Anaesthetic Gas Scavenging System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
43 |
5.1.7 |
Remote Screen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
43 |
5.1.8 |
Printer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
43 |
5.1.9 |
Breathing System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
44 |
5.1.10 |
Spirometer Connections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
44 |
5.1.11 |
Pressure Monitor Connections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
46 |
5.1.12 |
Bellows Assembly . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
47 |
5.2 |
Pre-use Checklists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
48 |
5.2.1 |
Daily Checklist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
48 |
5.2.2 |
Function Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
49 |
5.2.3 |
Weekly Checklist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
50 |
5.3 |
Oxygen Monitor Set-up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
51 |
5.3.1 |
Installation . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
51 |
5.3.2 |
Calibration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
51 |
5.3.3 |
Sensor Low Indication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
53 |
5.3.4 |
Setting the High and Low O2 Alarms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
53 |
6.SERVICE PROCEDURES
6.1 |
Service Intervals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
54 |
6.2 |
Control Unit Patient Block Removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
55 |
6.3 |
Valve Calibration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
56 |
7.SERVICE SCHEDULE
|
Service Schedule . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
57 |
8. |
PARTS LISTS |
|
|
|
Preventive Maintenance Kits . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
66 |
|
Assemblies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
67 |
9.APPENDIX
1. |
Back-up Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . 78 |
|
2. |
Menu System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . . |
79 |
3. |
Ventilator Spirometry System . . . . . . . . . . . . . . . . . . . . . . . . . . |
. . . . |
82 |
4. |
Cleaning / Sterilisation / Oxygen sensor replacement . . . . . . . . . . . |
. . . . . . |
85 |
5. |
Software Upgrade Installation Procedure . . . . . . . . . . . . . . . . . . |
. . . . . . . |
89 |
6. |
Calibration and Output Checks for a New Ventilator . . . . . . . . . . . . |
. . . . . . . |
90 |
7. |
Menu structure amendments (v1.86.01 / .02 / .04) . . . . . . . . . . . . . |
. . . . . . . |
94 |
(iv)

USER RESPONSIBILITY
This anaesthesia ventilator has been built to conform with the specification and operating procedures stated in this manual and/or accompanying labels and notices when checked, assembled, operated, maintained and serviced in accordance with these instructions.
To ensure the safety of this device it must be checked and serviced to at least the minimum standards laid out in this manual. A defective, or suspected defective, product must not under any circumstances be used.
The user must accept responsibility for any malfunction which results from noncompliance with the servicing requirements detailed in this manual.
Additionally, the user must accept responsibility for any malfunction which may result from misuse of any kind or noncompliance with other requirements detailed in this manual.
Worn, broken, distorted, contaminated or missing components must be replaced immediately. Should such a repair become necessary it is recommended that a request for service advice be made to the nearest Penlon accredited agent.
This device and any of its constituent parts must be repaired only in accordance with written instructions issued by Penlon Limited and must not be altered or modified in any way without the written approval of
Penlon Limited. The user of this equipment shall have the sole responsibility for any malfunction which results from improper use, maintenance, repair, damage or alteration by anyone other than Penlon or its appointed agents.
USA and Canadian Federal Law restricts the sale and use of this device to, or on the order of, a licensed practitioner.
Statements in this manual preceded by the following words are of special significance:
WARNING |
means there is a |
|
possibility of injury to the |
|
user or others. |
CAUTION |
means there is a possibility |
|
of damage to the apparatus |
|
or other property. |
NOTE |
indicates points of |
|
particular interest for more |
|
efficient and convenient |
|
operation. |
Always take particular notice of the warnings, cautions and notes provided throughout this manual.
1

1. WARNINGS AND CAUTIONS
The following WARNINGS and CAUTIONS must be read and understood before using this ventilator.
WARNINGS
General Information
1.Personnel must make themselves familiar with the contents of this manual and the machine’s function before using the ventilator.
Before Using the Ventilator
2.Before the ventilator is used clinically for the first time, verify that the hospital engineering department has carried out an earth continuity test.
3.Excessive electronic noise caused by other poorly regulated devices, such as an electrocautery unit, may adversely interfere with the proper functioning of the ventilator.
To avoid this problem, do not connect the ventilator’s power cord into the same electrical wall outlet or adaptor strip into which an electrocautery unit is connected.
4.If used with a mains extension cord, the unit may be subject to electro-magnetic interference.
5.The driving gas supply must be clean and dry to prevent ventilator malfunction.
6.This ventilator is designed to be driven by oxygen or medical air only. The drive gas is set during manufacture and the ventilator is calibrated for that gas.
Before the ventilator is used clinically for the first time, the commissioning engineer must confirm that the air/oxygen selection is set correctly for the drive gas that is to be used.
The use of any other gas will cause inaccurate operation and may damage the ventilator, resulting in potential injury to the patient.
7.The driving gas is discharged through the opening in the back of the ventilator control unit.
The discharged gas may contaminate the environment, and should therefore be extracted using a gas scavenging system.
8.The bellows can only support approximately 1 kPa (10 cmH2O) differential positive pressure, above which it may be dislodged from the mounting ring, resulting in dangerous malfunction of the ventilator.
Do not connect a positive end expiratory pressure (PEEP) valve or other restrictive device to the exhaust port on the bellows base.
This would increase the pressure inside the bellows and the bellows could detach from the base, causing serious malfunction.
9.Breathing System
The breathing system which conveys gases from the anaesthetic machine to the patient, and disposes of expired gases, must conform to the requirements of ISO 8835-2.
Because breathing systems require frequent cleaning and disinfection they are not a permanent part of the anaesthetic ventilator and therefore cannot be directly under the control of the anaesthetic ventilator manufacturer. However, we strongly recommend that only breathing systems which have been approved and authorised by the manufacturer for use with AV-S should be employed.
Do not use conductive breathing system hoses.
When mechanical ventilation is employed the patient breathing system must be connected directly to a pressure relief valve to prevent the possibility of barotrauma.
10.The spirometer sensors are mounted within the A200SP absorber. Do not fit a spirometer sensor to any other location. The device will not measure exhaled volumes in any other position.
2

WARNINGS AND CAUTIONS
11.The operation of each alarm function should be verified daily.
Periodically check the alarms at clinically suitable intervals. If the audible alarm or the visual indicator of any alarm function fails to activate during any alarm condition or fails to reset after the alarm has been cleared, refer the unit to an authorised service technician.
12.Before using the ventilator check that all connections are correct, and verify that there are no leaks.
Patient circuit disconnects are a hazard to the patient. Extreme care should be taken to prevent such occurrences.
It is recommended that Safelock fittings are used throughout the breathing circuit.
13.Check that the cable between the control unit and remote display screen unit is connected before use.
Always use a cable type recommended by the manufacturer.
Using the Ventilator
14.The AV-S ventilator is not intended for use in intensive care applications.
15.This apparatus must not be used with, or in close proximity to, flammable anaesthetic agents.
There is a possible fire or explosion hazard.
16.Anaesthesia apparatus must be connected to an anaesthetic gas scavenging system (AGSS) to dispose of waste gas and prevent possible health hazards to operating room staff. This requirement must be observed during test procedures as well as during use with a patient.
The scavenging transfer and receiver system must conform to ISO 8835-3. Any problem arising from an improperly functioning scavenging system is solely the user’s responsibility.
Do not use a scavenging system that restricts drive gas flow when negative pressure is exerted on it.
17.When the ventilator is connected to a patient, it is recommended that a qualified practitioner is in attendance at all times to react to an alarm or other indication of a problem.
18.In compliance with good anaesthesia practice, an alternative means of ventilation must be available whenever the ventilator is in use.
19.It is recommended that the patient oxygen concentration should be monitored continuously.
20.If the drive gas supply pressure drops below a nominal 241 kPa (35 psi), the LOW DRIVE GAS SUPPLY alarm will activate both audibly and visually. Patient minute volume may be reduced due to lowered flow rates
21.An audible alarm indicates an anomalous condition and should never go unheeded.
22.The characteristics of the breathing circuit connected between the ventilator and the patient can modify or change patient ventilation.
To assist the maintenance of the delivered patient tidal volume, the ventilator control system software includes:
A)a compliance compensation algorithm,
B)a fresh gas compensation algorithm.
However, patient ventilation must be monitored independently from the ventilator.
It is the responsibility of the user to monitor patient ventilation.
23.Care must be taken to ensure that the flow sensors are connected correctly to the inspiratory and expiratory ports of the absorber.
24.The Vent Inop (ventilator inoperative) alarm indicates that one of the following conditions has occurred:
a)The drive gas solenoid has failed.
b)The flow control valve has failed.
c)Internal electronic fault.
d)Internal electrical fault.
e)Software error.
3

WARNINGS AND CAUTIONS
Note that if a ventilator error is detected, ‘Ventilator Inoperative’ will be displayed on the front control panel display.
25.The High and Low Airway Pressure Alarms are important for patient care. It is important that the sensor is properly located in the expiratory limb of the circuit - refer to section 5.1.10.
26.The patient must be continuously attended and monitored when Advanced Breathing Modes are in use.
User Maintenance
Control Unit
27.Opening the control unit by unauthorised personnel automatically voids all warranties and specifications.
Prevention of tampering with the control unit is exclusively the user’s responsibility. If the control unit seal is broken, the manufacturer assumes no liability for any malfunction or failure of the ventilator.
28.For continued protection against fire hazards, replace the two fuses only with the identical type and rating of fuse.
See section 4 for fuse rating.
29.If the internal battery is fully discharged, the ventilator will not function in the event of mains power failure. The battery must be recharged before the ventilator is used clinically, otherwise backup cannot be guaranteed.
See Appendix for battery maintenance. See also CAUTION No. 7.
Used or defective batteries must be disposed of according to hospital, local, state, and federal regulations.
30.No oil, grease or other flammable lubricant or sealant must be used on any part of the ventilator in close proximity to medical gas distribution components.
There is a risk of fire or explosion.
31.Exterior panels must not be removed by unauthorised personnel and the apparatus must not be operated with such panels missing.
There is a possible electric shock hazard.
Bellows Assembly
32.The valve seat on the patient gas exhalation diaphragm valve in the base of the bellows assembly must be cleaned regularly. Note that the bellows assembly is built into the A200SP Absorber - please refer to User Manual for this product.
Failure to keep the valve seat clean could result in the diaphragm sticking, thus preventing exhalation.
Great care must be taken not to damage the precision surface of the valve seat on the patient gas exhalation diaphragm valve in the base of the bellows assembly.
Never use any hard object or abrasive detergent to clean it; use only a soft cloth.
If the valve seat is damaged, the valve will leak and may cause serious ventilator malfunction.
4
WARNINGS AND CAUTIONS
CAUTIONS
1.Do not sterilise the ventilator control unit. The patient block assembly must be removed from the control unit before sterilisation ( see section 6.2.5).
All other internal components are not compatible with sterilisation techniques and damage may result.
2.For ventilator components which require
sterilisation, peak sterilisation temperatures should not exceed 134oC (275oF) to prevent possible damage.
(See section 6).
3.Care must be taken not to let any liquid run into the control unit; serious damage may result.
4.The exhalation valve located in the bellows base assembly and the paediatric bellows adaptor must be cleaned and sterilised separately. Note that the bellows assembly is built into the A200SP Absorber - please refer to User Manual for this product.
5.Always check for correct fitment, and carry out a full function test before clinical use, if the bellows has been removed and refitted for any reason. See section 6. Note that the bellows assembly is built into the A200SP Absorber - please refer to User Manual for this product.
6.Damage may occur to the battery if it is allowed to remain in a discharged state. Check the battery frequently if the ventilator is in storage (see Appendix 1).
7.Fresh gas compensation is disabled if :
a)The spirometry system is turned OFF through the menu system, or
b)The spirometry system is not functioning correctly.
8.Fresh gas mixture compensation is disabled if :
a)The spirometry system is turned OFF through the menu system, or
b)The spirometry system is not functioning correctly.
c)The O2 monitor is switched OFF.
9.Circuit compliance is not activated until Fresh Gas Compensation is switched OFF.
NOTES
1.The term ‘cycle’ is used to designate the transition to the exhalation phase.
2.The term ‘trigger’ is used to indicate the transition to the inhalation phase.
5

WARNINGS AND CAUTIONS - Oxygen Monitor
Oxygen Monitor
Note that the sensor for the oxygen monitor is built into the A200SP Absorber - for additional information, please refer to the A200SP User Manual.
WARNINGS
1.We recommend calibration of the oxygen monitor every time the system is turned on, as a safety precaution.
2.Do not attempt to open the fuel cell. The sensor contains small quantities of :
a)electrolyte, classified as a harmful irritant which is potentially hazardous, and
b)lead.
Used or defective cells must be disposed of according to hospital, local, state, and federal regulations.
3.ALWAYS check the integrity of the sensor assembly before use.
4.Once exhausted, the sensor must be disposed of according to hospital, local, state and federal regulations.
5.The sensor measures oxygen partial pressure, and its output will rise and fall due to pressure change.
An increase in pressure of 10% at the sensor inlet will produce a 10% increase in sensor output.
6.The oxygen sensor is not suitable for sterilisation.
If contamination is suspected, fit a new sensor (see section 6.4) and dispose of the contaminated unit according to hospital, local, state and federal regulations.
CAUTIONS
1.Do not sterilise any oxygen monitor component.
2.Do not autoclave or expose the sensor to high temperatures.
3.If the sensor shows signs of being affected by condensation, dry the sensor with soft tissue.
Do not use heat to dry the sensor.
NOTES
1.The O2 SENSOR FAULT alarm indicates that one of the following conditions has occurred.
a)Internal electrical fault
b)Software/electronics fault
c)Oxygen sensor fault.
2.The concentration read-out may, in certain conditions of excess pressure, show a value above 100%.
To accommodate these conditions it is possible to set the high alarm value up to 105% (see section 5).
3.To maintain maximum sensor life:
i)always switch off the anaesthetic machine after use, to ensure that the basal flow ceases.
ii)disconnect the breathing circuit after use.
4.The accuracy of flow and volume measurements may be reduced if the oxygen monitor is not in use.
5.Fresh gas mixture compensation is disabled if the oxygen monitor is switched OFF.
6

2. PURPOSE
The AV-S Ventilator is a software controlled, multi-mode ventilator, designed for
mechanical |
ventilation |
of adult and |
paediatric |
patients |
under general |
anaesthesia. |
|
|
In addition, in spontaneous mode, it can be used to monitor spontaneously breathing patients
It is designed for use in closed-circuit anaesthesia.
Indications for use of the device:
The AV-S Ventilator is intended to provide continuous mechanical ventilatory support during anaesthesia. The ventilator is a restricted medical device intended for use by qualified trained personnel under the direction of a physician. Specifically the ventilator is applicable for adult and paediatric patients.
The ventilator is intended for use by health care providers, i.e. Physicians, Nurses and Technicians with patients during general anaesthesia.
The AV-S ventilator is not intended for use in intensive care applications.
Oxygen Monitor
The Oxygen Monitor is intended to continuously measure and display the concentration of oxygen in breathing gas mixtures used in anaesthesia, and is intended for adult and paediatric patients.
The oxygen monitor is an integral part of the ventilator.
The oxygen monitor is intended for use by health care providers, i.e. Physicians, Nurses and Technicians for use with patients during general anaesthesia.
7
3. DESCRIPTION
3.1General Description
The AV-S Ventilator is a pneumatically driven, software controlled, multi-mode ventilator.
The ventilator is a time-cycled, volume/pressure controlled, and pressure limited.
The ventilator has compliance compensation and a user selectable option of an inspiratory pause fixed at 25% of the inspiratory time.
In addition, fresh gas compensation and user selectable gas mixture compensation is a standard feature.
Ventilation Modes
Volume Mode - continuous mandatory ventilation Pressure Mode - pressure controlled ventilation Spontaneous, with advanced patient support - SIMV, SMMV, PSV, PEEP
Patient Monitoring
Airway pressure, measured from the expiratory limb of the breathing circuit.
Tidal Volume and Minute Volume measurement is provided by a dual spirometry system
An integral oxygen monitor system measures oxygen concentration in the breathing circuit inspiratory limb.
The print function provides a permanent record of function activity for up to eight hours during a procedure, or can be used to record waveforms.
Screen
Remote, arm-mounted, 210 mm (8.4 inch) high definition, colour TFT screen, with single/dual waveform display.
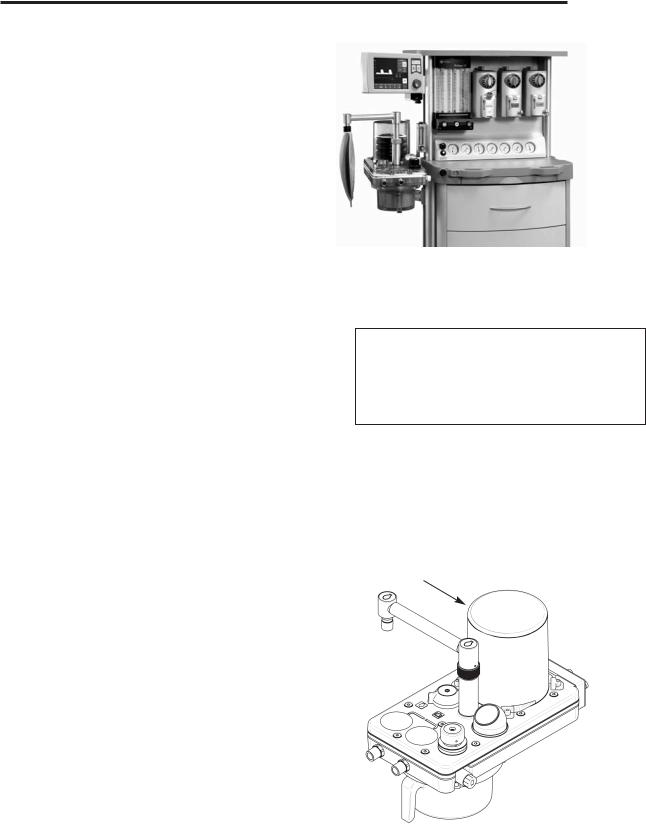
Bellows unit
The bellows unit (1) is built into the A200SP absorber. A paediatric bellows assembly is available as an option
Drive gas supply
The drive gas supply can be oxygen or air.
The supply must be at 310 to 689 kPa (45 to 100 psi).
Note that the drive gas is specified by the customer, and set during manufacture. Conversion from one drive gas to another must only be carried out by an authorised service engineer trained by the manufacturer.
AV-S Ventilator
Spontaneous Mode Patient Support
SIMV - Synchronised Intermittent Mandatory Ventilation
SMMV - Synchronised Mandatory Minute Ventilation
PSV - Pressure Supported Ventilation
PEEP - Positive End Expiratory Pressure
1
8
DESCRIPTION
5 |
6 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
3 |
7 |
2 |
1 |
|
|||
|
|
|
4
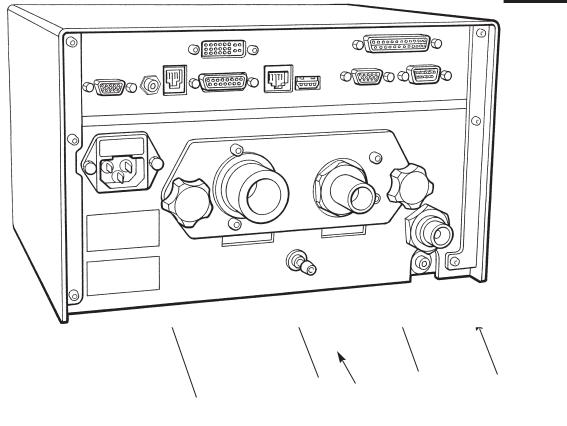
Control Unit
Rear Panel
Gas Connections
1.Ventilator drive gas inlet
-connect to anaesthetic machine auxiliary gas outlet
2.Bellows Drive Gas Output
-connect to bellows via A200SP absorber - see section 5.1.5
3.Outlet - Exhaust Valve
-connect to scavenge system - see section 5.1.6
Electrical Connection
4.Electrical mains input and fuse unit
Interface and Parameter inputs
5.A200SP Absorber Bag/Vent switch interface, and Spirometer connector
6.Prima SP2 Interface connector - (SP2 primary on/off switch)
7.Pressure Monitor Port
8.Input socket - Oxygen monitor sensor
Data and Printer Ports
9.Data Output
10.Output to remote display
11.Ethernet
12.USB
13.VGA
14.Printer port
15.RS232 (manufacturer’s use only)
NOTE
USB port is for access only by engineers trained by the manufacturer.
All other data ports are read only.
For further information, please contact your distributor’s service department, or the manufacturer.
9
DESCRIPTION
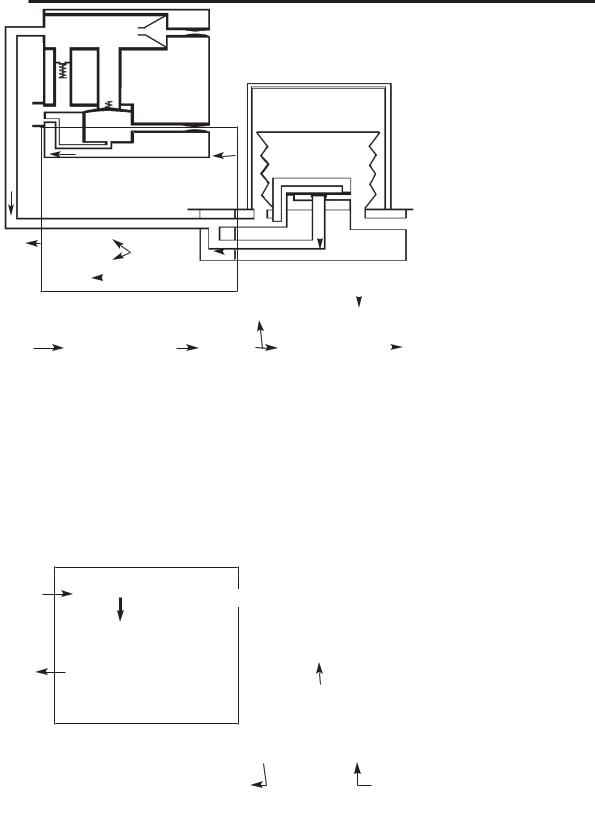
3.2Ventilation Cycle
This section provides a simplified description of the ventilation cycle.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
Inspiratory Phase |
|
|
|
|
1 |
|
|
|
|
|
|
|
|
The drive gas proportional |
||
|
|
|
|
|
|
|
|
|
|
|
|
valve (1) in the control unit |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
opens. |
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
Drive gas is delivered to the |
||
|
|
|
|
|
|
|
|
|
|
|
|
bellows housing (2). |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The |
patient proportional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
valve (3) opens, and gas |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
3 |
|
|
5 |
|
|
|
flows through the bleed |
||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
valve. The back pressure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ensures that the exhaust |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
valve (4) is kept closed. |
|
|
|
2 |
|
|
|
|
|
6 |
|
|
|
||||
|
|
|
|
|
|
|
|
|
Drive gas pressure builds |
||||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
7 |
up above the bellows (5), |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
which starts to move down. The diaphragm (6) in the bellows assembly base is held closed, and patient gas is forced out of the bellows base (7) into the breathing system.
2. Beginning of
Expiratory Phase
The drive gas proportional valve (1) closes.
The patient proportional valve (3) closes.
The exhaust valve (4) opens. Patient gas returns to the bellows (5).
As the bellows rises, redundant drive gas is pushed out through the exhaust valve.
10
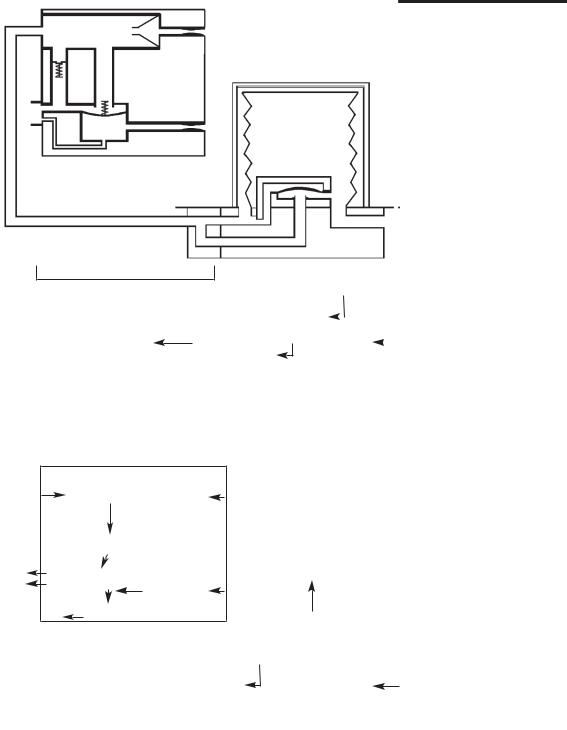
DESCRIPTION
|
|
3. |
End of |
|
||||
|
|
|
|
|
|
Expiratory Phase |
||
|
|
|
|
|
With the bellows at the top |
|||
|
|
|
|
|
of its housing fresh gas |
|||
|
|
|||||||
|
|
|
|
|
continues to flow. |
|
||
5 |
|
|||||||
|
|
|
To prevent a high pressure |
|||||
|
|
|
|
|
||||
|
|
|
|
|
build |
up |
the |
exhalation |
|
|
|
|
|
diaphragm |
(6) |
lifts and |
|
|
|
|
||||||
|
|
|
|
|
allows gas to exit through |
|||
|
|
|
|
|
the exhaust valve (4). |
|||
4. PEEP Positive End Expiratory Pressure
(user selectable)
The patient proportional valve (3) applies PEEP pressure plus 20 cmH2O to the exhaust valve, which
5
remains closed at this stage. As fresh gas flows in the patient circuit, any pressure increase above PEEP pressure in the bellows (5) will cause gas to bleed past the exhaust valve (4).
If there is a fall in pressure in the breathing circuit, the continuous flow from the drive gas proportional valve
(1) helps maintain the set PEEP pressure.
11
DESCRIPTION |
|
|
||
A |
|
|
|
Pneumatic Flow |
|
|
|
Diagram |
|
|
|
|
|
|
|
1 |
3 to 7 bar |
|
|
|
2 |
|
|
|
|
|
3 241 kPa (35 psi) |
|
|
|
4 |
|
|
|
|
5 |
6 |
|
|
|
|
|
0 - 80 cmH2O |
|
B |
7 |
8 |
14 |
C |
|
|
|||
|
|
9 |
|
|
|
10 |
12 |
|
|
|
|
|
|
|
|
11 |
|
15 |
|
|
0 - 90 cmH2O |
13 |
|
|
|
|
|
|
|
|
|
|
|
16 |
|
|
|
|
100 cmH2O |
|
|
|
17 |
18 |
12

DESCRIPTION
3.3 Pneumatic System
3.3.1System Operation
Refer to the pneumatic system diagram on the previous page.
A) Gas inlet manifold block
The AV-S Ventilator is designed to operate on a 310 - 689 kPa (45 -100 psi) drive gas supply (oxygen or air - to customer’s requirement).
1.DISS Connector
The gas source is connected to the DRIVE GAS SUPPLY fitting on the rear of the ventilator control unit.
The gas supply should be capable of a flow rate of 80 L/min while maintaining a minimum pressure in excess of 310 kPa (45 psi).
2.Filter
The drive gas is filtered with a 40-micron Input Gas Filter which protects the pneumatic components from incoming particulate matter.
3.The Low Supply Pressure Detector
The pressure switch is set at a predetermined level to detect a loss or reduction of the input gas source pressure.
When the pressure falls below 235 kPa (35 psi ± 1 psi), the LOW SUPPLY PRESSURE indicator will be displayed and the high priority audible alarm will activate.
4.Input Pressure Regulator
Regulates the input drive gas to 260 kPa ± 21 kPa (38 psi ± 3 psi).
5.Cut-off Valve
The valve isolates the the gas supply :
a)when the ventilator is switched off
b)when a fault condition occurs.
6.Airway Pressure Sensor
Connected to expiratory limb of breathing circuit.
B) Pneumatic Control Manifold Block
7.Drive Gas Proportional Valve
8.Drive Gas Flow Sensor
9.Drive Gas Pressure Sensor
10.Low Pressure Regulator
11.Patient Proportional Valve
12.PEEP pressure sensor
13.Restrictor
The restrictor allows a flow of up to 2 L/min (<2 L/min bleeding)
C) Exhaust Manifold Block
14.Check Valve
15.Diaphragm Valve
16.Pressure Relief valve - Set to 100 cmH2O
17.Exhaust Port ( to AGSS)
18.Bellows drive gas outlet (to bellows assembly)
13

DESCRIPTION
3.4Electrical System
Mains Supply
The mains supply inlet is designed for connection to any mains voltage from 100 to 240 VAC and a frequency of 50 to 60 Hz, without any adjustment.
The connector is a standard IEC type.
Back-up Battery
In the event of mains electrical failure, the backup battery cuts in automatically.
Standard battery:
A fully charged battery will power the ventilator for approximately 30 minutes.
High-power battery (option):
A fully charged battery will power the ventilator for approximately one hour.
See Appendix for battery care procedures.
14
DESCRIPTION
|
|
|
|
|
|
|
|
|
|
Gas Mixture |
|||||
cm H2O |
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
O2 + air |
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
%O2 |
100 |
|
|
SMMV |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
33 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Freeze |
|
Trigger |
|||
|
|
|
|
|
|
|
|
|
|
|
cmH2O |
||||
|
|
|
|
|
|
|
|
|
|
Waveform |
|
||||
|
|
|
|
|
|
|
|
|
|
|
-1.0 |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pmax |
Pmean |
|
|
|||
|
|
|
|
|
|
|
|
|
cmH2O |
cmH2O |
|
|
|||
|
|
|
|
|
|
|
|
|
24 |
10 |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spont |
|
|
|
|
|
|
|
secs |
|
|
|
|
|
|
Mode |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vm SET |
Vm MEAS |
SET |
Insp Time |
PEEP |
LIMIT |
|
|
|
|
Standby |
||||
|
|
Litres |
Litres |
BPM |
Sec |
cmH2O |
cmH2O |
|
|
|
|
||||
|
3.6 |
|
3.6 |
6 |
2 |
5 |
38 |
|
|
|
|
|
|||
 Touchscreen control
Touchscreen control
3.5Control Panel
3.5.1Touchscreen and Navigator Wheel / Push Button
3.5.1.1 Control Panel
1.On/Off control
Switch On:
Short internal test sequence
Switch Off:
Power down sequence with progress indicator
2.Status indicators for electrical power
(mains/battery supply)
Yellow indicator - illuminated whenever power is applied to the unit and internal battery is being charged
Green indicator - illuminates when the unit is switched on
3.Menu switch
The menu function provides access to user and service pages, including alarm settings.
4.Alarm mute switch
30 second or 120 second alarm silence, depending on alarm status.
Note also that some alarms are not mutable (see 3.11).
5.Navigator Wheel and Press Button
Turn the wheel to select a function or parameter, or to alter the value of an active parameter.
Press to confirm the setting.
AV-S
o IO
.
o .
2
1
4
3
5
15

DESCRIPTION
3.5.1.2 Selecting Functions and Parameters
The functions/parameters shown on the screen can be activated as follows:
a)touch the screen at the appropriate tab area.
b)rotate the navigator wheel and press it when the indicator arrow is on the required parameter tab
Note that parameters default to factory-set values when the ventilator is switched on and no further user selection is made.
3.5.2User Adjustable Parameters
Variable parameters can be altered by rotating the navigator wheel.
When the required value is displayed, press the active tab or the wheel to confirm the setting.
Tidal Volume Range |
20-1600 ml |
Rate |
4-100 bpm |
I:E Ratio |
1:0.3 to 1:8 |
PEEP |
4-20 cmH2O |
|
Can be set to OFF |
Pressure Limit |
|
Volume mode: |
10-80 cmH2O |
Pressure mode: |
10-50 cmH2O |
Alarm limits (user adjustable alarms only - see 3.11)
16
DESCRIPTION
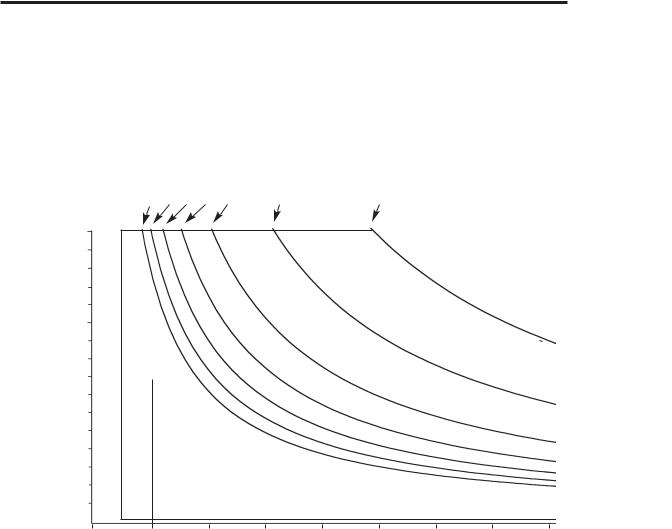
3.5.3Operational Capability
Tidal Volume, Rate, and I:E ratio settings are all limited by a maximum inspiratory flow of 75 L/min.
Tidal
Volume (litres) (Vt)
I:E Ratio
1:6 |
1:5 |
1:4 1:3 |
1:2 |
1:1 |
1:0.3 |
1.6
1.5
1.4
1.3
1.2
1.1
1.0
0.9
0.8
 X
X
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0 |
10 |
20 |
30 |
40 |
50 |
60 |
70 |
80 |
Rate (bpm)
The ventilator is capable of operating at the volumes and rates below each I:E ratio curve.
Example
1.Select required volume (Vt) (e.g. 0.8 L)
2.Select rate (e.g. 10 bpm).
3.Select I:E ratio of 1:2.
The point X on the graph lies beneath the 1:2 ratio curve, and is therefore within the ventilator’s capability.
17

DESCRIPTION
3.5.4Output Compensation Functions
WARNING
The AV-S automatically compensates for fresh gas (spirometry On), fresh gas mixture (spirometry and oxygen monitor On), and altitude.
However, the actual tidal volume delivered to the patient may be different to the ventilation parameters set by the user, due to:
A)an extreme compliance condition,
B)a substantial system leak,
C)patient circuit pressure effects, or
D)extreme fresh gas flows
In addition, high fresh gas flows will lead to an increased Vt being delivered to the patient.
The patient must be monitored independently from the ventilator.
It is the responsibility of the user to monitor the patient for adequate ventilation.
Fresh Gas Compensation
Adjusts delivered volume up to 60%
An alarm is triggered if the measured volume varies by 50% from the set volume.
This function is user adjustable
NOTE
Fresh gas compensation is disabled if :
a)The spirometry system is turned OFF through the menu system, or
b)The spirometry system is not functioning correctly.
Fresh Gas Mixture Compensation - models with Spirometry
The spirometry system compensates for fresh gas mixture - the user must access the menu system and select the gas mixture that will be used for each clinical procedure.
NOTE
Fresh gas mixture compensation is disabled if :
a)The spirometry system is turned OFF through the menu system, or
b)The spirometry system is not functioning correctly.
If the O2 monitor is switched OFF, a 40% / 60% mixture of O2/N2O is assumed.
Altitude Compensation
This function monitors ambient pressure, and adjusts the delivered volume accordingly
NOTE Altitude compensation is automatically applied during calibration of the oxygen monitor - see section 5.3.2.
18
DESCRIPTION
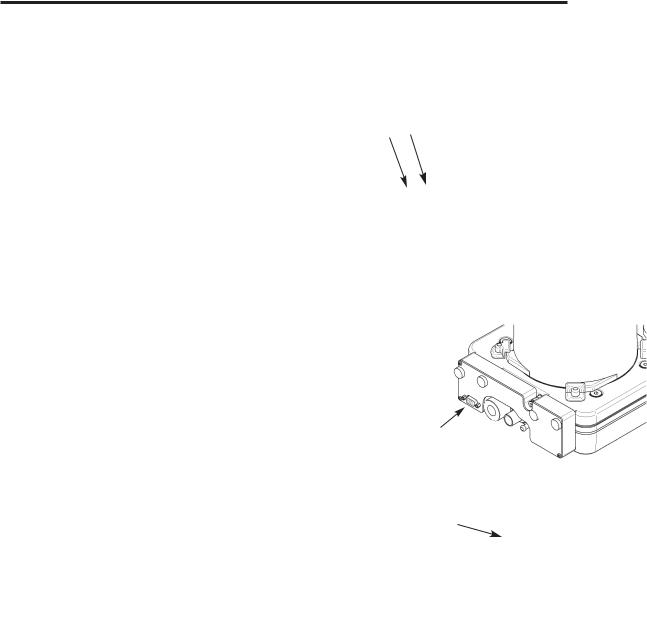
3.6 Interface to Prima SP2/3 and A200SP
The AV-S is designed to interface with the Prima SP2 Anaesthetic Machine and the A200SP Absorber.
3.6.1Prima SP2 Interface
The interface cable links the socket (A) on the control panel to a socket on the rear panel of the anaesthetic machine.
a)Turn the anaesthetic machine Gas Delivery Switch to ON.
The ventilator will power-up.
b)While the anaesthetic machine power is
ON, the Ventilator can be turned OFF and ON, using the ventilator On/Off switch, as described in section 3.5.1.
c)Turn the anaesthetic machine Gas Delivery Switch to OFF. The ventilator will power-down.
3.6.2A200SP Absorber Interface
The interface cable links the socket (B) on the control panel to a socket (C) at the rear of the absorber.
a)The A200SP is fitted with a sensor that detects the position of the absorber bag/vent control (D).
The sensor signal cabling is routed internally to connector (C) and a second cable runs to the the rear of the AV-S control unit.
b)Operation of the Bag/Vent control will trigger automatic Mode switching on the AV-S ventilator, as follows:
i)Ventilator in Volume or Pressure mode
Switching the absorber Bag/Vent control from Vent to Bag
-the ventilator will change from Volume Mode, or Pressure Mode, into Spontaneous Mode.
ii)Ventilator in Spontaneous Mode
Switching the absorber Bag/Vent control from Bag to Vent
A) If the ventilator was previously in Volume, or
Pressure, or Special Mode, and Spontaneous
Mode was automatically selected by the
B A
C
operation of the bag/vent control (from Vent to Bag, as described above):
- the ventilator will revert to that previous mode.
B)If the ventilator was in Standby Mode and
Spontaneous Mode selected on-screen:
- the ventilator will default to Volume Mode.
C) If the ventilator was put into Standby Mode after automatic mode switching to Spontaneous: - the ventilator will default to Volume Mode.
19

DESCRIPTION
3.7Ventilation Modes
3.7.1Standby Mode
Allows parameters to be set.
Some patient alarms are active:
High airway pressure (at 80 cmH2O) High/Low Oxygen
Negative pressure
Incorrect Rate/Ratio
20

DESCRIPTION
3.7.2Volume Mode
The ventilator delivers a mandatory set volume of gas at preset, fixed breath intervals.
The Patient is making no respiratory effort.
3.7.2.1 Fresh Gas Compensation
The delivered volume is adjusted by up to 60%. This delivered volume will consist of the volume delivered from the ventilator bellows, plus the fresh gas flow from the anaesthetic machine fresh gas supply, minus any compliance loss and minus any leak.
This gives a total actual inspired tidal volume. An alarm is triggered if the measured volume is 50% above or below the set volume
This function is user adjustable
Altitude Compensation
This function monitors ambient pressure, and adjusts the delivered volume accordingly
3.7.2.2 Operating Functions
Inspiratory Pause function:
This function creates a plateau that equates to 25% of the inspiratory time
Sigh function:
When the ventilator is in Volume Cycle mode the "Sigh" option is available. When selected, this option provides extra volume for 1 to 4 breaths in 50 (the user can select 1, 2, 3, or 4 breaths).
The extra volume will be approximately 50% above the tidal volume set by the user.
Note that the High Volume Alarm is not triggered when sigh is selected.
Volume measurement:
Volumes are measured if the Spirometry function is selected.
Automatic High or Low volume alarms are triggered if the measured volume is 50% above or below the set volume.
User adjustable option
If the maximum pressure limit is achieved, the ventilator cycles to the expiratory phase.
3.7.2.3 Volume Type Selection
Use the menu to switch between Tidal Volume and Minute Volume.
NOTE Minute Volume is derived from a rolling average during a 30 second period.
Volume Mode Parameters |
|
Tidal volume |
20 - 1600 mL |
Rate |
4-100 bpm |
I:E ratio |
1:0.3 - 1:8 |
PEEP 'Off' or adjustable |
4-20 cmH2O |
Inspiratory pressure limit |
10 to 100 cmH2O |
Inspiratory pause |
25% |
(does not affect I:E ratio) |
|
Sigh |
Approximately 1.5 x |
|
Set Vt is delivered |
|
once, twice, three |
|
times or four times |
|
every 50 breaths (user |
|
selects frequency) |
|
|
21

DESCRIPTION
3.7.3Pressure Mode
3.7.3.1 Parameters
In pressure mode the ventilator delivers a flow of gas to achieve a set pressure at fixed breath intervals.
The Patient is making no respiratory effort.
This is a common mode for the ventilation of small paediatric patients.
Inspiratory pressure |
10 - 70 cmH2O |
Rate |
4 - 100 bpm |
I:E ratio |
1:0.3 - 1:8 |
PEEP 'Off' or adjustable: 4 - 20 cmH2O
Inspiratory decelerating flow is controlled by the ventilator according to the pressure setting.
There is no Inspiratory Pause function in pressure mode.
3.7.3.2 Pressure Mode Operating Functions
Pressure mode defaults to a target pressure of 10 cmH2O at switch on.
A high Inspiratory Flow is used to achieve and maintain the target pressure.
The exhaust valve operates to prevent excess pressure.
22

DESCRIPTION
3.7.4Spontaneous Mode
3.7.4.1 Parameters
The ventilator monitors the following patient parameters:
Rate
I:E ratio
Pressure
Tidal volume
In spontaneous mode the waveform displays are active, and inspiratory oxygen levels are measured
3.7.4.2 Spontaneous Mode Operating Functions
Selection during Ventilation
Move the absorber Bag/vent switch to ‘Bag’ - the ventilator will switch from Pressure Mode or Volume Mode to Spontaneous Mode (see 3.6.2 - Absorber Interface).
Functions
No mechanical ventilation
No Inspiratory Pause function
Patient Monitoring (Bag mode and Ventilator mode): Airway pressures
FiO2,
Tidal volume, Rate
I:E ratio,
Supply pressures
Advanced Ventilation Modes
Patient support modes are selectable from this mode - see below, and section 3.7.5.
3.7.4.3 Patient Support Modes
The following support modes are selectable from the 'Special Modes' menu, and must be pre-select from the main menu, whilst in Standby.
SIMV - Synchronised Intermittent Mandatory Ventilation
SMMV - Synchronised Mandatory Minute Ventilation
PSV - Pressure Supported Ventilation
CAUTION
The required patient support mode must be pre-selected in Standby Mode (select from main menu), before it can be activated during the ventilation of a patient.
Please refer to sections 3.7.5.1, 3.7.5.2, 3.7.5.3.
Note that if the system fails to detect an absorber bag/vent switch, a confirm message will be displayed.
23
DESCRIPTION
3.7.5Advanced Spontaneous Breathing Modes
3.7.5.1SIMV
Synchronised Intermittent Mandatory Ventilation
SIMV provides a minimum level of tidal volume.
SIMV allows spontaneous breaths and a set mandatory breath, synchronised with the start of a patient breath
SIMV must be pre-selected in Standby Mode
Select Standby
Select Menu
Select Special Modes
Select Support Mode Select SIMV Escape Menu
SIMV will be displayed on the main screen when Spontaneous mode is selected or triggered.
NOTE
1.The trigger window is pre-set to 60% of the BPM cycle time.
2.The trigger is flow activated.
3.If Spirometry is disabled then SIMV is not available
4.If the pressure limit and alarm are activated the inspiratory phase is terminated
Activate SIMV during Ventilation
NOTE
SIMV will not function unless already preselected in Standby Mode
1.Select ‘Special Mode’ on the display. If the absorber Bag/Vent switch is not detected, a message will appear:
‘SET ABSORBER TO VENT’ Press the navigator wheel / push button to confirm.
2.Move the absorber Bag/vent switch to ‘Ventilator’.
3.Check that SIMV is functioning correctly.
SIMV Default Settings
The ventilator will default to pre-set values for Tidal volume (Vt), Rate, Inspiratory Time and Trigger Level, after selecting 'SIMV'.
Note:
1.Vt can be adjusted before SIMV is confirmed.
2.The trigger setting is adjustable between 0.7 and 4.0 L/min.
C E
D
Pmax
PEEP
0 cmH2O
A A
 B
B 
 B
B 
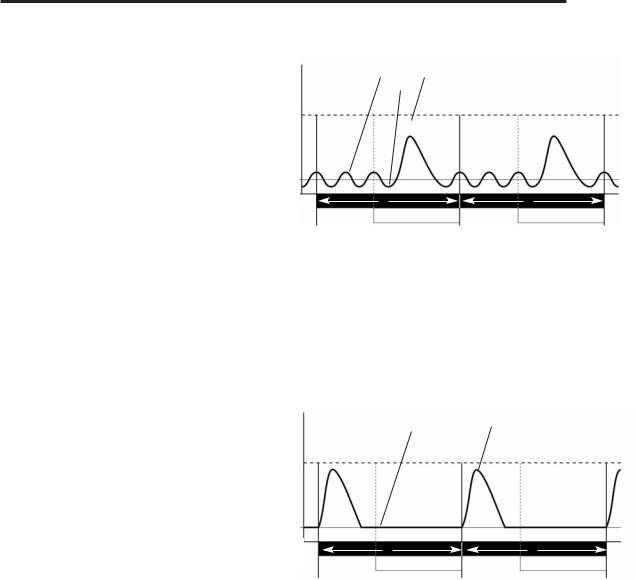
SIMV - Spontaneously Breathing Patient
A = Cycle Time (set from BPM)
B = Trigger Window
C = Spontaneous Breath
D = Trigger
E = Mandatory breath at the set tidal volume (Vt)
Inspiratory flow in the Trigger Window (generated by the patient’s spontaneous breath) results in a synchronised mandatory breath at a preset volume and rate
D
C
Pmax
PEEP
0 cmH2O
A A
 B
B 
 B
B 
SIMV - No breathing effort by Patient
A = Cycle Time (set from BPM) B = Trigger Window
C = Flat Pressure Trace (no breathing effort)
D = Mandatory breath at the end of the Trigger Window at the set Vt
If the patient makes no effort to breathe during a cycle, a mandatory breath, at the end of the trigger window, will still be delivered at the preset volume and rate.
24
 Loading...
Loading...