

NORTH AMERICAN DRÄGER The Evolution of Ventilation Brochures

The Evolution
of Ventilation
Ernst Bahns

Important Note:
Medical knowledge changes
constantly as a result of
new research and clinical
experience. The author of this
introductory guide has made
every effort to ensure that the
information given is completely
up to date, particularly as
regards applications and
effects of operation. However,
responsibility for all clinical
measures must remain with
the reader.
Author’s address:
Dr. Ernst Bahns
Drägerwerk Aktiengesellschaft
Moislinger Allee 53-55
23542 Lübeck
All rights, in particular those
of duplication and distribution,
are reserved by Drägerwerk AG.
No part of this work may be
reproduced or stored in any
form without the written
permission of Drägerwerk AG.
ISBN 3-926762-17-9

The Evolution of Ventilation –
from Pulmotor to Evita
An Introductory Guide to Ventilation with Evita

4
Content
Introduction
■ A century of evolution 6
■ The quality aspects of a ventilator 8
The history of ventilation
■ The dawn of mechanical ventilation 10
■ Pioneering days in ventilation: The “iron lung” 12
■ Early intensive care ventilation: The Assistors 14
■ Modern intensive care ventilation:
From Spiromat to Evita
16
■ The role of the therapist 18
■ Ventilation and respiration 20
The modes of ventilation
■ Three problems of ventilation 22
■ Pressure-limited ventilation with the UV-1 24
■ New ventilation technology with EV-A 26
■ Simple and open to spontaneous breathing:
BIPAP/PCV
⊕ 28
■ Pressure-optimized and open to spontaneous
breathing: AutoFlow
30
■ Spontaneous breathing: An evolution in itself 32
■ Synchronizing support and
spontaneous breathing
34
■ Trends in the evolution of the
ventilation modes
36
Content 5
Monitoring
■ From measurement device to
ventilation monitor
38
■ From momentary recording to trend analysis 40
■ From instructor to diagnostic assistant 42
■ Ventilation monitoring in the age
of the computer
44
Operation
■ Functions and operation 46
■ Powerful and efficient, yet easy to operate –
a contradiction in terms?
48
Conclusion
■ Ventilation without a ventilator? 50
Bibliography 52

Introduction6
A century of evolution
Evolution describes the development of life from a
simple to a highly-developed form. The theory of
evolution says that all life which exists today is the
result of a process of continuous self-development.
In other words, the theory not only says that
something is the way we currently see it, but also
tells us why this is so. By looking more closely at the
causes, evolution can give us insight into the paths
which development will take in the future.
This booklet will follow this theoretical approach
in describing the evolution of ventilation. Not only
historical facts will be presented, but at the same
time the causes of developments will be illuminated,
showing in which direction ventilation is likely to
develop.
There are good reasons why it is important to
take a critical look at the evolution of ventilation –
after all, it is not only true of biology but also
of medicine that development is not always
synonymous with progress.
Just like in biology, with its excess production of
species, a surplus of technical possibilities can be
identified in medicine.
Just like in biology, where the limits to growth are
determined by the finite nature of the living space
available, there are limits in medicine too. Here the
boundaries are set by ethical and economic
considerations: not everything which is technically
possible is morally acceptable and not everything is
affordable.
The dawn of artificial ventilation was marked by a
more or less completely uncritical embracing of new
technologies, leading to such a wealth of complexity
that it was no longer possible to retain a clear
overview.
The boundaries of medical
progress

Introduction 7
We have only very recently become aware of the
boundaries to the evolution of ventilation, however,
these days, new technologies are no longer
uncritically deployed in ventilation, and future
developments are to be target-oriented rather than
simply technology-guided.
It is the aim of this booklet not only to report on
the past, but also to contribute to the discussion
concerning the future of ventilation. From the point
of view of evolution, the intention is to portray
ventilation in a manner which will be of benefit not
only to medical and technical specialists, but also to
anyone interested in the subject, giving them the
opportunity to take part in the discussion on the
development of ventilation.
Given this desire to illustrate ventilation even to
those readers who are not confronted on a daily
basis with the subject, it is inevitable that some
principles will be dealt with which the more expert
reader will already be familiar with.
Although the process of evolution is described
here using only the example of Dräger ventilation,
this is not intended to disguise the fact that there
have also been others who have contributed
significantly to the evolution of ventilation. For the
sake of simplicity, however, this booklet deals
exclusively with ventilation from the House of
Dräger.
Following a brief description of the basic
elements of a ventilator, the history of ventilation
will be presented in excerpt form, as and when this
appears relevant to the process of evolution. For us,
the history of ventilation starts at Dräger with an
idea dreamed up by the founder of our company,
Heinrich Dräger …
Target-oriented rather
than technology-guided
development

Introduction8
The quality aspects
of a ventilator
Ventilation supports or substitutes damaged
respiration. A simple form of ventilation is mouthto-mouth resuscitation, and the technical aids used
in ventilation extend from the manually operated
ventilation bag to the modern contemporary
ventilator.
A ventilator’s efficiency depends primarily on
three factors, namely the quality of the ventilation
modes, of the ventilation monitoring system used
and of the operating concept. The development
of these fundamental elements of a ventilator
will initially be described in more detail, before
subsequent sections turn to the advent of the early
ventilators.
The chief focus as regards the ventilation modes
was originally on providing a short-term supply of
breathing gas in the event of a failure of the
patient’s own breathing. Hence the first ventilators
were purely emergency ventilators. However, where
longer treatment was called for, the life-saving
ventilation modes used at the time placed such a
strain on the lungs that it became extremely difficult
for the patient to return to breathing normally again.
Initially, auxiliary aids were employed to adapt the
ventilation modes to the patient’s physiology. Since
these were able to limit the damaging effects of
ventilation, they could be deployed in specific
cases by specialist physicians. Only recently have
ventilation modes been developed which allow
ventilation to be adapted automatically to the
patient.
The monitoring devices used in the early
ventilators did not extend beyond airway pressure
measurements and simple device function checks.
It was only some time later that more complex
Quality depends on
three factors
Ventilation modes
Monitoring system
Introduction 9
relationships could be identified by means of
additional monitoring systems. In the following
period, monitoring functions increasingly became an
integral part of ventilators. One notable advance in
this context was the quality of the information
display, which progressed from a simple measured
value indication to the use of a screen display.
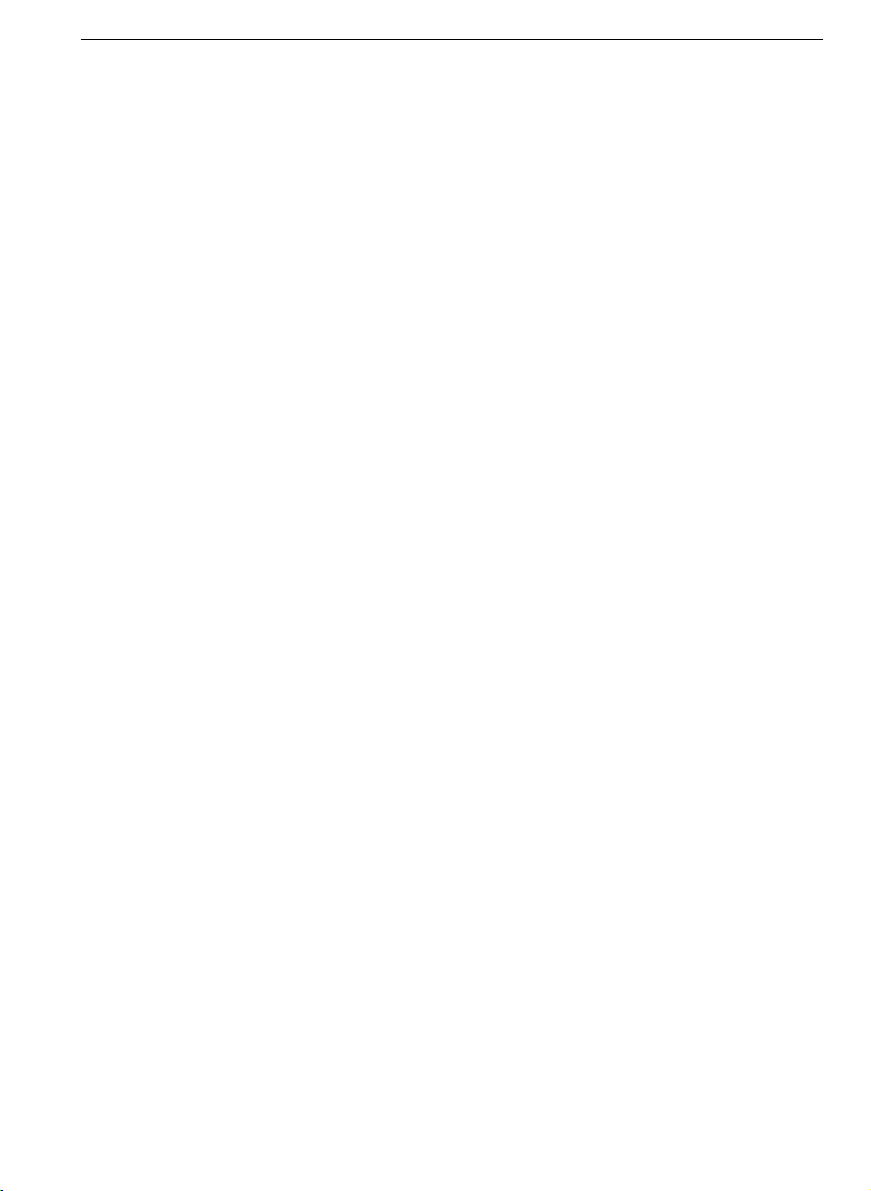
The entirety of the elements required to operate a
ventilator is termed the user interface. Due to the
increasing range of functions offered by the devices,
their operation unfortunately has also become ever
more complex; and this has gone hand in hand with
a constant rise in the number of control elements.
Only very recently has there been a qualitative
advance in this respect: the setting of device
functions on a screen permits a greater range of
functions while at the same time simplifying
operation.
Operating concept
Quality aspect
User benefit
OperationPerception Therapy
Ventilation
Monitoring
Human
Interface
Ventilation
Modes
Ventilator
The history of ventilation10
The dawn of mechanical
ventilation
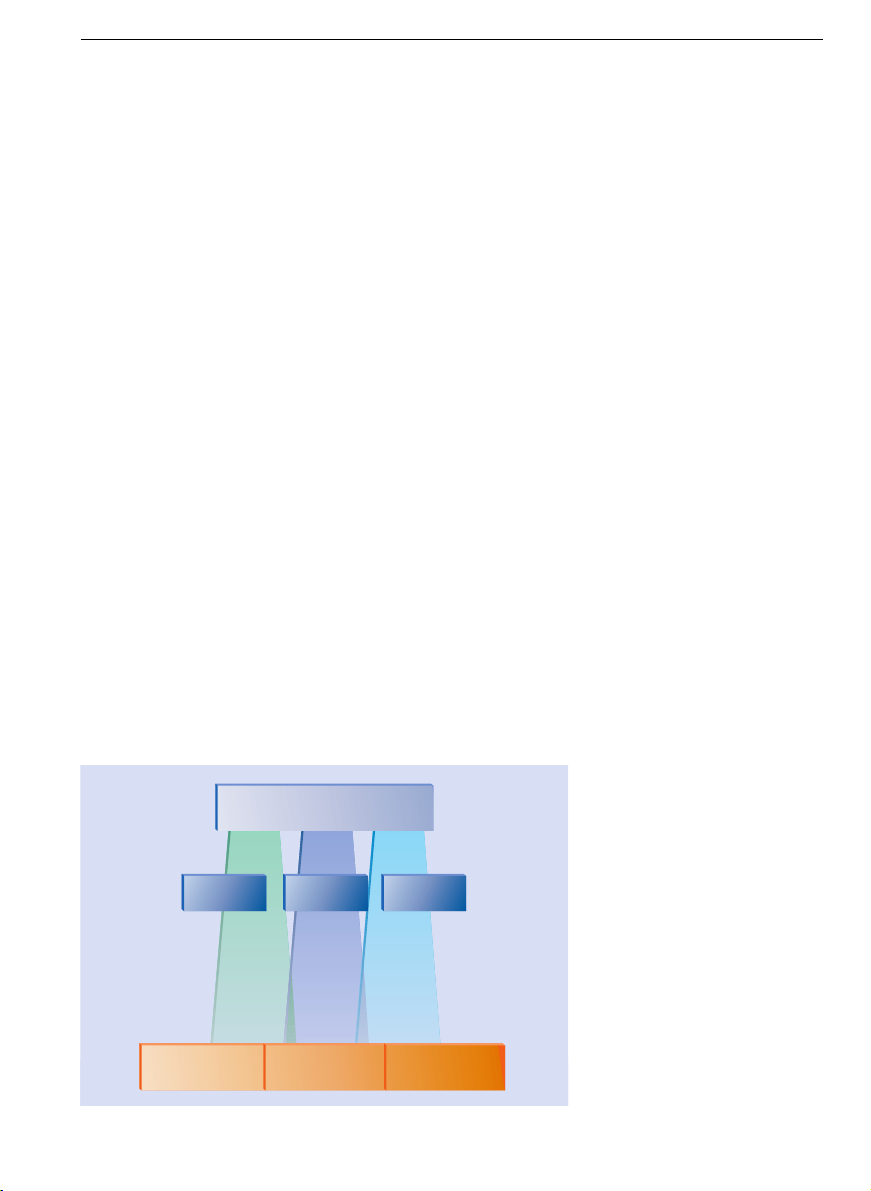
In his publication “Das Werden des Pulmotors”
[The Development of the Pulmotor] (4), Heinrich
Dräger recorded his thoughts on how to develop
a ventilator. He described a simple device for
“blowing fresh air or oxygen into the lung”. His
Pulmotor was controlled by a modified clockwork
mechanism.
This publication is remarkable less because of the
technology described in it, which appears extremely
simplistic compared with modern developments and
even at the time was somewhat controversial. What
is far more important is the reason which Heinrich
Dräger puts forward for choosing the technology he
did.
Heinrich Dräger
The original Pulmotor

The history of ventilation 11
For his apparatus he chose to use a technical
principle which replaces the human physiology as
naturally as possible. With his concept Heinrich
Dräger was decades ahead of his time.
As he saw it, the physiological function which
needed to be replaced was a regular and constant
movement of the respiratory apparatus. For this
reason he chose for his ventilation machine a
technical principle which involved an unchanged
inspiratory and expiratory phase during artificial
ventilation. This type of ventilation is what is now
described as time-cycled.
The rest of the world, including, incidentally,
those who worked on further developing the
Pulmotor, followed a different path. They decided
to control the respiratory phases using a technical
principle which would switch from expiration to
inspiration and vice versa once certain ventilatory
pressures were reached. These are known as
pressure-controlled systems.
In time, pressure-controlled ventilators became
more robust, reliable and accurate – in short, the
technology improved. Today, it would seem that
pressure-controlled ventilators had already reached
technological perfection, and in this sense a path
was pursued which the technology of the time was
better able to master.
As we have already seen, H. Dräger was well
ahead of his time in this respect: modern ventilators
are no longer pressure-controlled but predominantly
time-cycled. Whether Heinrich Dräger realized at
the time that he came much closer to reflecting
human physiology with his principle than others, we
will never know. What is a historical fact, however,
is that his time-cycled Pulmotor, patented in 1907,
pointed the right way.
Artificial ventilation as
substitute for a biological
function
Technologically optimized
ventilators

The history of ventilation12
Pioneering days in
ventilation: The “iron lung”
The Pulmotor was designed exclusively for shortterm usage. However, a number of diseases required
long-term ventilation. For instance, during the polio
epidemics which followed the Second World War,
numerous patients with respiratory paralysis needed
to be ventilated over a longer period of time. For this
purpose large, rigid containers were developed into
which the ventilated patient was placed.
Somewhat misleadingly, this apparatus was
known as an “iron lung”. To describe its function,
however, it would have been more fitting to call it
an “iron thorax”, since this more accurately reflects
the role of the rigid containers. Inside the container,
a flexible membrane ensured a constant change of
pressure, thus ventilating the lung like an artificial
diaphragm.
If the post-war period with its “iron lungs” is
described here as a time of pioneering, then this is
mainly as a result of Dönhardt’s accounts, which
describe in a particularly refreshing manner with
what great spirit of improvisation and with which
resources ventilators were developed not even fifty
years ago (3).
In one “iron lung” a torpedo tube was used as a
pressure chamber, while the ventilation mechanism
was driven by a smithy’s bellows, and the motor was
taken from a fishing boat …
The pioneers, which on their own initiative
initially built the first post-war “iron lungs” by hand,
soon found willing partners at Drägerwerk. With
their decades of experience in developing rescue
apparatus for miners and divers, the engineers took
the ideas of pressure-exchange ventilation and
adapted them for series production.
The limitations of the
Pulmotor

The history of ventilation 13
The “iron lungs” made it possible to raise significantly the survival rate of patients suffering from
respiratory paralysis as a result of polio. Nevertheless, the large amount of space needed for the
containers and the fact that the patient was less
accessible to nursing staff represented major
disadvantages.
As the next stage in the development of the “iron
lungs” came thoracic ventilators. In these devices it
was only the patient’s thorax which was subjected to
changing pressure, yet despite this further technical
development the pressure-exchange ventilators
were only used for a short time.
This was on account of the fact that a new
impulse brought about a renaissance of positive
pressure ventilation at the expense of the pressureexchange ventilators. This time the impulse came
not from technology, but from clinical practice.
Thoracic ventilator being
used in a hospital
The iron lung

The history of ventilation14
Early intensive care
ventilation: The Assistors
As early as the nineteen fifties, a new discovery
in clinical research prompted a rethinking in
ventilation therapy. The biggest problem namely
was not the reversal of the pressure conditions
during positive pressure ventilation, but far more
important was the fact that therapists relied more on
their own subjective clinical impressions than on
exact measuring parameters for assessing
ventilation (2).
This lack of knowledge concerning the ventilation
volumes administered thus frequently resulted in
incorrect treatment. Patients suffered either from an
inadequate supply of breathing gas or were exposed
to a high level of stress by unnecessarily rigorous
ventilation.
New findings, particularly from Sweden, led to
positive pressure ventilation once again regaining
popularity due to the fact that it was easier to
control. Two concepts were pursued in this respect:
on the one hand the breathing gas volume was
monitored during pressure-controlled ventilation,
and on the other a constant tidal volume was
delivered from the outset.
For the new areas of application, Dräger developed a whole series of devices both for pressurecontrolled and for volume-constant ventilation,
which for a while existed side by side, though it
should be pointed out that the concept of volumeconstant ventilation was implemented with some
delay as compared with the progress of the
Scandinavians. In pressure-controlled ventilation
the successful Pulmotor principle was further
developed in the Assistors (5).
In addition to pressure control, another common
feature of the Assistors was the possibility of
Controlled Ventilation
on the basis of exact
measurements
The history of ventilation 15
triggering a mechanical breath with a spontaneous
respiratory effort on the part of the patient. Furthermore, all the Assistors allowed the volume to be
monitored and aerosols to be nebulized by means of
an integrated nebulizer connection.
The Assistor 640 basic unit allowed assisted
ventilation which both supported and deepened
spontaneous breathing. In the Assistor 641 the
timing mechanism was pneumatic, but by the time
the Assistor 642 appeared, an electric timer was
already in use. In the Assistor 644 the duration of use
was increased by means of a new breathing air
humidification system, and the range of patients
which could be treated was extended to include
paediatric patients.
The Assistor 744 improved the quality of
ventilation, particularly in paediatrics, by using a
more sensitive trigger. What is more, the somewhat
unattractive external appearance of the early
Assistors was completely revised, and a user-friendly
and aesthetic product design became an
increasingly important feature of ventilator
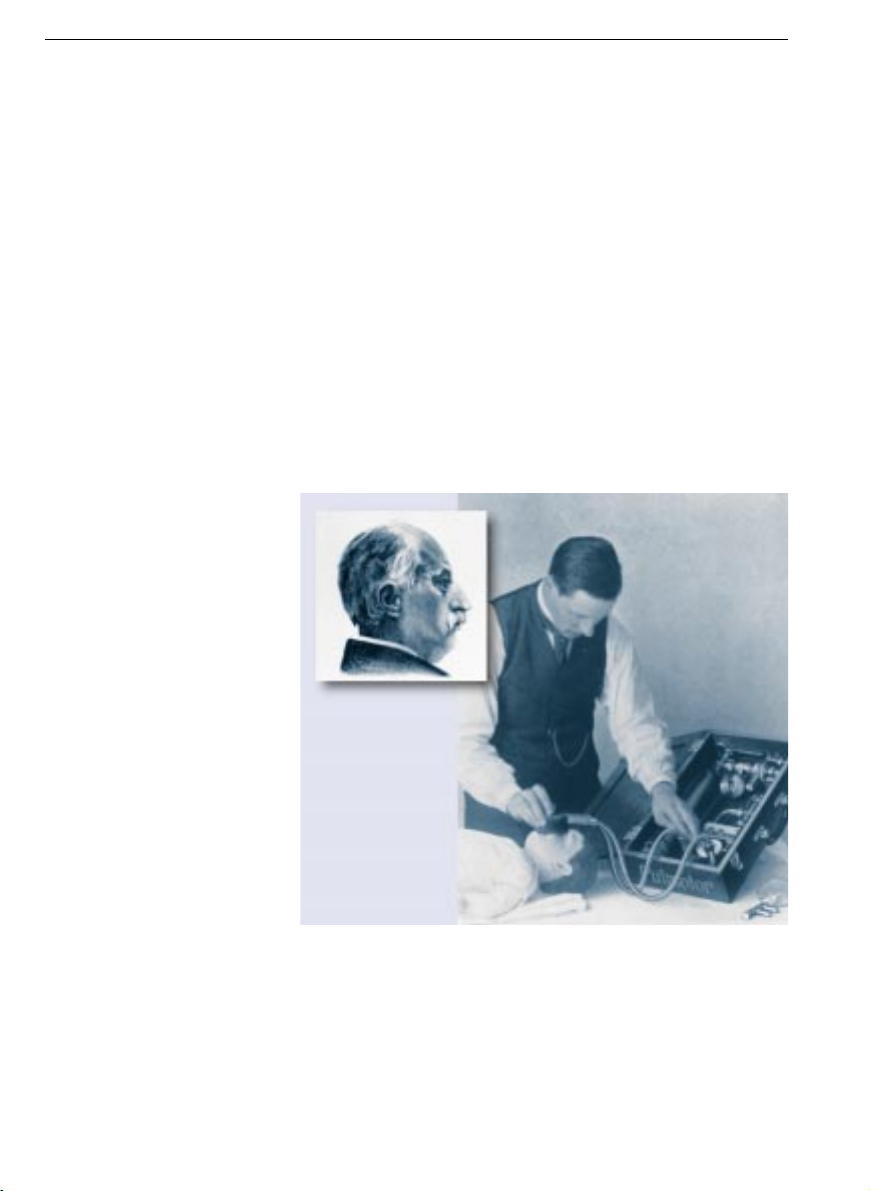
development.
The development of the
Assistor for pressurecontrolled ventilation
1965
1970
1960
Assistor
642
Assistor
644
Assistor
744
Assistor
640
Assistor
641
With the development of the Assistors, the area of
ventilator application had already been extended
from simple treatment of polio to post-operative
ventilation and inhalation therapy for patients with
chronic lung disorders.
Modern ventilation goes one step further. It not
only aims to act as a stop-gap for the duration of the
respiratory disorder, but also attempts to adapt the
mode of ventilation to the cause of the disorder,
providing where possible targeted treatment of the
problem.
Targeted intensive care therapy makes new
demands of ventilators, creating a need, for
example, for variable ventilation modes.
1980
1990
1970
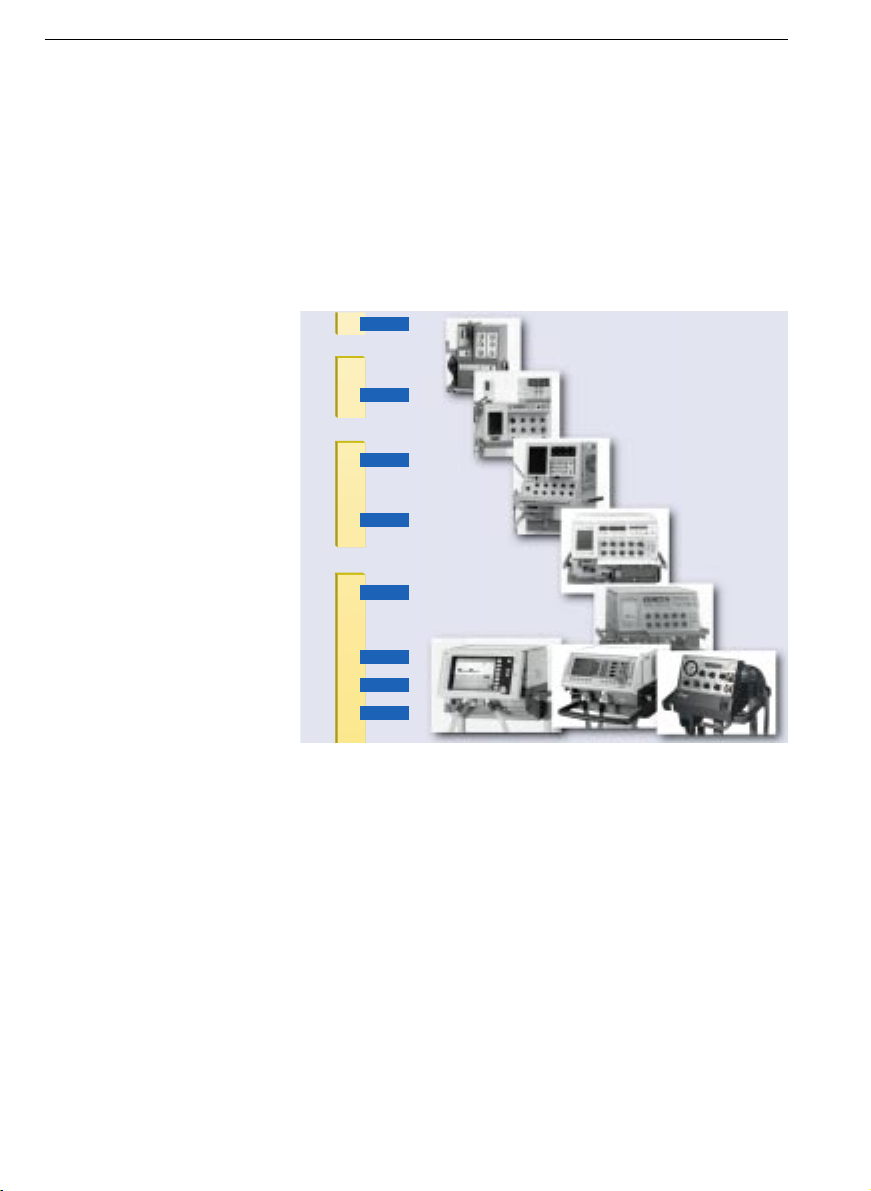
Evita 4
Evita2 dura
MicroVent
Evita 1
Evita 2
EV-A
UV1/UV2
Spiromat
The history of ventilation16
Modern intensive
care ventilation:
From Spiromat to Evita
Intensive care ventilators
over the years
Objectives of modern
ventilation

The history of ventilation 17
For the ventilators to be able to fulfil these new
demands, they needed to become more flexible.
Direct setting of breathing times and volumes was
required, as was time-cycled, volume-constant
ventilation.
The first Dräger ventilators able to meet these
needs were the Spiromats which appeared in 1955.
While the universal ventilator UV-1 from 1977 and
the later UV-2 retained the Spiromat’s conventional
bellows ventilation, in which the breathing gas
is pressed out of the ventilator bellows into the
patient’s lung, they already started to use electronics
in their control and monitoring systems.
In 1982, the EV-A electronic ventilator introduced
microprocessor-controlled gas flow regulation into
the world of Dräger ventilation, thus allowing the
flow rate to be accurately controlled throughout
the breathing cycle. Another new feature was the
display of ventilation curves on an integrated screen,
which has been a standard element in Dräger
intensive care ventilators ever since.
With the advent of the Evita series, microprocessor technology in ventilation became more
advanced, making it possible to adapt the machine’s
ventilation to the patient’s own spontaneous
breathing. In very recent times, the integrated
screen has ceased to be merely a medium for the
display of measured values, now offering direct
operation of the ventilator.
Recently there have been three device concepts in
Dräger intensive care ventilation which have been
running parallel to one another – the Evita 4 for the
top-class segment, the Evita 2 dura for standard
needs and the compact size ventilator MicroVent.
Modern intensive care
ventilators allow timecycled, volume-constant
ventilation
A display screen for
ventilation curves has been
an integral part of the
ventilator since 1982
 Loading...
Loading...