

Page 1
INSTRUCTIONS
EVIS LUCERA GASTROINTESTINAL VIDEOSCOPE
OLYMPUS GIF-N260
OLYMPUS GIF-XP260
OLYMPUS GIF-XQ260
OLYMPUS GIF-Q260
OLYMPUS GIF-H260
OLYMPUS GIF-H260Z
EVIS LUCERA COLONOVIDEOSCOPE
OLYMPUS CF-Q260AL/I
OLYMPUS CF-Q260DL/I
OLYMPUS CF-H260AL/I
OLYMPUS CF-H260AZL/I
OLYMPUS PCF-Q260AL/I
Refer to the endoscope’s companion manual, the “REPROCESSING MANUAL” whose
cover lists the model of your endoscope, for reprocessing information.
Page 2

Page 3

Contents
Contents
Symbols......................................................................................... 1
Important Information — Please Read Before Use.................... 2
Intended use ............................................................................................ 2
Applicability of endoscopy and endoscopic treatment .............................. 3
Instruction manual .................................................................................... 3
User qualifications .................................................................................... 4
Instrument compatibility ........................................................................... 4
Reprocessing before the first use/reprocessing and storage after use..... 5
Spare equipment ...................................................................................... 5
Maintenance management ....................................................................... 5
Prohibition of improper repair and modification ........................................ 5
Signal words.............................................................................................. 6
Warnings and cautions ............................................................................. 6
Examples of inappropriate handling.......................................................... 12
Chapter 1 Checking the Package Contents............................ 13
Chapter 2 Instrument Nomenclature and Specifications ...... 18
2.1 Nomenclature.................................................................................. 18
2.2 Endoscope functions....................................................................... 30
2.3 Specifications.................................................................................. 33
2.4 Attaching the chain for water-resistant cap (MAJ-1119) ................. 46
Chapter 3 Preparation and Inspection .................................... 49
3.1 Preparation of the equipment.......................................................... 50
3.2 Inspection of the endoscope ........................................................... 52
3.3 Preparation and inspection of accessories ..................................... 58
3.4 Attaching accessories to the endoscope ........................................ 62
3.5 Inspection and connection of ancillary equipment .......................... 65
3.6 Inspection of the endoscopic system .............................................. 69
Chapter 4 Operation ................................................................. 75
4.1 Insertion .......................................................................................... 79
4.2 Using endo-therapy accessories..................................................... 88
4.3 Withdrawal of the endoscope.......................................................... 94
4.4 Transportation of the endoscope .................................................... 95
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
i
Page 4

Contents
Chapter 5 Troubleshooting ...................................................... 97
5.1 Troubleshooting guide .................................................................... 97
5.2 Withdrawal of the endoscope with an abnormality.......................... 102
5.3 Returning the endoscope for repair................................................. 105
Appendix........................................................................................ 107
System chart ............................................................................................ 107
EMC information........................................................................................ 133
ii
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 5
Symbols
Symbols
The meaning(s) of the symbol(s) shown on the package with the components,
the back cover of this instruction manual and/or this instrument are as follows:
Refer to instructions.
Endoscope
TYPE BF applied part
Manufacturer
Authorized representative in the European Community
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
1
Page 6

Important Information — Please Read Before Use
Important Information — Please Read
Before Use
Intended use
These instruments have been designed to be used with an Olympus video
system center, light source, endoscope position detecting unit (for CF-Q260DL/I
only), magnification controller (for CF-H260AZL/I only), documentation
equipment, monitor, endo-therapy accessories such as a biopsy forceps and
other ancillary equipment.
Use the EVIS LUCERA GASTROINTESTINAL VIDEOSCOPE GIF-N260 for
transoral or transnasal endoscopy and endoscopic surgery within the upper
digestive tract (including the esophagus, stomach and duodenum).
Use the EVIS LUCERA GASTROINTESTINAL VIDEOSCOPE GIF-XP260,
GIF-XQ260, GIF-Q260, GIF-H260, GIF-H260Z for endoscopy and endoscopic
surgery within the upper digestive tract (including the esophagus, stomach and
duodenum).
Use the EVIS LUCERA COLONOVIDEOSCOPE CF-Q260AL/I, CF-H260AL/I,
PCF-Q260AL/I, CF-H260AZL/I, CF-Q260DL/I for endoscopy and endoscopic
surgery within the lower digestive tract (including the anus, rectum, sigmoid
colon, colon and ileocecal valve).
Do not use these instruments for any purpose other than their intended uses.
Select the endoscope to be used according to the objective of the intended
procedure based on the full understanding of the endoscope’s specifications and
functionality as described in this instruction manual.
2
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 7

Important Information — Please Read Before Use
Applicability of endoscopy and endoscopic treatment
If there is an official standard on the applicability of endoscopy and endoscopic
treatment that is defined by the hospital’s administration or other official
institutions such as academic societies on endoscopy, follow that standard.
Before starting endoscopy and endoscopic treatment, thoroughly evaluate its
properties, purposes, effects, and possible risk (their natures, extent and
probability). Perform endoscopy and endoscopic treatment only when its
potential benefits are greater than its risks.
Fully explain to the patient the potential benefits and risks of the endoscopy and
endoscopic treatment as well as any examination/treatment methods that can be
performed in its place, and perform the endoscopy and endoscopic treatment
only after obtaining the consent of the patient.
Even after starting the endoscopy and endoscopic treatment, continue to
evaluate the potential benefits and risks, and immediately stop the
endoscopy/treatment and take proper measures if the risks to the patient
become greater than the potential benefits.
Instruction manual
This instruction manual contains essential information on using this instrument
safely and effectively. Before use, thoroughly review this manual and the
manuals of all equipment which will be used during the procedure and use the
equipment as instructed.
Note that the complete instruction manual set for this endoscope consists of this
manual and the “REPROCESSING MANUAL” whose cover lists the model of
your endoscope. It also accompanied the endoscope at shipment.
Keep this and all related instruction manuals in a safe, accessible location.
If you have any questions or comments about any information in this manual,
please contact Olympus.
Terms used in this manual
Special light observation:
This is an observation using filtered light.
NBI (Narrow Band Imaging) observation:
This is a special light observation using the narrow band observation light.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
3
Page 8

Important Information — Please Read Before Use
Normal light observation (WLI (White Light Imaging) observation):
This is the ordinary observation using the RGB light.
User qualifications
If there is an official standard on user qualifications to perform endoscopy and
endoscopic treatment that is defined by the medical administration or other
official institutions, such as academic society on endoscopy, follow that standard.
If there is no official qualification standard, the operator of this instrument must
be a physician approved by the medical safety manager of the hospital or person
in charge of the department (department of internal medicine, etc.).
The physician should be capable of safety performing the planned endoscopy
and endoscopic treatment following guidelines set by the academic societies on
endoscopy, etc., and considering the difficulty of endoscopy and endoscopic
treatment. This manual does not explain or discuss endoscopic procedures.
Instrument compatibility
Refer to the “System chart” in the Appendix to confirm that this instrument is
compatible with the ancillary equipment being used. Using incompatible
equipment can result in patient or operator injury and/or equipment damage.
This instrument complies with the EMC standard for medical electrical
equipment; edition 2 (IEC 60601-1-2: 2001). However, when connected with an
instrument that complies with the EMC standard for medical electrical
equipment; edition 1 (IEC 60601-1-2: 1993), the whole system complies with
edition 1.
4
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 9

Important Information — Please Read Before Use
Reprocessing before the first use/reprocessing and storage after use
This instrument was not cleaned, disinfected or sterilized before shipment.
Before using this instrument for the first time, reprocess it according to the
instructions given in the endoscope’s companion manual, the “REPROCESSING
MANUAL” whose cover lists the model of your endoscope.
After using this instrument, reprocess and store it according to the instructions
given in the endoscope’s companion reprocessing manual. Improper and/or
incomplete reprocessing or storage can present an infection-control risk, cause
equipment damage or reduce performance.
Spare equipment
Be sure to prepare another endoscope to avoid that the examination will be
interrupted due to equipment failure or malfunction.
Maintenance management
The probability of failure of the endoscope and ancillary equipment increases as
the number of procedures performed and/or the total operating hours increase.
In addition to the inspection before each procedure, the person in charge of
medical equipment maintenance in each hospital should inspect the items
specified in this manual periodically. An endoscope with which an irregularity is
suspected should not be used, but should be inspected by following Section 5.1,
“Troubleshooting guide” on page 97. If the irregularity is still suspected after
inspection, contact Olympus.
Prohibition of improper repair and modification
This instrument does not contain any user-serviceable parts. Do not
disassemble, modify or attempt to repair it; patient or operator injury and/or
equipment damage can result.
Equipment which has been disassembled, repaired, altered, changed or
modified by persons other than Olympus’ own authorized service personnel is
excluded from Olympus’ limited warranty and is not warranted by Olympus in
any manner.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
5
Page 10

Important Information — Please Read Before Use
Signal words
The following signal words are used throughout this manual:
Indicates a potentially hazardous situation which, if not
avoided, could result in death or serious injury.
Indicates a potentially hazardous situation which, if not
avoided, may result in minor or moderate injury. It may also
be used to alert against unsafe practices or potential
equipment damage.
Indicates additional helpful information.
Warnings and cautions
Follow the warnings and cautions given below when handling this instrument.
This information is to be supplemented by the warnings and cautions given in
each chapter.
• After using this instrument, reprocess and store it according
• Before endoscopy, remove any metallic objects (watch,
• Do not strike, bend, hit, pull, twist, or drop the endoscope’s
to the instructions given in the endoscope’s companion
reprocessing manual whose cover lists the model of your
endoscope. Using improperly or incompletely reprocessed or
stored instruments may cause patient cross-contamination
and/or infection.
glasses, necklace, etc.) from the patient. If performing
high-frequency cauterization treatment becomes necessary
while the patient wears a metallic object, it may cause burns
on the patient in areas around the metallic object.
distal end, insertion tube, bending section, control section,
universal cord, or endoscope connector of the endoscope
with excessive force. The endoscope may be damaged and
could cause patient injury, burns, bleeding and/or
perforations. It could also cause parts of the endoscope to fall
off inside the patient.
6
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 11

Important Information — Please Read Before Use
• When performing transnasal insertion of the GIF-N260,
please follow the cautions below.
− The shape and size of the nasal cavity and its suitability
for transnasal insertion may vary from patient to patient.
No endoscope, including this one, can always be inserted
transnasally with all patients. Before proceeding, always
be sure to confirm that transnasal insertion is possible
with the patient by always considering both the size of the
patient’s nasal cavity as well as the size of the
endoscope’s insertion tube. Otherwise, operator and/or
patient injury can result or the endoscope could become
lodged and be difficult to withdraw.
− Transnasal insertion is accompanied by the risk of
inflammation of the nasal cavity. If this happens, the nasal
passage will be constricted, making it more difficult to
withdraw the endoscope. In this case, do not use force to
withdraw the endoscope because patient injury such as
bleeding or perforation may result.
− Transnasal insertion is accompanied by the risk of
bleeding in the nasal cavity. Be sure to be prepared to
deal with any bleeding. When withdrawing the
endoscope, observe the inside of the nasal cavity to
ensure that there is no bleeding. Even when the
endoscope has been withdrawn without bleeding, do not
allow the patient to blow his or her nose strongly because
this could cause it to start bleeding.
− Before transnasal insertion, apply the appropriate
pretreatment and lubrication to the patient to enlarge the
nasal cavity. Otherwise, operator and/or patient injury can
result or the endoscope could become lodged and be
difficult to withdraw. When applying a pretreatment agent
through a tube, insert the tube into the same path as the
path planned for the endoscope insertion. Otherwise, the
treatment will have no effect. The effects of the
pretreatment agent and lubricant will decrease the longer
the procedure lasts. Apply the pretreatment agent or
lubricant as required during the procedure
when withdrawal seems to be difficult.
– for example,
− Transnasal insertion of the endoscope should be
performed carefully. If resistance to insertion is felt, or the
patient reports pain, stop insertion immediately.
Otherwise, operator and/or patient injury can result or the
endoscope could become lodged and be difficult to
withdraw.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
7
Page 12

Important Information — Please Read Before Use
• Never perform angulation control forcibly or abruptly. Never
• Never insert or withdraw the endoscope’s insertion tube while
• Never perform flexibility adjustment, operate the bending
− If it becomes impossible to withdraw the transnasally
inserted endoscope, pull its distal end out of the mouth,
cut the flexible tube using wire cutters, and after ensuring
that the cut section will not injure the body cavity or nasal
cavity of the patient, withdraw the endoscope carefully.
Therefore, always prepare wire cutters in advance.
forcefully pull, twist or rotate the angulated bending section.
Patient injury, bleeding and/or perforation can result. It may
also become impossible to straighten the bending section
during an examination.
the bending section is locked in position. Patient injury,
bleeding and/or perforation can result.
section, feed air or perform suction, insert or withdraw the
endoscope’s insertion tube, or use endo-therapy accessories
without viewing the endoscopic image. Patient injury,
bleeding and/or perforation can result.
• Never perform flexibility adjustment, operate the bending
section, feed air or perform suction, insert or withdraw the
endoscope’s insertion tube, or use endo-therapy accessories
while the image is frozen. Patient injury, bleeding and/or
perforation can result.
• Regardless of the flexibility of the endoscope’s insertion tube,
never insert or withdraw the insertion tube abruptly or with
excessive force. Patient injury, bleeding and/or perforation
can result.
• The bending section will never bend to the RIGHT or LEFT
direction but to the UP or DOWN direction. To insert or
withdraw, operate the endoscope by considering the direction
in which the bending section is angulated. Never apply
excessive force to the RIGHT or LEFT direction when
inserting or withdrawing the endoscope. Patient injury,
bleeding and/or perforation can result (for GIF-N260 only).
• Never insert or withdraw the endoscope’s insertion tube, use
endo-therapy accessories while the image is magnified.
Patient injury, bleeding and/or perforation can result (when
using the GIF-H260Z, CF-H260AZL/I or using the image
magnification function of the video system center).
• Do not touch the light guide of the endoscope connector
immediately after removing it from the light source because it
is extremely hot. Operator or patient burns can result.
8
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 13

Important Information — Please Read Before Use
• When the endoscopic image does not appear on the monitor,
the CCD may have been damaged. Turn the video system
center OFF immediately. Continued power supply in such a
case will cause the distal end to become hot and could cause
operator and/or patient burns.
• If it is difficult to insert the endoscope, do not forcibly insert
the endoscope; stop the endoscopy. Forcible insertion can
result in patient injury, bleeding and/or perforation.
• When combining the endoscope with a splinting tube, there is
the risk of perforation or bleeding due to entanglement of the
mucous membrane, or of the tube to become separated from
the endoscope and remaining in the body. Before use, be
sure to read the instruction manual for the splinting tube to
fully understand its characteristics.
• Do not rely on the NBI imaging modality alone for primary
detection of lesions or to make a decision regarding any
potential diagnostic or therapeutic intervention.
• Do not pull the universal cord during an examination. The
endoscope connector will be pulled out from the output
socket of the light source and the endoscopic image will not
be visible.
• Do not coil the insertion tube or universal cord with a
diameter of less than 12 cm. Equipment damage can result.
• Do not touch the electrical contacts inside the electrical
connector. CCD damage may result.
• Do not apply shock to the distal end of the insertion tube,
particularly the objective lens surface at the distal end. Visual
abnormalities may result.
• Do not twist or bend the bending section with your hands.
Equipment damage may result.
• Do not squeeze the bending section forcefully. The covering
of the bending section may stretch or break and cause water
leaks.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
9
Page 14
Important Information — Please Read Before Use
• Turn the video system center OFF before connecting or
• The endoscope’s remote switches cannot be removed from
• If remote switch 1 does not return to the OFF position after
• Do not hit or bend the electrical contacts on the endoscope
disconnecting the videoscope cable from the electrical
connector on the endoscope. Turn the video system center
ON or OFF only when the videoscope cable is connected to
both the video system center and the electrical connector on
the endoscope. Failure to do so can result in equipment
damage, including destruction of the CCD.
the control section. Pressing, pulling or twisting them with
excessive force can break the switches and/or may cause
water leaks.
being pressed strongly from the side, gently pull the switch
upwards to return it to the OFF position.
connector. The connection to the light source may be
impaired and faulty contact can result.
• Do not attempt to bend the endoscope’s insertion tube with
excessive force. Otherwise, the insertion tube may be
damaged.
• Do not attempt to bend the endoscope’s insertion tube with
excessive force unless its flexibility is set to the most-rigid
position. Otherwise, the insertion tube may be damaged (for
endoscopes with flexibility adjustment only).
• Do not pull the magnification control cable during an
examination. The endoscope connector will be pulled out
from the output socket of the light source and the endoscopic
image will not be visible. The magnification control cable will
be pulled out from the endoscope’s zoom connector and the
endoscopic image will not zoom in or out (for CF-H260AZL/I
only).
• Turn the magnification controller OFF before connecting or
disconnecting the magnification control cable from the
endoscope’s zoom connector. Failure to do so can result in
equipment damage (for CF-H260AZL/I only).
• Do not pull the UPD cable during an examination. The
endoscope connector will be pulled out from the output
socket of the light source and the endoscopic image will not
be visible. The UPD cable will be pulled out from the UPD
scope connector and the scope model will not be visible (for
CF-Q260DL/I only).
10
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 15
Important Information — Please Read Before Use
• Turn the endoscope position detecting unit (UPD) OFF
before connecting or disconnecting the UPD cable from the
UPD scope connector. Turn the UPD ON or OFF only when
the UPD cable is connected to the UPD scope connector.
Failure to do so can result in UPD damage (for CF-Q260DL/I
only).
• To check the electromagnetic influence from other equipment
(any equipment other than this instrument or the components
that constitute this system), the system should be observed
to verify its normal operation in the configuration in which it
will be used.
• Electromagnetic interference may occur on this instrument
near equipment marked with the following symbol or other
portable and mobile RF (Radio Frequency) communications
equipment such as cellular phones. If electromagnetic
interference occurs, mitigation measures may be necessary,
such as reorienting or relocating this instrument, or shielding
the location.
This endoscope contains a memory chip that stores
information about the endoscope and communicates this
information to the video system center CV-260SL, CV-260.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
11
Page 16

Important Information — Please Read Before Use
Examples of inappropriate handling
Details on clinical endoscopic technique are the responsibility of trained
specialists. Patient safety in endoscopic examinations and endoscopic treatment
can be ensured through appropriate handling by the physician and the medical
facility. Examples of inappropriate handling are described below;
• Over-insufflating the lumen may cause patient pain, injury, bleeding
and/or perforation.
• Applying suction with the distal end in prolonged contact with the
mucosal surface, with higher suction pressure than required or with
prolonged suction time may cause bleeding and/or lesions.
• The endoscope has not been designed for use in retroflexed
observation in parts of the body other than the stomach. Performing
retroflexed observation in a narrow lumen may make it impossible to
straighten and/or withdraw the endoscope. Retroflexed observation in
parts of the body other than the stomach should be performed only
when the usefulness of doing so is determined to be greater than the
risk that is posed to the patient.
• Inserting, withdrawing and using endo-therapy accessories without a
clear endoscopic image may cause patient injury, burns, bleeding and/or
perforation.
• Inserting or withdrawing the endoscope, feeding air, applying suction or
operating the bending section without a clear endoscopic image may
cause patient injury, bleeding and/or perforation.
12
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 17

Chapter 1 Checking the Package Contents
Chapter 1 Checking the Package
Contents
Match all items in the package with the components shown below. Inspect each
item for damage. If the instrument is damaged, a component is missing or you
have any questions, do not use the instrument; immediately contact Olympus.
This instrument was not disinfected or sterilized before shipment.
Before using this instrument for the first time, reprocess it according to the
instructions described in the endoscope’s companion manual, the
“REPROCESSING MANUAL” whose cover lists the model of your endoscope.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
13
Page 18
Chapter 1 Checking the Package Contents
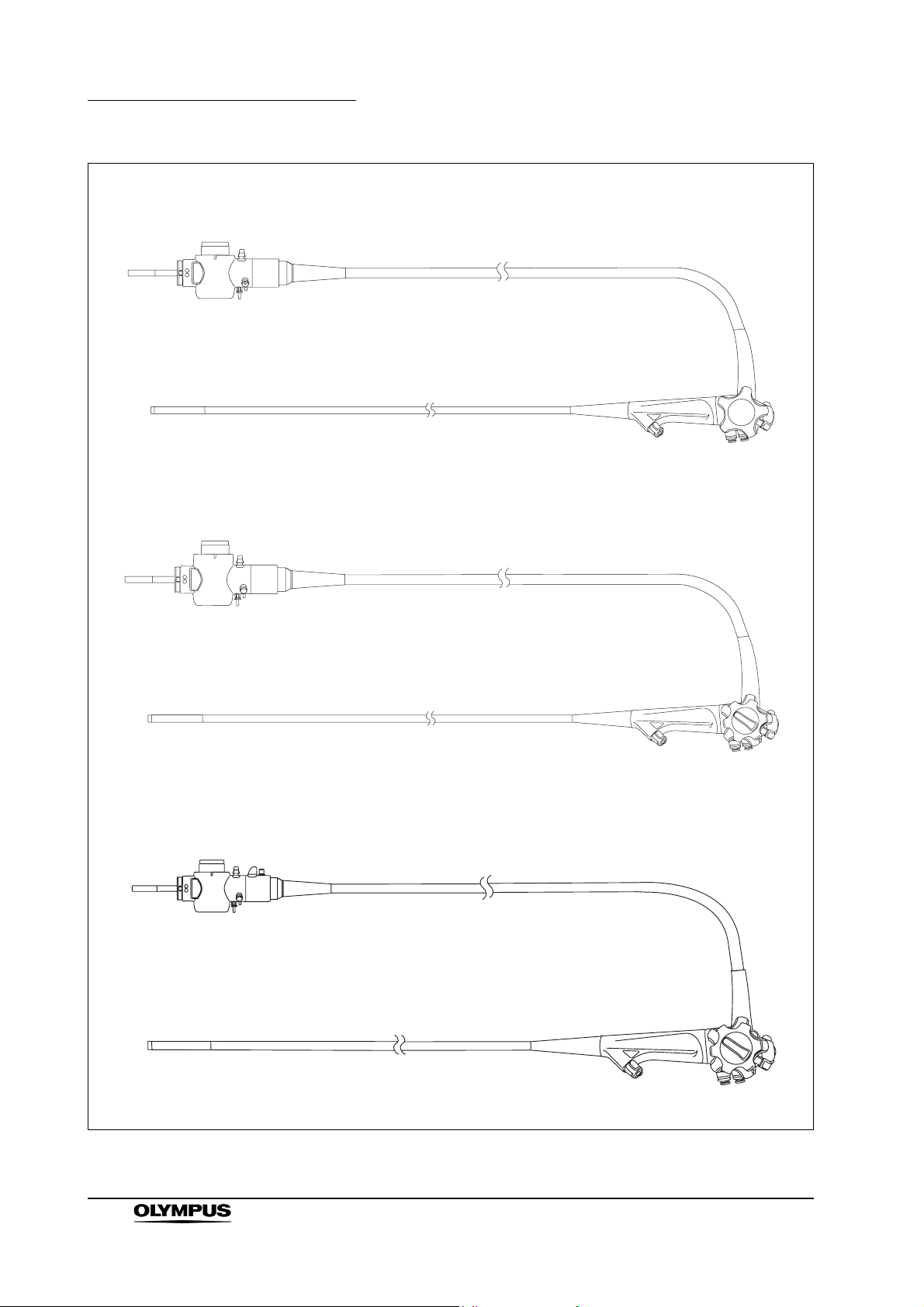
GIF-N260
GIF-XP260, GIF-XQ260, GIF-Q260, GIF-H260
Endoscope
GIF-H260Z
Endoscope
Endoscope
14
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 19
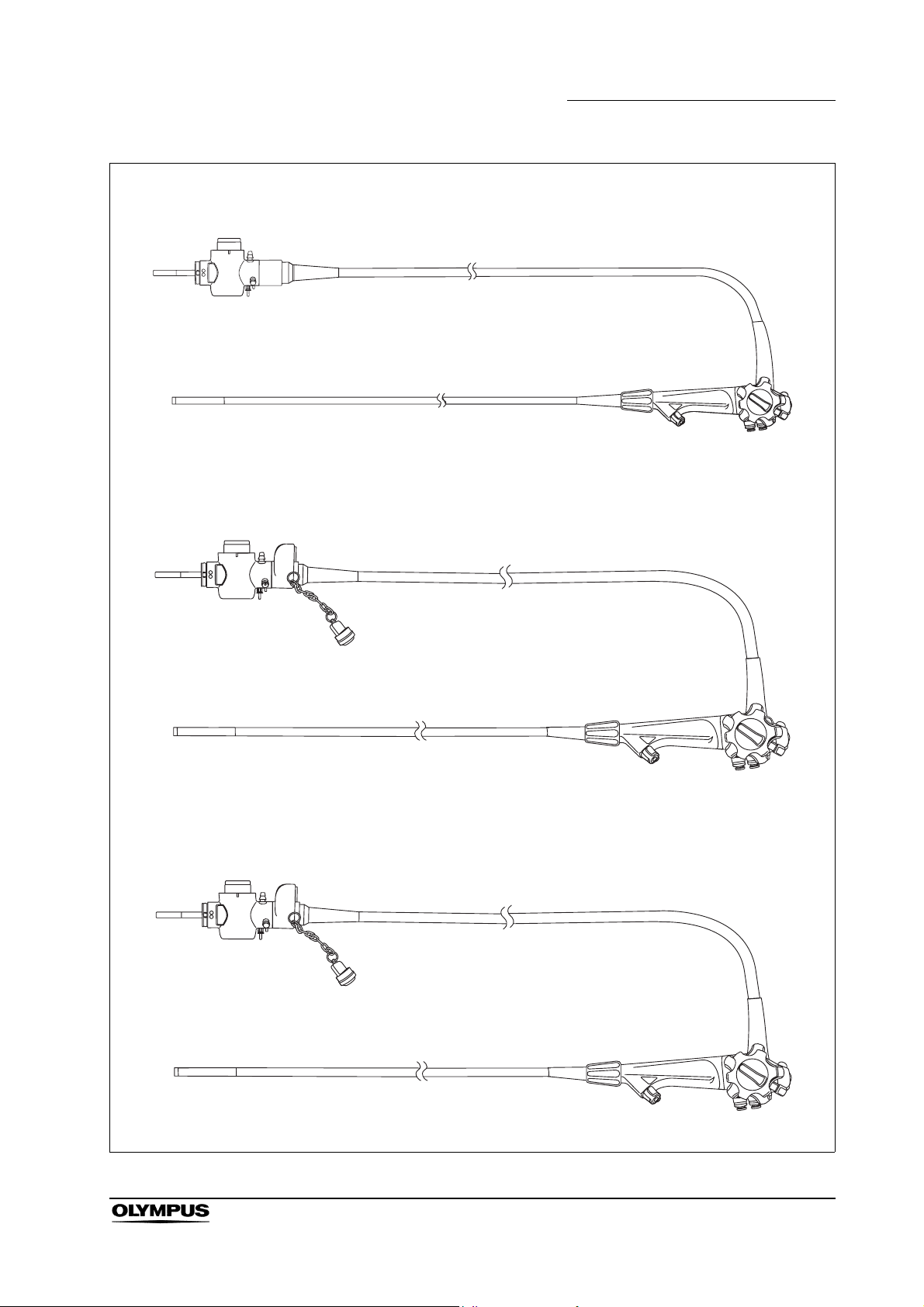
CF-Q260AL/I, CF-H260AL/I, PCF-Q260AL/I
CF-H260AZL/I
Chapter 1 Checking the Package Contents
Endoscope
CF-Q260DL/I
Endoscope
Endoscope
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
15
Page 20
Chapter 1 Checking the Package Contents
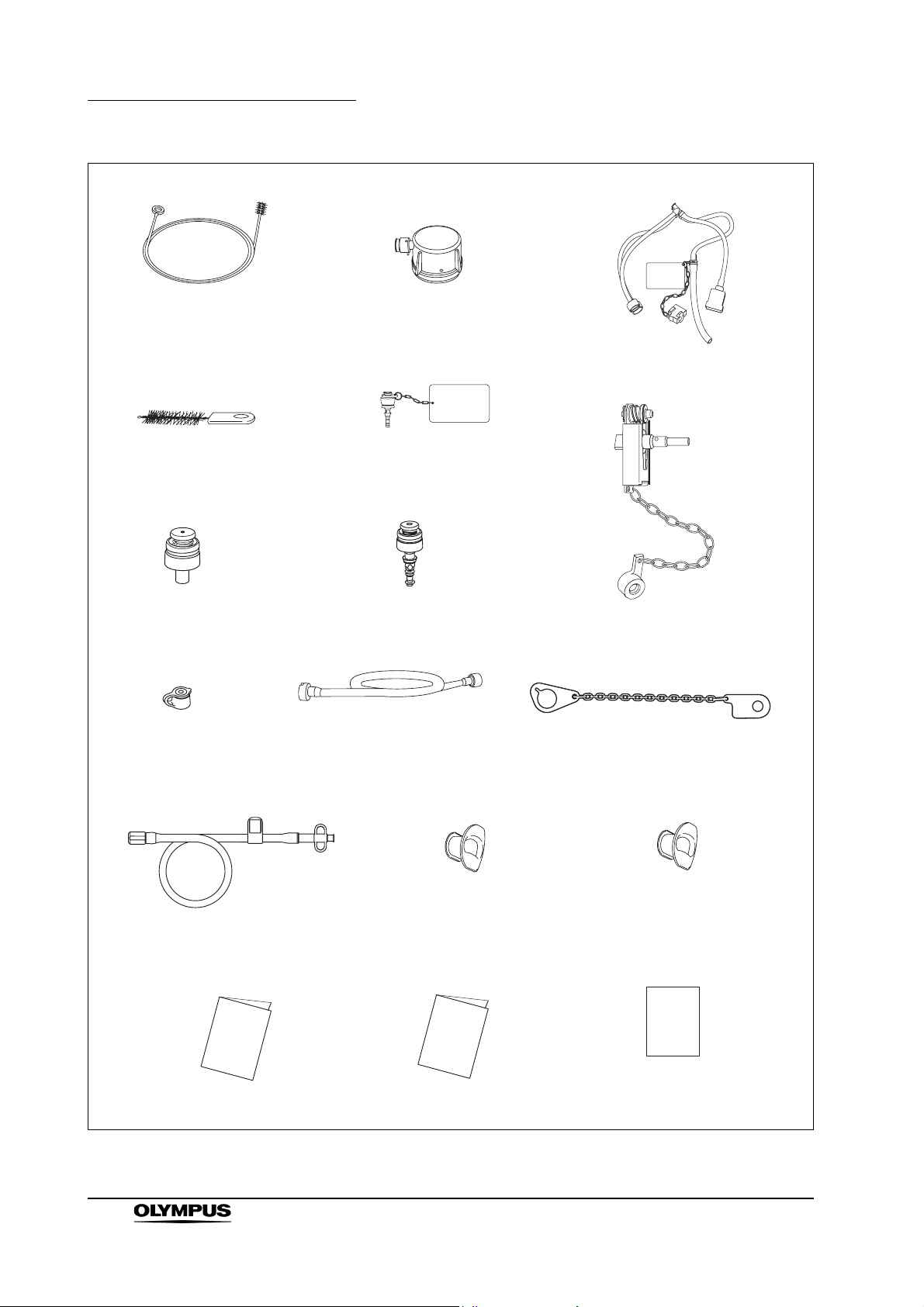
Channel cleaning brush (BW-20T) Water-resistant cap (MH-553)
Injection tube (MH-946)
Channel-opening cleaning
brush (MH-507)
Suction valve
(MH-443) (2 pcs)
Biopsy valve
(MB-358) (10 pcs)
Auxiliary water tube
(MAJ-855) (for GIF-H260Z only)
Suction cleaning adapter
(MH-856)
AW channel cleaning
adapter (MH-948)
Air/water valve
(MH-438) (2 pcs)
Mouthpiece
(MB-142 for GIF-XQ260,
GIF-Q260, GIF-H260,
GIF-H260Z) (2 pcs)
Channel plug (MH-944)
Chain for water-resistant cap (MAJ-1119)
Mouthpiece
(MA-474, MB-142 for
GIF-N260, GIF-XP260)
(1 pc each)
16
Operation manual
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Reprocessing manual
Instructions (leaflet type,
for endoscopes with
flexibility adjustment only)
Page 21

Chapter 1 Checking the Package Contents
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
17
Page 22
Chapter 2 Instrument Nomenclature and Specifications
Chapter 2 Instrument Nomenclature
and Specifications
2.1 Nomenclature
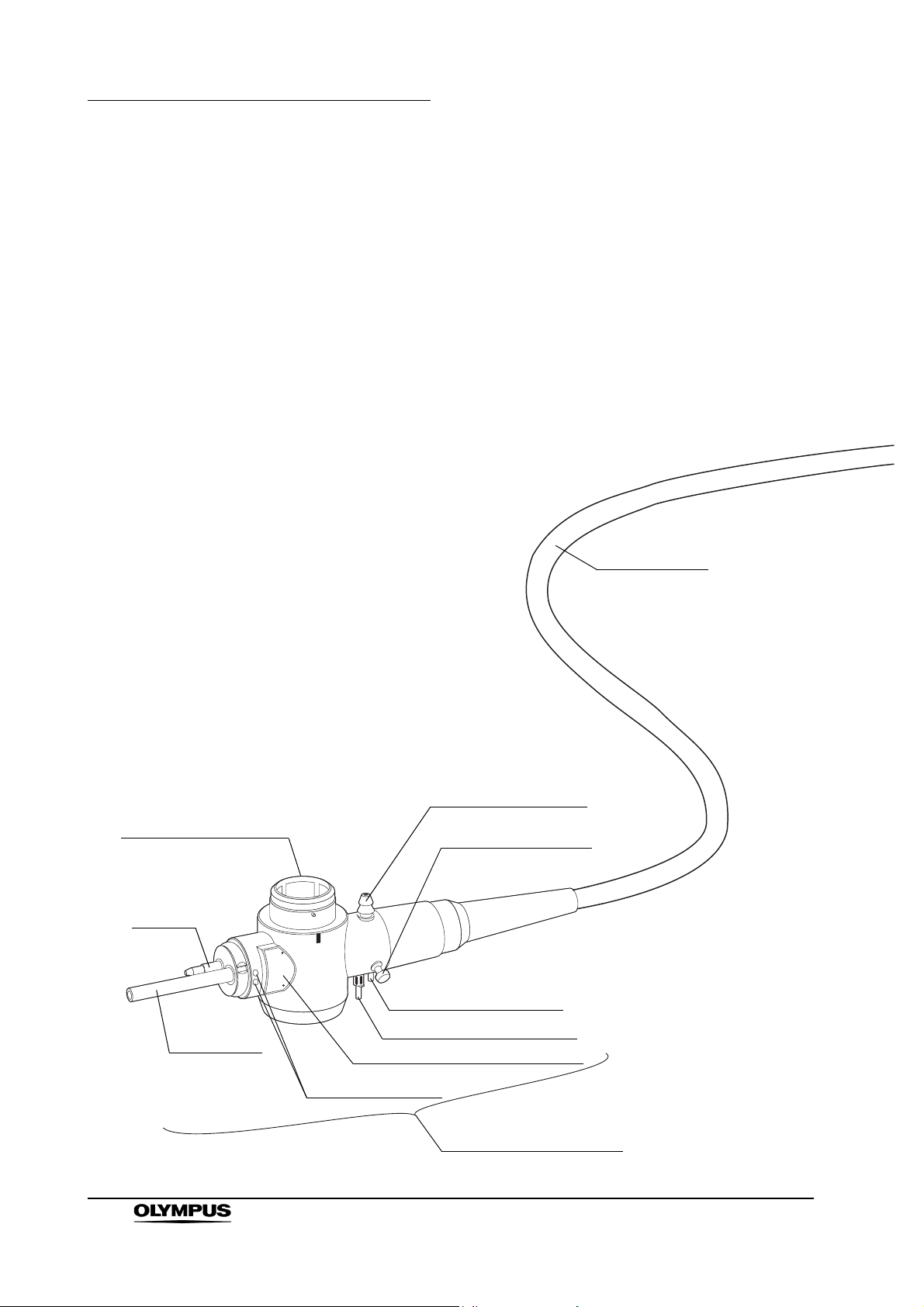
GIF-N260
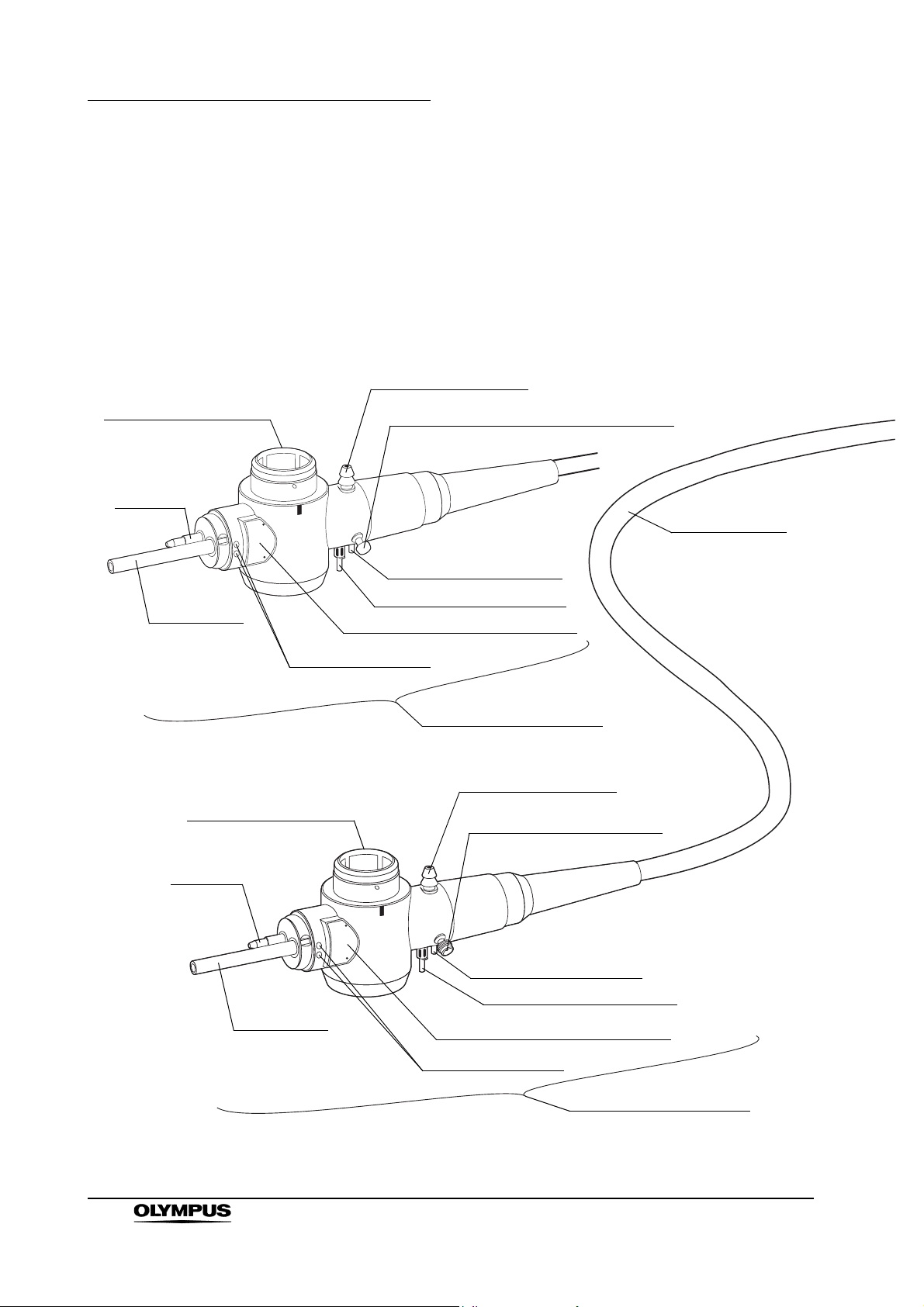
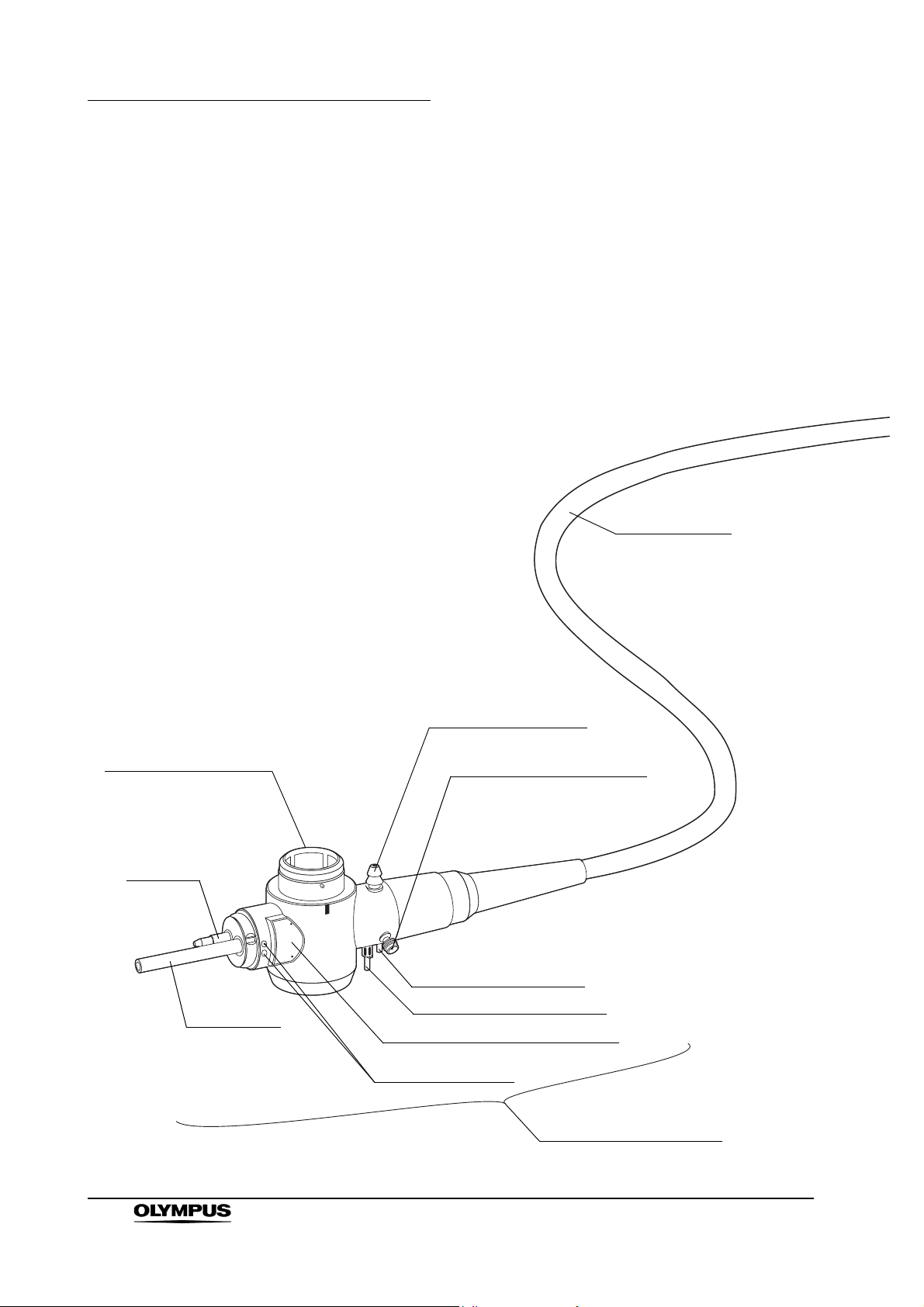
5. Electrical connector
Air pipe
Universal cord
1. Suction connector
26. Chain connector
3. Air supply connector
18
Light guide
3. Water supply connector
Product name and serial number
Electrical contacts
4. Endoscope connector
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 23
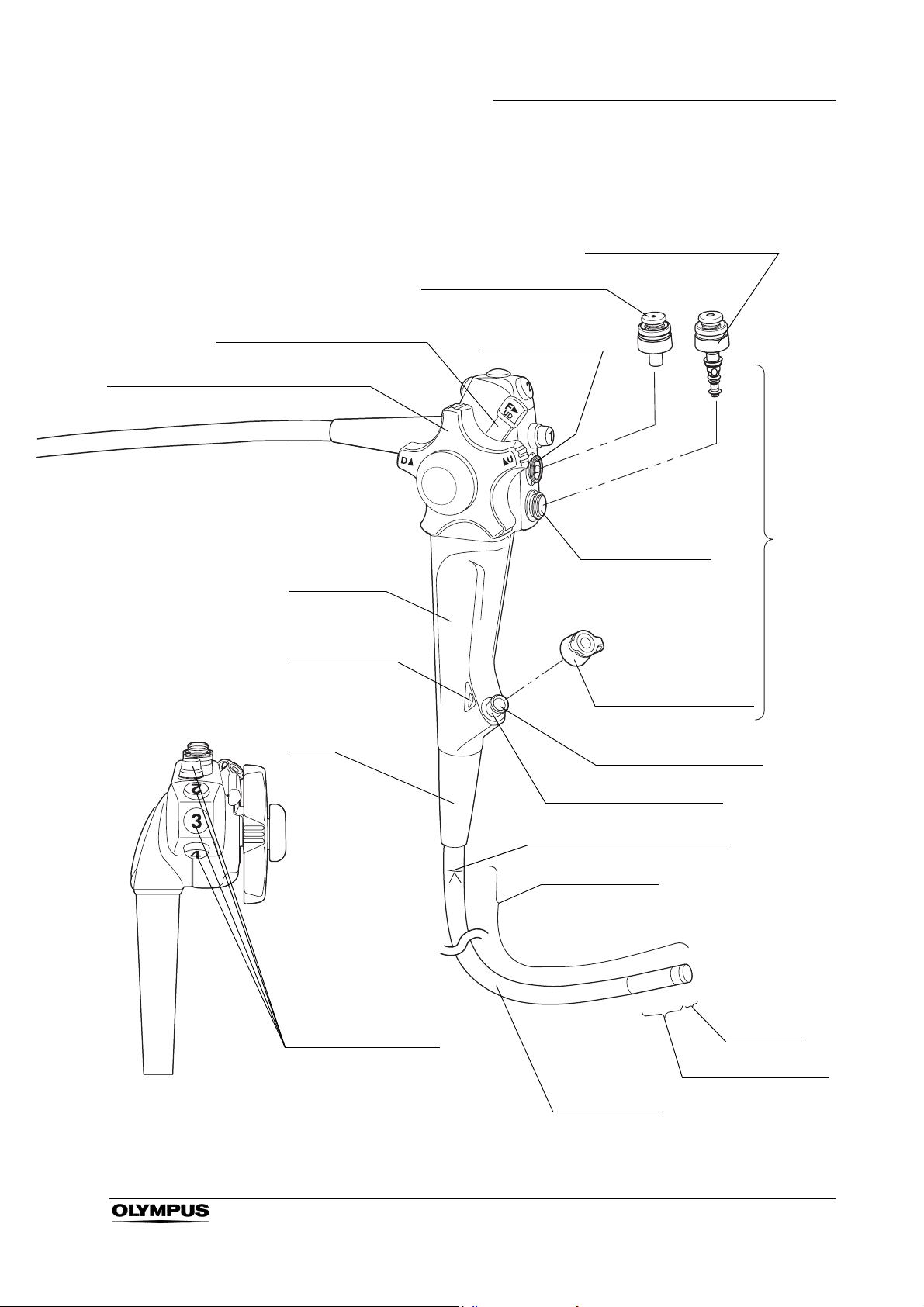
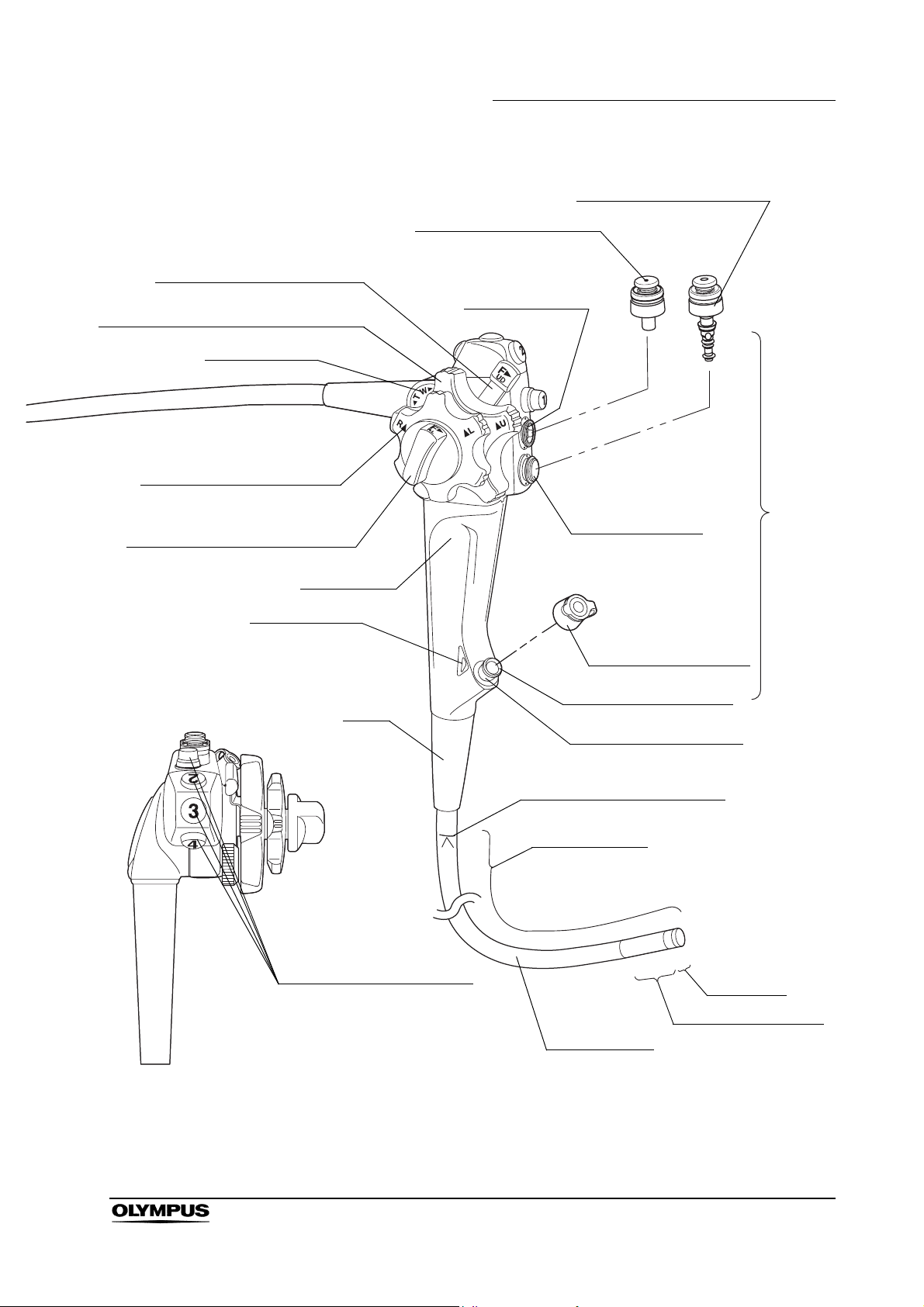
Chapter 2 Instrument Nomenclature and Specifications
8. Suction valve (MH-443)
9. Air/water valve (MH-438)
7. UP/DOWN angulation lock
6. UP/DOWN angulation control knob
Grip section
14. Color code
Boot
Suction cylinder
Air/water cylinder
Biopsy valve (MB-358)
10. Instrument channel
Control
section
Top view
Instrument channel port
11. Insertion tube limit mark
Working length
13. Remote switches
12. Bending section
Insertion tube
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Distal end
19
Page 24
Chapter 2 Instrument Nomenclature and Specifications
GIF-XP260, GIF-XQ260, GIF-Q260, GIF-H260
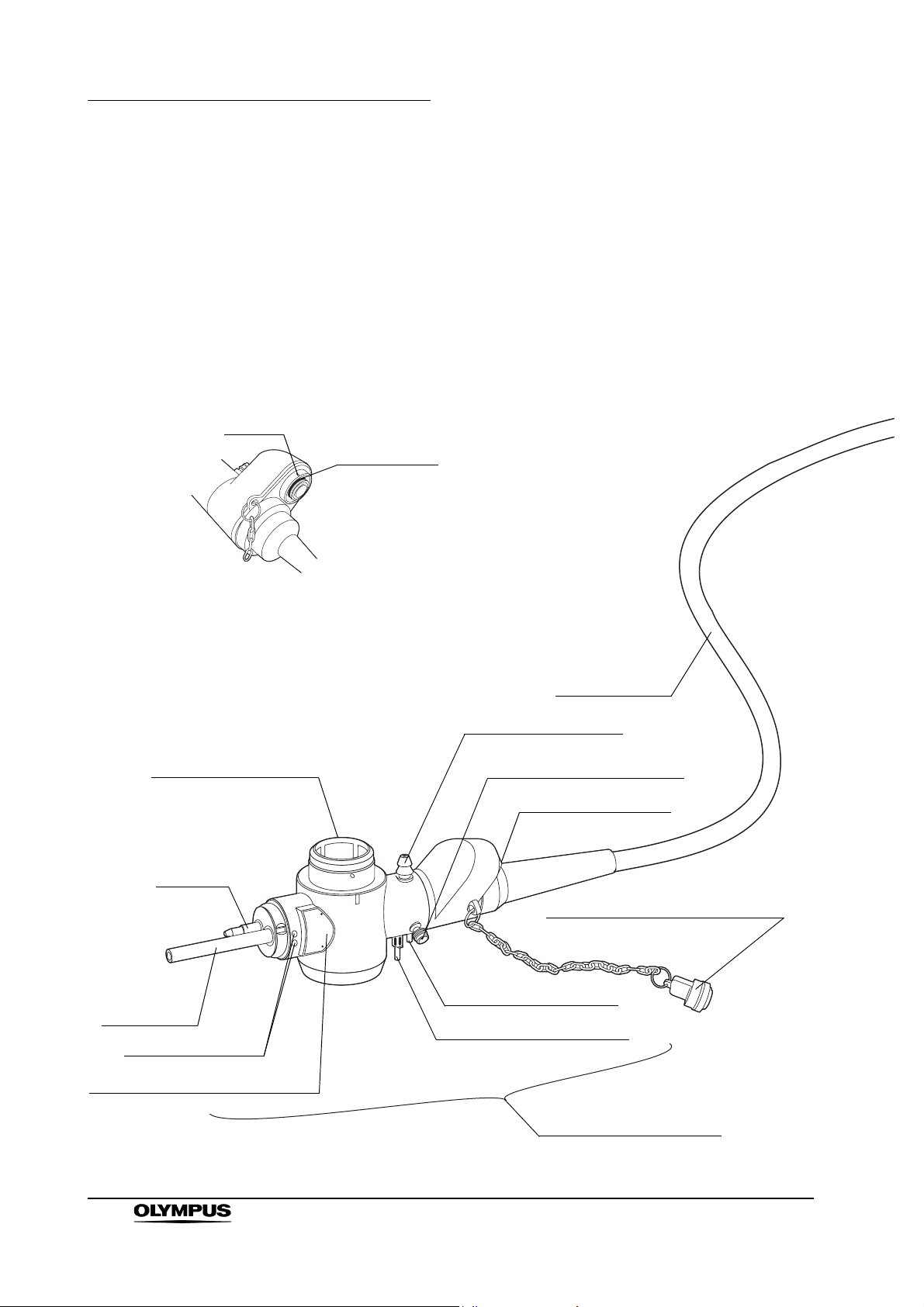
1. Suction connector
5. Electrical connector
Air pipe
Light guide
5. Electrical connector
26. Chain connector (for GIF-XP260 only)
Universal cord
3. Air supply connector
3. Water supply connector
Product name and serial number
Electrical contacts
4. Endoscope connector
1. Suction connector
2. S-cord connector mount
(except GIF-XP260)
20
Air pipe
3. Air supply connector
3. Water supply connector
Light guide
Product name and serial number
Electrical contacts
4. Endoscope connector
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 25
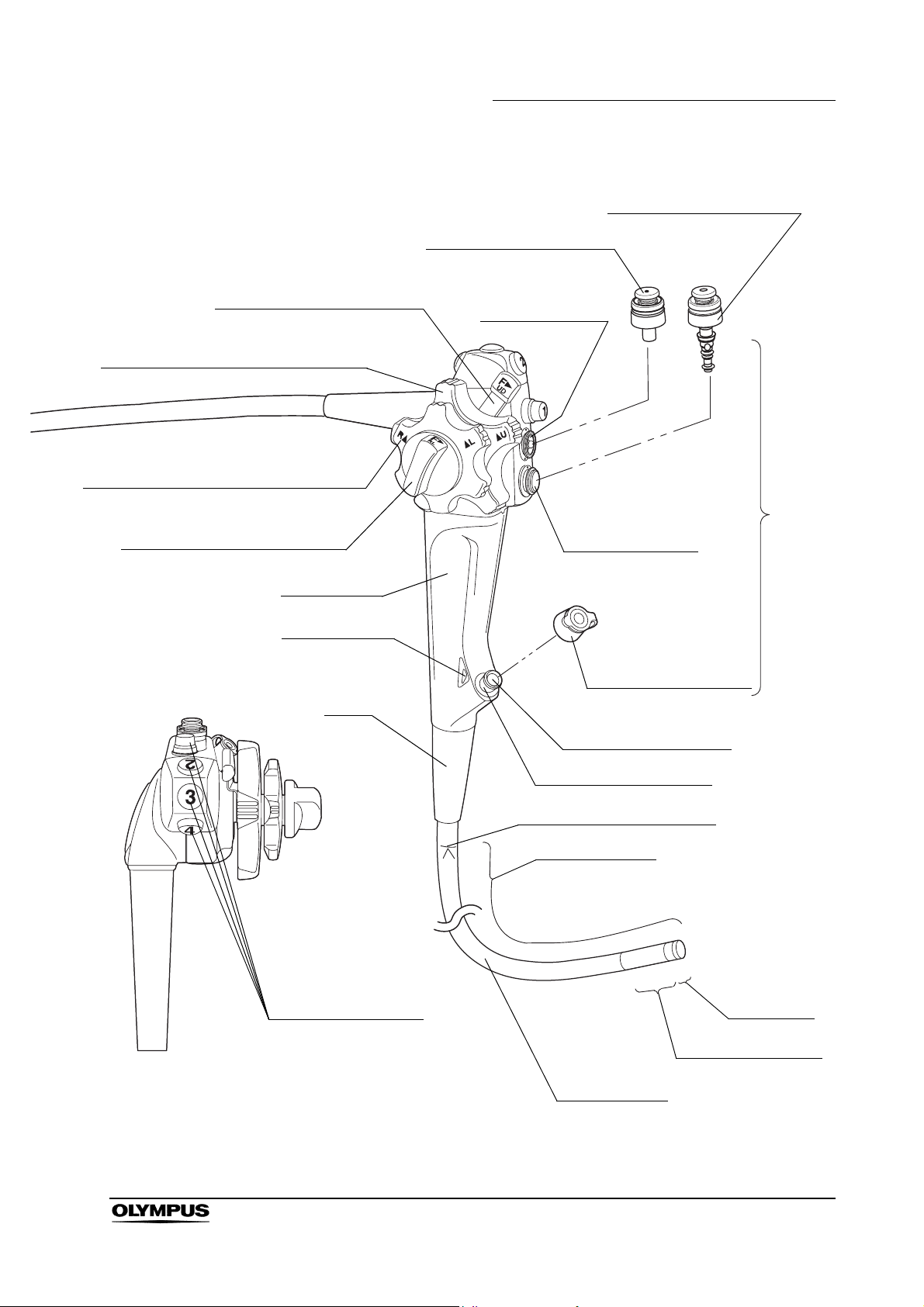
Chapter 2 Instrument Nomenclature and Specifications
8. Suction valve (MH-443)
9. Air/water valve (MH-438)
7. UP/DOWN angulation lock
6. UP/DOWN angulation control knob
16. RIGHT/LEFT angulation control knob
15. RIGHT/LEFT angulation lock
Grip section
14. Color code
Boot
Suction cylinder
Control
section
Air/water cylinder
Biopsy valve (MB-358)
10. Instrument channel
Instrument channel port
11. Insertion tube limit mark
Working length
13. Remote switches
Top view
Insertion tube
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Distal end
12. Bending section
21
Page 26
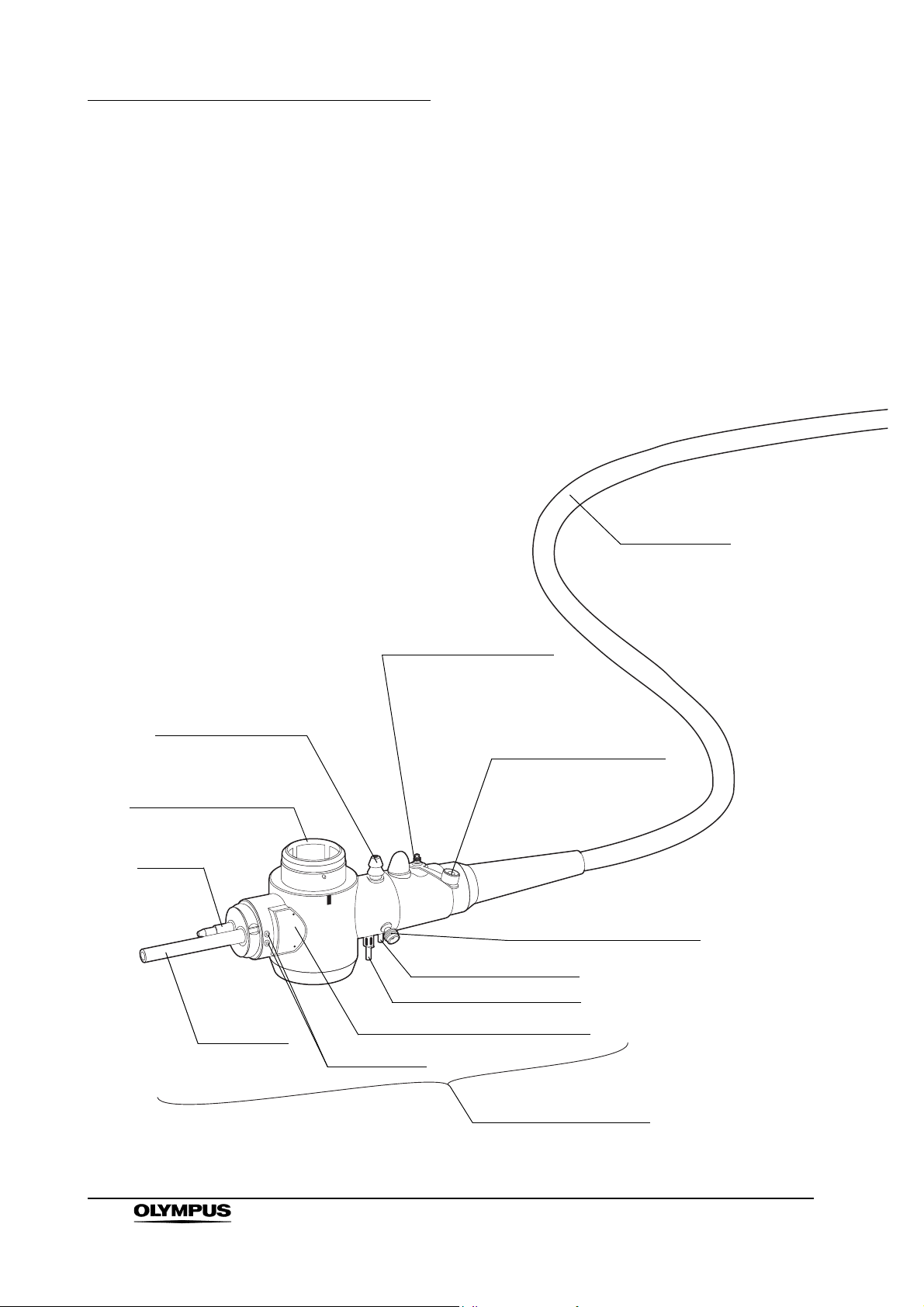
Chapter 2 Instrument Nomenclature and Specifications
GIF-H260Z
Universal cord
1. Suction connector
5. Electrical connector
Air pipe
Light guide
19. Auxiliary water inlet
Auxiliary water inlet cap
(MAJ-215)
2. S-cord connector mount
3. Air supply connector
3. Water supply connector
Product name and serial number
Contact pins
22
4. Endoscope connector
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 27
7. UP/DOWN angulation lock
6. UP/DOWN angulation control knob
18. Zoom lever
16. RIGHT/LEFT angulation
control knob
15. RIGHT/LEFT angulation lock
Chapter 2 Instrument Nomenclature and Specifications
8. Suction valve (MH-443)
Suction cylinder
Air/water cylinder
9. Air/water valve (MH-438)
Control
section
Top view
Grip section
14. Color code
Boot
13. Remote switches 1 to 4
Biopsy valve (MB-358)
10. Instrument channel
Instrument channel port
11. Insertion tube limit mark
Working length
Distal end
12. Bending section
Insertion tube
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
23
Page 28
Chapter 2 Instrument Nomenclature and Specifications
CF-Q260AL, CF-Q260AI, CF-H260AL, CF-H260AI,
PCF-Q260AL, PCF-Q260AI
Universal cord
5. Electrical connector
Air pipe
Light guide
1. Suction connector
2. S-cord connector mount
3. Air supply connector
3. Water supply connector
Product name and serial number
Electrical contacts
4. Endoscope connector
24
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 29

Chapter 2 Instrument Nomenclature and Specifications
8. Suction valve (MH-443)
9. Air/water valve (MH-438)
7. UP/DOWN angulation lock
6. UP/DOWN angulation control knob
16. RIGHT/LEFT angulation control knob
15. RIGHT/LEFT angulation lock
Grip section
14. Color code
Mark
17. Flexibility adjustment ring
Suction cylinder
Control
section
Air/water cylinder
Biopsy valve (MB-358)
10. Instrument channel
Instrument channel port
Marks
Boot
11. Insertion tube limit mark
Working length
13. Remote switches
Top view
Insertion tube
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Distal end
12. Bending section
25
Page 30
Chapter 2 Instrument Nomenclature and Specifications
CF-H260AZL, CF-H260AZI
Mark3
22. Seal ring
Front view of the zoom scope connector
5. Electrical connector
Air pipe
Light guide
Electrical contacts
Universal cord
1. Suction connector
2. S-cord connector mount
20. Zoom connector
21. Water-resistant cap (MAJ-583)
3. Air supply connector
3. Water supply connector
Product name and serial number
26
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
4. Endoscope connector
Page 31

7. UP/DOWN angulation lock
6. UP/DOWN angulation control knob
18. Zoom lever
16. RIGHT/LEFT angulation control knob
15. RIGHT/LEFT angulation lock
Chapter 2 Instrument Nomenclature and Specifications
9. Air/water valve (MH-438)
8. Suction valve (MH-443)
Suction cylinder
Control
section
Grip section
14. Color code
Mark
17. Flexibility adjustment ring
Boot
Air/water cylinder
Biopsy valve (MB-358)
10. Instrument channel
Instrument channel port
Marks
11. Insertion tube limit mark
Working length
13. Remote switches
Top view
Insertion tube
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Distal end
12. Bending section
27
Page 32

Chapter 2 Instrument Nomenclature and Specifications
CF-Q260DL, CF-Q260DI
Mark
22. Seal ring
Front view of the UPD scope connector
5. Electrical connector
Air pipe
Light guide
Electrical contacts
Universal cord
1. Suction connector
2. S-cord connector mount
23. UPD scope connector
24. Water-resistant cap (MAJ-942)
3. Air supply connector
3. Water supply connector
28
Product name and serial number
4. Endoscope connector
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 33

7. UP/DOWN angulation lock
6. UP/DOWN angulation control knob
16. RIGHT/LEFT angulation control knob
Chapter 2 Instrument Nomenclature and Specifications
9. Air/water valve (MH-438)
8. Suction valve (MH-443)
Suction cylinder
15. RIGHT/LEFT angulation lock
Grip section
14. Color code
17. Flexibility adjustment ring
Mark
Air/water cylinder
Biopsy valve (MB-358)
10. Instrument channel
Instrument channel port
Marks
Boot
11. Insertion tube limit mark
Working length
Control
section
13. Remote switches
Top view
Insertion tube
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Distal end
12. Bending section
29
Page 34

Chapter 2 Instrument Nomenclature and Specifications
2.2 Endoscope functions
1. Suction connector
Connects the endoscope to the suction tube of the suction pump.
2. S-cord connector mount (except GIF-N260, GIF-XP260)
Connects the endoscope with the Olympus electrosurgical unit via the
S-cord. The S-cord conducts leakage current from the endoscope to the
electrosurgical unit. To connect the S-cord, refer to the instruction manual
for the electrosurgical unit. Connect the fitting of the chain for
water-resistant cap to this mount as required (see Section 2.4 on page 46).
3. Water supply connector and air supply connector
Connects the endoscope to the water container via the water container tube,
to supply water to the distal end of the endoscope.
4. Endoscope connector
Connects the endoscope to the output socket of the light source and
transmits light from the light source to the endoscope.
5. Electrical connector
Connects the endoscope to the video system center via the videoscope
cable. The endoscope contains a memory chip that stores information about
the endoscope and communicates this information to the video system
center CV-260SL, CV-260. For more details, refer to the instruction manual
of the CV-260SL, CV-260.
6. UP/DOWN angulation control knob
When this knob is turned in the “ U” direction, the bending section moves
UP; when the knob is turned in the “D ” direction, the bending section
moves DOWN.
7. UP/DOWN angulation lock
Moving this lock in the “F ” direction frees angulation. Moving the lock in
the opposite direction locks the bending section at any desired position.
8. Suction valve (MH-443)
This valve is depressed to activate suction. The valve is used to remove any
fluid, debris, flatus or air from the patient.
9. Air/water valve (MH-438)
The hole in this valve is covered to insufflate air and the valve is depressed
to feed water for lens washing. It also can be used to feed air to remove any
fluid or debris adhering to the objective lens.
30
10. Instrument channel
The instrument channel functions as:
− channel for the insertion of endo-therapy accessories
− suction channel
− fluid feed channel (from a syringe via the biopsy valve)
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 35

Chapter 2 Instrument Nomenclature and Specifications
11. Insertion tube limit mark
This mark shows the maximum point to which the endoscope may be
inserted into the patient’s body.
12. Bending section
This section moves the distal end of the endoscope when the UP/DOWN
and RIGHT/LEFT angulation control knobs are operated (the GIF-N260 has
only the UP/DOWN angulation control knob).
13. Remote switches 1 to 4
The functions of remote switches 1 to 4 can be selected on the video system
center. When selecting the functions, also refer to the instruction manual for
the video system center.
14. Color code
This code is used to quickly determine the compatibility of endo-therapy
accessories. The endoscope can be used with endo-therapy accessories
that have the same color code.
• Blue: GIF-N260, GIF-XP260
• Yellow: GIF-XQ260, GIF-Q260, GIF-H260, GIF-H260Z,
CF-Q260AL/I, CF-H260AZL/I, PCF-Q260AL/I,
CF-Q260DL/I
• Orange: CF-H260AL/I
15. RIGHT/LEFT angulation lock (except GIF-N260)
Turning this lock in the “F ” direction frees angulation. Turning the lock in
the opposite direction locks the bending section at any desired position.
16. RIGHT/LEFT angulation control knob (except GIF-N260)
When this knob is turned in the “R ” direction, the bending section moves
RIGHT; when the knob is turned in the “ L” direction, the bending section
moves LEFT.
17. Flexibility adjustment ring (for endoscopes with flexibility adjustment only)
Turn this ring to adjust the flexibility of the insertion tube.
When the “z” mark on the ring is aligned with the “ ” mark at the bottom of
the grip section, the insertion tube is most flexible. To decrease the flexibility,
turn the ring so that the numbers are aligned with the “ ” mark (“3”
corresponds to the most-rigid condition). As the ring is turned from “z” to
“3”, the insertion tube’s flexibility gradually decreases.
18. Zoom lever (for GIF-H260Z, CF-H260AZL/I only)
Moving this lever toward “ T” magnifies the monitor image (close-up
observation). Moving the lever toward “W ” reduces the monitor image
(wide-angle observation).
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
31
Page 36

Chapter 2 Instrument Nomenclature and Specifications
19. Auxiliary water inlet (for GIF-H260Z only)
Connect the auxiliary water tube here. Feed water from this inlet through the
auxiliary water channel when necessary, (e.g. when blood adheres to
mucous membrane in the patient’s body cavity). When the auxiliary water
inlet is not being used, make sure that it is covered by the auxiliary water
inlet cap.
20. Zoom connector (for CF-H260AZL/I only)
This connector connects the endoscope to the magnification controller via
the magnification control cable.
21. Water-resistant cap (MAJ-583) (for CF-H260AZL/I only)
This cap is attached to the zoom connector for protection against water
penetration. If you purchase a water-resistant cap separately, attach its
chain to the endoscope.
22. Seal ring (for CF-H260AZL/I only)
This ring protects the zoom connector against water penetration when the
water-resistant cap (MAJ-583) is attached.
23. UPD scope connector (for CF-Q260DL/I only)
This connector connects the endoscope to the endoscope position detecting
unit (UPD) via the UPD cable.
24. Water-resistant cap (MAJ-942) (for CF-Q260DL/I only)
This cap is attached to the UPD scope connector for protection against
water penetration. If you purchase a water-resistant cap separately, attach
its chain to the endoscope.
25. Seal ring (for CF-Q260DL/I only)
This ring protects the UPD scope connector against water penetration when
the water-resistant cap (MAJ-942) is attached.
26. Chain connector (for GIF-N260, GIF-XP260 only)
This connector connects the fitting part of the chain for water-resistant cap
as required. Do not connect the S-cord of the electrosurgical unit.
32
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 37

2.3 Specifications
Environment
Chapter 2 Instrument Nomenclature and Specifications
Operating
environment
Transportation and
storage
environment
Ambient temperature 10 – 40°C
Relative humidity 30 – 85%
Atmospheric pressure 700 – 1060 hPa
Ambient temperature –47 to 70°C
Relative humidity 10 – 95%
Atmospheric pressure 700 – 1060 hPa
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
33
Page 38

Chapter 2 Instrument Nomenclature and Specifications
Specifications
Endoscope functions
Model
GIF-N260
∗
1
Optical system Field of view
Direction of view Forward viewing
Depth of field 3 – 100 mm
Insertion tube Distal end outer diameter ø4.9mm
Distal end enlarged 1. Air/water nozzle
2. Light guide lens
3. Objective lens
4. Instrument channel outlet
RIGHT LEFT
Insertion tube outer
diameter
Working length 110 0 m m
Instrument
channel
Channel inner diameter
Minimum visible distance 3 mm from the distal end
∗2
3.
ø5.2mm
120
°
UP
DOWN
ø2mm
1.
4.2.
34
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
Air flow rate
Note: Standard when CLV-260 (high
air pressure) is used.
Bending section Angulation range
Total length 1420 mm
NBI observation
∗3
UP 210
3
25 cm
/s
°, DOWN 120°
Available
∗1 GIF-N260 cannot be used to perform high-frequency cauterization or laser
cauterization.
∗2 Normal value
∗3 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 39

Chapter 2 Instrument Nomenclature and Specifications
Model
Optical system Field of view
Direction of view Forward viewing
Depth of field 3 – 100 mm
Insertion tube Distal end outer
diameter
Distal end enlarged 1. Air/water nozzle
∗
UP
1
1.
4.2.
GIF-XP260
120°
ø5mm
2. Light guide lens
3. Objective lens
4. Instrument channel outlet
3.
RIGHT LEFT
DOWN
Insertion tube outer
diameter
Working length 1030 mm
Instrument
channel
Air flow rate
Bending section Angulation range
Total l e ngth 1350 mm
NBI observation
Channel inner
diameter
Minimum visible
distance
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
∗3
∗2
Note: Standard when CLV-260 (high air
pressure) is used.
ø6.5mm
ø2mm
3 mm from the distal end
3
25 cm
°, DOWN 90°,
UP 210
RIGHT 100°, LEFT 100°
Available
/s
∗1 GIF-XP260 cannot be used to perform high-frequency cauterization or
laser cauterization.
∗2 Normal value
∗3 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
35
Page 40

Chapter 2 Instrument Nomenclature and Specifications
Model GIF-XQ260
Optical system Field of view
Direction of view Forward viewing
Depth of field 3 – 100 mm
140°
Insertion tube Distal end outer
diameter
Distal end enlarged 1. Air/water nozzle
Insertion tube outer
diameter
Working length 1030 mm
Instrument
channel
Channel inner
diameter
Minimum visible
distance
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
∗1
ø9mm
2. Light guide lens
3. Objective lens
4. Instrument channel outlet
UP
1.
RIGHT LEFT
DOWN
ø9mm
ø2.8mm
3 mm from the distal end
2.
4.3.
36
Air flow rate
Note: Standard when CLV-260 (high air
pressure) is used.
Bending section Angulation range
RIGHT 100°, LEFT 100°
Total length 1350 mm
NBI observation
∗2
UP 210
25 cm3/s
°, DOWN 90°,
Available
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 41

Chapter 2 Instrument Nomenclature and Specifications
Model GIF-Q260
Optical system Field of view
Direction of view Forward viewing
Depth of field 3 – 100 mm
140°
Insertion tube Distal end outer
diameter
Distal end enlarged 1. Air/water nozzle
Insertion tube outer
diameter
Working length 1030 mm
Instrument
channel
Channel inner
diameter
Minimum visible
distance
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
∗1
ø9.2mm
2. Light guide lens
3. Objective lens
4. Instrument channel outlet
UP
1.
RIGHT LEFT
DOWN
ø9.2mm
ø2.8mm
3 mm from the distal end
2.
4.3.
Air flow rate
Note: Standard when CLV-260 (high air
pressure) is used.
Bending section Angulation range
RIGHT 100°, LEFT 100°
Total l e ngth 1350 mm
NBI observation
∗2
UP 210
25 cm3/s
°, DOWN 90°,
Available
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
37
Page 42

Chapter 2 Instrument Nomenclature and Specifications
Model GIF-H260
Optical system Field of view
Direction of view Forward viewing
Depth of field 3 – 100 mm
140°
Insertion tube Distal end outer
diameter
Distal end enlarged 1. Air/water nozzle
Insertion tube outer
diameter
Working length 1030 mm
Instrument
channel
Channel inner
diameter
Minimum visible
distance
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
∗1
ø9.8mm
2. Light guide lens
3. Objective lens
4. Instrument channel outlet
UP
1.
RIGHT LEFT
DOWN
ø9.5mm
ø2.8mm
3 mm from the distal end
2.
4.3.
38
Air flow rate
Note: Standard when CLV-260 (high air
pressure) is used.
Bending section Angulation range
RIGHT 100°, LEFT 100°
Total length 1350 mm
NBI observation
∗2
UP 210
25 cm3/s
°, DOWN 90°,
Available
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 43

Chapter 2 Instrument Nomenclature and Specifications
Model GIF-H260Z
Optical system Field of view 140° (WIDE position)
75° (TELE position)
Direction of view Forward viewing
Depth of field 7 – 100 mm (WIDE position)
1.5 – 3 mm (TELE position)
(The focus range is switchable.)
Insertion tube Distal end outer diameter ø 10.8 mm
Distal end enlarged 1. Air/water nozzle
2. Light guide lens
3. Objective lens
4. Instrument channel
5. Auxiliary water channel
UP
2.
3.
RIGHT
1.
5.
DOWN
Insertion tube outer
diameter
Working length 1030 mm
Instrument
channel
Air flow rate
Bending section Angulation range UP 210°, DOWN 90°,
Total l e ngth 1350 mm
NBI observation
Channel inner diameter
Minimum visible distance 4 mm from the distal end
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
∗2
∗1
Note: Standard when CLV-260 (high
air pressure) is used.
ø 10.5 mm
ø2.8mm
(in WIDE position)
25 cm
RIGHT 100°, LEFT 100°
Available
LEFT
4.
3
/s
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
39
Page 44

Chapter 2 Instrument Nomenclature and Specifications
Model CF-Q260AL CF-Q260AI
Optical system Field of view
Direction of view Forward viewing
Depth of field 4 – 100 mm
140°
Insertion tube Distal end outer
diameter
Distal end enlarged 1. Air/water nozzle
Insertion tube outer
diameter
Working length 1680 mm 1330 mm
Range of the flexibility
adjustment
Instrument
channel
Channel inner
diameter
Minimum visible
distance
∗1
ø 12.2 mm
2. Light guide lens
3. Objective lens
4. Instrument channel outlet
UP
3.
RIGHT LEFT
DOWN
ø12mm
The rigidity in the most-rigid condition is
about twice that in the most-flexible
condition.
ø3.2mm
4 mm from the distal end
1.
2.4.
40
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
Air flow rate
Note: Standard when CLV-260 (high air
pressure) is used.
Bending section Angulation range
RIGHT 160°, LEFT 160°
Total length 2005 mm 1655 mm
NBI observation
∗2
UP 180
30 cm3/s
°, DOWN 180°,
Available
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 45

Chapter 2 Instrument Nomenclature and Specifications
Model CF-Q260DL CF-Q260DI
Optical system Field of view
Direction of view Forward viewing
Depth of field 5 – 100 mm
140°
Insertion tube Distal end outer
diameter
Distal end enlarged 1. Air/water nozzle
Insertion tube outer
diameter
Working length 1680 mm 1330 mm
Range of the flexibility
adjustment
Instrument
channel
Channel inner
diameter
Minimum visible
distance
∗1
ø12.2mm
2. Light guide lens
3. Objective lens
4. Instrument channel
UP
3.
RIGHT LEFT
DOWN
ø12.4mm
The rigidity in the most-rigid condition is
about twice that in the most-flexible
condition.
ø3.2mm
5 mm from the distal end
1.
2.4.
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
Air flow rate
Note: Standard when CLV-260 (high air
pressure) is used.
Bending section Angulation range
RIGHT 160°, LEFT 160°
Total l e ngth 2005 mm 1655 mm
NBI observation
∗2
UP 180
30 cm3/s
°, DOWN 180°,
Available
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
41
Page 46

Chapter 2 Instrument Nomenclature and Specifications
Model CF-H260AL CF-H260AI
Optical system Field of view
Direction of view Forward viewing
Depth of field 5 – 100 mm
140°
Insertion tube Distal end outer
diameter
Distal end enlarged 1. Air/water nozzle
Insertion tube outer
diameter
Working length 1680 mm 1330 mm
Range of the flexibility
adjustment
Instrument
channel
Channel inner
diameter
Minimum visible
distance
∗1
ø 13.2 mm
2. Light guide lens
3. Objective lens
4. Instrument channel outlet
UP
3.
RIGHT LEFT
DOWN
ø 12.9 mm
The rigidity in the most-rigid condition is
about twice that in the most-flexible
condition.
ø3.7mm
4 mm from the distal end
1.
2.4.
42
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
Air flow rate
Note: Standard when CLV-260 (high air
pressure) is used.
Bending section Angulation range
RIGHT 160°, LEFT 160°
Total length 2005 mm 1655 mm
NBI observation
∗2
UP 180
30 cm3/s
°, DOWN 180°,
Available
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 47

Chapter 2 Instrument Nomenclature and Specifications
Model CF-H260AZL CF-H260AZI
Optical system Field of view
Direction of view Forward viewing
Depth of field 7 – 100 mm (WIDE position)
Insertion tube Distal end outer diameter ø 13.6 mm
Distal end enlarged 1. Air/water nozzle
140° (WIDE position)
80
° (TELE position)
2 – 3 mm (TELE position)
(The focus range is switchable)
2. Light guide lens
3. Objective lens
4. Instrument channel
UP
3.
RIGHT LEFT
DOWN
1.
2.4.
Insertion tube outer
diameter
Working length 1680 mm 1330 mm
Range of the flexibility
adjustment
Instrument
channel
Air flow rate
Bending section Angulation range
Channel inner diameter
Minimum visible distance 4 mm from the distal end
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
ø 12.9 mm
The rigidity in the most-rigid condition
is about twice that in the most-flexible
condition.
∗1
Note: Standard when CLV-260 (high
air pressure) is used.
ø3.2mm
(in WIDE position)
3
/s
30 cm
UP 180
RIGHT 160°, LEFT 160°
°, DOWN 180°,
Total l e ngth 2005 mm 1655 mm
NBI observation
∗2
Available
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
43
Page 48

Chapter 2 Instrument Nomenclature and Specifications
Model PCF-Q260AL PCF-Q260AI
Optical system Field of view
Direction of view Forward viewing
Depth of field 5 – 100 mm
140°
Insertion tube Distal end outer
diameter
Distal end enlarged 1. Air/water nozzle
Insertion tube outer
diameter
Working length 1680 mm 1330 mm
Range of the flexibility
adjustment
Instrument
channel
Channel inner
diameter
Minimum visible
distance
∗1
ø11.3mm
2. Light guide lens
3. Objective lens
4. Instrument channel
UP
3.
RIGHT LEFT
DOWN
ø11.3mm
The rigidity in the most-rigid condition is
about twice that in the most-flexible
condition.
ø3.2mm
5 mm from the distal end
1.
2.4.
44
Direction from which
endo-therapy
accessories enter and
exit the endoscopic
image
Air flow rate
Note: Standard when CLV-260 (high air
pressure) is used.
Bending section Angulation range
RIGHT 160°, LEFT 160°
Total length 2005 mm 1655 mm
NBI observation
∗2
UP 180
30 cm3/s
°, DOWN 180°,
Available
∗1 Normal value
∗2 For more details, refer to the instruction manual of the CV-260SL.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 49

Chapter 2 Instrument Nomenclature and Specifications
Medical
Device
Directive
EMC Applied standard;
IEC 60601-1-2: 2001
Year o f
manufacture
2612345
This device complies with the requirements
of Directive 93/42/EEC concerning medical
devices.
Classification: Class II a
This instrument complies with the standards
listed in the left column.
CISPR 11 of emission:
Group 1, Class A
(CF-Q260DL/I only)
Group 1, Class B
(except CF-Q260DL/I)
This instrument complies with the EMC
standard for medical electrical equipment;
edition 2 (IEC 60601-1-2: 2001). However,
when connecting to an instrument that
complies with the EMC standard for medical
electrical equipment; edition 1
(IEC 60601-1-2: 1993), the whole system
complies with edition 1.
The last digit of the year of manufacture is
the second digit of the serial number.
Degree of
protection
against
electric shock
TYPE BF applied part
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
45
Page 50

Chapter 2 Instrument Nomenclature and Specifications
2.4 Attaching the chain for water-resistant cap (MAJ-1119)
• Do not lift the endoscope by the chain for water-resistant cap.
Otherwise, operator and/or patient injury can result, or the
endoscope and/or water-resistant cap may be damaged
when the fitting part comes off the S-cord connector mount or
the chain connector of the GIF-N260 and GIF-XP260.
• Only connect the fitting to the S-cord connector mount or the
chain connector of the GIF-N260 and GIF-XP260.
Connecting the fitting to the suction connector may impair the
connection of the suction tube to the suction connector. It
may also cause the suction tube to become disconnected
from the endoscope and allow patient debris to spray.
• The chain for water-resistant cap and water-resistant cap
itself cannot be ultrasonically cleaned; doing so could
damage them. The water-resistant cap with the chain can
only be ultrasonically cleaned if connected to endoscopes
that are being cleaned in an endoscope reprocessor (such as
OER, OER-A) with an ultrasonic cleaning phase.
• When attaching the water-resistant cap to the electrical
connector, do not pinch the chain for water-resistant cap
between the electrical connector of the endoscope and the
water-resistant cap. Otherwise, equipment damage may
result.
• The chain for water-resistant cap and water-resistant cap
cannot be Ethylene oxide gas sterilized; doing so may
damage them. If the water-resistant cap is connected to the
endoscope by the chain, be sure to remove the chain and the
water-resistant cap from the endoscope before Ethylene
oxide gas sterilization.
• The chain for water-resistant cap and water-resistant cap
cannot be steam sterilized (autoclaved); doing so can
damage them severely.
46
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 51

Notch
Chapter 2 Instrument Nomenclature and Specifications
Chain part
Connecting plate
Figure 2.1
To ensure that you do not forget to attach the water-resistant
cap, it is recommended that you connect it to the
endoscope’s S-cord connector mount or the chain connector
of the GIF-N260 and GIF-XP260 using the chain for
water-resistant cap.
Fitting part
Hole
1. Confirm that the chain for water-resistant cap is free from cracks, flaws,
wear, deformation or other damages (see Figure 2.1).
2. Align the notch on the connecting plate with the pin on the venting connector
of water-resistant cap (MH-553, see Figure 2.2).
3. Place the connecting plate over the venting connector (see Figure 2.2).
4. Confirm that the connecting plate is securely attached to the foot of the
venting connector and can be smoothly rotated (see Figure 2.2).
5. Place the hole on the fitting part over the endoscope’s S-cord connector
mount or the chain connector of the GIF-N260 and GIF-XP260 (see Figure
2.3).
6. Confirm that the fitting part is securely attached to the foot of the S-cord
connector mount or the chain connector of GIF-N260 and GIF-XP260 and
can be smoothly rotated.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
47
Page 52

Chapter 2 Instrument Nomenclature and Specifications
Connecting plate
Venting connector
Water-resistant cap
Figure 2.2
Notch
Pin
Fitting part
Hole
S-cord connector
mount or chain
connector
Figure 2.3
The instructions on the remaining pages of this manual are
given under the assumption that the chain for water-resistant
cap is detached from the endoscope.
48
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 53

Chapter 3 Preparation and Inspection
Chapter 3 Preparation and Inspection
Before each case, prepare and inspect this instrument as instructed below.
Inspect other equipment to be used with this instrument as instructed in their
respective instruction manuals. If any irregularities are suspected after
inspection, follow the instructions as described in Chapter 5, “Troubleshooting”.
If this instrument malfunctions, do not use it. Return it to Olympus for repair as
described in Section 5.3, “Returning the endoscope for repair” on page 105.
• Using an endoscope that is not functioning properly may
compromise patient or operator safety and may result in
more severe equipment damage.
• This instrument was not cleaned, disinfected or sterilized
before shipment. Before using this instrument for the first
time, reprocess it according to the instructions as described
in the endoscope’s companion manual, the
“REPROCESSING MANUAL” whose cover lists the model of
your endoscope.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
49
Page 54

Chapter 3 Preparation and Inspection
3.1 Preparation of the equipment
Prepare the equipment shown in Figure 3.1 (for compatibility, see the “System
chart” in the Appendix) and personal protective equipment, such as eye wear,
face mask, moisture-resistant clothing and chemical-resistant gloves, before
each use. Refer to the respective instruction manuals for each piece of
equipment.
Monitor
Video system center
Water
container
UPD cable
(for CF-Q260DL/I
only)
Light source
Magnification controller cable
(for CF-H260AZL/I only)
Magnification controller
(for CF-H260AZL/I only)
Suction pump
Endoscope
Endoscope position
detecting unit
(for CF-Q260DL/I only)
50
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 55

Endo-therapy accessories
Chapter 3 Preparation and Inspection
Mouthpiece (for GIF models only)
Water pump (OFP) or a
syringe (for GIF-H260Z only)
• Paper towels • Trays • Lint-free cloths • Personal protective equipment
Auxiliary water tube (for GIF-H260Z only)
Figure 3.1
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
51
Page 56

Chapter 3 Preparation and Inspection
3.2 Inspection of the endoscope
Clean and disinfect or sterilize the endoscope as described in the
“REPROCESSING MANUAL” whose cover lists the model of your endoscope.
Then remove the water-resistant cap from the endoscope connector.
Inspection of the endoscope
1.
Inspect the control section and the endoscope connector for excessive scratching, deformation, loose parts or other irregularities.
2. Inspect the boot and the insertion tube near the boot for bends, twists or
other irregularities.
3. Inspect the external surface of the entire insertion tube including the
bending section and the distal end for dents, bulges, swelling, scratching,
holes, sagging, transformation, bends, adhesion of foreign bodies, dropout
of parts, any protruding objects or other irregularities.
4. Holding the insertion tube gently with one hand, carefully run your fingertips
over the entire length of the insertion tube in both directions (see Figure
3.2). Confirm that no objects or metallic wire protrude from the insertion
tube. Also confirm that the insertion tube is not abnormally rigid.
Figure 3.2
5. Using both hands, bend the insertion tube of the endoscope into a
semicircle. Then, moving your hands as shown by the arrows in Figure 3.3,
confirm that the entire insertion tube can be smoothly bent to form a
semicircle and that the insertion tube is pliable. When inspecting
endoscopes with flexibility adjustment, perform the test with the insertion
tube at both its most-flexible and most-rigid settings (for endoscopes with
flexibility adjustment only).
52
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 57

Chapter 3 Preparation and Inspection
Figure 3.3
6. Gently hold the midpoint of the bending section and a point 20 cm from the
distal end. Push and pull gently to confirm that the junction between the
bending section and the insertion tube is not loose.
7. Inspect the objective lens and light guide lens at the distal end of the
endoscope’s insertion tube for scratching, cracks, stains or other
irregularities.
8. Inspect the air/water nozzle at the distal end of the endoscope’s insertion
tube for abnormal swelling, bulges, dents or other irregularities.
Inspection of the flexibility adjustment mechanism (for endoscopes with flexibility adjustment only)
Confirm that the marks (“z”, “1”, “2”, “3”) on the flexibility adjustment ring
1.
and the “ ” mark at the bottom of the grip section are clearly visible (see
Figure 3.4).
Figure 3.4
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
53
Page 58

Chapter 3 Preparation and Inspection
2. Confirm that the flexibility adjustment ring can be turned smoothly when the
insertion tube is straight.
3. Set the insertion tube to the most-flexible and most-rigid conditions,
respectively. In each case, hold the marks of 30 and 50 cm of the insertion
tube with two hands, and bend it gently as shown in Figure 3.5. Confirm that
the actual flexibility changes according to the flexibility adjustment setting.
Do not use the endoscope if the marking are not clearly
visible. If the operator is uncertain of the flexibility of the
endoscope, insertion and manipulation of the endoscope
may cause patient pain and/or injury.
If the insertion tube is coiled into a too small diameter, the
flexibility adjustment ring may not operate smoothly. This
does not indicate a malfunction.
30 cm
50 cm
Figure 3.5
Inspection of the zoom lever (for GIF-H260Z and CF-H260AZL/I only)
Move the zoom lever slowly in each direction unit it stops. Confirm that it moves
smoothly and correctly.
54
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 59

Inspection of the bending mechanisms
Perform the following inspections while the bending section is straight.
• If the movement of the UP/DOWN angulation lock,
RIGHT/LEFT angulation lock and their angulation control
knobs are loose and/or not smooth, or the bending section
does not angulate smoothly, the bending mechanism may be
abnormal. In this case, do not use the endoscope because it
may be impossible to straighten the bending section during
an examination (except GIF-N260).
• If the movement of the UP/DOWN angulation lock and its
angulation control knob are loose and/or not smooth, or the
bending section does not angulate smoothly, the bending
mechanism may be abnormal. In this case, do not use the
endoscope because it may be impossible to straighten the
bending section during an examination (for GIF-N260 only).
Chapter 3 Preparation and Inspection
Inspection for smooth operation
1. Confirm that both the UP/DOWN and RIGHT/LEFT angulation locks move
all the way in the “F ” direction (the GIF-N260 has only the UP/DOWN
angulation lock).
2. Turn the UP/DOWN and RIGHT/LEFT angulation control knobs slowly in
each direction until they stop, and return them to their respective neutral
positions (the GIF-N260 has only the UP/DOWN angulation knob). Confirm
that the bending section angulates smoothly and correctly, that maximum
angulation can be achieved and that the bending section returns to its
respective neutral positions.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
55
Page 60

Chapter 3 Preparation and Inspection
3. When the UP/DOWN and RIGHT/LEFT angulation control knobs are turned
to their respective neutral positions as shown in Figure 3.6, confirm that the
bending section returns smoothly to an approximately straight condition
(except GIF-N260).
Figure 3.6
4. When the UP/DOWN angulation control knob is turned to its neutral position
as shown in Figure 3.7, confirm that the bending section returns smoothly to
an approximately straight condition (for GIF-N260 only).
Figure 3.7
56
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 61

Chapter 3 Preparation and Inspection
Inspection of the UP/DOWN angulation mechanism
1. Move the UP/DOWN angulation lock all the way in the opposite direction of
the “F ” mark. Then turn the UP/DOWN angulation control knob in the
“ U” or the “D ” direction until it stops.
2. Confirm that the angle of the bending section is roughly stabilized when the
UP/DOWN angulation control knob is released.
3. Confirm that the bending section straightens out when the UP/DOWN
angulation lock is moved all the way in the “F ” direction and the
UP/DOWN angulation control knob is released.
Inspection of the RIGHT/LEFT angulation mechanism
(except GIF-N260)
1. Turn the RIGHT/LEFT angulation lock all the way in the opposite direction of
the “F ” mark. Then turn the RIGHT/LEFT angulation control knob in the
“R ” or the “ L” direction until it stops.
2. Confirm that the angle of the bending section is roughly stabilized when the
RIGHT/LEFT angulation control knob is released.
3. Confirm that the bending section straightens out when the RIGHT/LEFT
angulation lock is turned in the “F ” direction and the RIGHT/LEFT
angulation control knob is released.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
57
Page 62

Chapter 3 Preparation and Inspection
3.3 Preparation and inspection of accessories
Clean and disinfect or sterilize the air/water valve, suction valve, biopsy valve
and auxiliary water tube as described in the endoscope’s companion
reprocessing manual, the “REPROCESSING MANUAL” whose cover lists the
model of your endoscope.
Inspection of the air/water and suction valves
Confirm that the top hole of the air/water valve is not blocked
(see Figure 3.8). If the hole is blocked, air is fed continuously
and patient pain, bleeding and/or perforation can result.
1. Confirm that the holes of the valves are not blocked (see Figures 3.8 and
3.9).
2. Confirm that the valves are not deformed or cracked (see Figures 3.8 and
3.9).
3. Check for excessive scratching or tears in the air/water valve’s seals (see
Figure 3.8).
Hole
Spring
Seals
Air/water valve (MH-438)
Figure 3.8
Skirt
Hole
58
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 63

Figure 3.9
Chapter 3 Preparation and Inspection
Spring
Skirt
Hole
Suction valve (MH-443)
The air/water and suction valves are consumables. If the
inspection of the air/water or suction valve reveals any
irregularities, use new valves.
Inspection of the biopsy valve
The biopsy valve is a consumable that should be inspected
before each use. Replace it with a new one if irregularities
are observed during the following inspection. An irregular,
abnormal or damaged valve can reduce the efficacy of the
endoscope’s suction system, and may leak or spray patient
debris or fluids, posing an infection-control risk.
1. Confirm that the slit and hole on the biopsy valve have no splits, cracks,
deformation, discoloration or other damage (see Figure 3.10).
Normal Abnormal
Slit
Hole
Cap
Main body
Discoloration
Splits, cracks
Figure 3.10
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
59
Page 64

Chapter 3 Preparation and Inspection
2. Attach the cap to the main body (see Figure 3.11).
Slit
Cap
Figure 3.11
Main body
Inspection of the auxiliary water inlet cap (for GIF-H260Z only)
1.
Confirm that the auxiliary water inlet cap attached to the endoscope
connector has no dents, cracks or other irregularities (see Figure 3.12).
2. If irregularities are observed, replace it with a new one as described in
“Attaching the auxiliary water inlet cap (for GIF-H260Z only)” on page 64.
Auxiliary water inlet
Endoscope connector
Auxiliary water inlet cap
60
Figure 3.12
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 65

Inspection of the auxiliary water tube (for GIF-H260Z only)
Inspect the auxiliary water tube for cracks, scratches, flaws and other damage
(see Figure 3.13).
Chapter 3 Preparation and Inspection
Clip
Figure 3.13
Luer port
Inspection of the mouthpiece (for GIF models only)
Do not use a mouthpiece that is damaged, deformed or
reveals other irregularities. Doing so may cause patient injury
and/or equipment damage.
Placing the mouthpiece in the patient’s mouth before the
procedure prevents the patient from biting and/or damaging
the endoscope’s insertion tube.
1. Confirm that the mouthpiece is free from cracks, deformation or
discoloration (see Figure 3.14).
Opening
Main body
Figure 3.14
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Outer flange
61
Page 66

Chapter 3 Preparation and Inspection
2. Using your fingers, check for excessive scratching or other irregularities on
all surfaces of the mouthpiece (see Figure 3.14).
3.4 Attaching accessories to the endoscope
The air/water valve and the suction valve do not require
lubrication. Lubricants can cause swelling of the valves’
seals, which will impair valve function.
Attaching the suction valve
1.
Align the two metal ridges on the underside of the suction valve with the two
holes in the suction cylinder.
2. Attach the suction valve to the suction cylinder of the endoscope (see Figure
3.15). Confirm that the valve fits properly without any bulging of the skirt.
Also confirm that the valve cannot be rotated.
Two metal ridges
Figure 3.15
Skirt
Side view
Bottom view Top view
The suction valve will make a whistling noise when it is dry;
this does not indicate a malfunction.
Suction cylinder
Suction cylinder
Two holes
62
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 67

Attaching the air/water valve
1.
Attach the air/water valve to the air/water cylinder of the endoscope (see
Figure 3.16).
2. Confirm that the valve fits properly without any bulging of the skirt.
Air/water valve
Air/water cylinder
Chapter 3 Preparation and Inspection
Suction valve
Skirt
Suction cylinder
Figure 3.16
The air/water valve may stick at first, but it should operate
smoothly after it is depressed a few times.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
63
Page 68

Chapter 3 Preparation and Inspection
Attaching the biopsy valve
Attach the biopsy valve to the instrument channel port of the endoscope (see
Figure 3.17). Confirm that the biopsy valve fits properly.
If a biopsy valve is not properly connected to the instrument
channel port, it can reduce the efficacy of the endoscope’s
suction system and may cause patient debris to leak or spray
from the endoscope.
Biopsy valve
Instrument
channel port
Figure 3.17
Attaching the auxiliary water inlet cap (for GIF-H260Z only)
If the auxiliary water inlet cap is not attached, attach the fitting ring to the
auxiliary water inlet on the endoscope connector (see Figure 3.18).
Fitting ring
Auxiliary water inlet
Endoscope connector
Figure 3.18
Auxiliary water inlet cap
64
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 69

Chapter 3 Preparation and Inspection
3.5 Inspection and connection of ancillary equipment
Inspection of ancillary equipment
• Attach the water container to the specified receptacle on the
trolley or the light source. If the water container is attached
anywhere else, water may drip from the water container’s
water supply tube, and equipment malfunction can result.
• Take care not to spill water from the water container’s
connection adapter when detaching the connection adapter
from the endoscope. Spilled water could splash on the
equipment, and it may cause equipment malfunction.
Prepare and inspect the light source, video system center, monitor, magnification
controller (for CF-H260AZL/I only), endoscope position detecting unit (for
CF-Q260DL/I only), water container, suction pump and endo-therapy
accessories as described in their respective instruction manuals.
The NBI observation is available when the EVIS LUCERA
video system center CV-260SL and the EVIS LUCERA
xenon light source CLV-260SL are used with the endoscope.
Connection of the endoscope and ancillary equipment
Firmly connect the suction tube from the suction pump to the
suction connector on the endoscope connector. If the suction
tube is not attached properly, debris may drip from the tube
and can present an infection-control risk, cause damage
and/or reduce suction capability.
When using the GIF-H260, GIF-H260Z, CF-H260AL/I and
CF-H260AZL/I, use the videoscope cable LUCERA
(MAJ-1154). These endoscopes are not compatible with the
videoscope cable 200 (MH-977).
1. If any ancillary equipment is ON, turn it OFF.
2. Insert the endoscope connector completely into the scope socket (output
socket when using the CLV-U20/U40) of the light source.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
65
Page 70

Chapter 3 Preparation and Inspection
3. Connect the water container’s connection adapter to the air supply
connector and water supply connector (see Figure 3.19).
4. Confirm that the water container’s connection adapter fits properly and that
it cannot be rotated.
(1) (2) (3) (4)
Water container’s connection adapter
Air supply connector
Water supply connector
Endoscope connector
5. Align the mark on the videoscope cable LUCERA or the videoscope cable
Mark 2 (gray)
Figure 3.19
200 with mark 1 on the endoscope connector and push it in until it stops
(see Figure 3.20).
Mark (gray)
Mark 1 (gray)
66
Figure 3.20
6. Turn the connector of the videoscope cable clockwise until it stops (see
Figure 3.20).
7. Confirm that the mark on the videoscope cable is aligned with mark 2 on the
endoscope connector.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 71

Chapter 3 Preparation and Inspection
8. Align the notch on the endoscope plug of the magnification control cable
with mark 3 on the zoom connector of the endoscope and push the
endoscope plug into the zoom connector until it stops (see Figure 3.21 for
CF-H260AZL/I only).
Mark 3
(protrusion)
Notch
Endoscope plug
Endoscope plug
Figure 3.21
If force is used on the magnification control cable, the
endoscope is designed to detach at the endoscope plug, not
at the endoscope connector (for CF-H260ZL/I only).
9. Align the notch on the endoscope plug of the UPD cable with mark 3 on the
UPD scope connector of the endoscope and push the endoscope plug into
the UPD scope connector until it stops (see Figure 3.22 for CF-Q260DL/I
only).
Mark 3
(protrusion)
Notch
Position detecting connector
Figure 3.22
If force is used on the UPD cable, the endoscope is designed
to detach at the endoscope plug, not at the endoscope
connector (for CF-Q260DL/I only).
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
67
Page 72

Chapter 3 Preparation and Inspection
10. Connect the suction tube from the suction pump to the suction connector on
the endoscope connector (see Figure 3.23).
Figure 3.23
11. Open the auxiliary water inlet cap (see Figure 3.24 for GIF-H260Z only).
Suction pump
Suction connector
Suction tube
12. Connect the auxiliary water tube to the auxiliary water inlet on the
endoscope connector and turn it clockwise until it stops (see Figure 3.24 for
GIF-H260Z only).
Auxiliary water tube
Auxiliary water inlet
Endoscope connector
Figure 3.24
Auxiliary water inlet cap
68
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 73

Chapter 3 Preparation and Inspection
3.6 Inspection of the endoscopic system
Inspection of the endoscopic image
Do not stare directly at the distal end of the endoscope while
the examination light is ON. Otherwise, eye injury may result.
1. Turn the video system center, light source, monitor, magnification controller
(for CF-H260AZL/I only) and endoscope position detecting unit (for
CF-Q260DL/I only) ON and inspect the WLI endoscopic image as described
in their respective instruction manuals.
2. Confirm that light is output from the endoscope’s distal end.
3. While observing the palm of your hand, confirm that the WLI endoscopic
image is free from noise, blur, fog or other irregularities.
4. Angulate the endoscope and confirm that the WLI endoscopic image does
not momentarily disappear or displays any other irregularities.
If the object cannot be seen clearly, wipe the objective lens
using a clean lint-free cloth moistened with 70% ethyl or
isopropyl alcohol.
Inspection of remote switch
All remote control switches should be checked to work
normally even when they are not expected for use. The
endoscopic image may freeze or other irregularities may
occur during examination and may cause patient injury,
bleeding and/or perforation.
Depress every remote control switch and confirm that the specified functions
work normally.
Inspection of the air feeding function
1.
Set the airflow regulator on the light source to “High”, as described in the
light source’s instruction manual.
2. Immerse the distal end of the insertion tube in sterile water to a depth of
10 cm and confirm that no air bubbles are emitted when the air/water valve
is not operated.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
69
Page 74

Chapter 3 Preparation and Inspection
3. Cover the hole in the air/water valve with your finger and confirm that air
bubbles are continuously emitted from the air/water nozzle.
4. Uncover the hole in the air/water valve and confirm that no air bubbles are
emitted from the air/water nozzle.
If a stream of air bubbles is emitted from the air/water nozzle
even though the air/water valve is not being operated and the
distal end of the insertion tube is 10 cm or more below the
surface of the sterile water, there may be an irregularity in the
air feeding function. If the endoscope is used while air is
continuously fed, over-insufflation and patient injury may
result. If air bubbles are emitted from the air/water nozzle,
remove and reattach the air/water valve correctly, or replace
it with a new one. If this fails to stop air bubbles from being
emitted, do not use the endoscope, as there may be a
malfunction. Contact Olympus.
When the distal end of the insertion tube is immersed less
than 10 cm below the surface of the sterile water, a small
amount of air bubbles may be emitted from the air/water
nozzle even when the air/water valve is not operated. This
does not indicate a malfunction.
Inspection of the objective lens cleaning function
Use sterile water only. Non sterile water may cause patient
cross-contamination and/or infection.
• When the air/water valve is depressed for the first time, it
may take a few seconds before water is emitted.
• If the air/water valve returns to its original position slowly after
water feeding, remove the air/water valve and moisten the
seals with sterile water.
• During the inspection, place the distal end of the endoscope
in a beaker or other container so that the floor does not get
wet.
70
1. Keep the air/water valve’s hole covered with your finger and depress the
valve. Observe the endoscopic image and confirm that water flows on the
entire objective lens.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 75

2. Release the air/water valve. Observe the endoscopic image and confirm
that the emission of water stops and that the valve returns smoothly to its
original position.
3. While observing the endoscopic image, feed air after feeding water by
covering the hole in the air/water valve with your finger. Confirm that the
emitted air removes the remaining water from the objective lens and clears
the endoscopic image.
Inspection of the suction function
• If the suction valve does not operate smoothly, detach it and
reattach it, or replace it with a new one. If the endoscope is
used while the suction valve is not working properly, it may
be impossible to stop suction, which could cause patient
injury. If the reattached or replaced suction valve fails to
operate smoothly, the endoscope may be malfunctioning;
stop using it and contact Olympus.
Chapter 3 Preparation and Inspection
• If the biopsy valve leaks, replace it with a new one. A leaking
biopsy valve can reduce the efficacy of the endoscope’s
suction system, and may leak or spray patient debris or
fluids, posing an infection-control risk.
1. Place the container of sterile water and the endoscope on the same height.
For the inspection, adjust the suction pressure to the same level as it will be
during the procedure.
2. Immerse the distal end of the insertion tube in sterile water with the
endoscope’s instrument channel port at the same height as the water level
in the water container. Press the suction valve and confirm that water is
continuously aspirated into the suction bottle of the suction pump.
3. Release the suction valve. Confirm that suction stops and the valve returns
to its original position.
4. Depress the suction valve and aspirate water for one second. Then, release
the suction valve for one second. Repeat this several times and confirm that
no water leaks from the biopsy valve.
5. Remove the distal end of the endoscope from the water. Depress the
suction valve and aspirate air for a few seconds to remove any water from
the instrument and suction channels.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
71
Page 76

Chapter 3 Preparation and Inspection
Inspection of the instrument channel
1. Insert the endo-therapy accessory through the biopsy valve. Confirm that
the endo-therapy accessory extends smoothly from the distal end. Also
make sure that no foreign objects come out of the distal end.
2. Confirm that the endo-therapy accessory is withdrawn smoothly from the
biopsy valve.
Inspection of the zoom function (for GIF-H260Z only)
1.
When using the video system center CV-260SL, select the “WLI observation mode” as indicated in the instruction manual of the video system center.
Keep your eyes away from the distal end when inserting
endo-therapy accessories. Extending the endo-therapy
accessory from the distal end could cause eye injury.
2. Move the zoom lever toward “ T” until it stops and confirm that the image
of an object located about 2 mm from the distal end is clearly visible.
3. Move the zoom lever toward “W ” until it stops and confirm that the image
of an object located at about 20 mm from the distal end is clearly visible.
4. While observing the palm of your hand, move the zoom lever toward “ T”
and confirm that the endoscopic image changes smoothly the wide-angle
image into the magnified image.
5. While observing the palm of your hand, turn the zoom lever toward “W ”
and confirm that the endoscopic image changes smoothly the magnified
image into the wide-angle image.
Inspection of the zoom function (for CF-H260AZL/I only)
1.
When using the video system center CV-260SL, select the “WLI observation
mode” as indicated in the instruction manual of the video system center.
2. If the magnification controller is OFF, turn it ON and set the speed mode as
described in its instruction manual.
3. Move the zoom lever toward “ T”. After about 3 seconds, confirm that the
image of an object located about 2 mm from the distal end is clearly visible.
72
4. Move the zoom lever toward “W ”. After about 3 seconds, confirm that the
image of an object located at about 20 mm from the distal end is clearly
visible.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 77

Chapter 3 Preparation and Inspection
5. While observing the palm of your hand, move the zoom lever toward “ T”
and confirm that the endoscopic image changes smoothly the wide-angle
image into the magnified image.
6. While observing the palm of your hand, move the zoom lever toward “W ”
and confirm that the endoscopic image changes smoothly the magnified
image into the wide-angle image.
• Immediately after turning the magnification controller ON, a
widest angle image will be observed.
• If the endoscope is stored at a lower temperature than room
temperature, the speed of the magnification control could be
slow. In this case, wait for a moment until the endoscope
reaches room temperature and check the magnification
control function again.
Inspection of the auxiliary water feeding function (for GIF-H260Z only)
• Use sterile water only. Non-sterile water may cause patient
cross-contamination and/or infection.
• Note that the luer port on the MAJ-855 includes a one-way
valve to prevent backflow – do not use the MAJ-855 without
the luer port in place, otherwise backflow of contaminated
material may occur and equipment damage or patient injury
may result.
1. Attach a syringe containing sterile water or the water tube from a water
pump to the luer port of the auxiliary water tube (see Figure 3.25). Feed
water and confirm that water is emitted from the auxiliary water channel at
the distal end of the insertion tube.
2. Make sure that no water leaks from the connection between the connecting
end of the auxiliary water tube and the auxiliary water inlet.
3. Make sure that no water leaks from the connection between the luer port of
the auxiliary water tube and the syringe or water tube.
4. Disconnect the water tube from the water pump or the syringe from the luer
port of the auxiliary water tube. Make sure that no water leaks at the luer
port of the auxiliary water tube and/or the distal end of the insertion tube.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
73
Page 78

Chapter 3 Preparation and Inspection
If the auxiliary water channel is used for feeding water, never
disconnect the auxiliary water tube during an examination;
leave it attached until the endoscope is precleaned. If the
auxiliary water tube is detached before precleaning, water
remaining in the auxiliary water channel may be spilled on
the surrounding equipment. This could cause damage to
and/or malfunction of the equipment.
Syringe or water tube
from a water pump
Luer port
Auxiliary water tube
Connecting end
Figure 3.25
Inspection of the endoscope position detecting function (for CF-Q260DL/I only)
If the endoscope position detecting unit is turned OFF, turn it ON. Inspect “scope
model” as described in the position detecting unit’s instruction manual.
The scope model may not be displayed depending on the
endoscope’s position. Operate the endoscope position
detecting unit as described in its instruction manual.
74
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 79

Chapter 4 Operation
The operator of this instrument must be a physician or medical personnel under
the supervision of a physician and must have received sufficient training in
clinical endoscopic technique. This manual, therefore, does not explain or
discuss clinical endoscopic procedures. It only describes basic operation and
precautions related to the operation of this instrument.
• Wear personal protective equipment to guard against
dangerous chemicals and potentially infectious material
during the procedure. Wear appropriate personal protective
equipment, such as eye wear, face mask, moisture-resistant
clothing and chemical-resistant gloves that fit properly and
are long enough so that your skin is not exposed.
Chapter 4 Operation
• The temperature of the distal end of the endoscope may
exceed 41°C and reach 50°C due to intense endoscopic
illumination. Surface temperatures over 41°C may cause
mucosal burns. Always use the minimum level of illumination,
minimum time and suitable distance necessary for adequate
viewing. Whenever possible, avoid close stationary viewing
and do not leave the distal end of the endoscope close to the
mucous membrane for a long time.
• Whenever possible, do not leave the endoscope illuminated
before and/or after an examination. Continued illumination
will cause the distal end of the endoscope to become hot and
could cause operator and/or patient burns.
• Turn the video system center ON to operate a light source’s
automatic brightness function. When the video system center
is OFF, it cannot operate the light source’s automatic
brightness function, and the light intensity is set to the
maximum level. In this case, the distal end of the endoscope
can become hot and could cause operator and/or patient
burns (when using the light source other than CLV-260SL,
CLV-260).
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
75
Page 80

Chapter 4 Operation
• Never insert or withdraw the endoscope under any of the
following conditions. Otherwise, patient injury, bleeding
and/or perforation can result.
− While the endo-therapy accessory extends from the distal
end of the endoscope.
− While the bending section is locked in position.
− Insertion or withdrawal with excessive force, or forcible
insertion or withdrawal.
− While the image is magnified (when using the GIF-H260Z,
CF-H260AZL/I or using the image magnification function
of video system center CV-260SL, CV-260).
• Transnasal insertion is accompanied by the risk of
inflammation of the nasal cavity. If this happens, the nasal
passage will be constricted, making it more difficult to
withdraw the endoscope. In this case, do not use force to
withdraw the endoscope because patient injury such as
bleeding or perforation may result.
• Transnasal insertion is accompanied by the risk of bleeding
in the nasal cavity. Be sure to be prepared to deal with any
bleeding. When withdrawing the endoscope, observe the
inside of the nasal cavity to ensure that there is no bleeding.
Even when the endoscope has been withdrawn without
bleeding, do not allow the patient to blow his or her nose
strongly because this could cause it to start bleeding.
• Before transnasal insertion, apply the appropriate
pretreatment and lubrication to the patient to enlarge the
nasal cavity. Otherwise, operator and/or patient injury can
result or the endoscope could become lodged and be difficult
to withdraw. When applying a pretreatment agent through a
tube, insert the tube into the same path as the path planned
for the endoscope insertion. Otherwise, the treatment will
have no effect. The effects of the pretreatment agent and
lubricant will decrease the longer the procedure lasts. Apply
the pretreatment agent or lubricant as required during the
procedure
difficult.
– for example, when withdrawal seems to be
76
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 81

Chapter 4 Operation
• The bending section will never bend to the RIGHT or LEFT
direction but to the UP or DOWN direction. To insert or
withdraw, operate the endoscope by considering the direction
in which the bending section is angulated. Never apply
excessive force to the RIGHT or LEFT direction when
inserting or withdrawing the endoscope. Patient injury,
bleeding and/or perforation can result (for GIF-N260 only).
• If any of the following phenomena occurs during an
examination, immediately stop the examination and withdraw
the endoscope from the patient as described in Section 5.2,
“Withdrawal of the endoscope with an abnormality” on
page 102.
− If any abnormality is suspected with the functionality of
the endoscope.
− If the endoscopic image on the monitor disappears or
freezes unexpectedly.
− If the angulation control knob is locked.
− If the angulation control mechanism is not functioning
properly.
− If the zoom malfunctions (when using the GIF-H260Z,
CF-H260AZL/I or using the image magnification function
of video system center CV-260SL, CV-260).
− If the flexibility adjustment ring becomes jammed (for
endoscopes with flexibility adjustment only).
Continued use of the endoscope under these conditions
could result in patient injury, bleeding and/or perforation.
• If an abnormal endoscopic image or function is observed, but
quickly corrects itself, the endoscope may have
malfunctioned. Continuous use of such an endoscope may
cause the abnormality to occur again, at which time it may
not return to the normal condition. In this case, stop the
examination immediately and slowly withdraw the endoscope
while viewing the endoscopic image. Otherwise, patient
injury, bleeding and/or perforation can result.
• Never perform flexibility adjustment while the endo-therapy
accessory extends from the distal end of the endoscope.
Patient injury, bleeding and/or perforation can result (for
endoscopes with flexibility adjustment only).
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
77
Page 82

Chapter 4 Operation
• Regardless of the flexibility of the endoscope’s insertion tube,
it can cause patient injury, bleeding and/or perforation if it is
forcibly inserted, withdrawn and/or twisted with excessive
force. It is generally believed that an endoscope with a
more-rigid insertion tube is easier to manipulate in the
intestines if used properly. However, it should be noted that
such an endoscope, if used improperly, is more likely to
cause patient pain, injury, bleeding and/or perforation than an
endoscope with a more flexible insertion tube (for
endoscopes with flexibility adjustment only).
• The flexibility of the insertion tube of the CF-Q260AL/I can be
adjusted to less than, equal to or more than that of the
CF-240L/I. The range of the flexibility adjustment of the
CF-Q260AL/I is equal to that of the CF-240AL/I.
The flexibility of the insertion tube of the CF-Q260DL/I can be
adjusted to less than, equal to or more than that of the
CF-240L/I and CF-Q240L/I. The range of the flexibility
adjustment of the CF-Q260DL/I is equal to that of the
CF-240DL/I.
The flexibility of the insertion tube of the CF-H260AL/I and
CF-H260AZL/I can be adjusted to less than, equal to or more
than that of the CF-Q240L/I and CF-Q240ZL/I. The range of
the flexibility adjustment of the CF-H260AL/I and
CF-H260AZL/I is equal to the CF-Q240AL/I.
The flexibility of the insertion tube of the PCF-Q260AL/I can
be adjusted to less than, equal to or more than that of the
PCF-240L/I.
The insertion tube of the endoscope should be adjusted to
the appropriate flexibility for each case. Always confirm the
flexibility of the insertion tube by holding the insertion tube
with two hands before inserting it into the patient, and adjust
the flexibility as necessary according to the case, region and
patient’s condition during an examination. If you are unsure
of the appropriate flexibility of the insertion tube, set it to the
most-flexible condition. Continuing the examination while the
insertion tube is set to an inappropriate degree of flexibility
may cause patient pain, injury, bleeding and/or perforation
(for endoscopes with flexibility adjustment only).
78
• The endoscopic image may be disturbed while switching
observation modes. Therefore, do not perform an endoscopic
operation or treatment while switching the observation mode.
Otherwise, injury in the body cavity may result.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 83

Chapter 4 Operation
• Set the brightness of the light source to the minimum level
necessary to perform the procedure safely. If the endoscope
is used for a prolonged period at or near maximum light
intensity, vapor may be observed in the endoscopic image.
This is caused by the evaporation of organic material (blood,
moisture in stool, etc.) due to heat generated by the light
guide near the light guide lens. If this vapor continues to
interfere with the examination, remove the endoscope, wipe
the distal end with a lint-free cloth moistened with 70% ethyl
or isopropyl alcohol, reinsert the endoscope and continue the
examination.
• The color tone and brightness of the NBI observation is
different from the WLI observation. Use the NBI observation
only when fully understanding the feature.
4.1 Insertion
Holding and manipulating the endoscope
The control section of the endoscope is designed to be held in the left hand. The
air/water and suction valves can be operated using the left index finger. The
UP/DOWN angulation control knob and the zoom lever can be operated using
the left thumb. The right hand is free to manipulate the insertion tube and the
RIGHT/LEFT angulation control knob (see Figure 4.1, the GIF-N260 has only the
UP/DOWN angulation control knob).
Figure 4.1
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
79
Page 84

Chapter 4 Operation
Insertion of the endoscope
• The distal end and insertion tube diameter of the GIF-XP260
is smaller than for other GIF models, but this does not mean
that its design assumes an insertion method other than
transoral insertion. Do not attempt transnasal insertion, as
this may cause injury, bleeding or perforation inside the nasal
cavity.
• The shape and size of the nasal cavity and its suitability for
transnasal insertion may vary from patient to patient. No
endoscope, including this one, can always be inserted
transnasally with all patients. Before proceeding, always be
sure to confirm that transnasal insertion is possible with the
patient by always considering both the size of the patient’s
nasal cavity as well as the size of the endoscope’s insertion
tube. Otherwise, operator and/or patient injury can result, or
the endoscope could become lodged and be difficult to
withdraw.
• Transnasal insertion of the endoscope should be performed
carefully. If resistance to insertion is felt, or the patient reports
pain, stop insertion immediately. Otherwise, operator and/or
patient injury can result or the endoscope could become
lodged and be difficult to withdraw.
• To prevent the patient from accidentally biting the insertion
tube during an examination, it is strongly recommended that
a mouthpiece be placed in the patient’s mouth before
inserting the endoscope (for GIF models only).
• To prevent the patient from accidentally loosing dental
prosthesis, make sure that patient removes them before the
examination (for GIF models only).
• Do not apply olive oil or products containing petroleum-based
lubricants (e.g. vaseline). These products may cause
stretching and deterioration of the bending section’s
covering.
• Do not allow the insertion tube to be bent within a distance of
10 cm or less from the junction of the boot. Insertion tube
damage can occur (see Figures 4.2 and 4.3).
80
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 85

> 10 cm
Figure 4.2
Endoscopes with flexibility adjustment
Chapter 4 Operation
> 10 cm
Figure 4.3
For GIF models
1. Move the zoom lever toward “W ” until it stops so that the widest possible
angle is shown in the endoscopic image (for GIF-H260Z only).
2. If necessary, apply a medical-grade, water-soluble lubricant to the insertion
tube.
3. Place the mouthpiece between the patient’s teeth or gums, with the outer
flange on the outside of the patient’s mouth.
In case of transnasal insertion (for GIF-N260 only), the mouthpiece is not
used.
4. Insert the distal end of the endoscope through the opening of the
mouthpiece, then from the mouth to the pharynx, while viewing the
endoscopic image. Do not insert the insertion tube into the mouth beyond
the insertion tube limit mark.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
81
Page 86

Chapter 4 Operation
For CF/PCF models
To determine the correct splinting tube to be used with the
endoscope, select one of the combinations shown in the
“System chart” in the Appendix.
1. Move the zoom lever toward “W ” until it stops so that the widest possible
angle is shown in the endoscopic image (for CF-H260AZL/I only).
2. If necessary, apply a medical-grade, water-soluble lubricant to the insertion
tube.
3. Insert the insertion tube of the endoscope into the splinting tube if required,
and apply lubricant to the splinting tube.
4. Always view the endoscopic image when passing the distal end of the
endoscope from the anus to the rectum. Do not insert the insertion tube into
the anus beyond the insertion tube limit mark.
Angulation of the distal end
Avoid forcible or excessive angulation, as this imposes load
on the wire controlling the bending section. This may cause
stretching or tearing of the wire, which could impair the
movement of the bending section.
1. Operate the angulation control knobs as necessary to guide the distal end
for insertion and observation (the GIF-N260 has only the UP/DOWN
angulation control knob).
2. The endoscope’s angulation locks are used to hold the angulated distal end
in position (the GIF-N260 has only the UP/DOWN angulation lock).
• When passing an endo-therapy accessory through the
instrument channel while the angulation is locked, the angle
of the distal end may change. When it is necessary to keep
the angulation stationary, hold the angulation control knobs in
place with your hand (the GIF-N260 has only the UP/DOWN
angulation control knob).
82
• When operating the UP/DOWN or RIGHT/LEFT angulation
lock, hold the angulation control knob stationary with your
finger. If this is not done, the angulation will change (the
GIF-N260 has only the UP/DOWN angulation control knob).
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 87

Chapter 4 Operation
Flexibility adjustment (for endoscopes with flexibility adjustment only)
• Do not change the insertion tube’s flexibility abruptly.
Otherwise, patient pain, injury, bleeding and/or perforation
can result.
• If the endoscopic image moves suddenly or is lost, while you
are changing the insertion tube’s flexibility, stop changing the
flexibility and restore the optimum field of view. Moving the
flexibility adjustment ring without a clear endoscopic image
may cause patient pain, injury, bleeding and/or perforation.
• If the patient complains of pain, while you are changing the
insertion tube’s flexibility, stop changing the flexibility and
ensure the safety of the patient.
• If the rigidity of the insertion tube has to be increased during
an examination, confirm that there are no loops or excessive
bends in the insertion tube (using fluoroscopy or endoscope
position detecting unit for CF-Q260DL/I, if necessary) before
increasing its rigidity. If the force required to turn the flexibility
adjustment ring is greater during the procedure than it was
when inspecting the endoscope, it may mean that the
insertion tube is excessively bent inside the patient. In this
case, straighten the insertion tube as much as possible
before attempting to increase the rigidity. Failure to do so
may cause patient pain, injury, bleeding and/or perforation.
1. Before inserting or withdrawing the endoscope, set the insertion tube to an
appropriate level of flexibility by turning the flexibility adjustment ring as
required (see Figure 4.4).
Rigid Flexible
Figure 4.4
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
83
Page 88

Chapter 4 Operation
Air/water feeding and suction
2. When changing the insertion tube’s flexibility during a procedure, turn the
flexibility adjustment ring slowly, and closely monitor the position of the
flexibility index marking, the endoscopic image and the patient’s condition.
Whenever the endoscope is not in use, set the insertion tube
to its most-flexible condition. Otherwise, endoscope damage
may result.
• If the sterile water level in the water container is too low, then
air, not water, will be supplied. In this case, turn the airflow
regulator on the light source OFF and add sterile water to the
water container until it reaches the specified water level.
• If air/water feeding does not stop, turn the airflow regulator
on the light source OFF and replace the air/water valve with a
new one.
• Before using a syringe to inject liquid through the biopsy
valve, detach the valve’s cap from the main body. Then insert
the syringe straight into the valve and inject the liquid. If the
cap is not detached and/or the syringe is not inserted
straight, the biopsy valve could be damaged, which could
reduce the efficacy of the endoscope’s suction system, and
may leak or spray patient debris or fluids, posing an
infection-control risk.
• If the biopsy valve is left uncapped during the procedure,
debris or fluids could leak or spray from it, posing an
infection-control risk. When the valve is uncapped, place a
piece of sterile gauze over it to prevent leakage.
• If the endoscope is cold, dew condensation may form on the
surface of the objective lens, and the endoscopic image may
appear cloudy. In this case, increase the temperature of the
sterile water in the water container to between 40 – 50°C
(104 – 122°F) and then use the endoscope.
84
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 89

Air/water feeding
1.
Cover the air/water valve’s hole to feed air from the air/water nozzle at the
distal end (see Figure 4.5).
2. Depress the air/water valve to feed water onto the objective lens (see Figure
4.5).
Chapter 4 Operation
Suction valve
Air/water valve
Figure 4.5
Suction
• Avoid aspirating solid matter or thick fluids; instrument
channel, suction channel or suction valve clogging can occur.
If the suction valve clogs and suction cannot be stopped,
disconnect the suction tube from the suction connector on
the endoscope connector. Turn the suction pump OFF,
detach the suction valve and remove solid matter or thick
fluids.
• When aspirating, maintain the suction pressure at the lowest
level necessary to perform the procedure. Excessive suction
pressure could cause aspiration of and/or injury to the
mucous membrane. In addition, patient fluids could leak or
spray from the biopsy valve, posing an infection-control risk.
• When aspirating, attach the cap to the main body of the
biopsy valve. The uncapped biopsy valve can reduce the
efficacy of the endoscope’s suction system, and may leak or
spray patient debris or fluids, posing an infection-control risk.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
85
Page 90

Chapter 4 Operation
During the procedure, take notice that the suction bottle does
not fill completely. Aspirating fluids into a full bottle may
cause the suction pump to malfunction.
Depress the suction valve to aspirate excess fluid or other debris obscuring the
endoscopic image (see Figure 4.5).
Performing both air feeding and suction at the same time
sometimes makes it easier to remove water droplets from the
objective lens surface.
Auxiliary water feeding (for GIF-H260Z only)
Use sterile water only. Non-sterile water may cause patient
infection.
• If the auxiliary water channel is used for feeding water, never
disconnect the auxiliary water tube from the auxiliary water
inlet during an examination; leave it attached until the
endoscope is precleaned. If the auxiliary water tube is
detached before precleaning, water remaining in the auxiliary
water channel may be spilled on the surrounding equipment.
This could cause damage and/or malfunction of the
equipment.
• When the auxiliary water tube is not connected to the
auxiliary water inlet, be sure to have the auxiliary water inlet
cap attached to the auxiliary water inlet. Otherwise, patient
debris or fluids that back flowed may drip out of the auxiliary
water inlet.
1. Attach a syringe containing sterile water or the water tube from a water
pump to the luer port of the auxiliary water tube. Feed water.
2. When disconnecting the syringe or the water tube from the water pump
during examination, disconnect it directly from the luer port but leave the
auxiliary water tube itself attached.
86
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 91

Chapter 4 Operation
Observation of the endoscopic image
Do not rely only on the NBI observation modality for primary
detection of lesions or to make a decision regarding any
potential diagnostic or therapeutic intervention.
Refer to the light source’s instruction manual for instructions on how to adjust the
brightness.
Operating the zoom function (for GIF-H260Z, CF-H260AZL/I only)
1.
Refer to the magnification controller’s instruction manual for the operation of
the magnification controller (for CF-H260AZL/I only).
2. Before insertion or withdrawal of the endoscope, move the zoom lever
toward “W ” so that the widest possible angle is shown in the endoscopic
image.
3. When magnifying the endoscopic image, move the zoom lever toward “ T”
and move the distal end of the endoscope closer to the object you wish to
observe.
• While the endoscopic image is magnified, objects at a
distance from the distal end of the endoscope may be out of
focus. This is not a malfunction; move the distal end closer to
the object you wish to observe.
• The CV-260SL and CV-260 indicates “the scale display” on a
monitor. Refer to the instruction manual of the CV-260SL and
CV-260 for details of the “the scale display” function.
Operating the endoscope position detecting function (for CF-Q260DL/I only)
Refer to the endoscope position detecting unit’s instruction manual for
instructions on how to operate the endoscope position detecting unit.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
87
Page 92

Chapter 4 Operation
4.2 Using endo-therapy accessories
For more information on combining the endoscope with particular endo-therapy
accessories, refer to the “System chart” in the Appendix and the instruction
manuals of the accessories. Refer to the accessories instruction manuals for
operating instructions.
• Do not use the GIF-N260 and GIF-XP260 for high-frequency
cauterization or laser cauterization treatment. Otherwise,
patient injury or equipment damage may result.
• When using endo-therapy accessories, keep the distance
between the distal end of the endoscope and the mucous
membrane greater than the endoscope’s minimum visible
distance so that the endo-therapy accessory remains visible
in the endoscopic image. If the distal end of the endoscope is
placed closer than its own minimum visible distance, the
position of the accessory cannot be seen in the endoscopic
image, which could cause serious patient injury and/or
equipment damage. The minimum visible distance depends
on the type of endoscope being used. Refer to Section 2.3,
“Specifications” on page 33.
• When inserting or withdrawing an endo-therapy accessory,
confirm that its distal end is closed or completely retracted
into the sheath. Slowly insert or withdraw the endo-therapy
accessory straight into/from the slit of the biopsy valve.
Otherwise, the biopsy valve may be damaged and pieces of it
could fall off.
• If the insertion or withdrawal of endo-therapy accessories is
difficult, straighten the bending section as much as possible
without losing the endoscopic image. Inserting or
withdrawing endo-therapy accessories with excessive force
may damage the instrument channel or endo-therapy
accessories cause some parts to fall off and/or cause patient
injury.
• If the distal end of an endo-therapy accessory is not visible in
the endoscopic image, do not open the distal end or extend
the needle of the instrument. This could cause patient injury,
bleeding, perforation and/or equipment damage.
88
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 93

Chapter 4 Operation
• When using endo-therapy accessories, always use the
widest possible angle. When the image is magnified, it may
not be possible to see the position of the accessory in the
endoscopic image. This could cause patient injury, bleeding
and/or perforation (when using the GIF-H260Z,
CF-H260AZL/I or using the image magnification function of
video system center CV-260SL, CV-260).
• When using a distal attachment, the distal end of the
endoscope becomes longer and its outer diameter is larger.
Handle the endoscope carefully so as not to cause
perforation or other patient injury. When performing the
endoscopic treatment using this equipment, take extra care.
• When a distal attachment is mounted on the endoscope, do
not angulate the endoscope abruptly. This could cause
patient injury, such as mucous membrane damage.
• Do not inflate air or a non-flammable gas excessively into the
patient. This could cause gas embolism.
• Do not switch the observation mode while using an
endo-therapy accessory. Otherwise, injury, burns, bleeding or
perforation in the body cavity may result.
• When using a biopsy forceps with a needle, confirm that the
needle is not bent excessively. A bent needle could protrude
from the closed cups of the biopsy forceps. Using such a
biopsy forceps could damage the instrument channel and/or
cause patient injury.
• When using an injector, be sure not to extend or retract the
needle from the catheter of the injector until the injector is
extended from the distal end of the endoscope. The needle
could damage the instrument channel if extended inside the
channel, or if the injector is inserted or withdrawn while the
needle is extended.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
89
Page 94

Chapter 4 Operation
Insertion of endo-therapy accessories into the endoscope
• Do not insert endo-therapy accessories forcibly or abruptly.
Otherwise, the endo-therapy accessory may extend from the
distal end of the endoscope abruptly, which could cause
patient injury, bleeding and/or perforation.
• It is easier to insert an endo-therapy accessory into the
instrument channel port if the biopsy valve’s cap is detached
from the main body (see Figure 3.11 on page 60). As a result,
the open biopsy valve can reduce the efficacy of the
endoscope’s suction system, and may leak or spray patient
debris or fluids, posing an infection-control risk. When not
using an endo-therapy accessory, attach the cap to the main
body of the biopsy valve.
• When the biopsy valve’s cap is detached from the main body,
it may cause patient debris or fluids to leak or spray from the
endoscope, posing an infection-control risk. When the biopsy
valve’s cap has to be detached, place a piece of sterile gauze
over it to prevent leakage.
• Do not let the endo-therapy accessory “hang down” from the
biopsy valve. Doing so can create a space between the
accessory and the valve’s slit or hole and/or damage the
valve, which can reduce the efficacy of the endoscope’s
suction system, and may leak or spray patient debris or
fluids, posing an infection-control risk.
• When inserting an endo-therapy accessory, hold it close to
the biopsy valve and insert it slowly and straight into the
biopsy valve. Otherwise, the endo-therapy accessory and/or
biopsy valve could be damaged. This can reduce the efficacy
of the endoscope’s suction system, and may leak or spray
patient debris or fluids, posing an infection-control risk.
1. Select endo-therapy accessories compatible with the instrument from the
“System chart” in the Appendix. Refer to the accessories instruction
manuals for operating instructions.
2. Hold the UP/DOWN and RIGHT/LEFT angulation knobs stationary (the
GIF-N260 has only the UP/DOWN angulation knob).
3. Confirm that the tip of the endo-therapy accessory is closed or retracted into
its sheath and insert the endo-therapy accessory slowly and straight into the
slit of the biopsy valve.
90
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 95

Chapter 4 Operation
• Do not open the tip of the endo-therapy accessory or extend
the tip of the endo-therapy accessory from its sheath while
the accessory is in the instrument channel. The instrument
channel and/or the endo-therapy accessory may become
damaged.
• Hold the endo-therapy accessory close to the biopsy valve
and insert it straight into the biopsy valve using slow, short
strokes. Otherwise, the endo-therapy accessory could bend
or break.
4. Hold the endo-therapy accessory approximately 4 cm from the biopsy valve
and advance it slowly and straight it into the biopsy valve using short strokes
while observing the endoscopic image.
• When the tip of the endo-therapy accessory extends
approximately 1 cm from the distal end of the endoscope, the
accessory will appear in the endoscopic image.
• When the accessory appears in the endoscopic image, it
may also reflect the light from the endoscope and/or cast its
shadow in the endoscopic image. This does not indicate a
malfunction (for GIF-N260 and GIF-XP260 only).
Operation of endo-therapy accessories
Operate the endo-therapy accessory according to the directions given in its
instruction manual.
Withdrawal of endo-therapy accessories
• Patient debris might spray when the endo-therapy
accessories are withdrawn from the biopsy valve. To prevent
this, hold a piece of gauze around the accessory and the
biopsy valve during withdrawal.
• Do not withdraw the endo-therapy accessory if the tip is open
or extended from its sheath; patient injury, bleeding,
perforation and/or instrument damage may occur.
• Withdraw the endo-therapy accessory slowly and straight out
of the biopsy valve. Otherwise, the valve’s slit and/or hole
could be damaged. This can reduce the efficacy of the
endoscope’s suction system, and may leak or spray patient
debris or fluids, posing an infection-control risk.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
91
Page 96

Chapter 4 Operation
Use of non-flammable gases (for CF/PCF models only)
• If the endo-therapy accessory cannot be withdrawn from the
endoscope, close the endo-therapy accessory and/or retract
it into its sheath, then carefully withdraw both the endoscope
and the endo-therapy accessory together under endoscopic
observation. Take care not to cause tissue trauma.
Withdraw the endo-therapy accessory slowly while the tip of the endo-therapy
accessory is closed and/or retracted into its sheath.
Performing treatment while the intestines is filled with a
flammable gas could result in an explosion, fire and/or
serious patient injury. If the intestines contains a flammable
gas, replace it with air or a non-flammable gas such as CO
before performing high-frequency treatment or laser
cauterization treatment.
2
Using CO2 during endoscopic examinations of the colon and
rectum, etc. may reduce post-examination pain.
When a non-flammable gas is used, only water containers MH-970 or MAJ-902
may be used with the endoscope. Carefully follow their instruction manuals.
High-frequency cauterization treatment (except GIF-N260 and GIF-XP260)
• If the intestines contains a flammable gas, replace it with air
or a non-flammable gas such as CO
high-frequency cauterization treatment. Otherwise, fire or
explosion could result.
• Not all parts of the endoscope are electrically insulated.
When applying high-frequency current, there is a danger of
unintentional diathermy burns. Always wear electrically
insulating chemical-resistant gloves.
before performing
2
92
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 97

Chapter 4 Operation
• Never emit high-frequency current before confirming that the
distal end of the high-frequency endo-therapy accessory is in
the endoscope’s field of view. Also confirm that the electrode
section and the mucous membrane in the vicinity of the target
area are at an appropriate distance from the distal end of the
endoscope. If the high-frequency current is emitted while the
distal end of the endo-therapy accessory is not visible or too
close to the distal end of the endoscope, patient injury,
bleeding and/or perforation as well as equipment damage
can result.
Prepare, inspect and connect the electrosurgical unit and electrosurgical
accessories as described in their instruction manuals.
The application of high-frequency current may interfere with
the endoscopic image. This does not indicate a malfunction.
Laser cauterization treatment (except GIF-N260 and GIF-XP260)
• Performing treatment while the intestines is filled with a
flammable gas could result in an explosion, fire and/or
serious patient injury. If the intestines contains a flammable
gas, replace it with air or a non-flammable gas such as CO
before performing laser cauterization treatment.
• To avoid patient injury, burns, bleeding and/or perforation as
well as damage to the endoscope, do not activate laser
radiation before confirming that the tip of the laser probe
appears in the proper position in the endoscopic image. Keep
an appropriate distance between the target and the
endoscope’s distal end and always use the lowest power
output possible.
• Before inserting or withdrawing the laser probe, return the
UP/DOWN and RIGHT/LEFT angulation control knobs to
their neutral positions (see Figure 3.6 on page 56) so that the
bending section will be straight. If it is bent, the instrument
channel and/or the laser probe may be damaged.
2
• Allow the tip of the laser probe to cool down before pulling it
back into the instrument channel. If the laser probe is
withdrawn while hot, channel damage may occur.
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
93
Page 98

Chapter 4 Operation
• Do not use a damaged laser probe. A laser probe with a
damaged sheath or distal end may cause patient injury
and/or equipment damage.
Prepare, inspect and connect the laser unit and laser probe as described in their
instruction manuals.
4.3 Withdrawal of the endoscope
• If blood unexpectedly adheres to the surface of the insertion
tube of the withdrawn endoscope, carefully check the
condition of the patient.
• If it becomes impossible to withdraw the transnasally inserted
endoscope, pull its distal end out of the mouth, cut the
flexible tube using wire cutters, and after ensuring that the cut
section will not injure the body cavity or nasal cavity of the
patient, withdraw the endoscope carefully. Therefore, always
prepare wire cutters in advance.
1. Move the zoom lever toward “W ” so that the widest possible angle is
shown in the endoscopic image (for GIF-H260Z and CF-H260AZL/I only).
2. When using the image magnification function of video system center
CV-260SL, CV-260, release the function.
3. Aspirate accumulated air, blood, mucus or other debris by depressing the
suction valve.
4. Turn the UP/DOWN and RIGHT/LEFT angulation locks to the “F ”
direction to release them (the GIF-N260 has only the UP/DOWN angulation
lock).
5. Carefully withdraw the endoscope while observing the endoscopic image.
When the splinting tube is used, withdraw both the endoscope and the
splinting tube together from the patient’s anus (for CF/PCF models only).
6. Carefully withdraw the endoscope while observing the endoscopic image.
Remove the mouthpiece from the patient’s mouth (for GIF models only).
94
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
Page 99

4.4 Transportation of the endoscope
Transporting within the hospital
1.
Set the insertion tube to the softest condition (for endoscopes with flexibility adjustment only).
2. When carrying the endoscope with the auxiliary water tube connected to the
auxiliary water inlet, attach the clip of the auxiliary water tube to the
universal cord (see Figure 4.6 for GIF-H260Z only).
Chapter 4 Operation
Clip
Figure 4.6
3. When carrying the endoscope by hand, loop the universal cord, hold the
endoscope connector with the control section in one hand and hold the
distal end of the insertion tube securely, but gently without squeezing, in the
other hand (see Figure 4.7).
Figure 4.7
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
95
Page 100

Chapter 4 Operation
Transporting outside the hospital
Transport the endoscope in the carrying case.
Always clean, disinfect or sterilize the endoscope after
removing it from the carrying case. If the endoscope is not
cleaned, disinfected or sterilized, it could pose an
infection-control risk.
• The carrying case cannot be cleaned, disinfected or
sterilized. Clean and disinfect or sterilize the endoscope
before placing it in the carrying case.
• Do not attach the water-resistant cap when transporting the
endoscope, to avoid damage to the endoscope caused by
changes in air pressure.
• Before putting the endoscope in the carrying case, always
make sure that the insertion tube is set to the most-flexible
condition. Putting the endoscope in the carrying case while
the insertion tube is rigid could damage the endoscope (for
endoscopes with flexibility adjustment only).
96
EVIS LUCERA GIF/CF/PCF TYPE 260 Series OPERATION MANUAL
 Loading...
Loading...