

COVIDIEN Peripherally Inserted Central Catheter User Manual [en, es, fr]

Argyle
TM
Peripheral Inserted Central Catheter (PICC)
Cathéter central périphérique (PICC)
Catéter central de inserción periférica (PICC)
Cateter central de inserção periférica (PICC)

n
en
DESCRIPTION:
A radiopaque, polyurethane Peripherally Inserted Central Catheter (PICC)
INDICATIONS:
The catheter is designed for cases in which venous catheterization or long term I.V. administration is
necessary. Placement is routinely achieved from a peripheral venous site, but the catheter may be
placed via subclavian cutdown as well. The catheter may be used to administer uids for hydration and
parenteral nutrition, as well as other commonly used intravenous medications.
Note:
Before performing catheter placement all directions, precautions, contraindications, and
warnings must be read and clearly understood. A standard protocol should be established
prior to use of the Argyle™ PICC, and the catheter is only to be placed by personnel with
appropriate training. The CDC (Centers for Disease Control) guidelines can be consulted
to assist with the development of protocols for the care and use of peripherally inserted
venous catheters.
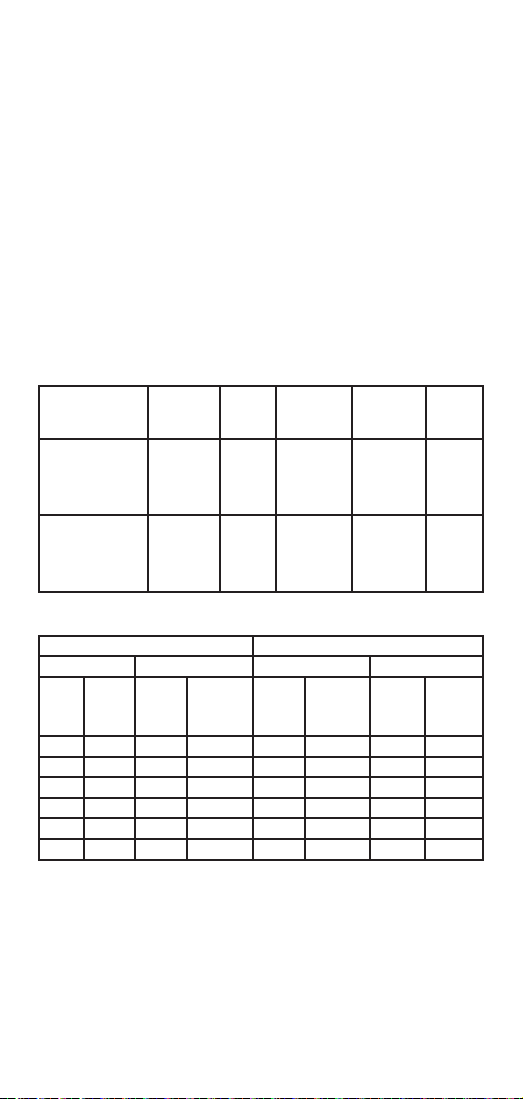
CATHETER SPECIFICATIONS (NOMINAL):
Reorder # Description French
43303 Peripheral Inserted
43304 Peripheral Inserted
1
Dual Lumen Primary and Secondary lumen areas are the same and “D” shaped.
Length
Trimmed
(cm)
0 30 0.18 55 0.15 6 0.13 6
4 26 0.15 63 0.14 7 0.12 7
8 22 0.13 71 0.13 8 0.11 8
12 18 0.12 81 0.12 10 0.10 10
16 14 0.12 91 0.12 12 0.10 12
20 10 0.12 114 0.12 16 0.10 16
Central Catheter (PICC)
Single Lumen
Central Catheter (PICC)
Dual Lumen
Remaining
Eective
Length (cm)
Single Lumen PICC Primar y Lumen Secondary Lumen
Priming
Flow Rate 100
Volume
cm Gravity
(mL)
EectiveLength
Size
(Fr)
1.9 30 0.6 0.4
1.9 30 0.6 N/A
Priming
Volume
(mL/hr)
(mL)
(cm)
OuterDiameter
Dual Lumen PICC
Flow Rate 100
cm Gravity
(mL/hr)
(mm)
Priming
Volume
(mL)
Inner
Diameter
(mm)
1
Flow Rate
100 cm
Gravity
(mL/hr)
• The dual lumen PICC is capable of infusing a 20% IV fat emulsion at 50 mL/Hr with less than 12 psi
infusion pump pressure.
• Graduation marks are printed every cm starting at 3cm at the distal end and terminating at 30cm at
the proximal end near the stabilizing wing. The 5cm marks are bold with the 20cm and 30cm marks
identied with two and three bold marks respectively.
• At the time of manufacture the distal tip is formed with a straight or blunt cut conguration.
PRECAUTIONS, CONTRAINDICATIONS AND WARNINGS:
• Do not use if unit package is opened or damaged.
• Use of aseptic technique and Universal Precautions should be followed during the placement and
maintenance of the catheter.
• To ensure the catheter does not migrate, and to be certain it is not inadvertently broken, it must be
secured according to the instructions.
• Do not place the catheter tip or allow the catheter tip to migrate into the low right atrium. This
2

could cause cardiac penetration and subsequent pericardial eusion and tamponade.
• The catheter must not be withdrawn while a “splittable needle” introducer is in the patient. Doing
so could cause shearing of the catheter. Note: Introducers other than the “catheter over needle” type
should be used following the manufacturers specic instructions.
• Do not use a sharp clamp or instrument to handle the catheter since even a minor cut
could tear or break the catheter.
• Do not stretch catheter. Too much tension could tear the catheter.
• To avoid damage to blood vessels and viscus, catheters should not be subjected to
injection pressures greater than 25 psi. Use of a small diameter syringe (such as a
tuberculin) can result in very high pressures. If the catheter were occluded, high
pressure could rupture it or force the cause of the occlusion to be injected into the
patient. Only use syringes 5cc or larger with this product.
• Prevent powder on sterile gloves from making contact with the catheter.
• After placement, care should be taken to prevent the kinking or occlusion of catheter while securing
it because ow could be reduced or stopped.
• The catheter must not be sutured.
• Holes located on the stabilizing wing, if present, are intended to be used with Argyle™ catheter
securement devices and are not intended for suturing.
• If phlebitis, infection, or symptoms of patient reaction should occur, all I.V. catheters being utilized
must be treated as a possible reason for the complication.
• Guidewires or stylets are not intended to be used with this catheter.
• Do not use alcohol or acetone based skin preparations, adhesive enhancers, or solutions
directly on the catheter
• Note: Do not apply tape to the catheter
• Contraindications include the following:
Rapid large infusion Cellulitis sites
Rapid bolus infusion R adiation therapy planned at the site
Hemodialysis Severe coagulopathies
Plasmapheresis Contractures of limb to be used
High pressure injection Existing thrombophlebitis at site
for diagnostic purposes Blood infusion
Burn sites Aspiration of blood for sampling
Dermatitis sites
POTENTIAL COMPLICATIONS:
While an indwelling venous catheter supplies vital venous access for critically ill patients, the potential
for serious complication exists, such as:
Air Embolus Arrhythmia
Arterial Puncture Bleeding
Catheter Fragment Embolus Erosion/Perforation of Vessel/Heart
Hematoma Hemothorax
Hydrothorax Infection and Catheter Related Sepsis
Intimal Dissection Migration of Catheter
Myocardial Damage Nerve Damage
including Perforation Pneumothorax
Pulmonary Artery Rupture Thrombosis
Valvular Damage
RECOMMENDED CATHETER PLACEMENT PROCEDURE:
1. Obtain informed consent per hospital protocol.
2. Select an appropriate vein for cannulation. Suggested access sites include the external jugular,
basilic, cephalic, femoral, or great saphenous vein.
3. Position the patient. If arm is used, extend the patient’s arm laterally 90 degrees to the body for
adequate visualization of site.
4. Measure the approximate distance from the insertion site to the point at which the catheter tip
will be placed. Optional: Trim the catheter to length according to hospital or institutional protocol.
Catheter Trimming Recommendations: Maintain asceptic technique while using a sharp sterile
scalpel or sterile scissors to cut the distal end of the catheter squarely to produce a clean, smooth
cut surface. Inspect cut surface to assure there is no loose material.
5. Use standard hospital protocol and aseptic techniques to prepare the venipuncture site.
3

6. Use lightly heparinized saline to ush the catheter.
7. In order to distend the selected vessel, a tourniquet may be applied.
8. Place fenestrated drape over anticipated puncture site.
9. Puncture the skin approximately 1cm below the proposed access site of the distended vessel with
the introducer. Observe ashback once vein is accessed.
If using “catheter over needle” introducer, remove needle portion prior to inserting PICC into
catheter portion of introducer.
10. Grasp the distal end of the catheter with non-serrated forceps approximately 1cm from the end
and advance the catheter the predetermined distance through the introducer using short, gentle
strokes. (For access via antecubital area, when tip reaches deltoid region, release tourniquet and
turn patient’s head toward access site with chin down to pinch o external jugular vein.)
Note: If catheter meets resistance while being advanced, do not force it. A low pressure ush of
saline may free the tip allowing the catheter to proceed. In the event of vasospasm, apply heat
and proceed according to hospital or institutional protocol.
IMPORTANT CAUTION: AT NO TIME SHOULD THE CATHETER BE WITHDRAWN BACK
THROUGH A SPLITTABLE NEEDLE. IF IT BECOMES IMPOSSIBLE TO ADVANCE THE CATHETER
INTO A SATISFACTORY POSITION, THEN THE NEEDLE AND CATHETER MUST BE WITHDRAWN
SIMULTANEOUSLY. THE RESULT OF WITHDRAWING A CATHETER BACK THROUGH THE
NEEDLE CAN BE CATHETER EMBOLISM.
11. Apply pressure to vein distal to introducer tip to stabilize catheter and carefully withdraw
introducer from puncture site.
Caution: Do not stabilize catheter by applying pressure at point of introducer needle
while withdrawing “splittable needle” introducer – doing so could damage catheter.
12. Apply gentle pressure to insertion site with a gauze pad to stanch blood ow.
13. If using “splittable needle” introducer follow manufacturer’s instructions.
14. If using “catheter over needle” introducer follow manufacturer’s instructions.
15. To achieve proper tip placement after introducer has been removed, non-serrated forceps may be
used to advance the catheter into the venipuncture.
16. Aspirate with a syringe (with heparinized saline) to ensure a good blood return. Flush catheter to
conrm patency.
Note: Do not aspirate blood from the catheter for sampling purposes.
17. Remove drape.
18. If catheter is centrally placed:
a. Temporarily secure catheter.
b. Conrm proper catheter tip placement radiographically.
c. Proper central catheter tip location is within the inferior vena cava or superior vena cava or at
the juncture of the superior vena cava and the right atrium.
Caution: Placing catheter in lower right atrium could cause cardiac penetration and
subsequent pericardial eusion and tamponade.
19. Remove the temporary dressing and prepare the site for nal dressing.
Note: Use of skin preps on neonates can cause abrasions or skin sloughing when dressing
is removed.
20. Chart procedure performed noting catheter length. Record whether or not the catheter was
trimmed and to what length.
SECURING THE CATHETER:
The venipuncture site should be protected and the catheter secured with a transparent dressing. Secure
the catheter and dressing to the venipuncture site according to hospital or institutional protocol.
Note: Applying the dressing directly to the catheter can help prevent migration.
Note: Suturing is contraindicated.
Note: Holes located on the stabilizing wing, if present, are intended to be used with Argyle™
catheter securement devices and are not intended for suturing.
Note: Do not use alcohol or acetone based skin preparations, adhesive enhancers, or
solutions directly on the catheter.
Note: Do not apply tape to the catheter.
Recommended Catheter Maintenance:
These recommendations are meant to provide a foundation for developing a protocol for maintaining
the sterility of the catheter and the insertion site, and reducing the chance of the catheter’s accidental
displacement.
4

Dressing Change:
1. The dressing should be changed according to hospital or institutional protocol.
2. Ensure that there are no kinks in the tubing and lay the catheter against the patient’s skin.
3. Ensure that the portion of catheter outside of the body corresponds to previous catheter
measurement.
4. Using the same technique as described in “Securing the Catheter”, apply the dressing.
5. Once dressing is changed, check the entire I.V. tubing and pump setup to ensure the system is
owing freely at the prescribed rate.
6. Document the procedure, any observations, and patient’s condition.
Flushing:
Flush catheter with heparinized saline using positive pressure technique according to hospital or
institutional protocol. Check the prime volume printed on the catheter or the instructions for use to
help determine ushing volumes.
Occluded or Partially Occluded Catheter:
Catheters that present resistance to ushing and aspiration may be partially or completely
occluded. Do not ush against resistance. If the lumen will neither ush nor aspirate and it has
been determined that the catheter is occluded with blood, it is recommended that the catheter be
replaced.
Catheter Removal:
Typically, the catheter can be easily removed. To remove it, grasp the catheter and draw it straight
out, in a line parallel to the vein.
Note: In some cases, the catheter will oer resistance upon removal, generally when it has been
in place for more than ve days. If resistance is encountered, pull gently on the catheter and
re-tape. The catheter should be checked every four hours until it can be removed without diculty.
Additionally, warm compresses applied at and above the insertion site may aid in catheter removal.
5
n
fr
DESCRIPTION :
Cathéter central périphérique (PICC) radio-opaque en polyuréthane
INDICATIONS :
Ce cathéter est conçu pour les cas où un cathétérisme veineux ou une administration i.v. de longue durée
est nécessaire. La mise en place s’eec tue généralement depuis un site veineux périphérique mais il
est également possible de poser le cathéter par dénudation du site sous-clavier. Le cathéter peut être
employé pour l’administration de liquides d’hydratation et la nutrition parentérale, aussi bien que de
toute autre médication intraveineuse courante.
Remarque :
Il faut lire et bien comprendre toutes les instructions, les précautions, les contre-
indications et les avertissements avant de procéder à la mise en place d’un cathéter. Un
protocole standard doit être établi avant l’utilisation du PICC Argyle™, et le cathéter doit
être mis en place uniquement par du personnel ayant suivi une formation adéquate.
On peut se reporter aux lignes directrices des CDC (Centers for Disease Control) pour des
renseignements sur l’élaboration de protocoles de soin et d’utilisation des cathéters veineux
périphériques.
CARACTÉRISTIQUES TECHNIQUES (NOMINALES) DU CATHÉTER :
Numéro de
réapprovisionnement
43303 Cathéter central
43304 Cathéter central
1
Les lumières primaire et secondaire des cathéters à double lumière sont identiques et en forme de « D ».
Longueur
Longueur
coupée
(cm)
restante
0 30 0.18 55 0.15 6 0.13 6
4 26 0.15 63 0.14 7 0.12 7
8 22 0.13 71 0.13 8 0.11 8
12 18 0.12 81 0.12 10 0.10 10
16 14 0.12 91 0.12 12 0.10 12
20 10 0.12 114 0.12 16 0.10 16
Description Calibre
périphérique
(PICC)
À lumière
unique
périphérique
(PICC)
À double
lumière
PICC à lumière unique Lumière primaire Lumière secondaire
Volume
réelle
d'amorçage
(ml)
(cm)
en French
Débit 100 cm
par gravité
(ml/h)
Longueur
(Fr)
réelle
(cm)
1.9 30 0.6 0.4
1.9 30 0.6 S/O
PICC à double lumière
Volume
Débit 100 cm
d’amorçage
par gravité
(ml)
(ml/h)
Diamètre
externe
(mm)
Volume
d’amorçage
(ml)
Diamètre
interne
(mm)
1
Débit 100 cm
par gravité
(ml/h)
• Le PICC à double lumière permet d’injecter une émulsion lipidique à 20 % par i.v. à un débit de 50
ml/h avec une pression de pompe à perfusion inférieure à 83 kPa (12 psi).
• Des traits de graduation sont imprimés à chaque centimètre, à partir de 3 cm à l’extrémité distale et
jusqu’à 30 cm à l’ex trémité proximale près de l’ailette stabilisatrice. Les marques à tous les 5 cm sont
identiées par des traits gras, alors que les marques à 20 cm et à 30 cm sont identiées par des traits
gras doubles et triples, respectivement.
• Au moment de la fabrication, l’extrémité distale est produite sous forme droite ou arrondie.
6
 Loading...
Loading...