

Page 1
Instruction Manual
For the Digital Monitoring System
(Software version SMB SW-V08.02; MPB SW-V06.02)
Page 2

SenTec Digital Monitoring System
Noninvasive Ventilation and Oxygenation Monitoring
[Sarah Miller]
Page 3
19 20 21 22 23 24
15 16 17 18
12 sec
100
70
75
25
- 15 min 0 min
- 15 min 0 min
0 min
39.4
50
30
PCO2
mmHg
84
140
50
PR
bpm
96
100
85
%SpO2
2.0 PI
100%
+
-
7.7h
AD
°C
42.0
RHP
0
[John Smith]
2014-04-28 15:28:31
1 2 3 4
5
6
7
8101213
14
11 9
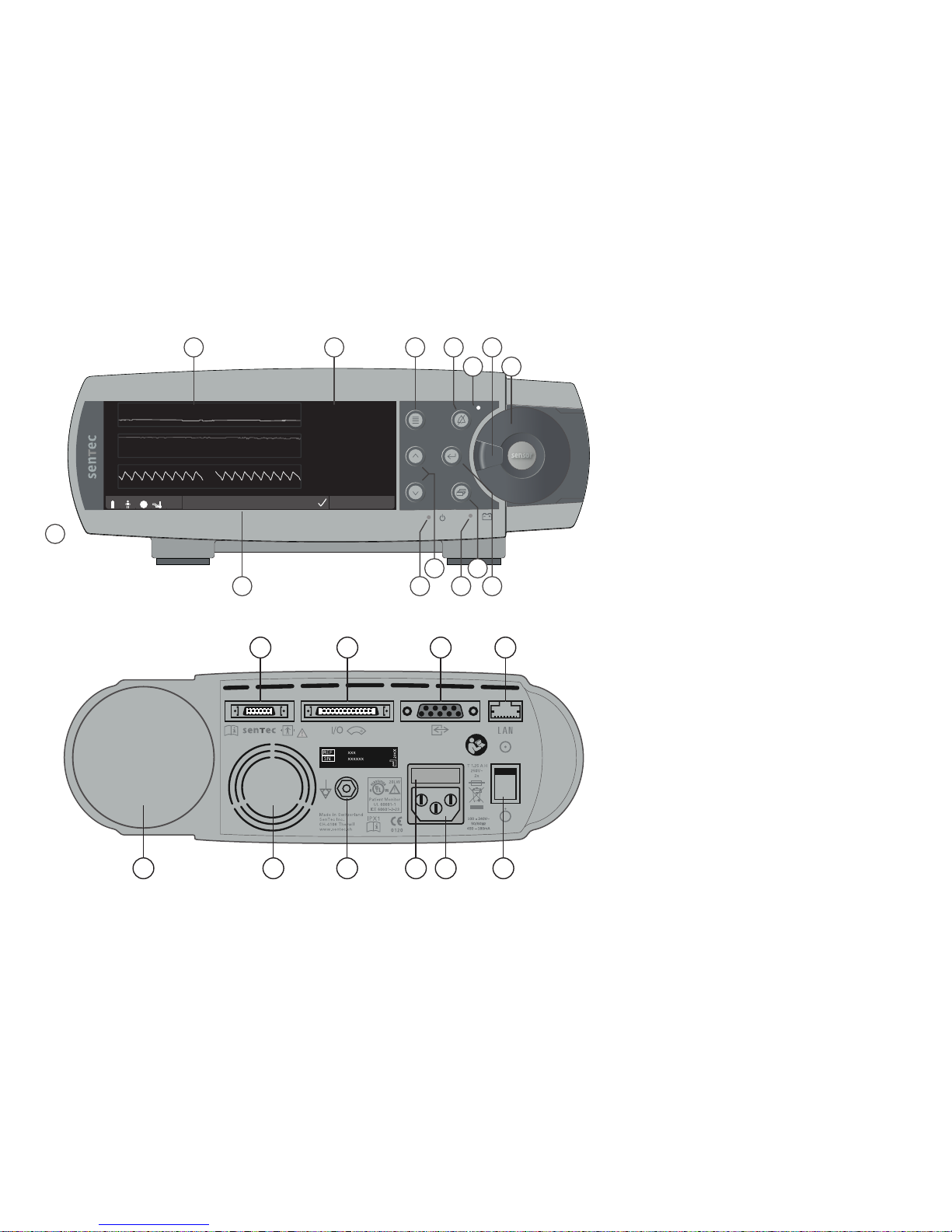
1 Trend Display Area
2 Numerical Display Area
3 Menu/Previous Level Button
4 AUDIO PAUSED/OFF Button
5 AUDIO PAUSED/OFF Indicator (yellow LED)
6 Door Handle
7 Docking Station Door (colored dot in center
of door indicates the SDM’s PO
2
activation
status: blue if activated, orange otherwise)
8 Enter Button
9 Display Button
10 AC Power/Battery Indicator
(green/yellow LED)
11 UP/DOWN Buttons
12 ON/OFF Indicator (green LED)
13 Status Bar
14 Speaker (on the side)
15 Sensor Connection Port
16 Multipurpose l/O-Port
(Nurse Call & Analog Output)
17 Serial Data Port (RS-232)
18 Network Port (LAN)
19 Gas Bottle Slot
20 Fan
21 Equipotential Terminal Connector (ground)
22 Fuse Holder
23 AC Power Connector
24 ON/OFF Switch
Page 4

C
L
A
S
S
I
F
I
E
D
U
L
C U
S
R
Warranty
The manufacturer warrants to the initial purchaser that each new component of the SenTec Digital Monitoring System will be free from defects in
workmanship and materials. The manufacturer’s sole obligation under this warranty is to at its own choice repair or replace any component – for
which the manufacturer acknowledges the warranty cover – with a replacement component.
Warranty Exclusions and System Performance
SenTec AG can neither guarantee or verify instrument performance characteristics nor accept warranty claims or product liability claims if the
recommended procedures are not carried out, if the product has been subject to misuse, neglect or accident, if the product has been damaged
by extraneous causes, if accessories other than those recommended by SenTec AG are used, if the warranty seal on the lower side of the monitor
is broken, or if instrument repairs are not carried out by SenTec authorized service personnel.
CAUTION: Federal law (U.S.) restricts this device to sale by or on the order of a physician.
Patents/Trademarks/Copyright
International Industrial Design No. DM/054179, Japanese Design No. 1137696, U.S. Design Patent No. D483488. Canadian Patent No. 2466105,
European Patent No. 1335666, German Patent No. 50111822.5-08, Spanish Patent No. 2278818, Hongkong Patent No. HK1059553, U.S. Patent
No. 6760610. Chinese Patent No. ZL02829715.6, European Patent No. 1535055, German Patent No. 50213115.2, Spanish Patent No. 2316584,
Indian Patent No. 201300, Japanese Patent No. 4344691, U.S. Patent No. 7862698. SenTec™, V-Sign™, OxiVenT
TM
, V-STATS™, V-CareNeT™,
V-Check™, Staysite™, Illuminate Ventilation™ and Advancing Noninvasive Patient Monitoring™ are trademarks of SenTec AG / © 2018 SenTec AG.
All rights reserved. The contents of this document may not be reproduced in any form or communicated to any third party without the prior
written consent of SenTec AG. While every effort is made to ensure the correctness of the information provided in this document, SenTec AG
assumes no responsibility for errors or omissions. This document is subject to change without notice.
Patient Monitor
IN ACCORDANCE WITH IEC 60601-1; ANSI/AAMI ES60601-1; CAN/CSA C22.2 No. 60601-1,
IEC 60601-1-2, IEC 60601-2-23, ISO 80601-2-61
Manufacturer: SenTec AG, Ringstrasse 39, CH-4106 Therwil, Switzerland,
www.sentec.com
Page 5
Page 3 . Contents
Contents
Intended Use, Principles of Operation and Limitations .............................................................. 5
Intended Use of the SenTec Digital Monitoring System (SDMS) ......................................................................................5
Transcutaneous PCO2 and PO
2
..........................................................................................................................................5
Pulse Oximetry .................................................................................................................................................................7
SenTec TC Sensors ...........................................................................................................................................................9
The SenTec Digital Monitoring System (SDMS) ........................................................................ 10
Setting up the SDMS ................................................................................................................. 12
Connect SDM to AC Power ............................................................................................................................................. 12
Battery Operation of the SDM ........................................................................................................................................ 12
Turning on the SDM ........................................................................................................................................................ 12
Installation of the Gas Bottle (Service Gas-0812) .......................................................................................................... 13
Connection/Disconnection of Digital Sensor Adapter Cable ........................................................................................... 13
Connection of a SenTec TC Sensor ................................................................................................................................. 14
Sensor Check, Sensor Calibration/Storage and Membrane Change ......................................... 15
Checking a SenTec TC Sensor ........................................................................................................................................15
Sensor Calibration and Storage ......................................................................................................................................16
Changing the Sensor Membrane .................................................................................................................................... 17
Patient Monitoring with the SDMS ............................................................................................ 20
Selection of Patient Type, Measurement Site, and Sensor Attachment Accessory ........................................................ 20
Check SDM Settings and System Readiness ................................................................................................................... 22
Sensor Application Using a Multi-Site Attachment Ring/Easy ......................................................................................... 24
Sensor Application Using an Ear Clip .............................................................................................................................. 27
Patient Monitoring ..........................................................................................................................................................29
Sensor Removal with Multi-Site Attachment Ring/Easy .................................................................................................. 38
Sensor Removal with Ear Clip ......................................................................................................................................... 40
Page 6

Controls, Indicators and Alarms ................................................................................................ 42
Controls (Buttons) .......................................................................................................................................................... 42
LED Indicators ................................................................................................................................................................ 45
Auditory Indicators/Signals ............................................................................................................................................. 45
Alarms ............................................................................................................................................................................ 46
Status Bar with Status Icons and Status Messages ........................................................................................................ 48
Maintenance of the SDMS ......................................................................................................... 50
Routine Checks ............................................................................................................................................................... 50
Service ............................................................................................................................................................................ 51
Specifications of tcPCO2 , tcPO2 and Pulse Oximetry ................................................................ 52
Specifications of tcPCO2 and tcPO
2
................................................................................................................................. 52
Specifications of Pulse Oximetry ..................................................................................................................................... 53
Glossary of Symbols .................................................................................................................. 54
Page 7

Page 5 . Intended Use, Principles of Operation and Limitations
Intended Use of the SenTec Digital
Monitoring System (SDMS)
The SenTec Digital Monitoring System (SDMS) – consisting
of the SenTec Digital Monitor (SDM), sensors and accessories
(p. 10) – is indicated for continuous, noninvasive monitoring
of carbon dioxide tension and oxygen tension as well as oxygen
saturation and pulse rate in adult and pediatric patients. In
neonatal patients the SDMS is indicated for carbon dioxide and
oxygen tension monitoring only. Oxygen tension monitoring is
contraindicated for patients under gas anesthesia.
The SDMS is indicated for use in clinical and non-clinical
settings such as hospitals, hospital-type facilities, intra-hospital
transport environments, clinics, physician offices, ambulatory
surgery centers and – if under clinical supervision – home
environments. The SDMS is for prescription use only.
Note: The above phrasing corresponds to an abbreviated
version of the SDMS’ Intended Use. Please refer to the current
issue of the Technical Manual for the SDM (HB-005752) for the
full phrasing of the SDMS’ Intended Use.
Intended Use, Principles of Operation and Limitations
Transcutaneous PCO2 and PO
2
Principles of Operations of tcPCO2 and tcPO
2
Carbon dioxide (CO2) and Oxygen (O2) are gases that readily
diffuse through body and skin tissue and, therefore, can be
measured by an adequate noninvasive sensor being applied at
the skin surface. If the skin tissue beneath the sensor site is
warmed up to a constant temperature local capillary blood flow
increases, metabolism stabilizes, gas diffusion improves and,
hence, reproducibility and accuracy of CO
2/O2
measurements
at the skin surface improves.
CO
2
tensions measured at the skin surface (PcCO2) are usually
consistently higher than arterial PCO
2
values (PaCO2) in patients
of all ages. It is therefore possible to estimate PaCO
2
from
the measured PcCO
2
using an adequate algorithm. TcPCO2
designates an estimate of PaCO
2
calculated from the measured
PcCO
2
with an algorithm developed by J.W. Severinghaus.
The ‘Severinghaus Equation’ first corrects PcCO
2
measured at
the sensor temperature (T) to 37 °C by using an anaerobic
temperature factor (A) and then subtracts an estimate of the
local ‘Metabolic Offset’ (M).
Note: Hence, the tcPCO
2
values displayed by the SDM are
corrected/normalized to 37 °C and provide an estimate of
PaCO
2
at 37 °C. On the SDM and throughout this manual
(unless explicitly stated otherwise) ‘tcPCO
2
’ is displayed/
labeled as ‘PCO
2
’.
Page 8

In newborns PO2 measured at the skin surface (PcO2) correlates
with arterial PO
2
(PaO2) almost in a one to one relationship at
a sensor temperature of 43 to 44 °C, whereby the accuracy
of PcO
2
compared to PaO2 is best up to PaO2 of 80 mmHg
(10.67 kPa), above which it increasingly tends to read lower
than PaO
2
(especially in adults). As target PaO2 levels in
newborns are usually below 90 mmHg (12 kPa), a correction
of PcO
2
values measured at a sensor temperature of 43 to
44 °C is normally not necessary. TcPO
2
designates an estimate
of PaO
2
and corresponds to the measured PcO2.
Note: On the SDM and throughout this manual (unless
explicitly stated otherwise) ‘tcPO
2
’ is displayed/labeled as ‘PO2’.
Good to know!
Warming the skin tissue beneath the sensor to a constant
temperature improves accuracy as it a) increases capillary
blood flow/induces local arterialization, b) stabilizes
metabolism, and c) improves gas diffusion through skin
tissue. With increasing sensor temperature the application
duration (‘Site Time’) must be evaluated carefully and
adjusted accordingly to reduce the risk of burns. Special
attention must be given to patients with sensitive skin
at the sensor site (e.g. preterm or geriatric patients, burn
victims, patients with skin diseases) and/or very low skin
tissue perfusion beneath the sensor site (e.g. hypothermic
patients, patients with vasoconstrictions, low blood pressure,
or circulatory centralization (shock)).
Please refer to Technical Manual for the SDM (HB-005752)
and the references cited therein for additional information on
transcutaneous blood gas monitoring.
Limitations of tcPCO2 and tcPO
2
The following clinical situations or factors may limit the
correlation between transcutaneous and arterial blood gas
tensions:
• Hypo-perfused skin tissue beneath the sensor site due
to low cardiac index, circulatory centralization (shock),
hypothermia (e.g. during surgery), use of vasoactive drugs,
arterial occlusive diseases, mechanical pressure exercised
on measurement site, or inadequate (too low) sensor
temperature.
• Arterio-venous shunts, e.g. ductus arteriosus (PO
2
specific).
• Hyperoxemia (PaO
2
> 100 mmHg (13.3 kPa)) (PO2 specific).
• Inadequate measurement site (placement over large
superficial veins, on areas with skin edema (e.g. oedema
neonatorum), skin breakdown, and other skin anomalies).
• Improper sensor application resulting in an inadequate, not
hermetically sealed contact between the sensor surface and
the patient’s skin causing the CO
2
and O2 gases diffusing out
of the skin to intermix with ambient air.
• Exposure of the sensor to high ambient light levels (PO
2
specific).
CAUTION: Compared to the corresponding arterial blood
gases PCO
2
readings are typically too high and PO2 readings
typically too low if the measurement site is hypo-perfused.
CAUTION: The SDMS is not a blood gas device. Keep
the above mentioned limitations in mind when interpreting
PCO
2
and PO2 values displayed by the SDM.
Page 9

Page 7 . Intended Use, Principles of Operation and Limitations
When comparing PCO
2
/PO2 values displayed by the SDM with
PaCO
2
/PaO2 values obtained from arterial blood gas (ABG)
analysis, pay attention to the following points:
• Carefully draw and handle blood samples.
• Blood sampling should be performed in steady state
conditions.
• The PaCO
2
/PaO2 value obtained from ABG analysis should be
compared to the SDM’s PCO
2
/PO2 reading at the time of blood
sampling.
• In patients with functional shunts, the sensor application site
and the arterial sampling site should be on the same side of
the shunt.
• If the menu-parameter ‘Severinghaus Correction Mode’
is set to ‘Auto’, the PCO
2
values displayed by the SDM are
automatically corrected to 37 °C (regardless of the patient’s
core temperature). When performing the ABG analysis, be
sure to properly enter the patient’s core temperature into the
blood gas analyzer. Use the blood gas analyzer’s ‘37 °C-PaCO
2
’
value to compare with the SDM’s PCO
2
value.
• Verify proper operation of the blood gas analyzer. Periodically
compare the blood gas analyzer’s barometric pressure against
a known calibrated reference barometer.
Pulse Oximetry
Principles of Operations of Pulse Oximetry
The SDMS uses pulse oximetry to measure functional oxygen
saturation (SpO
2
) and pulse rate (PR). Pulse oximetry
is based on two principles: firstly, oxyhemoglobin and
deoxyhemoglobin differ in their absorption of red and infrared
light (spectrophotometry) and secondly, the volume of arterial
blood in tissue (and hence, light absorption by that blood)
changes during the pulse (plethysmography).
Pulse oximeter sensors pass red and infrared light into a
pulsating arteriolar vascular bed and measure changes in light
absorption during the pulsatile cycle. Red and infrared lowvoltage light-emitting diodes (LED) serve as light sources and
a photodiode serves as photodetector. The software of a pulse
oximeter uses the ratio of absorbed red to infrared light to
calculate SpO
2
.
Pulse oximeters use the pulsatile nature of arterial blood flow
to differentiate the oxygen saturation of hemoglobin in arterial
blood from the one in venous blood or tissue. During systole,
a new pulse of arterial blood enters the vascular bed: blood
volume and light absorption increase. During diastole, blood
volume and light absorption decrease. By focusing on the
pulsatile light signals, effects of nonpulsatile absorbers such as
tissue, bone and venous blood are eliminated.
Page 10

Note: The SDMS measures and displays functional oxygen
saturation: the amount of oxygenated hemoglobin expressed
as a percentage of the hemoglobin that can transport oxygen.
The SDMS does not measure fractional saturation: oxygenated
hemoglobin expressed as a percentage of all hemoglobin, including dysfunctional hemoglobin such as carboxyhemoglobin
or methemoglobin.
Good to know!
Oxygen saturation measurement techniques – including pulse
oximetry – are not able to detect hyperoxemia.
Due to the S-shape of the oxyhemoglobin dissociation curve
(ODC) SpO
2
alone cannot reliably detect hypoventilation in
patients being administered with supplemental oxygen.
Limitations of Pulse Oximetry
The following clinical situations or factors may limit the
correlation between functional oxygen saturation (SpO
2
) and
arterial oxygen saturation (SaO
2
) and may cause the loss of
the pulse signal:
• dysfunctional hemoglobins (COHb, MetHb)
• anemia
• intravascular dyes, such as indocyanine green or methylene
blue
• low perfusion at the measurement site (e.g. caused by inflated
blood pressure cuff, severe hypotension, vasoconstriction in
response to hypothermia, medication, or a spell of Rynaud’s
syndrome)
• venous pulsations (e.g. due to use of the forehead, cheek
or earlobe as a measurement site on a patient in steep
Trendelenburg position)
• certain cardiovascular pathologies
• skin pigmentation
• externally applied coloring agents
(e.g. nail polish, dye, pigmented cream)
• prolonged and/or excessive patient movement
• exposure of the sensor to high ambient light levels
• defibrillation
Page 11

Page 9 . Intended Use, Principles of Operation and Limitations
SenTec TC Sensors
SenTec TC Sensors provide superior performance, are robust,
reliable and require comparatively low maintenance. They
combine within a patented digital sensor design the optical
components needed for 2-wavelength, reflectance pulse
oximetry with the components needed to measure PCO
2
and –
in case of the OxiVenT™ Sensor only – PO
2
.
PO
2
(OxiVenT™ Sensor) is measured with dynamic fluorescence
quenching, an oxygen sensing technology measuring the
oxygen molecules present in the vicinity of a fluorescent dye
being immobilized in a thin carrying layer incorporated within
the sensor surface.
The PCO
2
measurement of SenTec TC Sensors (V-Sign™
Sensor 2, OxiVenT™ Sensor) is based on a Stow-Severinghaus
type PCO
2
sensor, i.e. a thin electrolyte layer is confined to
the sensor surface with a hydrophobic, CO
2
and O2 permeable
membrane. Membrane and electrolyte must be exchanged
every 28 to 42 days. With SenTec’s patented Membrane
Changer the membrane and electrolyte can be changed
with the ease of 4 identical Press-and-Turn steps in a highly
reproducible manner (p. 17).
Calibration of the PCO
2
segment of SenTec TC Sensors is
recommended every 6 to 12 hours and mandatory every 12 to
16 hours (p. 16). The PO
2
measurement of the OxiVenT™
Sensor is virtually drift free and, hence, calibration free.
Nevertheless, the SDM, as a precaution, calibrates PO
2
during
each mandatory calibration and subsequently approximately
once every 24 hours during one of the anyways ongoing PCO
2
calibrations.
To achieve local arterialization of the skin tissue at the
measurement site, SenTec TC Sensors are operated at a
constant sensor temperature of typically 41 °C in neonatal and
42 °C in adult/pediatric patients if PO
2
is disabled and – if PO2
is enabled – of typically 43 °C in neonatal and 44 °C in adult/
pediatric patients, respectively. Controls of sensor temperature
and application duration are designed to meet all applicable
standards. To guarantee safe operation, SenTec TC Sensors
reliably supervise the sensor temperature with two independent
circuits. Additionally, the SDM firmware redundantly controls
the temperature of the connected sensor.
Page 12

The SenTec Digital Monitoring System (SDMS)
The SenTec Digital Monitoring System (SDMS) comprises the
following main components:
SenTec Digital Monitor (SDM)
Note: SDMs with firmware version SMB SW-V08.00/MPB SW-
V06.00 or newer are available in a software-configuration
without activated PO
2
-option (SDM) and in a configuration with
activated PO
2
-option (SDM-PO2). The respective configuration
is indicated on the SDM’s ‘Power On Self Test’ Screen and
on the second page of the menu ‘System Information’.
Furthermore, the colored dot in the center of a SDM’s Docking
Station Door
7
is orange, if PO2 is not activated, and blue, if
PO
2
is activated.
V-Sign™ Sensor 2 (for PCO
2
, SpO2/PR monitoring) or
OxiVenT™ Sensor (for PCO
2
, PO2, SpO2/PR monitoring)
Note: Throughout this manual the notion ‘SenTec TC Sensor’
refers to SenTec sensors providing transcutaneous blood gas
measurements (i.e. to the V-Sign™ Sensor 2 and the OxiVenT™
Sensor).
Digital Sensor Adapter Cable (to connect a SenTec TC Sensor
to SDM)
Ear Clip and Multi-Site Attachment Rings (to attach SenTec
TC Sensors to patients)
Staysite™ Adhesive (to improve attachment of Multi-Site
Attachment Rings, e.g. in high humidity environments, for patients
who perspire profusely and/or in challenging patient motion
conditions).
Contact Gel (contact liquid for the application of SenTec TC
Sensors)
Service Gas (to calibrate SenTec TC Sensors)
Membrane Changer (to change membrane and electrolyte
of SenTec TC Sensors)
V-STATS™ (PC based Trend Data Download/Analysis, Remote
Monitoring, and Configuration Software for SenTec Digital
Monitors)
SDMS Quick Reference Guide and SDMS Instruction
Manual (the present document)
SDMS Manual CD (with the exception of the ‘Service and
Repair Manual for the SDMS’ all manuals and Directions for
Use being related to the SDMS are provided on the Manual CD)
Note: The components listed above do not necessarily
correspond to the scope of delivery. A complete list of available
products including disposables and accessories is provided at
www.sentec.com/products.
Page 13

Page 11 . The SenTec Digital Monitoring System (SDMS)
Additional information on SenTec TC Sensors, the Ear Clip,
the Multi-Site Attachment Rings, the Staysite™ Adhesive,
the Membrane Changer, and the Membrane Changer Inserts
is provided in the respective Directions for Use. Detailed
information on the SenTec Digital Monitor is provided in the
Technical Manual for the SDM (HB-005752). Information on
maintenance, service and repair procedures that do not require
opening the cover of the SDM as well as on maintenance and
service procedures for SenTec TC Sensors are provided in the
SDMS Service Manual (HB-005615).
To ensure proper operation of the SDMS, precisely follow the
instructions provided in this Instruction Manual step by step.
WARNING: The instructions given in the SDMS Quick
Reference Guide, the SDMS Instruction Manual, the Technical
Manual for the SDM, and on the SDMS Manual CD must be
followed in order to ensure proper instrument performance
and to avoid electrical hazards.
Note: Statements in this manual are only applicable for SDMs
with the software version indicated on the cover page.
Note: The SDMS Quick Reference Guide, the SDMS
Instruction Manual and various other manuals are
available for online viewing at www.sentec.com/ifu.
Note: SDMS related tutorials are available for online
viewing at www.sentec.com/tv.
Page 14
Setting up the SDMS
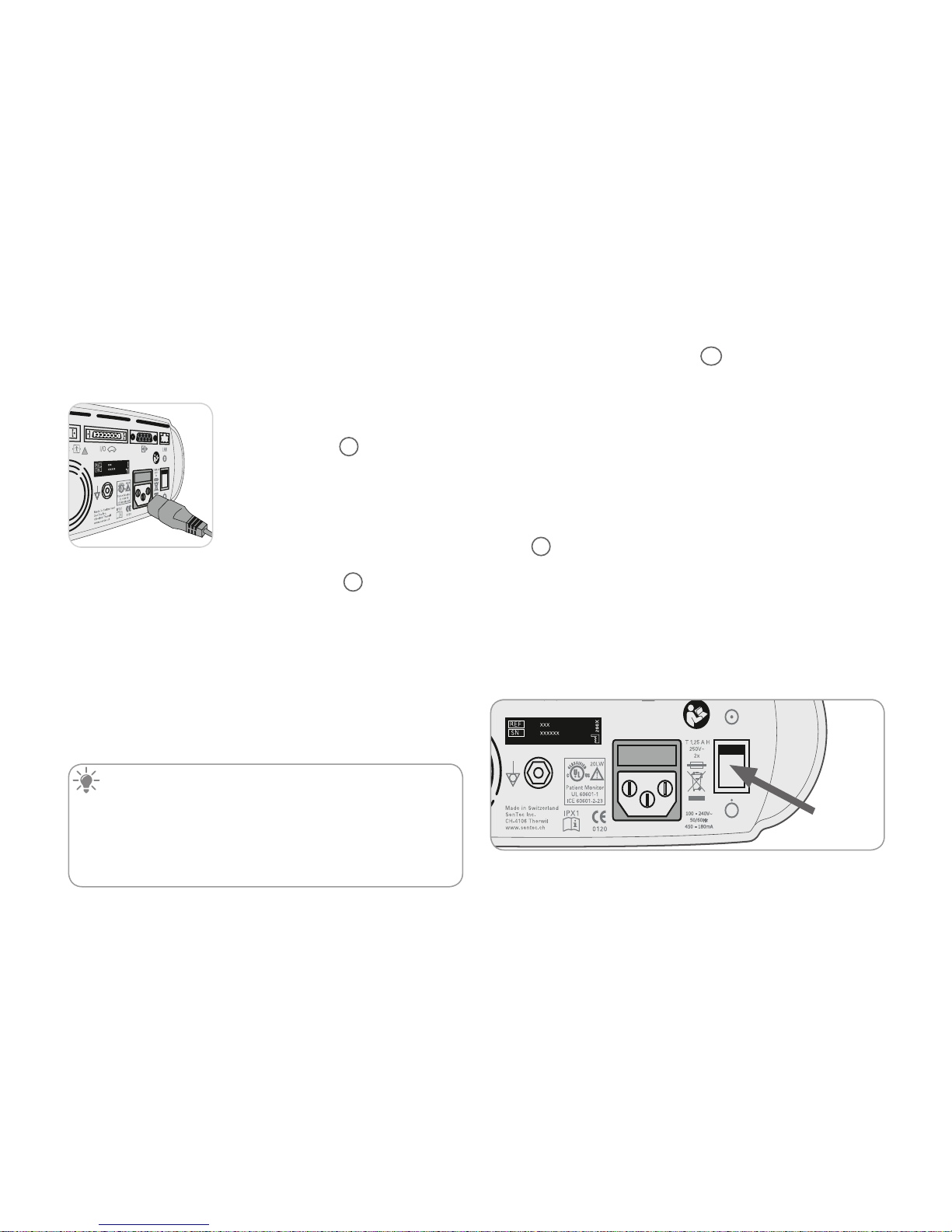
Connect SDM to AC Power
Plug the female connector of the power
cord into the AC power connector on the
rear of the monitor
23
.
Plug the male connector of the power
cord into a properly grounded AC
power outlet.
Note: The SDM will automatically
adapt to the applicable local voltage:
100 - 240V~ (50/60Hz).
Verify that the AC power/battery indicator
10
is lit. If the AC
power/battery indicator is not lit, check the power cord, fuses,
and the AC power outlet.
Battery Operation of the SDM
The SDM is equipped with a rechargeable internal Li-Ion
battery that can be used to power the monitor during transport
or when AC power is not available. The Status Icon ‘Battery’
(p. 48) indicates the remaining battery charge (%).
Good to know!
When using an SDM with a LED backlight display, a new, fully
charged battery will provide up to 10 hours of monitoring
time if Sleep Mode=OFF or Auto, and up to 12 hours of
monitoring time if Sleep Mode=ON. It takes approximately
7 hours to fully charge a drained battery.
The AC Power/Battery Indicator 10 provides information on
the charging status of the battery:
Green: SDM connected to AC power, battery fully charged
Yellow: SDM connected to AC power, battery charging
LED OFF: SDM not connected to AC power (i.e. powered by
internal battery)
Turning on the SDM
Turn on the SDM by pushing the ON/OFF Switch on the rear
panel
24
. The SDM will automatically perform a ‘Power On
Self Test’ (POST). Check the date/time settings of the SDM and
adjust if necessary.
Note: If the POST fails, discontinue use of the SDM and contact
qualified service personnel or your local SenTec representative.
Refer to the Technical Manual for the SDM (HB-005752) for a
detailed description of the POST.
ON/OFF
switch
Page 15

Page 13 . Setting up the SDMS
Installation of the Gas Bottle
(Service Gas-0812)
The gas bottle slot is located on the rear of the SDM 19.
Remove the old gas bottle by turning
it counter-clockwise.
Insert the new gas bottle by turning
it clockwise approx. 4.5 turns and
thoroughly tighten it (without applying
undue force).
CAUTION: Failure to properly insert the gas bottle
may result in incorrect sensor calibrations and may cause
increased gas consumption.
The Status Icon ‘Gas’ (p. 48) indicates the remaining capacity
of the gas bottle in %. It is only displayed if a SenTec TC
Sensor is connected to the SDM and is in the Docking Station.
WARNING: The Service Gas bottle is a pressurized
container. Protect from sunlight and do not expose to
temperatures exceeding 50 °C (122 °F). Do not pierce or
burn, even after use. Do not spray on a naked flame or any
incandescent material.
WARNING: Do not use expired gas bottles or gas
bottles from manufacturers other than SenTec. The use of
non-SenTec gas bottles may damage the Docking Station.
Improper calibration gas mixtures will result in incorrect
sensor calibrations and subsequently result in inaccurate
PCO
2
and/or PO2 data.
Dispose of empty gas bottles according to local waste disposal
regulations for aluminium containers.
Connection/Disconnection of Digital
Sensor Adapter Cable
Connect the Digital Sensor Adapter Cable to the SDM. The connection is properly established when both clamps of the plug
snap into place in the sensor connection port
15
.
Disconnect the cable from the SDM
by pressing the two latches on the
black plug to release the clamps (see
picture) and pull to remove the cable.
Press
Page 16
Connection of a SenTec TC Sensor
Take a SenTec TC Sensor (V-Sign™ Sensor 2 or OxiVenT™
Sensor).
Important: For PO
2
monitoring you must use an OxiVenT™
Sensor and an SDM with activated PO
2
-option.
Check the condition of the sensor membrane and the integrity
of the sensor (p. 15). Change the membrane if necessary
(p. 17). Do not use the sensor if any problems are noted.
Once sensor check/inspection of its membrane are completed
successfully, connect the SenTec TC Sensor to the Digital
Sensor Adapter Cable.
Thereafter, the SDM usually will display the message ‘Calibrate
sensor’ (for exceptions see description of the feature SMART
CALMEM, p. 17).
Insert the sensor into the Docking Station for sensor calibration
(p. 16).
If the sensor’s ‘Membrane Change Interval’ has elapsed
(this usually applies to new sensors), the SDM will trigger
the message ‘Change sensor membrane’ upon insertion of
the sensor into the Docking Station. In this case, you must
change the sensor membrane (p. 17) before the SDM starts
calibrating the sensor.
Note: If you have changed the sensor membrane just before
connecting the sensor to the SDM, it won’t be necessary
to change it once again. In this case, simply confirm the
membrane change on the monitor (menu ‘Membrane Change’ only accessible if the sensor is outside the Docking Station).
Page 17

Checking a SenTec TC Sensor
Check the condition of the sensor membrane and the integrity
of the sensor before and after each use and after changing the
membrane (p. 17)!
Ensure that the sensor is clean before visually checking it. If
necessary, carefully wipe off any residue from the sensor’s
surface (including membrane, housing and cable) with 70%
isopropanol or another approved cleaning agent (refer to
sensor’s Directions for Use).
a) Change the sensor membrane if it is damaged or missing,
has a loose fit, or if there is trapped air or dry electrolyte under
the membrane.
Page 15 . Sensor Check, Sensor Calibration/Storage and Membrane Change
CAUTION: Do not touch the delicate optical/glass
components embedded in the sensor’s surface should the
membrane be missing.
b) Do not use the sensor if there is any visible damage to
the sensor housing or cable, if the color of the ring around the
glass electrode has a metallic luster (should be brown), or if the
sensor’s red LED does not light when the sensor is connected
to the SDM. Instead, contact qualified service personnel or
your local SenTec representative regarding continued use or
replacement of the sensor.
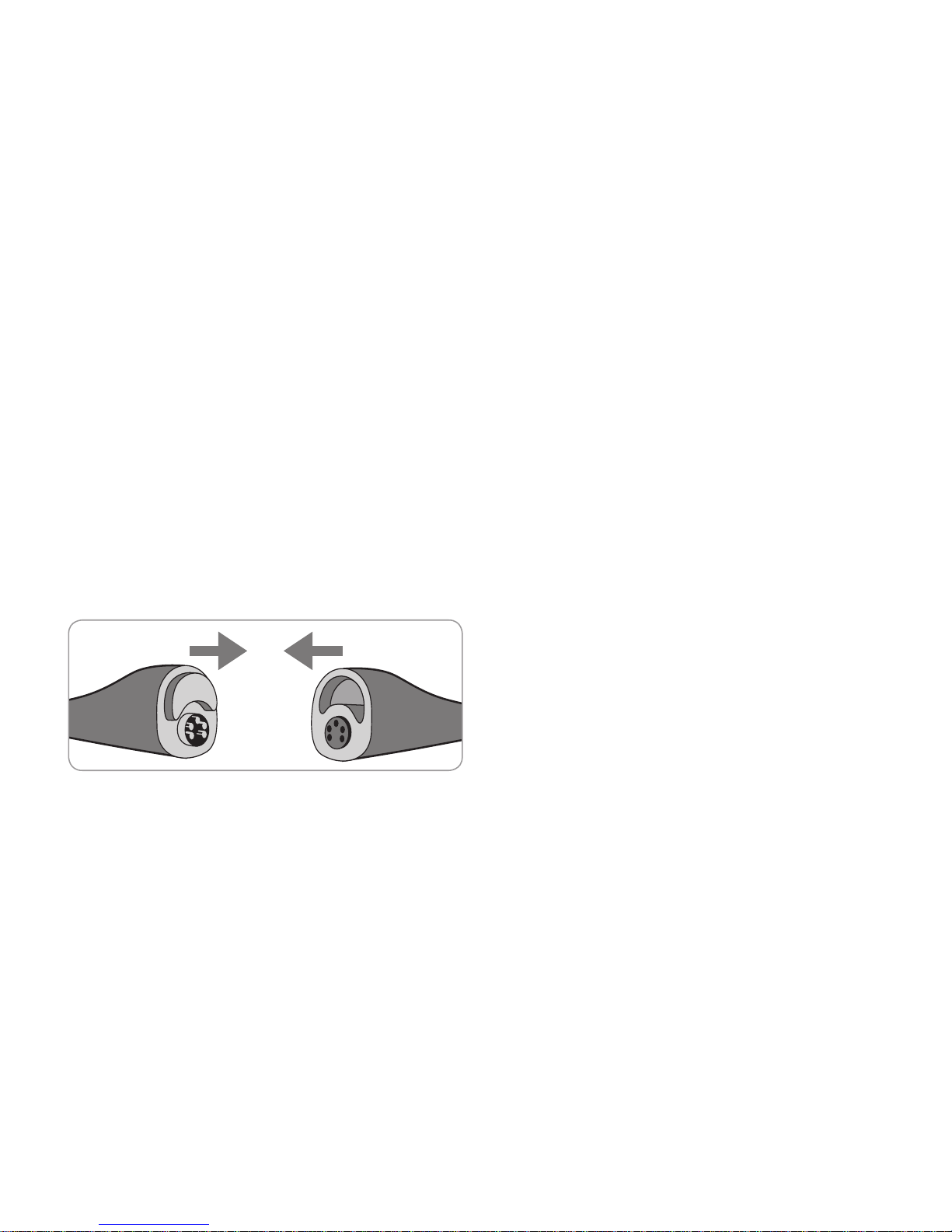
c) When operating with an OxiVenT™
Sensor, do not use the sensor if
the off-centered, white, round spot
on the sensor surface is missing
or is not illuminated in green-cyan
color when the OxiVenT™ Sensor is
connected to the SDM with enabled
PO
2
measurement function.
Sensor Check, Sensor Calibration/Storage and Membrane
Change
Page 18
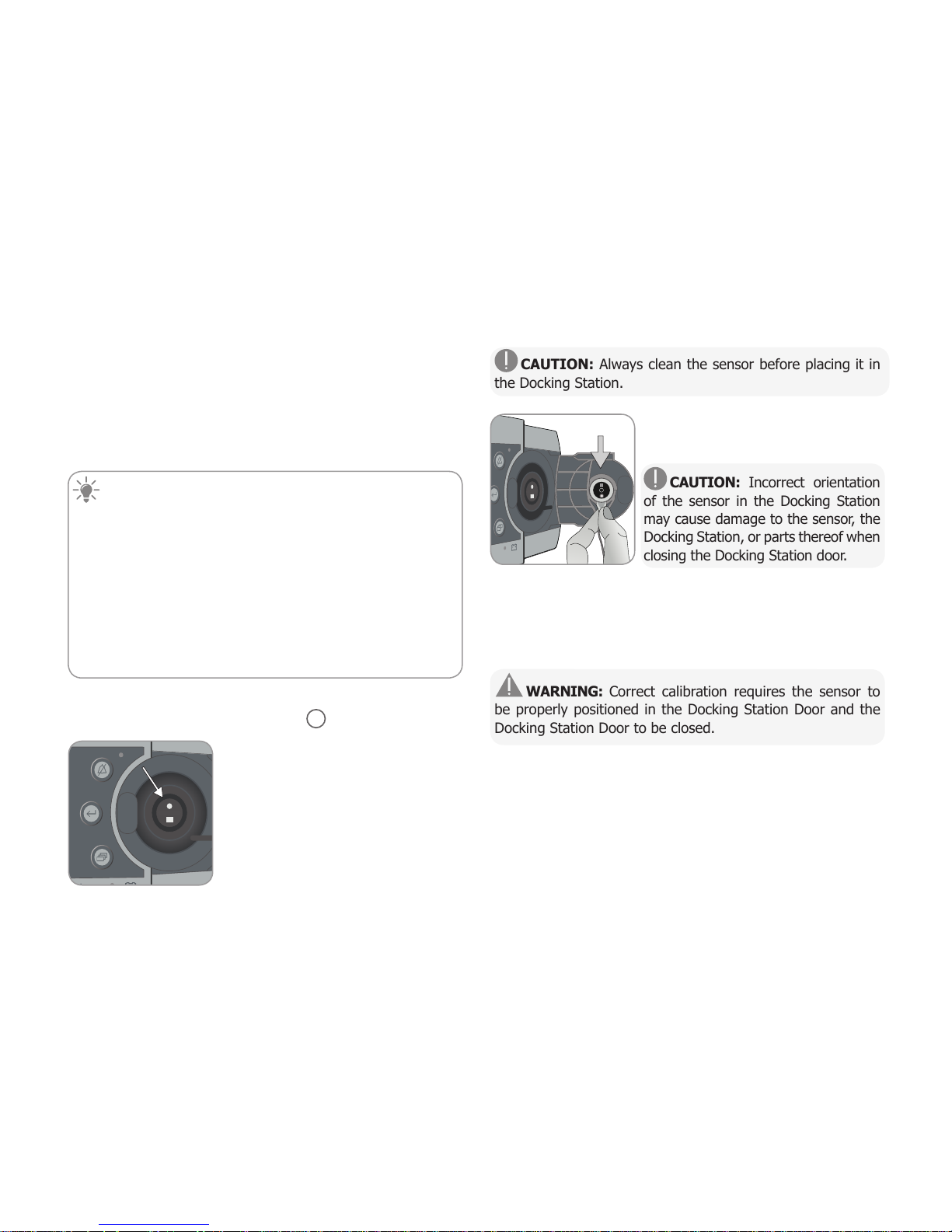
CAUTION: Always clean the sensor before placing it in
the Docking Station.
3. Hang the sensor into the holder in
the inside of the door. Ensure that the
sensor’s red light is visible.
CAUTION: Incorrect orientation
of the sensor in the Docking Station
may cause damage to the sensor, the
Docking Station, or parts thereof when
closing the Docking Station door.
4. Close the Docking Station Door. The SDM will check the
sensor and – if necessary – start the sensor calibration
(message ‘Calibration in progress’). The message ‘Ready for
use’ will display once calibration is finished.
WARNING: Correct calibration requires the sensor to
be properly positioned in the Docking Station Door and the
Docking Station Door to be closed.
Note: If the sensor is stored in the Docking Station, additional
sensor calibrations can be activated via a ‘Quick Access Menu’
(p. 42). If enabled, PO
2
is also calibrated during calibrations
that are activated with the menu-function ‘Calibrate sensor’.
Sensor Calibration and Storage
If a sensor calibration is mandatory, the SDM displays the
message ‘Calibrate sensor’, a low priority alarm sounds and
PCO
2
and PO2 are marked as ‘invalid’ (values replaced by ‘---’).
Good to know!
‘Calibration Intervals’ for SenTec TC Sensors can last up to
12 hours. Once the ‘Calibration Interval’ has elapsed, sensor
calibration is recommended (message ‘Sensor calibration
recommended’) and monitoring is possible for another 4
to 6 hours with PCO
2
marked as ‘questionable’ (p. 32).
Thereafter, sensor calibration is mandatory.
The SDM, as a precaution, calibrates PO
2
during each
mandatory calibration and subsequently approximately once
every 24 hours during one of the default PCO
2
calibrations.
To calibrate the sensor:
1. Open the Docking Station Door
7
by pulling the door
handle.
2. Check the gasket (arrow) in the
Docking Station. If necessary, clean
the Docking Station and gasket by
using a cotton swab moistened with
70% isopropanol (for other approved
cleaning agents refer to the Technical
Manual for the SDM).
Page 19

Page 17 . Sensor Check, Sensor Calibration/Storage and Membrane Change
Note: After switching on the SDM or after a membrane
change (p. 17), it is recommended to store the sensor
in the Docking Station at least for the duration indicated
by the yellow information message ‘Recommended Sensor
Stabilization [min]:’ on the ‘Ready for use’ screen and on the
‘Calibration’ screen.
Note: To maintain monitor readiness in-between monitoring,
always keep the monitor switched on and always store the
sensor in the Docking Station.
Good to know!
SMART CALMEM is a feature of SenTec TC Sensors permitting disconnection of the sensor from the SDM for up to
30 minutes without losing the calibration status. Thus,
monitoring can temporarily be interrupted without the need
to remove the sensor from the patient, e.g. to untangle
cables, to turn or move the patient, or if the patient needs
to go to the restroom. Furthermore, SMART CALMEM
reduces the number of required calibrations and, hence, the
consumption of calibration gas.
Changing the Sensor Membrane
The membrane of a SenTec TC Sensor must be changed if the
‘Membrane Change Interval’ has elapsed. In this case, the SDM
displays the message ‘Change sensor membrane’, triggers a
low priority alarm, marks PCO
2
/PO2 as invalid and activates
the menu ‘Membrane Change’ - provided the sensor is in the
Docking Station.
Good to know!
The ‘Membrane Change Interval’ is set to 28 days by
default. Depending on the specific requirements of various
clinical settings, the interval can be customized ranging from
1 to 42 days.
CAUTION: Without being requested by the SDM, the
sensor membrane must additionally be changed if any of the
conditions described in the section ‘Checking a SenTec TC
Sensor’ (p. 15) apply.
CAUTION: Use Membrane Changers with a green center
dot only for V-Sign™ Sensors. Membrane Changers with a
blue center dot can be used for all SenTec TC Sensors.
CAUTION: The Contact Gel is not needed in any of the
membrane change steps. The Contact Gel is only used for
sensor application.
Page 20

i
s
o
p
r
o
p
a
n
o
l
7
0
%
1
Note: A Membrane Change Tutorial is available for
online viewing at www.sentec.com/tv/v0.
Note: The Membrane Changer can be reused
by replacing its insert. To prepare the Membrane
Changer for reuse, refer to the Directions for Use
of the Membrane Changer Inserts or see tutorial at
www.sentec.com/tv/v1.
Inserting Sensor into Membrane Changer
1. Verify that the sensor is clean before
changing its membrane. If necessary,
carefully wipe off any residue from
the sensor’s surface (including
membrane, housing and cable) with
70% isopropanol (for other approved
cleaning agents refer to the sensor’s
Directions for Use).
2. Place the Membrane Changer on
a horizontal, dry surface with the
colored dot facing up.
3. Insert the sensor into the Membrane
Changer with the sensor side facing up.
The insert receiver
1
is designed so
that improper alignment of the sensor
is difficult if not impossible.
Note: Neither touch nor hold the sensor cable while the sensor
is inside in the Membrane Changer nor pick up the Membrane
Changer as this may lead to dislodging the sensor from the
Membrane Changer.
Four Press-and-Turn Steps
to Change the Membrane
The membrane change procedure consists of four identical
press-and-turn steps. To provide better guidance, these steps
are marked with the corresponding numbers on the Membrane
Changer.
Step 1 removes the old sensor membrane: Press down slowly
but firmly with palm of hand and hold for 3 seconds. Release
the top Carry out a visual check to ensure that the membrane
is removed. Turn the top portion one click clockwise to the next
step. Keep the Membrane Changer horizontal.
Step 2 cleans the sensor surface from old electrolyte: As in
step 1, press the membrane changer slowly but firmly, release
the top and turn clockwise to the next step.
Step 3 applies new electrolyte on the sensor surface: Press
the membrane changer slowly but firmly for 3 seconds, release
the top and turn clockwise to the next step.
Step 4 places a new membrane on the sensor: Press the
membrane changer top down slowly but firmly for 3 seconds,
release the top and turn clockwise to the √ symbol.
Page 21

1x
1x
1
1
1
Page 19 . Sensor Check, Sensor Calibration/Storage and Membrane Change
Keep the Membrane Changer horizontal while executing the
following Press-and-Turn step 4 times:
a. Press down slowly but
firmly with palm of the hand
and hold for 3 seconds.
b. Turn the top portion one
click clockwise to the next
stop. Keep the Membrane
Changer horizontal! Hold the
changer’s bottom half in place
while turning the top half.
Note: Do not press down on
the top while turning!
1x press
3 sec.
1
1
1
1
Removing Sensor from Membrane Changer
Press once again or lift the sensor to
release and remove the sensor from
the Membrane Changer.
Inspecting Sensor Membrane
Check the condition of the sensor membrane and the integrity
of the sensor (p. 15). Repeat the membrane change if necessary. Do not use the sensor if any problems are noted.
Confirming Membrane Change on SDM
Once the inspection of the sensor membrane is completed
successfully, confirm the membrane change on the monitor
(menu ‘Membrane Change’).
Note: The membrane timer only resets if you confirm the
membrane change on the monitor.
Note: The menu ‘Membrane Change’ is only accessible if the
Docking Station Door is open.
Page 22

Refer to the pictures below to select the patient type on the SDM, the measurement site and the sensor attachment accessory.
Refer to the following page for additional (important) information.
Patient Monitoring with the SDMS
Selection of Patient Type, Measurement Site, and Sensor Attachment Accessory
‘Adult’ if Older than Term Birth + 1 Month
Earlobe: Use Ear Clip for mature, intact skin.
All other sites: Use MAR/e-MI for mature, intact skin or MAR/e-SF for sensitive, fragile skin.
Selection of Sensor Attachment Accessory
: PCO2 : PCO2/SpO2/PR
‘Neonatal’ if Younger than Term Birth + 1 Month
: PCO2/PO2 : application area
application area
Page 23

Page 21 . Patient Monitoring with the SDMS
Note: For PO
2
monitoring, an OxiVenT™ Sensor and an
SDM with activated PO
2
-option is needed. The respective
configuration is indicated on the SDM’s ‘Power On Self
Test’ Screen and on the second page of the menu ‘System
Information’. Furthermore, the colored dot in the center of a
SDM’s Docking Station Door
7
is orange if PO2 is not activated
and blue if PO
2
is activated.
CAUTION: Choose a flat, well-perfused area of intact skin
(centrally located sites are preferable) for sensor attachment.
Avoid placement over large superficial veins or areas of skin
breakdown or edema.
CAUTION: A good, hermetically sealed contact between
the sensor and the skin is essential for TC monitoring!
Note: To attach a SenTec TC Sensor with the Ear Clip (p. 27),
the earlobe should be large enough to cover the entire
sensor membrane (dark surface of the sensor). Furthermore,
application of a SenTec TC Sensor on pierced earlobes may
result in incorrect PCO
2
/PO2 measurements. If the earlobe is
too small or has multiple piercings, consider using a Multi-Site
Attachment Ring (model MAR/e-MI or model MAR/e-SF) to
attach the sensor to an alternate site (p. 24).
Note: If more secure sensor attachment is required, e.g. in
high humidity environments, for patients who perspire profusely
and/or in challenging patient motion conditions, the Staysite™
Adhesive (model SA-MAR) can be used complementary with
the Multi-Site Attachment Rings. Please refer to the Directions
for Use for the Staysite™ Adhesive.
WARNING: The measurement of SpO2 and PR with
SenTec TC Sensors is only defined on sites specified in the
pictures above. In order to avoid erroneous readings and false
alarms of SpO
2
and PR, ensure that the appropriate patient
type (Adult) is selected. Ensure to disable the parameters
SpO
2
/PR for sensor application on other measurement sites.
WARNING: It is not recommended to use sensor
attachment accessories on patients who exhibit allergic
reactions to adhesive tapes. It is not recommended to use
the Contact Gel on patients who exhibit allergic reactions.
WARNING: To prevent skin burns, change the sensor
site at least every 4 hours for sensor temperatures higher
than 43 °C on neonates or higher than 44 °C on adult/pediatric
patients.
Page 24

Check SDM Settings and
System Readiness
Before initiating patient monitoring, ensure the current SDM
Settings/SDM Profile are appropriate for the patient, for the selected measurement site (p. 20), for the skin condition/skin
tissue perfusion at the selected measurement site and for the
specific clinical setting. At least check the patient type and the
enabled parameters as well as sensor temperature, ‘Site Time’
and alarm specific settings. Change SDM Settings/SDM Profile
if necessary. Furthermore, verify system readiness (message
‘Ready for use’) and check the ‘Available Monitoring Time’.
Note: If the connected sensor is in the Docking Station, the
‘Ready for use’ or ‘Calibration’ screen (summarizing important
system information (see below)) displays.
‘Ready for use’/‘Calibration’ screen
If the connected sensor is in the Docking Station ‘Ready for
use’ or ‘Calibration in progress’ displays in yellow big font in the
center of the ‘Ready for use’/‘Calibration’ screen.
1
3
2
4
5
6
7
Note: Pressing the Enter Button (p. 42) while the ‘Ready
for use’ screen displays activates a ‘Quick Access Menu’ with
the possibility to activate additional calibrations (p. 16), to
access the sub-menu ‘Profiles’, or to activate the V-Check™
Mode (p. 35).
The following information is displayed in the upper area of
the ‘Ready for use’/‘Calibration’ screen:
1
Patient Type Indicator (yellow): Displays the current
patient type (Neonatal or Adult).
2
Patient Info (orange): During remote monitoring using
V-CareNeT™ (if enabled), the ‘Patient Info’ (patient name,
patient number or a comment) displayed in the corresponding
station’s ‘Remote Monitoring Window’ is duplicated on the
SDM.
Note: The ‘Patient Info’ is also duplicated in the SDM’s main
menu and – if no status message has to be displayed – in the
SDM’s status bar enclosed in ‘[ ]’.
3
Sensor Type Indicator: Displays the model/type of the
currently connected sensor.
4
Current SDM Profile indicator: Indicates the name
of the currently selected ‘Standard Profile’ (e.g. ‘SLEEP’). An
asterisk (*) next to the profile name (e.g. ‘SLEEP*’) indicates
that at least one setting of the selected ‘Standard Profile’ is
modified (only displayed when SDM is in ‘Institutional Mode’).
Page 25

Page 23 . Patient Monitoring with the SDMS
SP OFF
(or ON and T≤ 41.0 °C in
adults/T ≤ 40.0 °C in neonates)
SP ON
(if T > 41.0 °C in adults/
T > 40.0 °C in neonates)
IH OFF
(or *)
IH ON
(if **)
Note: In ‘Institutional Mode’ it is possible – by using
V-STATS™ – to store up to 4 SDM Profiles on the SDM and select
one of these profiles as ‘Standard Profile’. During subsequent
use, the operator can restore the selected ‘Standard Profile’ (if
modified) or select a different ‘Standard Profile’ in the menu
‘Profiles’. Furthermore, if at power-up of the SDM the LAST
settings differ from those of the selected ‘Standard Profile’,
this menu activates and offers the option to keep the modified
settings, to restore the selected ‘Standard Profile’ or to select
another ‘Standard Profile’.
Good to know!
Various profiles preconfigured by SenTec and tailored to
optimally fit the specific needs of varying clinical settings are
available within V-STATS™.
5
Sensor Temperature: Displays the currently selected
sensor temperature (this indicator is only displayed if the
connected sensor is heated).
WARNING: The use of temperatures higher than 41 °C
requires special attention to patients with susceptible skin,
e.g. neonates, geriatric patients, burn victims, patients with
skin diseases.
6
Special Temperature Settings: Split-arrow indicating
the current configuration of INITIAL HEATING (IH, left part of
arrow) and SITE PROTECTION (SP, right part of arrow).
* ON and T = 44.5 °C in adults/T ≥ 43.5 °C in neonates
** T < 44.5 °C in adults/< 43.5 °C in neonates
7
V-Check™ Mode Indicator: If the V-Check™ Mode
(p. 35) is ON the ‘V-Check™ Mode Indicator’ displays on the
left of the ‘Sensor Temperature Indicator’
5
and the ‘Special
Temperature Settings Indicator’
6
.
The following information is displayed in the center of the
screen:
Enabled Parameters: Indicates the parameters that are
currently enabled. Ensure to select an option that is approved
for the patient’s age and the intended measurement site
(p. 20, 21).
Note: The selectable options depend on the sensor type, the
SDM’s PO
2
activation status, and the selected patient type.
Page 26

Available Monitoring Time [hrs]: Indicates the time
available for patient monitoring, i.e. the time interval after
removing the sensor from the Docking Station or applying
the sensor to the patient until the selected ‘Site Time’ or - if
PCO
2
is enabled - the ‘Calibration Interval’ (p. 16) will elapse
(whichever occurs first).
Membrane Change is due in [days]: Indicates the number
of days left until the next membrane change (p. 17) is
mandatory (only if PCO
2
is enabled).
Recommended Sensor Stabilization [mins]: Indicates
the recommended sensor stabilization duration in minutes.
Only displayed if sensor stabilization is recommended and if
the display of this message is enabled.
Status Bar: If the ‘Ready for use’ screen displays, temporary
display of the ‘Status Bar’ (p. 48) can be activated by
pressing any of the control-buttons (p. 42). The ‘Status
Bar’ also displays during an ongoing sensor calibration or if an
alarm condition occurs.
Note: If the SDM is in Sleep Mode, the display is inactive
(black). Press any of the control buttons (p. 42) to activate
the display.
Sensor Application Using a Multi-Site
Attachment Ring/Easy
According to the procedure described point by point below,
a Multi-Site Attachment Ring (MAR) or Multi-Site Attachment
Ring Easy (MARe) is first attached to the measurement site,
one small drop of contact liquid is then applied to the center
of the sensor and finally the sensor is snapped into the ring.
Alternatively, you may also click the sensor into the ring first,
remove the protective liner of the adhesive tape, and then
apply one small drop of contact liquid on the center of the
sensor. In this case ensure to keep the sensor/ring assembly
such that the contact liquid does not run off the sensor face
and flip-over the sensor/ring assembly just before attaching it
to the skin.
WARNING: Application of any pressure to the
measurement site (e.g. by using a pressure bandage) may
cause pressure ischemia at the measurement site and,
consequently, inaccurate measurements, necrosis or – in
combination with heated sensors – burns.
1. Check current SDM Settings/SDM Profile and verify system
readiness (message ‘Ready for use’, p. 22). Change SDM
Settings/SDM Profile if necessary.
2. Clean the site with a swab wetted with 70% isopropanol
(or according to your institution’s skin cleaning/degreasing
procedures) and let it dry. If necessary, remove hair.
Page 27

Page 25 . Patient Monitoring with the SDMS
3. Take a Multi-Site Attachment Ring/Easy out of the package
and pull off the liner protecting the adhesive tape of the ring.
CAUTION: The Multi-Site Attachment Rings (models
MAR-MI, MAR-SF, MARe-MI and MARe-SF) are for single-
use. Neither reattach used rings on the same nor on another
patient!
4. Attach the ring to the
measurement site. Verify that
the skin under the adhesive
is not wrinkled. Then press
gently on the retainer ring and
move your finger around the
ring circumference to ensure
a good adhesion of the ring’s
adhesive to the skin.
5. Open the Docking Station Door and
remove the sensor.
Note: Always grab the sensor at its
neck to avoid pulling and tearing the
sensor cable.
6. Close the Docking Station Door.
7. Check the condition of the sensor membrane and the integrity
of the sensor (p. 15). Change the membrane if necessary
(p. 17). Do not use the sensor if any problems are noted.
8. Apply one small drop of contact
liquid to the center of the sensor
surface. Ensure to keep the sensor
horizontal (membrane pointing
upwards) so that the contact liquid
does not run off the membrane. Flip
over the sensor just before inserting it
into the ring.
Note: As contact liquid, you may use SenTec’s Contact Gel,
clean tap water, sterile water or sterile saline solution.
Note: Alternatively, you can apply one small drop of contact
liquid to the skin area in the center of the attachment ring.
You may also use a cotton swab (Q-tip) to apply the contact
liquid.
Note: Avoid wetting the adhesive tape!
Note: As long the sensor is not yet applied to the patient, try
to keep the measurement site as horizontal as possible so that
the contact liquid does not run off the measurement site.
WARNING: Do not swallow Contact Gel. Keep away
from children. Avoid contact with eyes and injured skin. Do
not use on patients who exhibit allergic reactions. Use only
approved SenTec Contact Gel, clean tap water, sterile water
or sterile saline solution.
Page 28

b
9. Holding the sensor at its neck,
approach the MAR from the flap side
(a) or the MARe from any side (b) and
first insert the nose of the sensor into
the retainer ring. Then apply slight
downward pressure on its neck. The
spring tension of the retainer ring will
pull the sensor into place with little to
no pressure on the skin. Rotate the
sensor in the ring and press the sensor
gently against the skin to spread the
contact liquid.
Note: Check that the sensor can be
easily rotated to ensure it is snapped
in correctly.
10. Check sensor application! Ensure that air gaps are
eliminated between the skin and the sensor.
Note: A good, hermetically sealed contact between the sensor
and the skin is essential for TC monitoring!
WARNING: Ensure the sensor is applied correctly.
Incorrect application of the sensor can cause incorrect
measurements.
11. Twist the sensor into the best position. For forehead/
cheek placement wrap the sensor cable once around the ear
and tape the cable to the cheek or another applicable site. For
other application sites, tape the cable to the skin at a distance
of 5 to 10 cm from the sensor head. Route the sensor cable
properly to avoid entanglement
or strangulation and secure
it with a Clothing Clip to an
appropriate site of the patient’s
clothing or bed linen. Ensure
that the sensor cable is loose
enough for not to be stretched
during monitoring. Gently press
on the sensor as a final application check.
12. Verify that the SDM detects that the sensor was placed
on the patient, initiates monitoring and that the enabled
parameters stabilize. If necessary, readjust sensor application
or reposition the sensor.
Note: Typically, PCO
2
increases and PO2 (if enabled) decreases
to reach a stabilized value within 2 to 10 minutes (p. 30).
SpO
2
and PR usually stabilize within a few seconds.
Note: If more secure sensor attachment is required, e.g.
in high humidity environments, for patients who perspire
profusely and/or in challenging patient motion conditions, the
Staysite™ Adhesive (model SA-MAR) can complementary be
used in addition to the Multi-Site Attachment Rings. Please
refer to the Directions for Use for the Staysite™ Adhesive.
Page 29

I
s
o
p
r
o
p
a
n
o
l
7
0
%
squeeze
gently
Page 27 . Patient Monitoring with the SDMS
Sensor Application Using an Ear Clip
According to the procedure described point by point below, the
Ear Clip is first attached to the earlobe, then one small drop
of contact liquid is applied to the sensor surface, and, finally,
the sensor is snapped into the Ear Clip attached to the earlobe.
Alternatively, you may click the sensor into the clip’s retainer
ring first, apply one small drop of contact liquid to the center
of the sensor, pull off both liners protecting the clip’s adhesive
tapes, and then apply the sensor/clip assembly to the earlobe.
In this case, ensure to keep the clips jaws open and to hold
the sensor/clip assembly such that the contact liquid does not
run off the sensor face until the sensor/clip assembly is applied
to the earlobe.
WARNING: Application of any pressure to the
measurement site (e.g. by using a pressure bandage) may
cause pressure ischemia at the measurement site and,
consequently, inaccurate measurements, necrosis or – in
combination with heated sensors – burns.
1. Check current SDM Settings/SDM Profile and verify system
readiness (message ‘Ready for use’, p. 22). Change SDM
Settings/SDM Profile if necessary.
2. Clean the earlobe with a swab wetted
with 70% isopropanol (or according
to your institution’s skin cleaning/
degreasing procedures) and let it dry. If
necessary remove hair.
3. Take an Ear Clip out of the package,
open the clip jaws and pull off both
liners protecting the adhesive tapes of
the clip.
CAUTION: The SenTec Ear Clip (model EC-MI) is for
single-use. Neither reattach used clips on the same nor on
another patient!
4. Pull the earlobe to stretch its skin and
then attach the Ear Clip with its retainer
ring on the backside of the earlobe.
Verify that the skin under the retainer
ring’s adhesive is not wrinkled and that
the hole in the center of the retainer
ring completely covers the skin.
Then squeeze gently to ensure that
both adhesive tapes stick firmly to the
earlobe.
Page 30

WARNING: Do not swallow Contact Gel. Keep away
from children. Avoid contact with eyes and injured skin. Do
not use on patients who exhibit allergic reactions. Use only
approved SenTec Contact Gel, clean tap water, sterile water
or sterile saline solution.
9. Pull the earlobe with the Ear Clip in
horizontal position. Move the sensor
horizontally into place with the cable
preferably pointing to the crown of the
head. Insert the sensor into the clip’s
retainer ring by gently pressing it until
it snaps into the clip.
Note: Check that the sensor can be
easily rotated to ensure it is snapped
in correctly.
10. Check sensor application! The
sensor is applied correctly if its entire
dark surface is covered by the earlobe.
Ensure that air gaps are eliminated
between the skin and the sensor.
5. Open the Docking Station Door and
remove the sensor.
Note: Always grab the sensor at its
neck to avoid pulling and tearing the
sensor cable.
6. Close the Docking Station Door.
7. Check the condition of the sensor membrane and the integrity
of the sensor (p. 15). Change the membrane if necessary
(p. 17). Do not use the sensor if any problems are noted.
8. Take the sensor and apply one small
drop of contact liquid to the middle of
the sensor surface.
Note: Until the sensor is applied to the
earlobe, ensure to hold the sensor such
that the contact liquid does not run
off the sensor face. Avoid wetting the
adhesive tapes!
Note: Alternatively you may apply one small drop of contact
liquid to the visible skin area in the center of the Ear Clips
tainer ring or use a cotton swab (Q-tip) to apply the contact
liquid.
Page 31

Page 29 . Patient Monitoring with the SDMS
CAUTION: A good, hermetically sealed contact between
the sensor and the skin is essential for TC monitoring!
WARNING: Ensure the sensor is applied correctly.
Incorrect application of the sensor can cause incorrect
measurements.
11. Wrap the sensor cable around
the ear once and tape the cable to
the cheek as shown in the picture.
Route the sensor cable properly to
avoid entanglement or strangulation
and secure it with a Clothing Clip to
an appropriate site of the patient’s
clothing or bed linen. Ensure that the
sensor cable is loose enough for not to be stretched during
monitoring. Gently squeeze the sensor and Ear Clip as a final
application check.
12. Verify that the SDM detects that the sensor was placed
on the patient, initiates monitoring and that the enabled
parameters stabilize. If necessary, readjust sensor application
or reposition the sensor.
Note: Typically, PCO
2
increases and PO2 (if enabled) decreases
to reach a stabilized value within 2 to 10 minutes (p. 30).
SpO
2
and PR usually stabilize within a few seconds.
Patient Monitoring
‘Sensor-On-Patient’ Detection
Once the sensor is correctly applied to the patient (see previous sections), the SDM usually detects that the sensor was
put on the patient and initiates monitoring for the enabled
parameters. If the sensor is applied on a site approved for
SpO
2
/PR monitoring (p. 20), ‘Sensor-On-Patient’ is typical-
ly detected within a few seconds, otherwise within less than
2 minutes.
When obtaining an adequate patient signal is difficult, it may
be possible that the SDM is unable to automatically detect
‘Sensor-On-Patient’. If in this case PCO
2
is enabled, you may
use the ‘Start Monitoring’ function in the ‘Quick Access Menu’
(p. 42) to activate the ‘Enforced Sensor-On-Patient Mode’
bypassing normal ‘Sensor-On-Patient’ detection. To reset the
SDM to ‘Normal Sensor-On-Patient Mode’ simply insert the
sensor into the Docking Station.
Note: If the ‘Enforced Sensor-On-Patient Mode’ is active, the
SDM’s ‘Sensor-Off-Patient’ detection is disabled, i.e. in this case
no ‘Sensor off patient (8 )’ alarm will be triggered. There will
be a ‘Check Application’ Alarm instead, triggered within two
minutes, if the sensor is dislodged or intentionally removed
from the patient. If SpO
2
/PR are enabled, SDM’s algorithms
typically will flag the PCO
2
and PO2 readings to be unstable
(displayed in grey) and the SpO
2
and PR readings to be invalid
(respective values replaced by ‘---’) within 15 seconds and within
30 seconds the low priority alarm ‘SpO
2
signal quality’ will sound.
Page 32

If the penetration of ambient air is of short duration only,
TC-readings will typically restabilize within a few minutes.
After sensor application or occurrence of a ‘TC-Artifact’, the
SDM displays the message ‘PCO
2
/PO2 stabilizing’ if both TC-
parameters are stabilizing or ‘PCO
2
stabilizing’ or ‘PO2 stabilizing’,
respectively, if only one TC parameter is stabilizing. To indicate
that TC readings during stabilization do not reflect the patient’s
real PCO
2
and/or PO2 levels, the SDM displays PCO2 and/or PO2
readings in grey and inhibits alarms related to PCO
2
and/or PO2
limit violations during stabilization. Furthermore, if stabilization
for one or both TC parameters cannot be achieved within
10 minutes, the SDM will trigger the low priority alarm ‘Check
sensor application’ to indicate that correct sensor application
should be verified.
Once ‘Sensor-On-Patient’ is detected, the SDM initiates
monitoring and the enabled parameters stabilize. SpO
2
and PR
usually stabilize within a few seconds, whereas PCO
2
typically
increases and PO
2
typically decreases to reach a stabilized
value within 2 to 10 minutes (see below).
TC-Stabilization after Sensor Application or
‘TC-Artifacts’
A good, hermetically sealed contact between the TC Sensor
and the skin provided, TC-readings typically stabilize within 2
to 10 minutes after sensor application, i.e. the time required
to warm up the measurement site and to achieve equilibrium
between the gas concentrations in the skin tissue and the gas
concentrations on the sensor surface.
Good to know!
If INITIAL HEATING is ON, the sensor temperature is
increased for about 13 minutes after sensor application,
facilitating faster perfusion and results (+1.5 °C with a
maximum of 43.5 °C in Neonatal Mode and +2 °C with a
maximum of 44.5 °C in Adult Mode).
Note: The use of INITIAL HEATING is subject to institution’s
permission.
Once stabilized, TC-readings can be disturbed by so-called ‘TCArtifacts’. Ambient air penetrating between the sensor surface
and the skin – the most frequent reason for ‘TC-Artifacts’ –
typically will cause PCO
2
to fall and PO2 to rise very fast.
Page 33

Page 31 . Patient Monitoring with the SDMS
Good to know!
In order to reduce the number of ‘TC-Artifacts’, a good,
hermetically sealed contact between the sensor and the
skin is essential. Ensure to use one small drop of contact
liquid when applying the sensor. Furthermore, ensure to
verify good contact between the sensor and the skin after
sensor application and to properly secure the sensor cable as
well as to routinely inspect correct sensor application during
monitoring.
Note: Excessive motion may cause ‘TC-Artifacts’. In such
cases, try to keep the patient still or change the sensor to a
site involving less motion.
Preconfigured Measurement Screens
The SDM’s numeric values and online trends provide
continuous monitoring of the enabled parameters. Depending
on the sensor type, the selected patient type and the enabled
parameters, different sets of preconfigured measurement
screens are available (numerical, numerical with online trends,
numerical with online trend and ∆x-/baseline values (p. 32),
if SpO
2
/PR are enabled all with either a wiper bar Pleth Wave
or blip bar reflecting relative pulse amplitude). Use the Display
Button (p. 42) to toggle between the available measurement
displays.
Page 34

∆x-Values and Baseline Values
Certain preconfigured measurement screens provide online
trends with ∆x-values, baseline values and baselines for PCO
2
,
PO
2
, SpO2 and/or RHP.
A parameter’s ∆x-value is displayed to the right of its online
trend and corresponds to the difference between its current
reading and its reading x minutes ago. x is called ‘DeltaTime’ and is adjustable between 1 and 120 minutes within a
password-protected area of V-STATS™. The default value for
‘Delta-Time’ is 10 minutes.
Example: A ‘∆10-value for PCO
2’
of ‘+ 8.8 mmHg’ indicates
that the current PCO
2
reading is 8.8 mmHg higher than the
PCO
2
reading ten minutes ago.
Quality Indicators for Measurement Parameters
The SDM continuously evaluates the quality of the measured
parameters and the ∆x-values and baseline values derived
thereof by assessing the severity of conditions presented to
the SDM. The results of this evaluation are used to display
status messages and/or quality indicators for the different
parameters. While a parameter is marked as:
Valid: Alarm surveillance for the respective parameter (if
applicable) is active and the SDM displays the parameter in
the selected color.
Questionable (‘?’): Alarm surveillance for the respective
parameter (if applicable) is active and the SDM displays the
parameter in the selected color and a ‘?’ adjacent to the
parameter;
Unstable (grey): Alarm surveillance for the respective
parameter is not active and the SDM displays the parameter in
grey. PCO
2
, for example, is displayed in grey when stabilizing
after sensor application or occurrence of a ‘PCO
2
artifact’
(p. 30).
Invalid (‘---’): Alarm surveillance for the respective parameter
is not active and the SDM replaces the parameter with ‘---’.
Page 35

Page 33 . Patient Monitoring with the SDMS
Good to know!
The change of a parameter’s reading within a certain time
(‘Delta-Time’) may indicate a gradual worsening of the
patient’s status. A ‘∆10-value for PCO
2
’ of ‘+ 7 mmHg’ or
more in a patient receiving opioid analgesics and sedatives,
for example, indicates opioid induced hypoventilation
and, therefore, may help to earlier recognize a developing
respiratory depression, especially in patients receiving
supplemental oxygen.
During patient monitoring, a baseline can be set by using the
respective function in the ‘Quick Access Menu’. The point of
time, at which the baseline was set, and the baseline itself
are subsequently displayed graphically (vertical and horizontal
white lines). A timer in the top left of the screen indicates
the elapsed time (hh:mm) since the baseline was set. A parameter’s baseline is numerically indicated on the left and its
∆B-value, i.e. the difference between its current reading and
its reading at the point the baseline was set, on the right of its
online trend.
Example: ‘Baseline values for PCO
2
’ of ‘33.3 + 10.1 mmHg
(00:12)’ indicate that the current PCO
2
reading is 10.1 mmHg
higher than the baseline of 33.3 mmHg which was set
12 minutes ago.
Good to know!
To assess the possible impact of a change in patient treatment (e.g. changing ventilator settings, administration
of drugs such as sedatives or opioids, changing supply of
supplemental oxygen etc.) on the patient’s ventilation and/or
oxygenation, it is recommended to set a baseline just before
changing the treatment.
Operator Events
By using the ‘Quick Access Menu’ it is possible to store up
to eight different types of Operator Events in the internal
memory of the SDM for subsequent display in V-STATS™ after
downloading trend data. Within V-STATS™, operator events
are visualized as colored triangles and, among other, can be
used to split a measurement into multiple ‘Analysis Periods’
(e.g. to analyze the different phases of a split night).
Note: Operator Events are not visualized on the SDM.
RHP Online Trends/Setting RHP Reference
Once a SenTec TC Sensor is stabilized on the skin in an environment with constant ambient temperature, the heating
power required to maintain the sensor temperature depends
to a small fraction on the local skin blood flow beneath the sensor site and, hence, heating power fluctuations may indicate
changes in local skin blood flow.
Page 36

By using the menu-parameter ‘Heating Power Mode’ the operator can select between the display of the ‘Absolute Heating
Power’ (AHP), the ‘Relative Heating Power’ (RHP), or disable
the display of the heating power. AHP and RHP values are both
displayed in Milliwatts (mW).
In ‘RHP-Mode’, deviations of the current heating power from a
stored RHP-reference value are displayed as plus or minus RHP
values once the sensor is stabilized on the skin (‘plus’ if the
current heating power is higher than the RHP-reference value,
‘minus’ if lower, and ‘0’ if identical). On most measurement
screens, RHP readings are – as the AHP readings – displayed
in the ‘Heating Power Icon’ (p. 48). On certain measurement
screens, however, the RHP-value is displayed underneath the
PCO
2
or PO2 value and the RHP online trend is depicted under-
neath the PCO
2
or PO2 online trend.
The RHP-reference value (‘408’ in this example) and the time
that has elapsed since it has been determined/set (‘00:16’ in
this example) are displayed underneath the RHP online trend.
The dashed horizontal center-line in the RHP online trend
corresponds to a RHP of 0 mW and reflects the RHP-reference
value. RHP values below/above the center-line correspond to
episodes during which the sensor required less/more power to
maintain the sensor temperature than the AHP-reference value.
At constant ambient temperature, consequently, RHP values
below/above the center-line may indicate episodes with a
decreased/increased local skin blood flow beneath the sensor site.
Keeping in mind the possible influence of local skin blood
flow fluctuations on transcutaneous blood gases (p. 6), it
is understandable that an abrupt change of transcutaneous
blood gases coupled with a significant change of RHP readings
may indicate a change in local skin blood flow, while abrupt
changes of transcutaneous blood gases unaccompanied by a
significant change of RHP readings may indicate consistent
blood flow but a change in arterial blood gases. Providing
RHP online trends underneath PCO
2
online trends or PO2
online trends, consequently, permits the clinicians to assess
at a glance whether a change of PCO
2
and/or PO2 reflects a
corresponding change of the respective arterial blood gases or
is caused or influenced by a significant change of the local skin
blood flow beneath the sensor site.
If in RHP-mode the sensor is applied to the patient when no
RHP-reference value is yet available, the SDM automatically
determines the RHP-reference value once the sensor is stabilized on the skin (which is typically the case 5 to 10 minutes
after sensor application).
Page 37

Page 35 . Patient Monitoring with the SDMS
If the sensor is stabilized on the skin, the RHP-reference value
can be set either a) by using the respective function in the
‘Quick Access Menu’ that activates after pressing the Enter
Button when a measurement screen is active or b) by changing the menu-parameter ‘Heating Power Mode’ from ‘Relative’
to ‘Absolute’ or ‘OFF’ and back to ‘Relative’.
To clear/reset the RHP-reference value, either remove the sensor from the patient and insert it into the Docking Station or
set the menu-parameter ‘Relative Heating Mode’ to ‘OFF’.
‘V-Check™ Mode’
In standard configuration, the SDM’s numeric values and
online trends provide continuous monitoring of the enabled
parameters. If the menu-parameter ‘V-Check™ Mode’ is set
to ON (only selectable if enabled by the institution), the SDM
provides a Ventilation Spot Check with a statistical result
screen displaying mean, minimum, maximum, median and
standard deviation for the enabled parameters.
A V-Check™ Measurement consists of the V-Check™ Stabilization Phase (default duration 8 minutes) and the V-Check™
Measurement Phase (default duration 2 minutes). If the
V-Check™ Measurement is finished two short signal tones
sound and the V-Check™ Results Screen activates, displaying
the above mentioned statistical results for the data assessed
during the V-Check™ Measurement Phase. The V-Check™ Results Screen remains displayed until the Menu or Display Button are pressed or another V-Check™ Measurement is started.
Note: The ‘V-Check™ Mode Indicator’ appears on the ‘Ready
for use’ and ‘Calibration’ screen (p. 22) if the V-Check™
Mode is ON. On measurement screens (p. 31), the V-Check™
Down-Counter (format hh:mm:ss) is displayed on the very right
of the Status Bar (p. 48). This down-counter indicates the
duration of the V-Check™ Measurement if the V-Check™ Measurement has not yet been started, the remaining time to finish the V-Check™ Measurement during an ongoing V-Check™
Measurement, and 00:00:00 once the V-Check™ Measurement
is finished. If the SDMS is not ready for use, it indicates --:--:--.
Note: Print-out of the trend curves (including the statistical
results) is automatically activated upon completion the
V-Check™ Measurement if the protocol ‘Serial Printer’ is
selected and a printer is connected to the SDM.
Note: The SDM automatically stores V-Check™ Events in its
internal memory at the start and at the end of each V-Check™
Measurement Phase. After trend data download to V-STATS™
the start and end of a V-Check™ Measurement Phase are
visualized by two colored triangles and it is possible to generate
a report which includes the same information as is provided on
the SDM’s V-Check™ Results Screen.
Page 38

Good to know!
To use V-Check™, select the SenTec-preconfigured SDM
Profile V-CHECK as standard ‘SDM Profile’. This will set the
sensor temperature to 43.5 °C, the ‘Site Time’ to 0.5 hours,
SITE PROTECTION to ON, the ‘Calibration Interval’ to 1 hour,
and the ‘Time Range for Trends’ to 15 minutes.
PCO2 In-Vivo Correction
Subject to institution’s permission, ‘In-Vivo Correction’ (IC)
of PCO
2
values is possible at the bedside. The ‘PCO2 In-Vivo
Correction’ allows for adjusting the SDM’s PCO
2
readings based
on the result of an arterial blood gas analysis. The ‘PCO
2
InVivo Correction’ adjusts the ‘Metabolic Offset’ (M) used in the
‘Severinghaus Equation’ (p. 5) such that the difference
between the PCO
2
value displayed by the SDM when taking
the blood sample and the PaCO
2
value as determined by the
blood gas analysis cancels out. The ‘PCO
2
In-Vivo Correction’
should only be used when a systematic difference between
the SDM’s PCO
2
readings and PaCO2 is clearly established by
several arterial blood gas measurements
Note: ‘The Quick Access Menu’ provides a short-cut to the
sub-menu ‘PCO
2
In-Vivo Correction’, which is only accessible if
enabled by the institution.
Note: If PCO
2
values are in-vivo corrected, the ‘PCO2 In-Vivo
Correction’ indicator (‘IC-indicator’) is displayed adjacent to
the PCO
2
label (IC=xx.x (if ‘mmHg’); IC=x.xx (if ‘kPa’), where
xx.x/x.xx is the current offset, respectively; if additionally a
fixed ‘Severinghaus Correction’ is used, the ‘PCO
2
In-vivo
Correction’ offset is marked with an asterisk: e.g. ‘IC=x.xx*’.).
WARNING: A ‘PCO2 In-Vivo Correction’ should only
be enabled by personnel understanding the principles and
limitations of transcutaneous PCO
2
monitoring (p. 6).
If a ‘PCO
2
In-Vivo Correction’ is made it must be checked
periodically and adapted in case of changes.
Patient Data Management
The SDM automatically stores PCO2, PO2, SpO2, PR, RHP and
PI data as well as system status information in its internal
memory for subsequent on-screen viewing or printing of
graphical trends and statistical summary/histograms. The
Data Recording Interval is institution-selectable between
1 and 8 seconds and provides between 35.2 and 229.9 hours
of monitoring data, respectively. V-STATS™ provides fast data
download to the PC with V-STATS™ (approx. 3 min. for 8 hours
data at 4-seconds resolution) for subsequent display, analysis
and reporting within V-STATS™.
Patient data acquired by the SDM can be output through the
multipurpose I/O-port (analog output; nurse call), the serial
data port (RS-232) or the LAN port, all located on the rear
panel of the SDM. These ports can be connected to external
devices such as multiparameter bedside monitors, PCs,
poly(somno)graphs, nurse call systems, chart recorders or
data loggers.
Page 39

Page 37 . Patient Monitoring with the SDMS
Note: To terminate the ‘Site time elapsed’ alarm, remove the
sensor from the patient and either press the Enter Button while
the message ‘Sensor off patient (8 )’ displays or insert the
sensor into the Docking Station.
CAUTION: Do not reattach the sensor to the same site if
any skin irritations are noted during site inspection.
Good to know!
If the safety feature SITE PROTECTION is ON, the SDM
will reduce the sensor temperature to safe values once the
sensor application duration overruns the selected ‘Site Time’
by more than 10% or 30 minutes. PCO
2
/PO2 are marked as
‘invalid’ thereafter (values replaced by ‘---’).
During monitoring, the current setting for SITE PROTECTION
is indicated in the ‘Sensor Temperature’ icon (p. 48). A
‘red-blue rightward arrow with tip down’ displays if SITE
PROTECTION is ON, a ‘red rightward arrow’ if it is OFF.
By using V-CareNeT™, for example, remote monitoring and
secondary alarm surveillance of multiple SDMs connected to
the same network as the PC is possible. ‘Operator Events’,
‘Baselines’, and certain SDM settings can be set/controlled
remotely on the included SDMs. Furthermore, download of
SDM Trend Data is simultaneously possible for multiple SDMs.
‘Remaining Monitoring Time’/‘Site Time Elapsed’
Alarm
During monitoring, the ‘Remaining Monitoring Time’ Icon
(p. 48) continuously indicates the ‘Remaining Monitoring
Time’, i.e. the time until either the selected ‘Site Time’ or – if
PCO
2
is enabled – the ‘Calibration Interval’ elapse (whichever
will occur first).
When the ‘Calibration Interval’ elapses before the selected
‘Site Time’, the ‘Remaining Monitoring Time’ Icon is highlighted
yellow, the message ‘Sensor calibration recommended’ is displayed and monitoring is possible another 4 to 6 hours with
PCO
2
marked as ‘questionable’. Thereafter, sensor calibration
is mandatory and PCO
2
and PO2 are marked as ‘invalid’ (values
replaced by ‘---’). When the ‘Site Time’ elapses, the icon is
highlighted in red and the low priority alarm ‘Site time elapsed’
is triggered. In this case, the sensor must be removed from the
patient for site inspection.
Page 40

3. Clean the sensor with a swab wetted
with 70% isopropanol to remove any
contact liquid residues or dirt (for other
approved cleaning agents refer to the
sensor’s Directions for Use).
4. Check the condition of the sensor membrane and the
integrity of the sensor (p. 15). Change the membrane if
necessary (p. 17). Do not use the sensor if any problems
are noted.
Important: Before reapplying the sensor to the same site,
we recommend calibrating the sensor even if calibration is not
yet mandatory or recommended by the SDM. If you skip the
calibration, at least reset the Site Timer by pressing the Enter
Button when the message ‘Sensor off patient (8 )’ displays and
then continue at step 6.
5. To calibrate the sensor, open the
Docking Station Door and hang the
sensor in the holder inside the Docking
Station Door (the red light will appear).
Close the Docking Station Door.
Sensor Removal with
Multi-Site Attachment Ring/Easy
Remove the sensor from the patient when monitoring is
completed or monitoring time has elapsed (message ‘Site time
elapsed’ or ‘Calibrate sensor’).
CAUTION: For site inspection and/or calibration, the
Multi-Site Attachment Ring/Easy can remain on the same site
for up to 24 hours and may be reused for another sensor
application. It is recommended to remove and to discard the
Multi-Site Attachment Ring/Easy after 24 hours and to keep
the measurement site free of adhesive for 8 to 12 hours.
Sensor Removal for Subsequent Reattachment to
Same Site
1. Remove the adhesive tape securing the sensor cable.
2. Place a finger on each side of the
ring and rotate the sensor towards the
index finger. The index finger will act as
a wedge and will disengage the sensor
from the ring.
i
s
o
p
r
o
p
a
n
o
l
7
0
%
Page 41

Page 39 . Patient Monitoring with the SDMS
Note: Sensor calibration – if necessary – will start (message
‘Calibration in progress’). The message ‘Ready for use’ will
display once calibration is finished.
6. Clean the skin in the center of the ring with a dry swab or, if
necessary, a swab wetted with 70% isopropanol (or according
to your institution’s skin cleaning/degreasing procedures) to
remove any contact liquid residues or dirt and let it dry.
7. Carefully inspect the measurement site.
CAUTION: Do not reattach the sensor to the same site if
any skin irritations are noted during site inspection.
8. To reapply the sensor to the same site, continue at step 5
in section ‘Sensor Application using a Multi-Site Attachment
Ring/Easy’ (p. 25). Make sure to reapply one small drop
of contact liquid to the site before reinserting the sensor into
the MAR/e.
Sensor Removal without Reattachment to Same
Site
1. Remove the sensor together with the Multi-Site Attachment
Ring/Easy by carefully lifting the ring’s little tab
2. Clean the skin with a dry swab or, if necessary, a swab
with 70% isopropanol (or according to your institution’s skin
cleaning/degreasing procedures) to remove any contact liquid
residues or dirt and then carefully inspect the site to note any
potential skin irritations.
3. Remove the sensor from the MAR/e, discard the ring and
then follow steps 3 to 5 above to clean the sensor, to check the
condition of its membrane and its integrity as well as to insert
it in the Docking Station for calibration and/or storage.
CAUTION: To maintain monitor readiness and minimize
PCO
2
drift potential, always keep the SDM switched on and
store the sensor in the Docking Station in between monitoring.
Page 42

Sensor Removal with Ear Clip
Remove the sensor from the patient when monitoring is
completed or monitoring time has elapsed (message ‘Site time
elapsed’ or ‘Calibrate sensor’).
CAUTION: For site inspection and/or calibration,
the Ear Clip can remain on the same earlobe for up to 24
hours and may be reused for another sensor application.
It is recommended to remove and to discard the Ear Clip
after 24 hours and to keep the earlobe free of adhesive for
8 to 12 hours.
Sensor Removal for Subsequent Reattachment to
Earlobe
1. Remove the adhesive tape securing the sensor cable.
2. Grab the sensor at its neck with one
hand and detach it from the Ear Clip
while holding the clip in place with the
other hand.
3. Clean the sensor with a swab wetted
with 70% isopropanol to remove any
contact liquid residues or dirt (for other
approved cleaning agents refer to the
sensor’s Directions for Use).
4. Check the condition of the sensor membrane and the
integrity of the sensor (p. 15). Change the membrane if
necessary (p. 17). Do not use the sensor if any problems
are noted.
Important: Before reapplying the sensor to the same earlobe,
we recommend calibrating the sensor even if calibration is not
yet mandatory or recommended by the SDM. If you skip the
calibration, at least reset the Site Timer by pressing the Enter
Button when the message ‘Sensor off patient (8 )’ displays and
then continue at step 6.
5. To calibrate the sensor, open the
Docking Station Door and hang the
sensor in the holder inside the Docking
Station Door (the red light will appear).
Close the Docking Station Door.
i
s
o
p
r
o
p
a
n
o
l
7
0
%
Page 43

Page 41 . Patient Monitoring with the SDMS
Note: Sensor calibration – if necessary – will start (message
‘Calibration in progress’). The message ‘Ready for use’ will
display once calibration is finished.
6. Clean the skin in the center of the Ear Clip’s retainer ring
with a dry swab or, if necessary, a swab wetted with 70%
isopropanol (or according to your institution’s skin cleaning/
degreasing procedures) to remove any contact liquid residues
or dirt and let it dry.
7. Carefully inspect the earlobe.
CAUTION: Do not reattach the sensor to the same
earlobe if any skin irritations are noted during site inspection.
8. To reapply the sensor to the same earlobe, continue at step
5 in section ‘Sensor Application using an Ear Clip’ (p. 27).
Make sure to reapply one small drop of contact liquid to the
sensor’s center before reinserting it into the Ear Clip.
Sensor Removal without Reattachment to Same
Earlobe
1. Open the clip’s jaws and remove it
from the earlobe together with the sensor by turning it sideways.
2. Clean the earlobe with a dry swab or, if necessary, a swab
wetted with 70% isopropanol (or according to your institution’s
skin cleaning/ degreasing procedures) to remove any contact
liquid residues or dirt and then carefully inspect the earlobe to
note any potential skin irritations.
3. Remove the sensor from the Ear
Clip, discard the clip and then follow
steps 3 to 5 above to clean the sensor,
to check the condition of its membrane
and its integrity as well as to insert it in
the Docking Station for calibration and/
or storage.
CAUTION: To maintain monitor readiness and minimize
PCO
2
drift potential, always keep the SDM switched on and
store the sensor in the Docking Station in between monitoring.
Page 44

AUDIO
PAUSED
/AUDIO
OFF
Button
• to pause auditory alarm signals for 1 or 2 minutes
(depending on respective menu setting)
• to switch OFF auditory alarm signals permanently (by
pressing > 3 seconds)
Note: Switching off auditory alarm signals is only possible if enabled by the institution.
Note: This button is inactive if the menu parameter
‘Alarm Settings/Alarm Volume’ is set to OFF.
Enter
Button
• to activate the selected sub-menu or function
• to activate/deactivate ‘editing mode’ for the selected
menu parameter*
• to activate ‘Quick Access Menus’ (only if menu is not
open)
• to terminate the ‘Sensor off patient (8 )’** and ‘Remote
Monitoring Interrupted (8 )’ alarms
• to activate the second ‘System Information’ page (only
if first ‘System Information’ page is open)
Display
Button
• to toggle between the available measurement screens
• to deactivate ‘editing mode’ for the selected
menu-parameter*
• to exit the menu from any menu level (only if ‘editing
mode’ is inactive)
*For parameters that are highlighted with a blue menu bar in
‘editing mode’, changes become effective immediately without
confirmation (see example 1 below). For parameters that are
highlighted with a yellow menu bar in ‘editing mode’, changes
Menu/
Previous
Level
Button
• to activate the menu
• to return to the menu on the next higher level (only
if ‘editing mode’ is inactive, exits the menu if pressed
while at top level)
• to deactivate ‘editing mode’ for the selected
menu-parameter*
Note: Menu access can be disabled by the institution
(e.g. for home use)
UP
Button
• to select a menu-item by scrolling the blue menu bar
upwards through the menu (only if ‘editing mode’ is
inactive)
• to increase the value of the menu parameter for which
‘editing mode’ is active*
• to increase the brightness of the display (only if a
measurement screen is active)
DOWN
Button
• to select a menu-item by scrolling the blue menu bar
downwards through the menu (only if ‘editing mode’
is inactive)
• to decrease the value of the menu parameter for which
‘editing mode’ is active*
• to decrease the brightness of the display (only if a
measurement screen is active)
Controls, Indicators and Alarms
Controls (Buttons)
The ON/OFF switch is located on the rear panel of the SDM
24
. The following controls (buttons) are located on the front
panel of the SDM:
Page 45

Page 43 . Controls, Indicators and Alarms
must be confirmed by pressing the Enter Button to become effective (see example 2 below). To cancel changes/deactivate ‘editing
mode’, use the Menu/Previous Level Button or the Display Button.
** will also reset the Site Timer
Example 1: ‘SpO2 Low Limit’
The parameter ‘SpO2 Low Limit’ is included in the menu ‘Alarm
Settings’. It is an example of a parameter for which changes
made with the UP/Down Buttons become immediately ef-
fective without confirmation. To change the parameter
‘SpO
2
Low Limit’, proceed as follows:
• Press
to access the menu.
• Press
to open/activate the menu ‘Alarm Settings’.
• Press
3 times to scroll down the blue menu bar to the
parameter ‘SpO
2
Low Limit’.
• Press
to activate ‘editing mode’ for the parameter ‘SpO2
Low Limit’. Note that the ‘Enter’ symbol at the end of the line
is replaced by up/down arrows and that the color of the menu
bar remains blue.
• Press
or as many times as required to select the
desired SpO
2
low limit. Note that changes become effective
immediately.
• Press
, or to deactivate ‘editing mode’ for the
parameter ‘SpO
2
Low Limit’. Note that the ‘Enter’ symbol
reappears at the end of the line and that the color of the
menu bar remains blue.
• Press
to return to the main menu or to exit the
menu.
Note: Changes made with the UP/Down Buttons immediately become effective without confirmation for all parameters
except ‘Patient’, ‘Enabled Parameters’ and ‘Language’
(see example 2).
Example 2: ‘Language selection’
The parameter ‘Language’ is included in the menu ‘System Settings’. It is an example of a parameter for which changes must
be confirmed by pressing the Enter Button before they become effective. To change the parameter ‘Language’, proceed
as follows:
• Press
to access the menu.
• Press
3 times to scroll down the blue menu bar to the
menu ‘System Settings’.
• Press
to open/activate the menu ‘System Settings’.
• Press
3 times to scroll down the blue menu bar to the
parameter ‘Language’.
• Press
to activate ‘editing mode’ for the parameter
‘Language’. Note that the ‘Enter’ symbol at the end of the
line is replaced by up/down arrows followed by an ‘Enter’
symbol and that the color of the menu bar changes from blue
to yellow.
Page 46

• Press or as many times as required to select the
desired language. Note that changes do not become
effective.
• Press
to confirm the selected language and to deactivate
‘editing mode’. To cancel changes and deactivate ‘editing
mode’ press
or . Note that upon deactivation of the
‘editing mode’ the ‘Enter’ symbol reappears at the end of the
line and the color of the menu bar changes from yellow to
blue.
Note: After language confirmation, the SDM automatically
exits the menu.
Note: Operator access to the parameter ‘Language’ can
be disabled by the institution by using V-STATS™ within a
password protected area.
Example 3: ‘Confirmation of Membrane Change’
To reset the membrane timer after a successful membrane
change, the membrane change must be confirmed on the SDM
by using the function ‘Membrane Change Done’ in the menu
‘Membrane Change’. To confirm a membrane change, proceed
as follows:
• Press
to access the menu.
• Press
twice to scroll down the blue menu bar to the menu
‘Membrane Change’.
• Press
to open/activate the menu ‘Membrane Change’.
Note: The SDM automatically activates the menu ‘Membrane
Change’ if a sensor with an expired membrane is inside the
Docking Station.
• Press
once to scroll down the blue menu bar to the
function ‘Membrane Change Done’.
• Press
to confirm the membrane change.
Note: The menu ‘Membrane Change’ and the function
‘Membrane Change Done’ are dimmed grey (not accessible)
if the sensor is attached to the patient or inside the Docking
Station. In this case, remove the sensor from the patient or the
Docking Station to confirm the membrane change.
Page 47

Page 45 . Controls, Indicators and Alarms
Auditory Indicators/Signals
The SDM provides the following auditory signals:
• Auditory alarm signals for high, medium and low priority
alarm conditions (p. 46); use the parameter ‘Alarm Volume’
to adjust the volume of these signals.
• The ‘AUDIO OFF Reminder’ (short signal tone) sounds every
60 seconds if the auditory alarm signals are permanently
switched off. Operator access to switch off this reminder
signal is subject to institution’s permission; its volume is not
adjustable.
• The ‘Auditory Power On Self Test Signal’ (three short tones)
sounds during the ‘Power On Self Test’; its volume is not
adjustable.
• The ‘Ready for use’ Beep (short tone) sounds at the end of a
successful calibration of a SenTec TC Sensor. This signal can
only be switched ON/OFF by the institution; its volume is not
adjustable.
• The Key Click (short tone) indicates that a button has been
properly pressed; use the parameter Key Click to switch off/
adjust the volume of this signal.
LED Indicators
The following visual LED indicators are located on the front
panel of the SDM:
AUDIO
PAUSED/
AUDIO OFF
Indicator
• Yellow LED: Auditory alarm signals paused for
1 or 2 minutes
• Yellow LED flashes: Auditory alarm signals
permanently switched off (activated by pressing
AUDIO PAUSED/AUDIO OFF Button > 3 seconds)
• LED OFF: Auditory signals either active or per-
manently switched off by setting menu parameter
‘Alarm Settings/Alarm Volume’ to OFF.
ON/OFF
Indicator
• Green: SDM turned on
• LED OFF: SDM turned off
AC Power/
Battery
Indicator
• Green LED: Connected to AC power, battery fully
charged
• Yellow LED: Connected to AC power, battery
charging
• LED OFF: Not connected to AC power (i.e. pow-
ered by internal battery)
Note: The AC Power/Battery Indicator works irrespective of whether the SDM is switched on or off.
Page 48

• The ‘Pulse Beep’ (short tone) sounds once for each pulse. Its
automatic pitch modulation reflects changing SpO
2
levels; use
the parameter ‘Pulse Beep’ to switch off/adjust the volume of
this signal.
• The ‘Button Disabled Beep’ (long tone) sounds if a currently
disabled button is pressed (e.g. the Menu Button if ‘Menu
Access’ has been disabled by the institution); its volume is
not adjustable.
• The ‘Button Disabled Beep’ (low pitched tone) sounds if a
Control Button is pressed that is currently disabled (e.g. if the
Menu/Previous Level Button is pressed when ‘Menu Access’ is
disabled by institution).
• The ‘V-Check™ Completed Beep’ (high pitched two beep
tone) sounds upon termination of a V-Check™ Measurement;
use the parameter ‘Alarm Volume’ to adjust the volume of
this signal.
Note: The SDM ranks the priority of auditory alarm signals
and, to ensure that auditory signals do not superpose, only
outputs the highest priority acoustic signal.
Alarms
The SDM uses visual and auditory alarm signals to alert the
user when a physiological measurement parameter (PCO
2
, PO2,
SpO
2
, PR) violates its alarm limits and to inform the user about
technical conditions of the equipment that require operator
response or awareness. By degree of urgency, the SDM’s
alarm conditions are assigned to the following priorities: High
priority (SpO
2
limit violation), medium priority (PCO2, PO
2
or PR limit violation, ‘Battery Critical’ (if SDM not connected to
AC power)), low priority (various technical alarm conditions).
All alarm signals of the SDM automatically cease when the
associated triggering event has terminated.
WARNING: Setting alarm limits for physiological
measurement parameters to extreme values may render the
SDM’s alarm system useless for the respective parameter.
WARNING: Ensure to select the upper alarm limit for
PO
2
and SpO2 carefully and according to accepted clinical
standards. High oxygen levels may predispose a premature
infant to develop retinopathy.
Note: Alarm surveillance for physiological measurement
parameters (PCO
2
, PO2, SpO2, PR) is only active if the respective
parameter is valid or questionable (p. 32). Otherwise,
generation of alarm signals for the respective parameter is
automatically suspended.
Page 49

Page 47 . Controls, Indicators and Alarms
Visual Alarm Signals
The ‘Alarm Status Icon’ (p. 48) indicates the highest currently
active alarm priority. If a physiological parameter violates its
alarm limits, the respective parameter and the ‘Alarm Status
Icon’ flash (with 0.7 Hz for SpO
2
and 1.4 Hz for PCO2, PO2,
PR). ‘Status Messages’ (only one at a time) and/or various
‘Status Icons’ visualize technical alarm conditions and general
information on the system status. The SDM’s visual alarm
signals cannot be deactivated.
WARNING: If the display of the SDM is inactive when
the parameter ‘Display in Sleep Mode’ is set to ON, the display
will not reactivate if an alarm condition occurs. In this case,
visual alarm signals are not visible.
WARNING: Current values of monitored parameters
and visual alarm signals may become illegible if the display
brightness is dimmed too much.
WARNING: Do not inactivate or dim the brightness
of the monitor’s display if the patient’s safety could be
compromised.
Auditory Alarm Signals
The SDM’s auditory alarm signals are priority encoded. A high
priority alarm condition is indicated by a high-pitched fast
pulsing tone (two bursts of five short pulses repeated
every 10 seconds), a medium priority alarm condition by a
medium-pitched pulsing tone (one burst of three pulses
repeated every 10 seconds), and a low priority alarm condition
by a low-pitched slow pulsing tone (one burst of two pulses
repeated every 15 seconds). Alarm melodies can be enabled/
disabled by the institution.
The volume of auditory alarm signals can be adjusted (levels
OFF, 1 to 6, Rising). OFF is only selectable if enabled by the
institution. If ‘Rising’ is selected, the volume of auditory alarm
signals – starting at level 2 – increases at each burst by one
level. If OFF is selected, auditory alarm signals are permanently
switched off.
CAUTION: Using the AUDIO PAUSED/OFF Button,
auditory alarm signals can be paused or permanently switched
off (p. 42).
Note: If auditory alarm signals are permanently switched off,
the ‘AUDIO OFF Reminder’ sounds every 60 seconds (unless
disabled by the institution).
Page 50

2011-07-01 15:28:30
7.7h
100%
+
AD
°C
41.9
RHP
[Joe Miller]
-/-
Note: The operating status of the SDM’s auditory alarm signals
is visually indicated by the ‘AUDIO STATUS Icon’ (p. 48),
the ‘AUDIO PAUSED/AUDIO OFF Indicator’ (p. 45), and
acoustically indicated by the ‘AUDIO OFF Reminder’.
WARNING: If an alarm condition occurs while the
auditory alarm signals are paused or permanently switched
off, the only alarm indication will be visual, but no alarm tone
will sound.
WARNING: Verify that the alarm volume is adjusted
such that the alarm signals are clearly audible for the
operator in the intended environment. Do not disable the
audible alarm function or decrease the audible alarm volume
if the patient’s safety could be compromised.
WARNING: Ensure that the speaker is clear of any
obstructions. Failure to do so could result in an inaudible
alarm signal.
WARNING: The nurse call feature is inactive whenever
the auditory alarm signals are PAUSED or OFF.
Note: When the alarm system of an SDM that is remotely
monitored via V-CareNeT™ is in the AUDIO OFF state, the
SDM will terminate the AUDIO OFF state if the connection
between the SDM and the V-CareNeT™ Central Station is
interrupted. For details, refer to the Technical Manual for the
SDM (HB-005752).
Status Bar with Status Icons and Status
Messages
The Status Bar is located in the bottom of nearly all screens.
1 2 3 4 5
6 7 8 9
On the left, it displays up to 5 Status Icons (1 to 5).
The ‘Battery’ Icon
1
indicates the remaining battery capacity
in %. The icon highlights yellow when battery capacity is below
10% and red if the remaining battery capacity is critical.
On measurement/menu screens, position
2
displays the
‘Patient Type’ Icon (‘AD’ in ‘Adult’ mode or ‘NEO’ in ‘Neonatal’
mode), whereas position
2
displays the ‘Barometric Pressure’
Icon on the ‘Calibration Screen’. The ‘Barometric Pressure’
Icon indicates the measured ambient barometric pressure in
‘mmHg’ or ‘kPa’. The icon highlights red if a barometer fault
is detected and yellow if the barometric pressure is unstable
during sensor calibration.
The ‘Remaining Monitoring Time’ Icon
3
indicates the
‘Remaining Monitoring Time’ (Format: xx.x h) on measurement/
menu screens, whereas on the ‘Calibration Screen’ the same
icon indicates the ‘Available Monitoring Time’. The pie chart –
which is updated in steps of 20% – indicates the remaining
monitoring time in percentage. The Icon highlights yellow if
only the ‘Calibration Interval’ has elapsed and it highlights red
whenever the ‘Site Time’ has elapsed.
Page 51

Page 49 . Controls, Indicators and Alarms
The Alarm Status Icon
8
indicates the ranking of the
highest priority alarm condition (flashing white triangle with
curved line and exclamation mark on red background in a
high priority alarm condition; flashing black triangle with
curved line and exclamation mark on yellow background in
a medium priority alarm condition; black triangle with
curved line and exclamation mark on cyan background in a
low priority alarm condition; light grey check mark symbol
on dark-grey background if no alarm condition).
On the very right
9
, the Status Bar usually indicates the
monitor’s date/time in the ‘yyyy-mm-dd hh:mm:ss’ format. On
measurement screens (p. 31), the date/time indication is
replaced by the V-Check™ Down-Counter (format hh:mm:ss)
in V-Check™ Mode (p. 35). This down-counter indicates the
duration of the V-Check™ Measurement if the V-Check™ Measurement has not yet been started, the remaining time to finish the V-Check™ Measurement during an ongoing V-Check™
Measurement, and 00:00:00 once the V-Check™ Measurement
is finished. If the SDMS is not ready for use, it indicates --:--:--.
Good to know!
The date/time of the SDM can be adjusted in the menu; or, by
using V-STATS™, it is possible to set the SDM’s date/time to
the current date/time of the PC (i.e. to synchronize the date/
time setting of the SDM and the PC).
The ‘Sensor Temperature’ Icon 4 indicates the measured
sensor temperature (°C) and the current setting of SITE
PROTECTION. A ‘red-blue rightward arrow with tip down’
appears if SITE PROTECTION is ON, a ‘red rightward arrow’ if it
is OFF. The ‘Sensor Temperature’ Icon is marked yellow during
INITIAL HEATING, blue if SITE PROTECTION has reduced
the sensor temperature and red if the SDMS’ temperature
surveillance detected a sensor temperature-related problem.
On measurement/menu screens, position 5 either displays
the ‘Absolute Heating Power’ (AHP), the ‘Relative Heating
Power’ (RHP), both in mW, or no icon if Heating Power Mode
is OFF, whereas position
5
displays the ‘Gas Icon’ on the
‘Calibration Screen’. The ‘Gas Icon’ indicates the remaining
capacity of the Service Gas Bottle in %. It is marked yellow if
the remaining capacity is below 10% and red if the gas bottle
is empty (format: xxx%).
Note: On measurement/menu screens with RHP online trends,
no icon is displayed at position
5
.
The Status Text Field
6
in the middle displays Status Messages
(alarm/information messages). If there is no current Status
Message, the name of the presently active menu is displayed
in the status text field of menu screens and – during remote
monitoring via V-CareNeT™ – the ‘Patient Info’ is displayed in
the status text field of measurement screens.
The AUDIO Status Icon
7
on the right of the status text field
indicates the status of the SDM’s auditory alarm signals (ON,
PAUSED, OFF).
Page 52

Maintenance of the SDMS
During normal use, the SDM does not require any internal
adjustments or additional calibrations. However, to guarantee
continuous performance, reliability and safety of the SDMS,
routine checks and maintenance procedures (including
cleaning/disinfection) as well as safety and functionality checks
should be performed regularly.
The Technical Manual for the SenTec Digital Monitor (SDM)
provides instructions for cleaning and/or disinfecting the SDM
and the Digital Sensor Adapter Cable. Please refer to the
respective Directions for Use for instructions for cleaning and/
or disinfecting SenTec TC Sensors.
Routine Checks
The following checks should be performed regularly:
• Before and after every use check the SenTec TC Sensors
(p. 15).
• Weekly clean and disinfect SenTec TC Sensors and the Digital
Sensor Adapter Cable.
• ‘Power On Self Test’ (POST): Every time the SDM is switched
on (p. 12), the POST is performed automatically. If your
SDM is permanently switched on, switch it off and on again
once a month to perform a POST.
• Weekly clean the Docking Station gasket using a cotton
swab moistened with 70% isopropanol (for other approved
cleaning agents refer to the Technical Manual for the SDM).
• Monthly inspect the Docking Station Door and gasket for
mechanical and functional damages.
• Monthly check the SDM, sensors, sensor adapter cables and
power cord for mechanical or functional damages. Defective
parts must be replaced by original replacement parts.
• Monthly perform a ‘Sensitivity Test’ PCO
2
/PO2 (can be activated
in the menus ‘PCO
2
Settings’ or ‘PO2 Settings’).
• Monthly check the sensor temperature by comparing the
displayed sensor temperature to the sensor SET Temperature.
• Monthly check the barometer reading of the SDM against a
calibrated barometer.
• Monthly check the alarm function of the SDM and correct
functioning of its interfaces (if used).
Refer to the Service Manual for the SDMS and the Directions
for Use for the sensors for additional/complete check lists and
detailed maintenance procedures.
Note: Check the disposables monthly and replace any expired
products.
Page 53

Page 51 . Maintenance of the SDMS
Service
It is recommended that a complete safety and functionality
check is performed at regular intervals (recommended every
12 months but at least once every 24 months) or in accordance
with institutional, local and governmental regulations
(refer to the Service Manual for the SDMS for details).
To perform a safety check and for service or repair, contact
qualified service personnel or your local SenTec representative.
Please note that repair and service procedures which require
opening the cover of the SDM must be performed by SenTec
authorized service personnel.
WARNING: The cover should only be removed by
SenTec authorized service personnel. There are no user-
serviceable parts inside the SDM.
Page 54

Specifications of tcPCO2 and tcPO
2
tcPCO
2
Measurement range 0 – 200 mmHg (0 – 26.7 kPa)
Resolution 0.1 mmHg (0.01 kPa) below
100 mmHg (10 kPa) / 1 mmHg
(0.1 kPa) above 100 mmHg (10 kPa)
Drift Typically < 0.5%/hour
Response time (T90) Typically < 75 sec.
Linearity Typically < 1 mmHg (0.13 kPa)
Interferences by
anesthetic gases
Negligible
Stabilization/
artifact detection
After sensor application or occurrence of a tcPCO
2
artifact, tcPCO2
is displayed in grey until it
(re)stabilizes.
tcPO
2
Measurement range 0 – 800 mmHg (0 – 106.7 kPa)
Resolution 1 mmHg (0.1 kPa)
Drift Typically < 0.1%/hour
Response time (T90) Typically < 150 sec.
Linearity Typically < 1 mmHg (0.13 kPa)
Interferences by
anesthetic gases
Negligible
Stabilization/
artifact detection
After sensor application or occurrence of a tcPO
2
artifact, tcPO2
is displayed in grey until it
(re)stabilizes.
Specifications of tcPCO2 , tcPO2 and Pulse Oximetry
Page 55

Page 53 . Specifications of tcPCO2 , tcPO2 and Pulse Oximetry
Specifications of Pulse Oximetry
Oxygen Saturation (SpO2)
Approved sites
for SpO2/PR monitoring
with SenTec TC sensors
Earlobe, low on forehead,
cheek, upper arm,
scapula (shoulder blade)
Measurement range 1 – 100%
Resolution 1%
Accuracy
(Arms over 70 to 100% range; all above specified sites)
• V-Sign™ Sensor 2 ± 2%
• OxiVenT™ Sensor ± 2.25%
Note: The SDMS measures functional oxygen saturation.
Note: SpO
2
accuracy specification is based on controlled
hypoxia studies on healthy, adult volunteers over the specified
saturation range by applying a defined sensor type to the
specified measurement sites. Pulse oximeter SpO
2
readings
were compared to SaO
2
values of blood samples measured
by hemoximetry. SpO
2
accuracy is expressed as Arms (rootmean-square). The indicated variation equals plus or minus
one standard deviation (1SD), which encompasses 68% of the
population.
Note: A functional tester cannot be used to assess the SpO
2
accuracy.
Pulse Rate (PR)
Measurement range 30 – 250 bpm (beats per minute)
Resolution 1 bpm
Accuracy ± 3 bpm
Note: PR accuracy was determined using a Pulse Oximeter
Simulator (optical simulator for bench tests).
Note: A functional tester cannot be used to assess the PR
accuracy.
Page 56

Symbol Name Description of Symbol
Manufacturer
Indicates the medical device
manufacturer.
Date of
Manufacturer
Indicates the date when the
medical device was manufactured.
Use-by date
Indicates the date after which the
medical device is not to be used.
LOT
Batch code
Indicates the manufacturer’s batch
code so that the batch or lot can
be identified.
Catalogue
number
Indicates the manufacturer’s
catalogue number so that the
medical device can be identified.
Serial number
Indicates the manufacturer’s serial
number so that a specific medical
device can be identified.
Fragile,
handle with
care
Indicates a medical device that
can be broken or damaged if not
handled carefully.
Symbol Name Description of Symbol
Keep dry
Indicates a medical device that
needs to be protected from
moisture.
Temperature
limit
Indicates the temperature limits to
which the medical device can be
safely exposed (upper and lower
limits of temperature are indicated
adjacent to the upper and lower
horizontal lines).
Humidity
limitation
Indicates the range of humidity to
which the medical device can be
safely exposed (humidity limitation
indicated adjacent to the upper
and lower horizontal lines).
Do not re-use
(Single use)
Indicates a medical device that is
intended for one use, or for use
on a single patient during a single
procedure.
Consult
instructions
for use
Indicates the need for the user to
consult the instructions for use.
Follow
instructions
for use
Refer to accompanying documents
for further detailed instructions
and information.
Warning
Refer to accompanying documents
for warnings.
Glossary of Symbols
The table below summarizes symbols used on the SDMS
(including all its related parts), on the packaging and in the
associated documentation. These symbols indicate information
essential for proper use; the order of their appearance is not
prioritized.
Page 57

Page 55 . Glossary of Symbols
Symbol Name Description of Symbol
Equipotentiality
Equipotential Terminal (ground)
ON
(SDM rear
button)
Monitor ON
OFF
(SDM rear
button)
Monitor OFF
I/O
Multipurpose
Port
Nurse Call + Analog Output
Nurse Call
Nurse Call (integrated into
Multipurpose Port)
RS-232
Serial Data Port (RS-232)
LAN
LAN
Local Area Network Port
Defibrillation
Proof
Type BF
Degree of protection against
electrical shock:
Defibrillation-proof, Type BF
applied part
Fuse
Indicates fuse type
IPX1
Type IPX1
Degree of protection against
harmful ingress of water:
Drip-proof equipment
Symbol Name Description of Symbol
CE Label
Indicates that the product
complies with the requirements
of the Medical Device Directive
93/42/EEC June 1993.
If applicable, the 4-digit Notified
Body number is added near or
below the CE symbol.
Caution
Refer to accompanying documents
for further details.
UL Label
Declaration of conformity of the
equipment
WEEE
Disposal
European consumers are obliged
by law to dispose Waste Electrical
and Electronic Equipment (WEEE)
according to the WEEE Directive
2002/96/EC:
1. All electrical and electronic
waste must be stored, collected,
treated, recycled and disposed of
separately from other waste.
2. Consumers are obliged by law to
return electrical and electronic devices
at the end of their service lives to the
public collection points set up for this
purpose or point of sale. Details to
this are defined by the national law of
the respective country.
Note: By recycling materials or
other forms of utilizing old devices,
you are making an important
contribution to protecting our
environment.
Page 58

Symbol Name Description of Symbol
Audio
Paused/
Audio Off
Indicator
(On SDM front
panel)
LED yellow: Auditory alarm signals
paused for 1 or 2 minutes
LED flashes yellow: Auditory alarm
signals permanently switched off
(activated by pressing ‘AUDIO
PAUSED/AUDIO OFF Button’ > 3
seconds)
LED off: Auditory alarm signals
either active or permanently
switched off by setting menu
parameter ‘Alarm’ to OFF.
On/Off
Indicator
(On SDM front
panel)
LED green: SDM turned ON
LED off: SDM turned OFF
AC Power/
Battery
Indicator
(On SDM front
panel)
LED green: Connected to AC
power, battery fully charged
LED yellow: Connected to AC
power, battery charging
LED off: Not connected to AC
power (i.e. powered by internal
battery)
Note: The AC Power/Battery
Indicator functions irrespective
of the SDM being switched ON or
OFF.
Compressed
Gas
Warning safety sign to indicate the
product contains compressed gas
Page 59

Page 60

ADVANCING NONINVASIVE
PATIENT MONITORING
HB-005771-l ∙ Art. 100978
Date of release: 10/2018
 Loading...
Loading...