

Ulco Medical EV500 User Manual
EV500 ANAESTHETIC VENTILATOR
EV500 ANAESTHETIC VENTILATOREV500 ANAESTHETIC VENTILATOR
EV500 ANAESTHETIC VENTILATOR
USER
USER MANUAL
USERUSER
MANUAL
MANUAL MANUAL

EV500 User Manual
This page intentionally left blank
2
EV500 User Manual
Copyright © 1993, 2005, 2006 by Ulco Medical
All rights reserved.
No part of this publication may be reproduced in any form, in an electronic retrieval system
or otherwise, without the written permission of the Ulco Medical.
All Ulco products are subject to a program of continuous development and the
manufacturer reserves the right to make alterations in design and equipment without prior
notice.
Document Number: EV5-UM-001
Version: 2.5
3

EV500 User Manual
This page intentionally left blank
4

EV500 User Manual
Table of Contents
Table of Contents
Table of ContentsTable of Contents
1
Introduction ....................................................................................... 9
1.1 About this manual ..........................................................................................9
1.2 Intended Use ................................................................................................. 9
1.3 Device Classification...................................................................................... 9
1.4 Warnings and Cautions ............................................................................... 10
1.5 Monitoring and alarms ................................................................................. 10
2
Operating Instructions.................................................................... 11
2.1 Connect the Ventilator ................................................................................. 11
2.2 Check for Leaks...........................................................................................11
2.3 Check Alarm Functions................................................................................ 12
2.4 Settings........................................................................................................12
2.4.1 Timing ...............................................................................................12
2.4.2 Volume..............................................................................................12
2.4.3 PEEP ................................................................................................ 12
2.4.4 Pressure............................................................................................ 12
2.4.5 Flow .................................................................................................. 12
2.4.6 CPAP ................................................................................................12
2.5 Pressure Cycling Option (NOT FITTED AS STANDARD) ...........................13
2.6 In Use with a Patient....................................................................................13
2.6.1 Setting the alarm............................................................................... 14
2.6.2 To switch off...................................................................................... 14
3
Care and Maintenance .................................................................... 15
3.1 Cleaning intervals ........................................................................................ 15
3.2 Method for cleaning ventilator...................................................................... 15
3.3 Disinfection ..................................................................................................19
3.3.1 Chemical disinfecting ........................................................................19
3.3.2 Steam Autoclaving components........................................................ 19
3.3.3 Gas sterilising ................................................................................... 20
3.4 Care and Maintenance of Bellows ............................................................... 20
5

EV500 User Manual
4
Principles of Operation................................................................... 21
4.1 The electronic system.................................................................................. 21
4.2 The Pneumatic System................................................................................ 22
4.3 Ventilation Circuits .......................................................................................22
4.3.1 Circle system .................................................................................... 22
4.3.2 Tee piece ..........................................................................................22
4.3.3 Non-rebreathing one way systems.................................................... 23
5
Technical description ..................................................................... 25
5.1 Power supply ...............................................................................................25
5.2 Micro-controller............................................................................................25
5.3 Alarms ......................................................................................................... 25
5.4 Pressure transducer amplifier...................................................................... 26
6
Troubleshooting.............................................................................. 27
6.1 To access internal electronics ..................................................................... 27
6.2 Main PCB Assembly Parts List ....................................................................29
7
Service and Calibration................................................................... 33
7.1 Service intervals and components ............................................................... 33
7.2 VE500-99 Service kit ................................................................................... 33
7.3 Tools to be used ..........................................................................................34
7.4 Preparation to service EV500 Electronic Ventilator ..................................... 34
7.5 Service Procedure ....................................................................................... 35
7.6 Post Service Tests....................................................................................... 42
7.7 Performance check...................................................................................... 44
8
Physical Features............................................................................ 45
8.1 EV500 Ventilator (front view) .....................................................................45
8.2 EV500 Ventilator (rear view)........................................................................ 46
8.3 Connection Schematic................................................................................. 47
8.4 Assembly Drawings ..................................................................................... 48
8.5 Top Cover Assembly EV501M..................................................................... 49
8.6 Bottom Shelf Assembly EV502.................................................................... 49
8.7 Manometer Assembly EV105 ...................................................................... 50
6

EV500 User Manual
8.8 Head Assembly EV504................................................................................ 51
8.9 Weight Assembly VE50432 ......................................................................... 51
8.10 Connector Assembly Exhaust EV5043 .................................................... 52
8.11 Fastener Assembly AB20102................................................................... 52
8.12 Vent Canister Assembly VE505 ............................................................... 53
8.13 Bellows Assembly EV506 ........................................................................ 54
8.14 Volume Control Assembly VE507 ............................................................ 55
8.15 Venturi Block Assembly EV508................................................................ 56
8.16 Flow Block Assembly EV509 ................................................................... 57
8.17 Silencer Assembly VE511........................................................................ 58
8.18 Outer Silencer Assembly VE1112 ............................................................ 58
8.19 Ventilator Drive Assembly EV513 ............................................................ 59
8.20 Solenoid Valve Assembly EV514 .............................................................60
8.21 Selector Valve Assembly VE116.............................................................. 61
8.22 Inspiratory Pressure Valve Assembly EV519-IP ...................................... 61
8.23 Expiratory Pressure Valve Assembly EV519-EP...................................... 62
8.24 Hose Assembly – Oxygen HO-20 ............................................................ 62
9
Schematic Diagrams ....................................................................... 63
9.1 Magill Circuit ................................................................................................63
9.2 Bain Circuit .................................................................................................. 64
9.3 Circle System .............................................................................................. 65
9.4 Disassembly ................................................................................................ 66
9.5 Pneumatic Circuit......................................................................................... 67
10 Specifications.................................................................................. 69
10.1 Physical....................................................................................................69
10.2 Controls....................................................................................................69
10.3 Pneumatic Specifications .........................................................................69
10.4 Power Supply...........................................................................................69
10.5 Environmental ..........................................................................................70
10.6 Electromagnetic Compatibility.................................................................. 70
10.6.1 Electromagnetic Emissions ............................................................. 70
10.6.2 Electromagnetic Immunity ............................................................... 70
10.6.3 Recommended Separation Distance............................................... 71
7
EV500 User Manual
10.6.4 Recommended Separation Distances from Portable and Mobile RF
Communication Equipment........................................................................... 72
11 Terms and conditions ..................................................................... 73
8
EV500 User Manual
1111 Introduction
Introduction
IntroductionIntroduction
1.1
1.1 About this manual
About this manual
1.11.1
About this manualAbout this manual
This manual provides information for the preparation, use and care of the EV500
anaesthetic ventilator, together with suitable equipment from the Ulco range. Although
this equipment has been carefully designed for simplicity of assembly and use, it is
recommended that the contents of this manual be studied before attempting preparation or
care of the equipment. Explanatory diagrams are provided in order to help the reader
understand the concepts described.
This user manual should be read in conjunction with the user manual(s) for the vaporisers,
anaesthesia gas delivery system, absorbers and monitoring equipment.
1.2
1.2 Intended Use
Intended Use
1.21.2
Intended UseIntended Use
The EV500 Anaesthetic Ventilator is a medical device for providing Intermittent Positive
Pressure Ventilation during procedures requiring inhalation anaesthesia for human adults
and children above 5kg body weight.
The apparatus is intended for use solely in an operating or induction room.
The apparatus is intended to be used with hospital gas supply pressures within the range
280 - 500 kPa.
The apparatus is intended to be used under the continuous control of a person suitably
trained and clinically qualified in its use.
To comply with the Anaesthetic Workstation standard IEC 60601-2-13, the EV500 shall be
used with monitoring and alarms as described in Section 1.5.
In addition, the EV500 ventilator shall be used in conjunction with an automatic gas
scavenging system (AGSS).
1.3
1.3 Device Classification
Device Classification
1.31.3
Device ClassificationDevice Classification
The EV500 was assessed for safety to the international standard IEC 601-1:1988 + A1 +
A2.
The EV500 Anaesthetic Ventilator is classified as follows:
• Class I equipment for the purposes of electrical safety
• Type CF applied part
• Continuous Operation
9
EV500 User Manual
1.4
1.4 Warnings and Cautions
Warnings and Cautions
1.41.4
Warnings and CautionsWarnings and Cautions
• NOT FOR USE IN THE PRESENCE OF FLAMMABLE ANAESTHETIC AGENTS
• The ‘BOTTOM’ pressure alarm setting must be adjusted such that the green
pressure bar display brightens on the peak of every breath but the lower set limit
bar display is not flashing. If it is flashing then it indicates that it is set too low and
may not be sensitive to drop in cycling pressure. I.e. from a disconnection.
• If the unit alarms, check the patient. Establish that the patient is being ventilated
correctly.
• This equipment is an adjunct to patient safety and it must in no way replace the
normal monitoring by skilled personnel. The manufacturer accepts no responsibility
for incidents arising from either incorrect use or malfunction of this equipment.
• Power line voltage is present on the main PCB. Mains voltage can be encountered
at the fuses, mains inlet and PCB. Ensure the unit is unplugged whenever you are
disassembling it.
• It is strongly recommended that pulse oximeters, Oxygen analysers and end tidal
CO2 monitors be used. These will help to ensure patient safety, make precise
ventilation possible and so achieve the best possible ventilator parameters for the
patient.
• The unit will automatically switch off if the standby battery is too low to ensure
reliable operation.
• An authorised Ulco Technical Service Representative must perform maintenance
on this equipment. Ulco products in need of factory repairs must be sent to the
nearest local agent or directly to Ulco.
WARNING
DO NOT USE IN THE PRESENCE OF FLAMMABLE ANAESTHETICS
PLEASE NOTE OVERPRESSURE CYCLING (PAGE 5)
1.5
1.5 Monitoring and alarms
Monitoring and alarms
1.51.5
Monitoring and alarmsMonitoring and alarms
This unit must be used in conjunction with equipment providing the following alarms and
monitoring capabilities:
• Inspiratory oxygen concentration
• Anaesthetic agent concentration
• CO2 concentration
In addition, monitoring of exhaled volume is strongly recommended.
10

EV500 User Manual
2222 Operating Instructions
Operating Instructions
Operating InstructionsOperating Instructions
This all-purpose anaesthesia ventilator is TIME CYCLED and gas driven. It should be
connected to a supply line of 350-450 kPa (50-70 lb/sq inch), this being the standard
operating theatre supply line pressure for inhalation gases. Reduced cylinder pressure is
also within this range.
Medical grade oxygen or air can be used but oxygen is preferable as it is free from
impurities such as oil and moisture.
An operator unfamiliar with the ventilator should note the various controls and be sure to
understand how variations of each control affect patient ventilation. If uncertain, operators
should practice running the ventilator prior to connection to the patient and become
familiar in setting the volume, timing and the inspiratory pressure.
Inspiratory pressure adjustments can be done by occluding the ventilator’s patient outlet
during the inspiratory phase and adjusting the Insp. Pressure control whilst watching the
pressure gauge. Make sure the bellows are expanded and not fully compressed during
this adjustment as the gauge measures the circuit and not the driving pressure.
2.1
2.1 Connect the Ventilator
Connect the Ventilator
2.12.1
Connect the VentilatorConnect the Ventilator
Connect ventilator to anaesthetic machine as shown in the diagram and set the required
gas flow on the flowmeter, then press the oxygen flush to fill the bellows. Connect power
to the ventilator and ensure that the green MAINS LED is on.
2.2
2.2 Check for Leaks
Check for Leaks
2.22.2
Check for LeaksCheck for Leaks
This is done to confirm the satisfactory function of the one way valve at the base of the
bellows and to ensure the absence of leaks in and around the bellows.
With the ventilator turned off and the bellows fully expanded (gas flow approximately 1
L/min), occlude the patient connection. Loosen the lock nut of the volume control, and
slide the volume-adjusting spindle up and down. It should move freely, and the bellows
should return to its fully expanded position after a short duration (depending in the gas
flow). Set inspiration pressure to the maximum and turn the MODE selector to POS. The
ventilator should switch on and the audible alarm, the HIGH and LOW LEDs and the red
flashing MAINS LED should come on for approximately 1 second. The green pressure bar
graph and the red timing displays all come on. Take note if any segment or alarm is not
working.
On inspiration (with the outlet of the Y-piece occluded and the bellows fully expanded) the
ventilator gauge should register the maximum pressure without the bellows compressing
no more than a small amount and return to full expansion on expiration. If the bellows do
not return to their original volume and continue to lose further volume, a leak exists either
in the bellows, the one way valve or the breathing circuit
11

EV500 User Manual
2.3
2.3 Check Alarm Functions
Check Alarm Functions
2.32.3
Check Alarm FunctionsCheck Alarm Functions
Set the TOP SET LIMIT control such that the inspiratory pressure exceeds it. Check that
the HIGH LED is on, the alarm sounds and switches to Expiration (There is no audible
alarm if the alarm is muted by the OFF/RESET switch or if the unit is still in the 1 minute
mute period after being turned on).
Set the BOTTOM SET LIMIT control such that inspiratory pressure is less than it. Check
that after approximately 20 seconds, the LOW LED is on and that the alarm sounds (if it is
not muted).
2.4
2.4 Settings
Settings
2.42.4
SettingsSettings
2.4.1
2.4.1 Timing
2.4.12.4.1
Timing
TimingTiming
The timing is set by the INSPIRATORY TIME and RATE control knobs. The settings are
displayed by the LEDs under their corresponding inscriptions. Setting the RATE (breaths
per minute) will not alter the inspiratory time, but the resultant I:E ratio which is also
displayed will alter. Parameters will stay within the range set in the ‘Specifications’
section.
2.4.2
2.4.2 Volume
2.4.22.4.2
Volume
VolumeVolume
The tidal volume is set by adjusting the bellows limit rod (loosen the lock nut to adjust and
tighten after adjustment has been made) to the desired inscribed level. Note that the
markings are approximate and expired volume monitoring may be necessary for exact
volume determination.
2.4.3
2.4.3 PEEP
2.4.32.4.3
PEEP
PEEPPEEP
Should PEEP be necessary, turn the mode selector to PEEP and adjust the expiratory
pressure control to the required level during expiration. The maximum PEEP is limited to
20 cmH2O pressure.
2.4.4
2.4.4 Pressure
2.4.42.4.4
Pressure
PressurePressure
The inspiratory pressure control is adjusted so that when the patient is ventilated the
required volume is delivered within the previously set inspiratory time.
2.4.5
2.4.5 Flow
2.4.52.4.5
Flow
FlowFlow
This control changes the Inspiratory characteristics of the ventilator from a flow generator
(nil entrainment) in the closed position, to a pressure generator (full entrainment) in the
open position. Positions between these two extremes offer a unique ability to combine flow
and pressure generation.
2.4.6
2.4.6 CPAP
2.4.62.4.6
CPAP
CPAPCPAP
If CPAP is inadvertently selected the ventilator will stop cycling.
12
EV500 User Manual
Reset the mode selector to the POS or PEEP position to restart cycling.
2.5
2.5 Pressu
Pressure Cycling Option (NOT FITTED AS STANDARD)
2.52.5
PressuPressu
WARNING
To pressure cycle the ventilator, set Inspiratory time and inspiratory pressure to maximum
then set the upper limit LED to the required switching pressure. When the two LED’s
meets, the ventilator will switch to expiration. An audible BEEP will sound every time the
pressure limit is reached (over pressure limit).
NB. The rate display does not show the pressure cycling rate but the set rate that was
selected for time cycling. (This mode is intended as a safety system for overpressure).
2.6
2.6 In Use with a Patient
In Use with a Patient
2.62.6
In Use with a PatientIn Use with a Patient
Ensure that the proposed breathing circuit is compatible with the ventilator used. Turn on
the ventilator and adjust the timing, volume and pressure to approximate requirements.
Connect the patient and then make the final fine adjustments to suit the characteristics of
the lungs (i.e. individual variation in compliance, airways resistance and required minute
volume). Check that the expiratory pressure falls to zero at each cycle (i.e. no obstruction
in the expiratory pathway).
Pollution control systems may be attached to the exhaust of the ventilator. It is important
to guard against possible obstruction and excess suction. Both will be indicated on the
ventilator gauge (not returning to zero if obstructed or the bellows being sucked up during
the expiratory period if the suction is too high and a negative pressure is being generated).
Confirm adequate ventilation of the patient by observing good chest movement with each
inspiration. Make sure all connections are leak free and firmly connected. Unnecessary
high inspiration pressures should be avoided. Set the inspiratory pressure and time so
that the selected volume is delivered just before the inspiration ends to obtain a plateau.
With the circle system ensure that all dump (APL) valves are closed off as venting is
through the rear of the ventilator.
A suggested method of setting the inspiratory parameters is to first place the flow control
in the mid position. The required tidal volume is selected and the required inspiratory time
is set. The inspiratory pressure is then adjusted so that the tidal volume is delivered just
before the end of the inspiratory period. The suggested expiratory time is 3 times the
inspiratory time. For adults, for example, an inspiration time of 1 second (rate 15 BPM
ratio 1:3). When set as described the following features will be seen:
1. A short period of ‘inspiratory hold’ when the tidal volume has been delivered and
re Cycling Option (NOT FITTED AS STANDARD)
re Cycling Option (NOT FITTED AS STANDARD)re Cycling Option (NOT FITTED AS STANDARD)
the expiratory time has not yet begun. This is seen on the pressure gauge as a
pressure drop and a momentary hold at this lower pressure. This is an indication
of compliance (lung and chest wall) and compliance changes occurring during the
anaesthetic can be monitored.
2. The inspiratory ‘hold’ is a good indication that the circuit is leak free. A continually
falling pressure at this point (with healthy lungs) indicates a leak in the circuit (eg
deflated endotracheal tube cuff).
13
EV500 User Manual
3. Ventilation volume, once set, will remain constant throughout the anaesthetic in
spite of minor changes in compliance eg tilting the patient or a relaxant partially
wearing off.
4. If varying times constants exist within the lungs (eg severe COAD) better
ventilation of the slow fillers is achieved with an inspiratory hold phase and
atelectasis is prevented.
2.6.1
2.6.1 Setting the alarm
2.6.12.6.1
Setting the alarm
Setting the alarmSetting the alarm
1. Switch the ‘0-30/0-60’ switch to 0-30 unless you are using pressure in excess of
30 cmH2O.
2. Adjust the BOTTOM SET LIMIT such that it is lower than the peak inspiratory
pressure. The display should brighten on every breath without the lower bar
flashing. If it is flashing then it indicates that it is set too low and may not be
sensitive to drops in cycling pressure (eg from a disconnection).
3. Adjust the TOP SET LIMIT such that it is just higher than the peak inspiratory
pressure.
4. Check, after 1 minute, that the alarms are off. If the MAINS red LED is flashing
and the alarm is sounding intermittently, then either the alarms battery may need
to be renewed or the internal battery recharged.
5. If the numerical displays are flashing, then the parameter has changed
significantly from the previous breath.
6. If CPAP is being used, adjust the BOTTOM set limit counter clockwise until the
LOW alarm just extinguishes.
7. Pressing the PRESS FOR OFF button will mute the alarm for 1 minute.
2.6.2
2.6.2 To switch off
2.6.22.6.2
To switch off
To switch offTo switch off
To switch the unit off, switch off the ventilator and press the PRESS FOR OFF button until
the displays are off. ‘1’ will be displayed for approximately 20 seconds and turn off and
then only the green ‘MAINS’ LED should be on.
14
EV500 User Manual
3333 Care and Maintenance
Care and Maintenance
Care and Maintenance Care and Maintenance
3.1
3.1 Cleaning intervals
Cleaning intervals
3.13.1
Cleaning intervalsCleaning intervals
The ventilator is an automatic bag squeezer, and the bellows within the ventilator takes
the place of a normal rebreathing bag. Therefore, the bellows should be cleaned as often
as a rebreathing bag, usually after any infected case or at the end of the day. If an inline
bacterial filter is fitted on the breathing hose to the ventilator, cleaning will only be needed
once every one or two months.
Note: The filter should be replaced in accordance with the manufacturer’s
recommendations.
3.2
3.2 Method for cleaning ventilator
Method for cleaning ventilator
3.23.2
Method for cleaning ventilatorMethod for cleaning ventilator
The machine must be disconnected from the mains before cleaning or disinfecting. The
ventilator’s outer surfaces can be cleaned using a soft cloth and mild soap solution. After
washing, wipe with clean water and allow to dry. Do not allow fluids to penetrate the
housing or any of the external connectors.
In all cases, care must be taken in order to prevent liquids from entering the electronics
situated in the base of the ventilator.
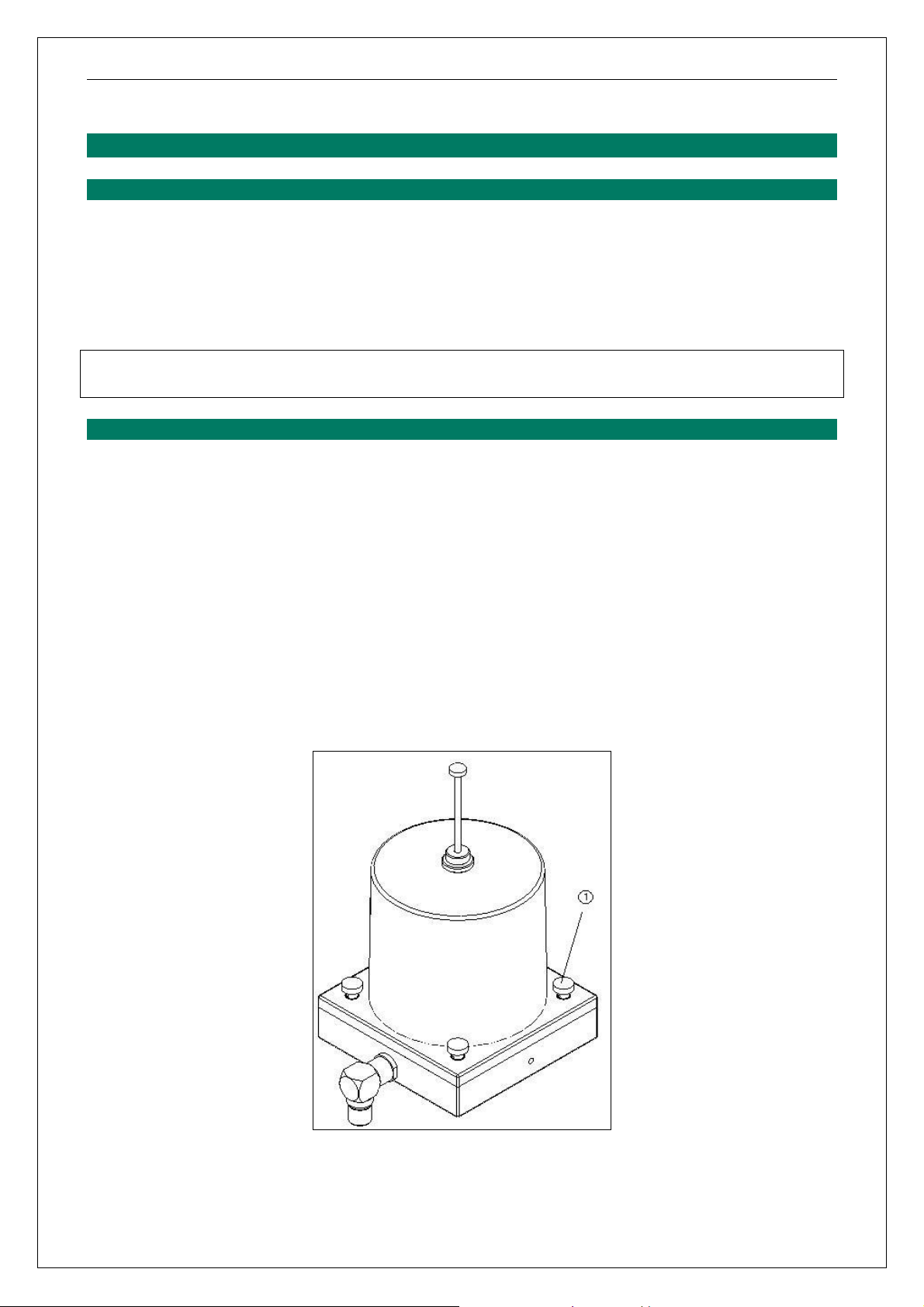
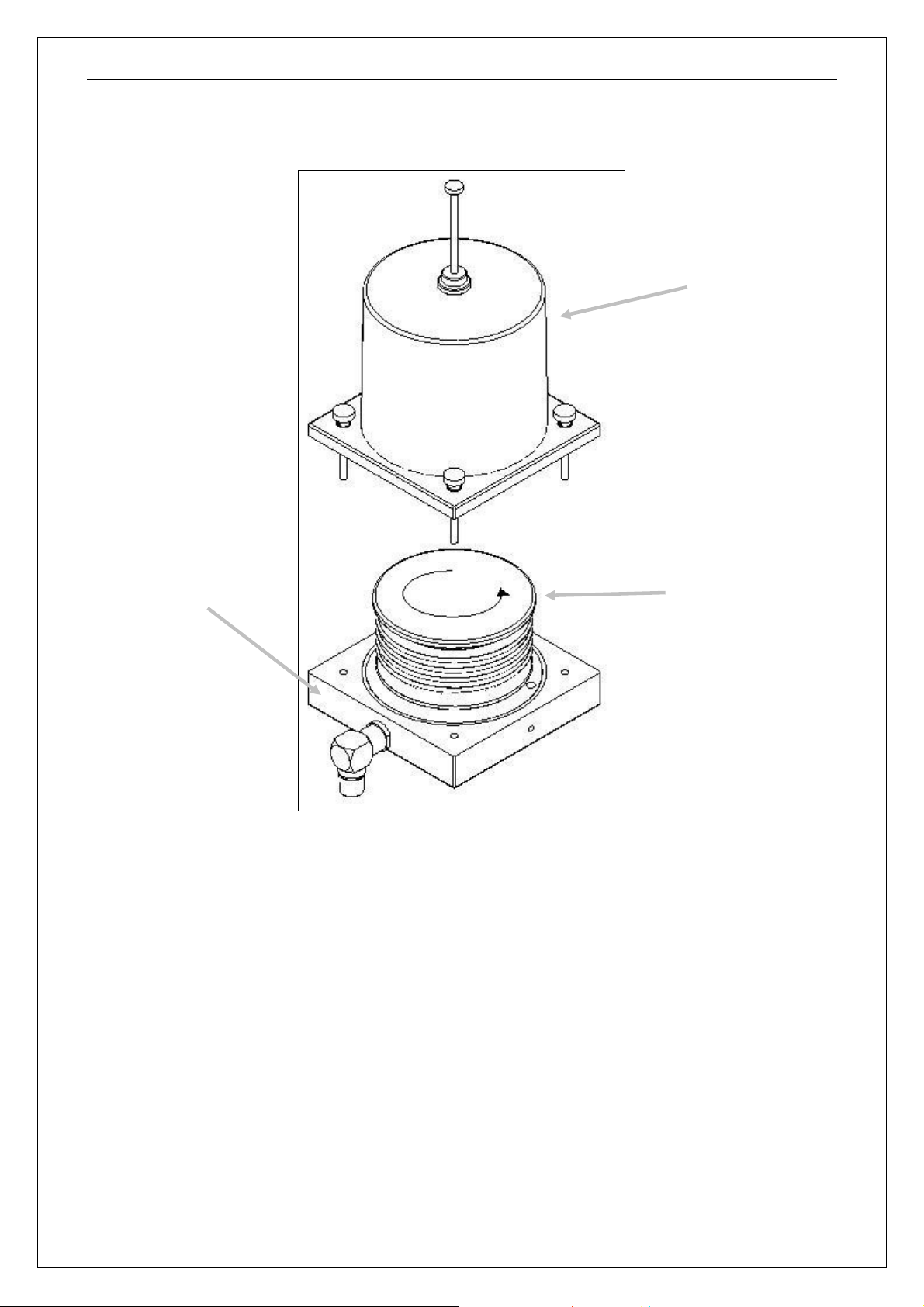
Dismantle the ventilator
1. Loosen the four knurled screws (labelled (1) in Figure 1) and remove the bellows
canister
Figure 1: Location of knurled screws
15
EV500 User Manual
Canister
Bellows
Ventilator
2. Remove the ventilator head assembly from the ventilator by pulling upward on the
delrin block.
Head
Assembly
Figure 2: Removal of bellows canister and bellows bag assembly
3. Remove the bellows assembly by rotating in counter-clockwise as shown in Figure 2.
16
EV500 User Manual
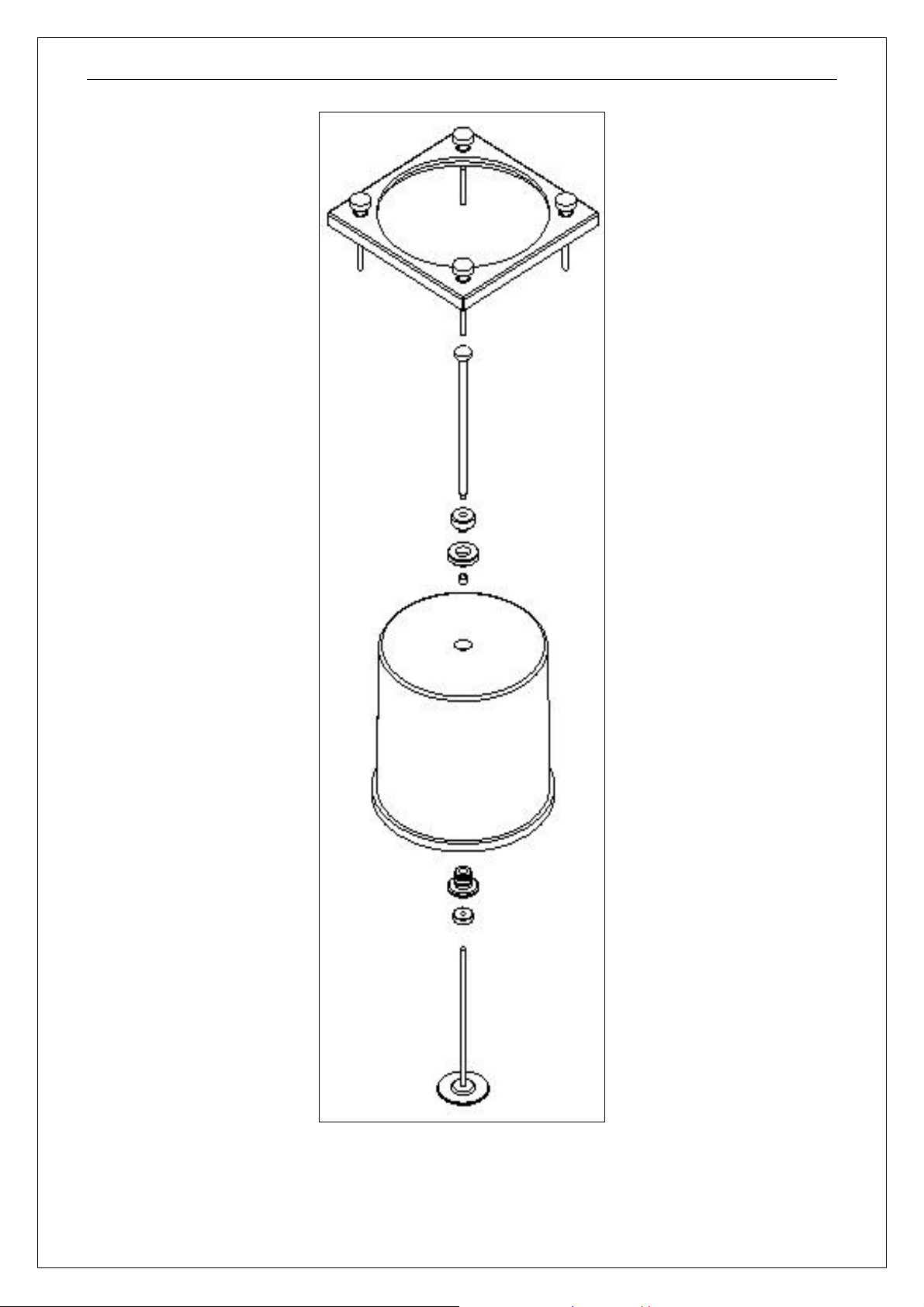
Figure 3: Disassembly of Volume control assembly
17
EV500 User Manual
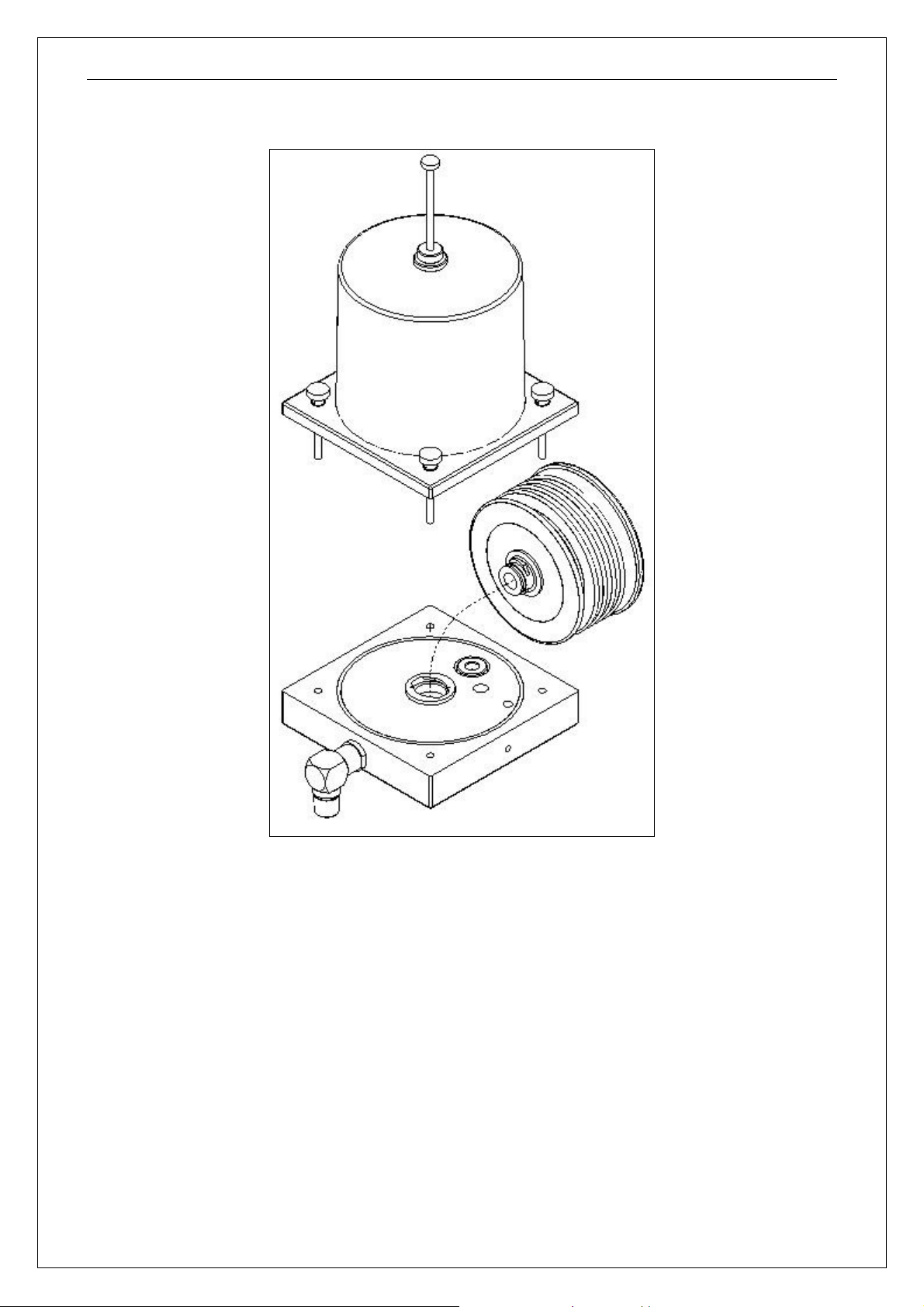
Figure 4: Bellows assembly removed from ventilator head
4. The ventilator head can be put through a washer at 80°C.
5. The bellows canister may be washed or autoclaved (volume control must be removed
as shown in Figure 3).
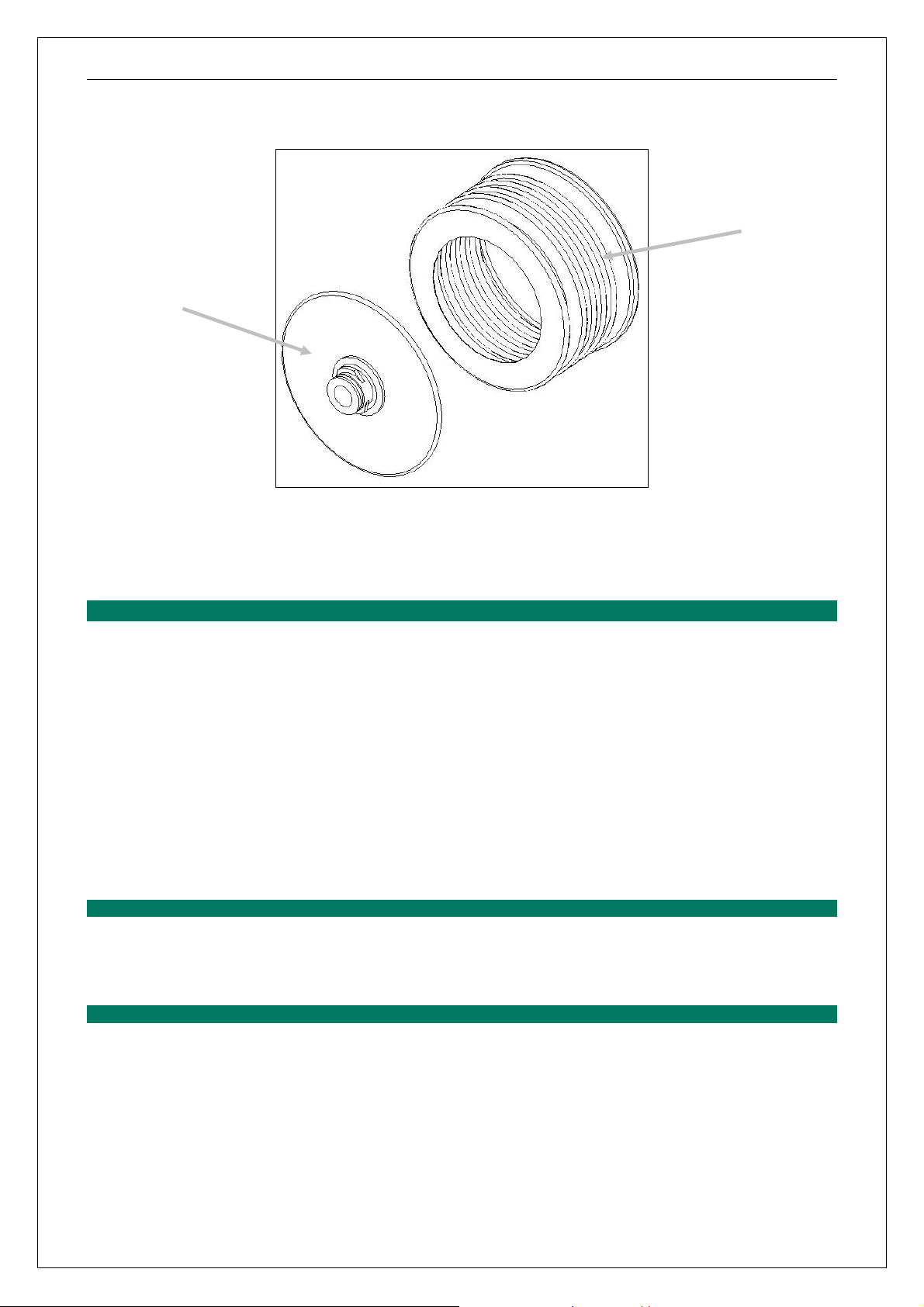
6. The base disk (mushroom) should be removed from the bellows assembly before
washing. Pull the rubber bag from the delrin base disk as shown in Figure 5. The
bellows may be washed or autoclaved. The base component (mushroom) should not
be autoclaved but can be put through a washer at 80°C.
18
EV500 User Manual
Bellows
Bellows
mushroom
Figure 5: Bellows assembly with mushroom removed
7. Dry all components thoroughly before re-assembly. Low pressure warm air should be
passed through the ventilator head by attaching a hose to the scavenge port.
3.3
3.3 Disinfection
Disinfection
3.33.3
DisinfectionDisinfection
If the unit has been contaminated, the whole ventilator may be gas sterilised. Do not
sterilise the ventilator using radiation sterilisation techniques.
A disinfectant may also be used when cleaning the ventilator, if diluted with water. First
wipe the whole ventilator with a damp sponge containing disinfectant, then remove the
canister, bellows and head assembly as described above and wipe the inside of the
ventilator (chamber).
Individual components may be cleaned using a washer (Meile or similar). Breathing
circuits and components such as ventilator bellows, canisters and head should be washed
at approximately 80°C with a slightly alkaline detergent solution (pH 10-11).
3.3.1
3.3.1 Chemical disinfecting
3.3.13.3.1
Chemical disinfecting
Chemical disinfectingChemical disinfecting
• Wash in soap solution and then dry
• Soak in 2% glutaraldehyde (pH 6.5) for 19-20 minutes. Rinse and dry thoroughly.
3.3.2
3.3.2 Steam Autoclaving components
3.3.23.3.2
Steam Autoclaving components
Steam Autoclaving componentsSteam Autoclaving components
Normally this is not required for anaesthesia equipment and accessories. If autoclaving is
needed, use the glove cycle. Do not autoclave the head assembly or the base disk of the
bellows bag assembly.
19

EV500 User Manual
3.3.3
3.3.3 Gas sterilising
3.3.33.3.3
Gas sterilising
Gas sterilisingGas sterilising
ETO gas sterilising can be carried out on all removable components after washing or on
the entire ventilator. Aerate thoroughly after gassing.
3.4
3.4 Care and Maintenance of Bellows
Care and Maintenance of Bellows
3.43.4
Care and Maintenance of BellowsCare and Maintenance of Bellows
Reversion and loss of strength is usually the result of exposure to high temperatures or
excessive age. Some other factors, which cause degradation of natural rubber, are copper
and manganese containing materials, which can include some water supply systems. The
copper acts as a catalyst to degrade the rubber and surprisingly small amounts can lead
to very rapid aging of the rubber, causing loss of strength.
Contact with solvents or oils can also damage rubber and can lead to tackiness and loss
of strength, but will usually swell the rubber while it is still present. The rubber is
compounded with antioxidants which are intended to preserve it against oxidation and
aging, but if very powerful detergents or soaps are used to clean the bellows, these may
leak out leaving the rubber largely unprotected.
Other agents, which will attack rubber, are SUNLIGHT, ULTRA VIOLET light and OZONE.
Temperatures in excess of 80°C will cause reversion and at 100°C this occurs quite
rapidly.
SUGGESTED PROTECTIVE METHODS
• Keep spare bellows in boxes and away from fluorescent (in the dark)
• Use only mild soaps and warm water to clean the bellows.
• The bellows should be dried while fully expanded.
20

EV500 User Manual
4444 Principles of Operation
Principles of Operation
Principles of OperationPrinciples of Operation
The ventilator is divided into 2 main systems, electronic and pneumatic.
4.1
4.1 The electronic system
The electronic system
4.14.1
The electronic systemThe electronic system
The electronic system is a micro-controller based system generating timing signals from a
quartz crystal oscillator. The timing signals are used to control pneumatic valves in the
system. The micro-controller uses internal feedback, COP (computer operating properly)
and watchdog pulses to monitor its performance and check for abnormalities. The microcontroller generates the LED display and the alarms. The main PCB module, the EV200,
has the power supply, battery charger, pressure transducer and peripheral drivers on
board. It incorporates a ventilation disconnection alarm system which monitors the patient
airway pressure. It is designed to indicate an alarm condition if:
the patient airway pressure has not cycled above and below a manually set
pressure level within 16 seconds
the patient airway pressure has exceeded the overpressure set point
in CPAP mode the pressure drops below the BOTTOM SET LIMIT for more than
1 second
the unit detects an internal system fault:
o the standby battery is too low (battery low LED flashes and the alarm
sounds intermittently)
o the alarm’s battery is too low (battery low LED flashes and the alarm
sounds intermittently)
o the standby battery has failed (battery low LED flashes and the alarm,
unless muted, sounds)
o the micro-controller has failed, i.e. watchdog alarm (continuous sounding
alarm)
The audible alarm is muted for one minute when the unit is turned on and when off/reset is
pressed. This allows for the patient and ventilator to be adjusted to establish correct
functional conditions.
To switch the unit off, the ventilator must be first turned off and the OFF/RESET button
held for approximately 2 seconds. An alarm will sound after approximately 1.5 seconds
until the unit is off to signal the OFF condition. The green pressure bar graph and the red
timing display will go blank except for ‘1:’ in the ratio display. This will stay on for
approximately 20 seconds and then blank as well.
Note that if the OFF/RESET button is held for approximately 15 seconds the unit will turn
off, even if the micro-controller has failed (watchdog alarm). If the ventilator is still on, the
unit will then turn back on (reset).
21

EV500 User Manual
The unit will turn off if the standby battery is too low to ensure reliable operation. This is
also to protect it from excessive discharge.
4.2
4.2 The Pneumatic System
The Pneumatic System
4.24.2
The Pneumatic SystemThe Pneumatic System
The pneumatic system is used to compress the bellows via needle valves, jets, and a
venturi. The motive force is derived from the driving gas.
With the ventilator connected to drive gas supply, switching the ventilator mode selector to
ON will cause a pressure switch to operate, causing power to be applied to the EV200
assembly. This will start the timing sequence. On inspiration, the EV200 turns on the high
pressure supply to the main (positive) jet. The flow to this jet is regulated by the
inspiration pressure control needle valve such that the venturi pressure ranges from
0cmH2O to 60 cmH2O. The inspiratory time display will brighten slightly. At the end of the
inspiration time, the EV200 deactivates the cycle valve, the inspiratory time display dims,
and the expiratory time display brightens.
If the MODE selector is in the PEEP position, then the EXP pressure control needle valve
regulates the flow (from the cycle valve in the resting state) such that the venturi pressure
ranges from 0 cmH2O to 20 cmH2O.
The patented venturi system prevents excessive pressure in the patient circuit, without the
need for spring operated relief valves that can stick. The venturi is directly connected to
the breathing circuit via the bellows and to atmosphere via a flap valve to prevent air
entrainment. Should air entrainment be required to increase flow, then the flow control
may be used. Flow can be increased to over 100 L/min.
When the pressure set by the control valve is reached, then the venturi stalls and the
excess pressure flows to atmosphere via the flap valve.
4.3
4.3 Ventilation Circuits
Ventilation Circuits
4.34.3
Ventilation CircuitsVentilation Circuits
4.3.1
4.3.1 Circle system
4.3.14.3.1
Circle system
Circle systemCircle system
The EV500 can be used with any standard anaesthesia machine with a circle system.
The ventilator replaces the rebreathing bag and the circle absorber dump valve is closed
off. Venting is through the ventilator.
4.3.2
4.3.2 Tee piece
4.3.24.3.2
Tee piece
Tee pieceTee piece
The tee piece is well suited for use with babies, although it can also be used with adults.
The Bain is a tee piece circuit. The ventilator is attached to the expiratory limb of the tee
piece. For babies and small children, a one way valve on the expiratory limb can also be
used and results in only fresh gas flow ventilating the patient.
It is sometimes used to avoid the possibility of a large volume of gas distending the lungs
of a neonate, but mostly ventilation is done without the one way valve and inspiration
pressure kept low. With adults (eg the Bain circuit), fresh gas flows must be kept high
enough to prevent excessive rebreathing.
22

EV500 User Manual
4.3.3
4.3.3 Non
4.3.34.3.3
Non----rebreathing one way systems
rebreathing one way systems
NonNon
rebreathing one way systemsrebreathing one way systems
These are for adult use and can be used for air or anaesthetic gases. The ventilator can
function as a minute volume divider by adjusting the volume setting to maximum. Each
filling volume of the bellows is then determined by the fresh gas flow during the expiration
period, and the inspiratory pressure is adjusted so that whatever volume is in the bellows
is delivered to the patient.
23
 Loading...
Loading...