

Neurotherm NT-1100 Service manual
NEUROTHERM
RADIO FREQUENCY
LESION GENERATOR
MODEL NT 1100
jService Manual

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
1.0 CONTENTS
1.1 List of Figures .................................................................................................................. 3
2.0 WARNINGS AND CAUTIONS ......................................................................................... 2-1
3.0 INTRODUCTION AND APPLICABI
LITY OF THIS MANUAL ........................................... 3-1
3.1 Introduction and applicability of this manual ................................................................. 3-1
3.2 Summary of Equipment Revision Changes .................................................................. 3-2
3.3 Summary of Board Revision Changes ......................................................................... 3-3
3.3.1 Revision A – All Boards NT1100 .............................................................. 3-3
3.3.2 Revision B – Boards in rack ................................................................................. 3-3
3.4 Manual Updates ........................................................................................................... 3-4
3.4.1 Neurotherm Radio Frequency Lesion Generator Unit Manual Changes .............. 3-4
3.4.2 Record of Manual Updates carried out ................................................................. 3-5
4.0 GENERAL DESCRIPTION AND PRINCIPLE OF LESIONING ....................................... 4-1
4.1 Specifications ............................................................................................................... 4-1
4.2 Principles of Lesioning ............................................................................................... 4-11
4.2.1 The basic physical principles of radiofrequency ablation .......................................... 4-11
4.2.2 Pulsed radiofrequency ........................................................................................ 4-14
4.2.3 The Pulse Dose Concept. ................................................................................... 4-17
4.3 General Description .................................................................................................... 4-22
4.4 General Signal Information ......................................................................................... 4-23
4.5 Connector Panel Layout ............................................................................................. 4-29
4.6 Back Panel Layout ..................................................................................................... 4-30
5.0 DETAILED DESCRIPTION OF MODULES ..................................................................... 5-1
5.1 Power Entry Module, Isolation Transformer and Power Supply Board ........................ 5-1
5.2 Fuse Board ................................................................................................................... 5-3
6.0 CIRCUIT DIAGRAMS AND COMPONENT LISTS ........................................................... 6-1
6.1 Power Supply Board - RF100C .................................................................................... 6-2
6.2 Fuse Board – RF101D ................................................................................................. 6-5
6.3 Impedance Board –RF 102D ........................................................................................ 6-8
6.4 Stimulate Board RF103D + Sub Board ...................................................................... 6-13
6.5 RF Amplifier Board RF 104 C ..................................................................................... 6-19
6.6 RF Voltage and Current Metering Board RF 105C ..................................................... 6-24
6.7 Temperature Board RF106 D ..................................................................................... 6-29
6.8 Interlock Board RF107D ............................................................................................. 6-35
6.9 Connection Board RF109B......................................................................................... 6-41
6.10 Interface Board RF110D ............................................................................................ 6-44
6.11 Computer Mother Board RF111B ............................................................................... 6-47
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
1.1 List of Figures
Model NT1100
4.1
Output Power/Load Resistance Curve
4.2 Typical available Stimulate Output Voltage/Load Resistance
4.3 Fundamental Radiofrequency Circuit
4.4 Mechanism of Radio Frequency Heating
4.5 Schematic of Tissue Temperature v Distance from Electrode Tip
4.6 Increase in Lesion Size v Time
4.7 Typical Pulsed RF Signal
4.8 Frequency Spectrum of a 2Hz Rectangular Pulse
4.9 Frequency Spectrum of a 500 KHz Signal
4.10 Pulsed RF – Amplitude Control
4.11 Pulsed RF – Pulse Width Control
4.12 Pulse Dose
4.13 General Schematic of the Neurotherm NT1100
5.1 Power Supply Unit - Circuit Diagram
5.2 Fuse Board – Circuit Diagram
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
6.1 Power Supply Board - -RF100C - Circuit Diagram
6.2 Power Supply Board -RF100C - Component Layout
6.3 Fuse Board -RF101D - Circuit Diagram
6.4 Fuse Board -RF101D - Component Layout
6.5 Impedance Board -RF102D - Circuit Diagram
6.6 Impedance Board -RF102D - Component Layout
6.7 Stimulate Board -RF103D - Circuit Diagram
6.8 Stimulate Board -RF103D - Component Layout
6.9 RF Amplifier Board -RF104C - Circuit Diagram
6.10 RF Amplifier Board -RF104C - Component Layout
6.11 V/I Board -RF105C - Circuit Diagram
6.12 V/I Board -RF105C - Component Layout
6.13 Temperature Board -RF106D - Circuit Diagram
6.14 Temperature Board -RF106D - Component Layout
6.15 Interlock Board -RF107D - Circuit Diagram
6.16 Interlock Board -RF107D - Component Layout
6.17 Connection Board -RF109B - Circuit Diagram
6.18 Connection Board -RF109B- Component Layout
6.19 Interface Board -RF110D- Circuit Diagram
6.20 Interface Board -RF110D- Component Layout
6.21 Computer Motherboard -RF111B- Circuit Diagram – Bus
Interface
6.22 Computer Motherboard -RF111B- Circuit Diagram - Digital
Outputs
6.23 Computer Motherboard -RF111B- Circuit Diagram-Ribbon
Connectors and PSU
6.24 Computer Motherboard -RF111B- Circuit Diagram – Digital
Inputs
6.25 Computer Motherboard -RF111B- Circuit Diagram– Analog
Inputs
6.26 Computer Motherboard -RF111B- Circuit Diagram– Analog
Outputs
6.27 Computer Motherboard -RF111B- Component Layout
6.28 Front Panel Wiring
6.29 General System Schematic
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
2-1
2.0 WARNINGS AND CAUTIONS
Warning indicates a potentially harmful situation to yourself or others.
HAZARDOUS ELECTRICAL OUTPUT: The equipment is for use ONLY by
qualified medical personnel.
Do NOT under any circumstance perform any testing or maintenance on the
equipment while it is being used on a patient.
Do NOT use extension cords or adapters of any type. The power cord and plug
must be intact and undamaged.
Should the power cord or plug become cracked, frayed, broken of otherwise
damaged, it must be replaced immediately.
If the equipment has in any way suffered mechanical damage it should be
returned to the Supplier for Inspection and Test before further use.
Unplug the power cord before cleaning or service.
The operator should not perform any servicing of the equipment. Any servicing
should only be carried out by qualified personnel.
EXPLOSION HAZARD: Equipment not suitable for use in the presence of a
flammable anaesthetic mixture with air or with oxygen or nitrous oxide.
ELECTRIC SHOCK HAZARD: Always turn the equipment off before cleaning
and DO NOT allow ANY fluid to enter the ventilation holes or sockets.
ELECTRIC SHOCK HAZARD: Do not touch any exposed wiring or conductive
surface, while cover is off and the equipment is energised. The voltage present
when the electric power is connected to the equipment can cause injury or death.
Never wear a grounding wrist strap when working on energised equipment.
FUSE REPLACEMENT: For continued protection against fire hazard, replace
only with same type and rating of fuse as displayed on the rear Serial Number
Plate.
IMPROPER LINE VOLTAGE: The voltage selector on the mains input socket is
factory set and should not be changed by the user. The serial number plate
shows the correct mains input voltage for the machine and the rating of the fuses
to be used in the mains input fuse holder. An incorrect voltage setting may result
in Neurotherm malfunction and potential damage.
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
2.0 WARNINGS AND CAUTIONS (continued)
A CAUTION indicates a condition that may lead to equipment damage or
malfunction.
Servicing of the equipment in accordance with this service manual should never
be undertaken in the absence of proper tools, test equipment and the most
recent revision of this service manual which is clearly and thoroughly understood.
When repairing circuit boards, great care should be taken in handling boards as
all boards contain static sensitive devices. Before servicing a board, ground
yourself and the relevant tool to discharge any accumulated static charge by
wearing a wrist strap and placing the board on a static mat. If a board has to be
returned, use anti-static bags or containers.
The tests and repairs outlined in this manual should only be attempted by trained
personnel. Unauthorised service may void the warranty of the unit.
Check the voltage rating on the rear Serial Number Plate before connecting the
equipment to AC Mains Power. The equipment must never be operated at the
wrong mains voltage.
Use insulated tools when adjusting the internal controls on the equipment.
When cleaning the outer casing or display panel of the equipment do not use
abrasive agents or solvents.
To reduce risk of electrical shock do not remove back panel of generator. Refer
servicing to qualified personnel.
2-2
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
3.0 INTRODUCTION AND APPLICABILITY OF THIS MANUAL
3.1 Introduction and applicability of this manual
This service
required to maintain and repair the Neurotherm Radio Frequency Lesion
Generator Unit, Model NT1100. The main body of this manual deals
with the present production revision of the equipment. Differences
between equipment revision are summarised in Section 3.2. Section
3.3 lists the technical changes made to the equipment.
The revision of the whole equipment is changed if such technical
changes are made which make some spare parts incompatible with
earlier units. The initial equipment numbering, as shown on the rear
Serial Number Plate contains no revision letter (e.g. Serial No. NT11007020-05) however later revisions will contain a revision letter (e.g.Serial
No. NT1100-7020-05 Rev A). If the whole machine is upgraded such
that early machines cannot be easily amended, then the upgraded
machines will start from a nominated serial number as indicated in
Section 3.2.
Within the equipment, function units such as Printed Circuit Boards will
be changed or updated from time to time, these may or may not
introduce a revision of the whole equipment. Each printed circuit board
contains an identity number and a serial number of the board together
with the issue number - designated by a letter. The initial issue letter
was A for all Boards. In all cases the spare parts order code is also the
Board Identity Number and Issue Number (e.g. RF 102E).
In order to understand this manual it is necessary to have a complete
understanding of the function and operations of the Lesion Generator
Machine. This information can be obtained from the Operators Manual
which contains full operating instructions.
Manual (Document No. R1000) gives the information
3-1
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
3.2 Summary of Equipment Revision Changes
Initial production revision of this equipment – Model NT1100
Initial production DEC 2005
Start from
NT 1100 – 7007-05
From
NT1100 – 7150 – 06 (May 2006)
Metal Rack used and all cards in rack were changed to move components away
from guides
3-2
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
3.3 Summary of Board Revision Changes
3.3.1 Revision A – All Boards NT1100
Initial production revision of this equipment
Power Supply Board RF100C
Fuse Board RF101C
Impedance Board RF102C
Stimulate Board RF103C
RF Power Amplifier Board RF104C
RF Voltage and Current Board RF105B
Temperature Board RF106C
Interlock Board RF107C
Front Panel and Connection Board RF109B
Interface Board RF110C
Computer Motherboard RF111B
Card Rack Backplanes RF115A and RF116A
3-3
3.3.2 Revision B – Boards in rack
Fuse Board RF101D
Impedance Board RF102D
Stimulate Board RF103D
RF Voltage and Current Board RF105C
Temperature Board RF106D
Interlock Board RF107D
Interface Board RF110D
Card Rack Backplanes RF115B and RF116B
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
3.4 Manual Updates
3.4.1 Neurotherm Radio Frequency Lesion Generator Unit Manual Changes
This is the NT 1100 Manual applicable to the machines from serial numbers shown
below:-
Issue No. From Page Change Date
Serial No
NT1100 – 7007-05 As issued DEC 2005
2 NT1100 – 7150-06 JUNE 2006
3-4
Model NT1100
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
3-5
3.4.2 Record of Manual Updates carried out
Update Number Carried out by Name Date
2 Howard Clarke June 2006
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4.0 GENERAL DESCRIPTION AND PRINCIPLE OF LESIONING
4.1 Specifications
SIZE:
Width 400 mm (15 ¾”)
Height 300 mm (11 ¾”)
Depth 415 mm (16 ½”)
WEIGHT:
12.5 kg (28 lbs)
ELECTRICAL:
EUROPE 230 Volts 50Hz Fused 1 Amp on live and neutral
USA/CANADA 110 Volts 60Hz Fused 2 Amp on live and neutral
Voltage change via rear connector
Power Consumption 150 watts
The power supply is built to Class 2 standard. The mains transformer and all
mains related parts are doubly insulated from the Main Enclosure. The mains
transformer has separate isolated bobbins for mains and low voltage windings.
Thermal fuses (rated to fail at 125°C) are fitted into all primary and secondary
windings.
The machine is not connected to mains earth (class2).
STANDARDS:
This instrument complies with
EN60601-1:1997
IEC60601-1-2:1993
IEC60601-2-2:1998
IEC60601-2-10: With Canadian deviations
With respect to electrical shock, fire and mechanical hazards only in accordance
with UL60601-1, IEC60601-1, CAN/CSA C22.2 No.601.1 and IEC 60601-2-2
4-1
Morgan Automation Ltd June 2006

IMPEDANCE
STIMULATION MODE
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-2
Measuring frequency
Measuring source voltage Less than 500 mV AC
Measuring Display 50-2000 ohms (one ohm resolution)
Accuracy
Features (a) Internal 500 ohm Test Resistor
(b) Impedance in all Lesion Modes and in Stimulation
(c) Audible Tone available where frequency varies
(d) Warning on screen if impedance is less than 50
Signal Shape Biphasic square wave with negative edge leading.
Output Range Voltage
Current
Pulses Rates Motor 2 or 5 Hz (Default 2Hz)
Sensory 10,20, 50, 75, 100, 150, 180, 200 Hz (Default 50 Hz)
Pulse Rate Accuracy
Pulse Widths 0.1, 0.2, 0.5 and 1.0 mS (Default 1.0 mS)
Pulse width Accuracy
53KHz (± 3KHz)
±5%
Mode when stimulation is off
with impedance over full impedance range (502000 ohms). Audible tone is adjustable and
mutable.
ohms or greater than 2000 ohms.
This wave is available in a variety of frequencies and
widths.
0-5v ± 3% for motor frequencies (2Hz and 5 Hz)
0-3v ± 5% (Default) for all other frequencies
0-0.5v ± 10% for all other frequencies
0-10mA±5% 50-2000 ohms
0-6mA± 5% 50-2000 ohms
0-1mA± 5% 50-2000 ohms
± 3%
± 5% for 0.2, 0.5 and 1.0 mS
± 15% for 0.1mS
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
Features (a) Hardware and Software lockout if
voltage / current control not initially set
to zero.
(b) Warning on screen if stimulation control
is not initially at zero.
(c) Flashing LED on front panel indicates
machine is delivering stimulation pulses.
(d) Stimulation Test Socket is provided on
front of machine to interface with the
standard stimulation test kit.
(e) Various screen displays for displaying
amplitude of each
stimulation procedure.
LESION MODE
RF Waveform 480 KHz ± 5% Sinusoidal
Power Output Continuously variable. Maximum power output 30
watts ± 5% into 200 ohms. Power is displayed in
certain Lesion Modes.
Voltage Display on screen 0-99RF volts (RMS)
Current Display on screen 0-999RF milliamps (RMS)
Self Test 150 ohm dummy load resistor built into machine
Lamp Indicator LED flashes when Lesion Power is being delivered.
Temperature Range
Time
Selectable 50-90°C for Thermal Lesion (Default 80°)
Selectable in 5° C steps in initial screen set ups
Selectable in 1°C steps when in Lesion Mode using
“Temp up and Temp down” buttons.
Selectable 0:30 to 10:00 mins (Default 1:00 minute)
Selectable in 30 seconds steps in initial screen set
ups
Selectable in 1 second steps when in Lesion Mode
using “Time up and Time Down” buttons
Special Temperature Profiles A series of fixed temperature/time profiles are
programmed into the generator: P1, P2, P3. The
user can also program a custom profile with the
following characteristics:
Start Temperature 50-60°C (Default 50°C)
Step Time 00:10 to 3:00 mins (Default 2 mins)
Step Rise 1°C or 5°C (Default 5°C)
Final Temperature 65° - 90° C (Default 65°C)
Final Dwell Time 1:00–10:00 Minutes
(Default 4.00 mins
4-3
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
Lesion Start Lesion starts as soon as temperature is within 5°C of
desired temperature.
Auto Mode With Lesion Power Control off, the procedure can be
carried out under Automatic control by pressing the
“Auto start” button. The temperature will ramp up at
8°C per second and time will start when the
measured temperature is within 5°C of desired
temperature.
The lesioning can be stopped at any time by
pressing the “Auto Stop” Button.
Display
Temperature is displayed against time as a curve on
the screen together with a display of “Measured
temperature” and “Time to completion of lesion”. RF
Lesion power (or voltage and current) together with
impedance are also displayed.
Audible Indicator An alarm tone (with a volume adjustment) will
indicate the end of the procedure.
PULSE RF MODE
In pulsed mode the waveform is pulsed rather than continuous.
Pulse Widths 5ms, 10ms, 20ms, 50ms (default 20 ms)
4-4
Pulse Frequencies 1Hz, 2Hz, 5Hz, (default 2 Hz)
Temperature Range Selectable in 42-65°C range, (default 42°C)
Time Selectable 00:30 to 20:00 minutes
(default 2:00 mins)
Set Volts/ Current Pulsed RF can be carried out in Auto Mode at fixed
voltage or current.
Voltage range 30-70 Volts (default 45 Volts)
Current range 50-350 mA
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-5
PULSE DOSE MODE
In Pulse Dose Mode the numbers of Pulses of Pulsed RF are counted. Pulse Dose
Procedures are carried out in Auto Mode.
Set Temperature
Pulse Counts
Rate
Width
Set Voltage Range
Set Current Range
42°C
120-1200 count (Default 240 counts)
2Hz
20 mS
30-70V (Default 45V)
50-350 mA
MULTIPLE PROBES
The Neurotherm can be operated with 1,2 or 3 probes. When in Stimulation
Mode each probe is selected by the operator for Stimulation. In RF Lesion,
Pulse RF or Pulse Dose Mode the generator energises all connected probes
in a time interlacing method. In multiple probe operation not all pulse rates are
available.
Features (a) Hardware and Software lockout if RF Power
Control not initially set to zero.
(b) Warning on screen if RF Control is not
initially set to zero or if Auto is selected and
RF control is not off.
(c) LED Flashes on front panel to indicate
machine is delivering power.
(d) Three output sockets to accept a variety of
probes, (including cordotomy (optional
extra)) and enable multiple probe peration.
(e) Hardware lockout if temperature exceeds 95°C.
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
MAJOR FEATURES
Touch Screen Operation – User interface set up and software control via TP 400
processor.
Windows CE4.2. NET Operating System.
12.1” LCD Sceen with Back lighting and wide antiglare visibility.
Printer Support Via Bluetooth adaptor internally fitted.
Remote Mimic
Screen
Storage Device
Service Ports
Optically isolated running over CAT5 Cable to
External TFT screen up to 300 metres.
USB Memory Stick for downloading log files.
Only accessible by service engineers for keyboard +
mouse.
Any equipment connected to rear sockets must comply with IEC60950 and
IEC60601-1
Use only parts supplied by Neurotherm Ltd. Any other parts will void the warranty
and may cause danger to the patient.
4-6
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Earth Leakage
1 Enclosure leakage current
Normal 40 microamsps 100 microamps
Reverse 40 microamsps 100 microamps
Single fault condition
Normal 40 microamsps 500 microamps
Reverse 40 microamps 500 microamps
2 Patient leakage current
Normal (AC) 5 microamps 100 microamps
Reverse (AC) 4 microamps 100 microamps
Single fault condition
Normal (AC) 7 microamps 500 microamps
Reverse AC) 7 microamps 500 microamps
3 Patient Leakage current
Normal (DC) 4 microamps 10 microamps
Reverse (DC) 4 microamps 10 microamps
Single fault condition
Normal (DC) 4 microamps 50 microamps
Reverse (DC) 4 microamps 50 microamps
4 Patient Auxiliary Leakage Current
Normal (AC) 4 microamps 100 microamps
Reverse (AC) 4 microamps 100 microamps
Single Fault Condition
Normal (AC) 6 microamps 500 microamps
Reverse (AC) 6 microamps 500 microamps
5 Patient Auxiliary Leakage Current
Normal (DC) 4 microamps 10 microamps
Reverse (DC) 4 microamps 10 microamps
Single Fault Condition
Normal (DC) 4 microamps 50 microamps
Reverse (DC) 4 microamps 50 microamps
6 Patient Leakage Floating Type
Normal 27 microamps 5000 microamps
Reverse 27 microamps 5000 microamps
Single Fault Condition
Normal 36 microamps 5000 microamps
Reverse 35 microamps 5000 microamps
4-7
Model NT1100
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Environmental Conditions
7 Transport
8 Storage Temperature
9 Operating Temperature
Model NT1100
Temperature
Humidity
Pressure
Humidity
Pressure
Humidity
-10°C to 70°C
0-95%RH
140-760mmHg
10°C to 60°C
10 to 80% RH
520-760mmHg
10°C to 40°C
10 to 80% RH
4-8
Non-Condensing
(0-12,200 metres)
(0-40, 000ft)
(0-3000 metres)
(0-10,000ft)
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-9
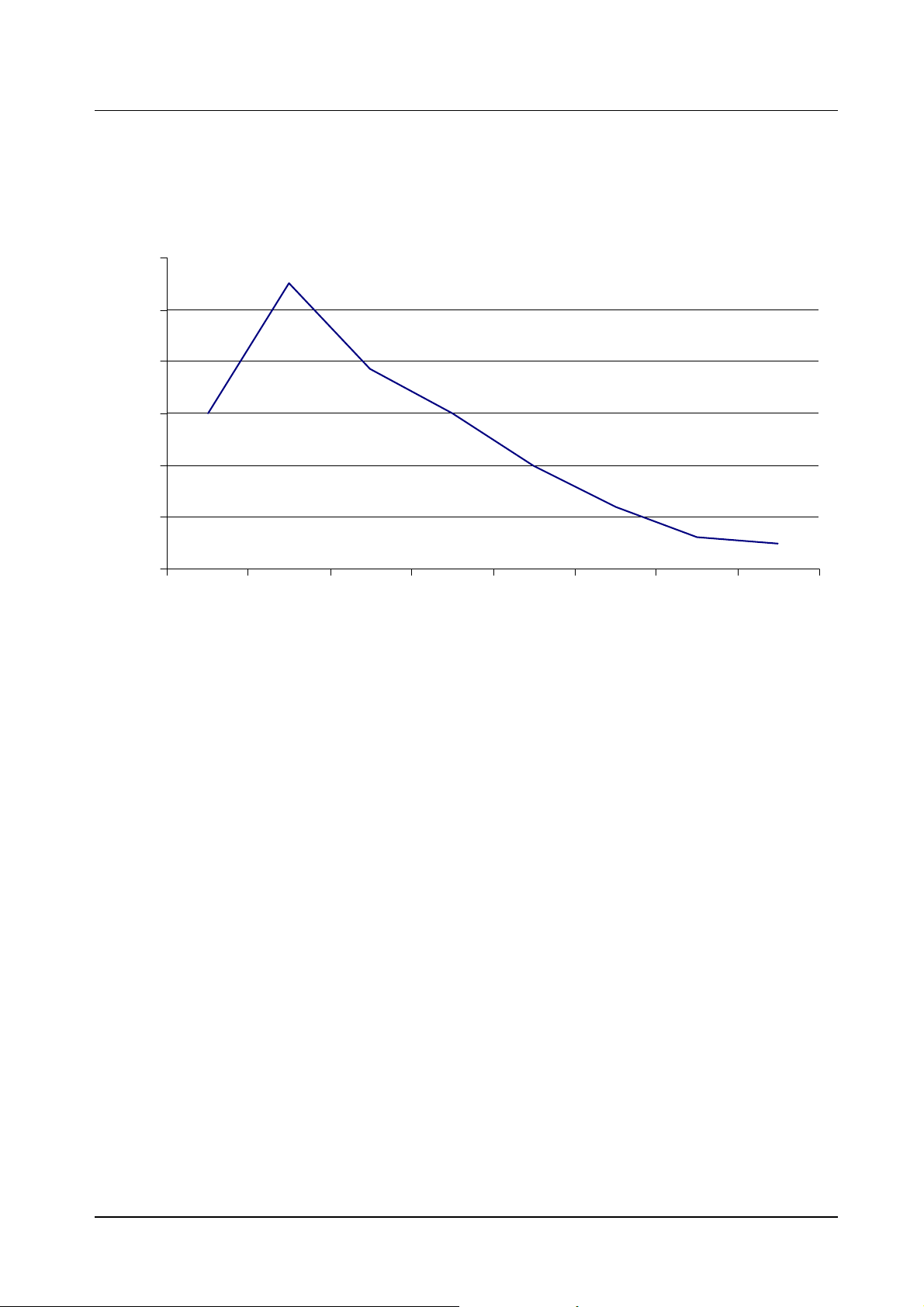
Figure 4.1 Output Power/Load Resistance Curve
60
50
40
30
Wattage
20
10
0
50 100 150 200 300 500 1000 1200
Impedance
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-10
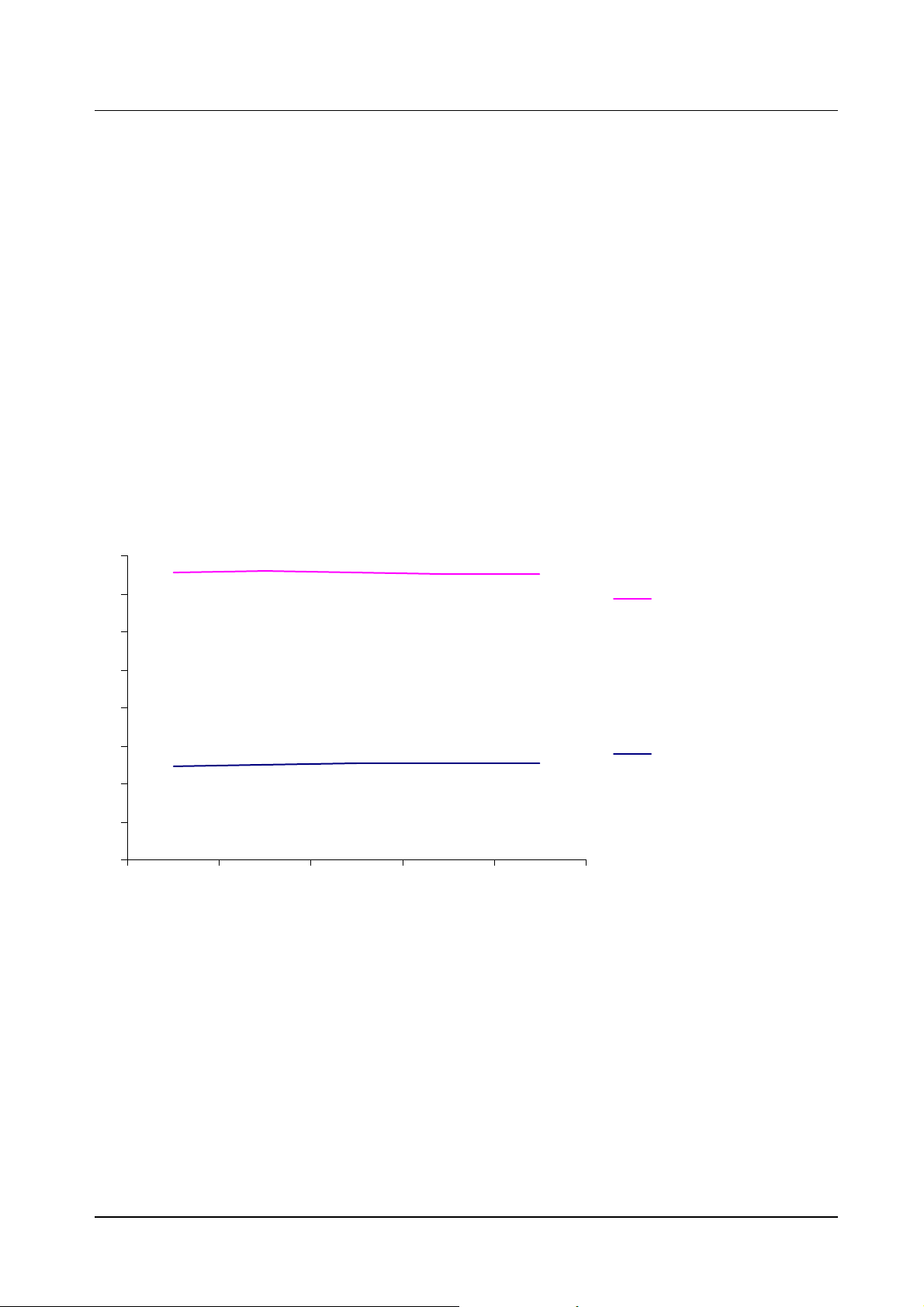
Figure 4.2 Typical available Stimulation Output Voltage / Load Resistance and
Stimulate Output Current/Load Resistance
Load Resistance
0
100 4.88 10.2
200 4.98 10.2
500 5.04 10.1
1000 5.05 10
2000 5.07 9.84
Stimulate Output Voltage
(5v Constant Voltage)
Stimulate Output Current
(10mA Constant Current)
16
14
12
10
Stimulate Output
Current
8
6
4
Stimulate Output
Voltage
2
0
100 200 500 1000 2000
Load Resistanc e - Ohms
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4.2 Principles of Lesioning
4.2.1 The basic physical principles of radiofrequency ablation
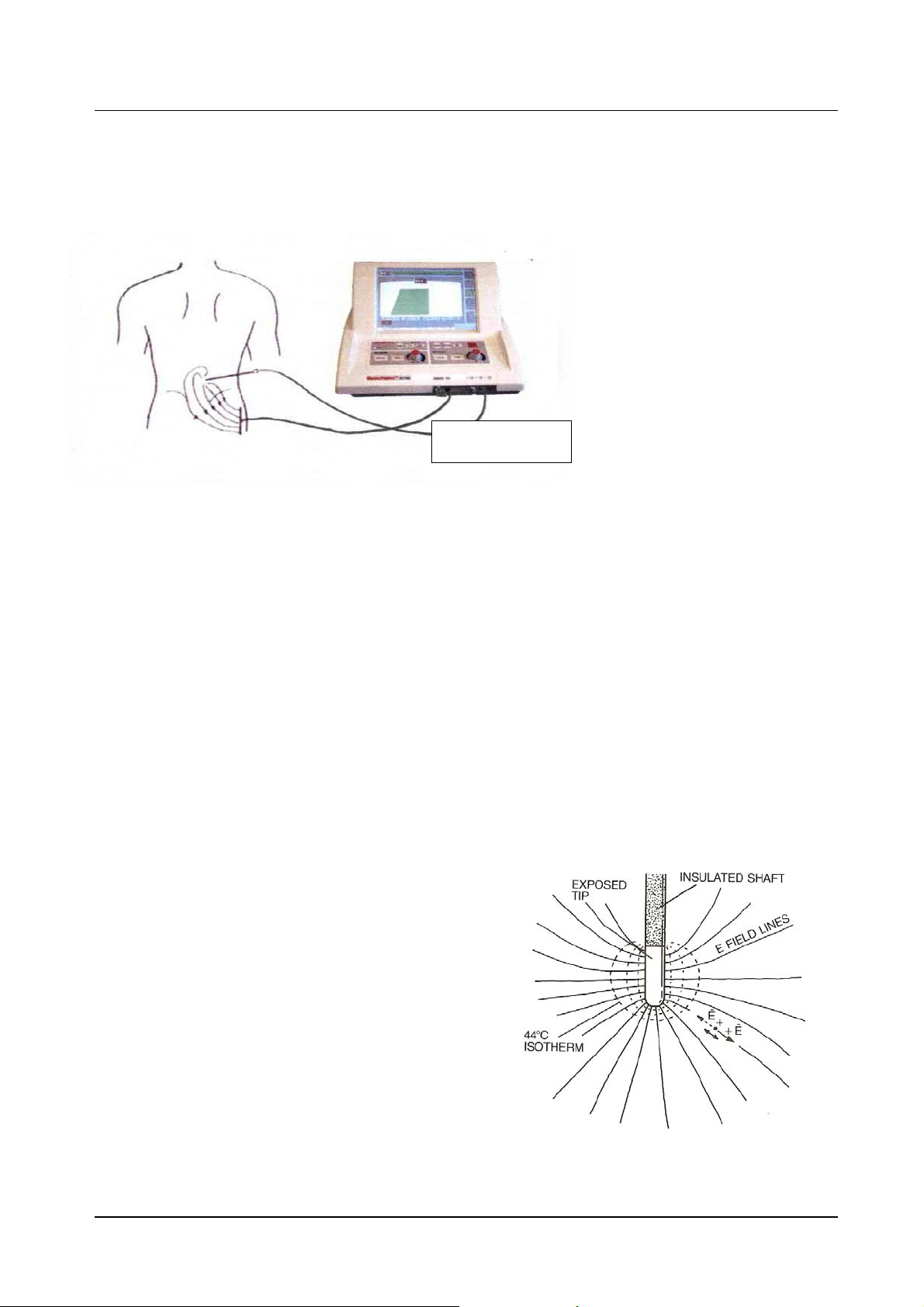
Figure 4.3 shows the
fundamental radiofrequency
circuit. The RF lesion generator
or power source provides a
source of RF. It is connected by
wires to 2 electrodes: one
inserted into the body, referred
to as the active electrode;
another in contact with the
Figure 4.3 Fundamental
surface of the body, referred to
as the dispersive electrode. This
is the so-called monopolar
configuration. The RF voltage
causes current to flow through the wires, through the electrodes, and to the patient’s body. The
patient's body is a conductive electrolytic media, and thus the patient’s body becomes part of the
RF circuit. This current spreads out from the electrodes and flows through the electrolytic tissue
medium of the body. The active and dispersive electrodes have a similar physical role in
delivering and receiving the current, but functionally, because of their differing areas, they have
very different effects with regard to the RF heating process.
The active electrode with its smaller surface area has much higher field densities in the
tissue adjacent to it. This higher field density causes significant heating near the active
electrode surface. The dispersive electrode has a much larger area, and, as a
consequence, the field density is much lower in the tissue adjacent to it. This results in a
lower radiofrequency heating effect, and thus if the dispersive electrode is large enough
no appreciable heating will occur near it. In fact, a large area surface plate to join to the
skin with a conductive gel for good conductivity will not heat appreciably even though this
same radiofrequency current will cause intense heating near the much smaller active
electrode. It is recommended for most radiofrequency procedures that the dispersive
electrode, therefore, should have an area of greater than 150 square centimeters to be
safe from any significant heat elevation when RF lesions delivering 50 watts or less are
used.
The mechanism for radiofrequency
heating is shown in figure 4.4. The
electric field lines emanate from the
active electrode tip and are created by
the voltage impressed upon it by the
radiofrequency generator. This electric
field creates an electric force on the
charged ions within the electrolytic
medium of the tissue. According to the
physics laws this force produces a
motion, and the motion is oscillatory at
the frequency of the RF current.
4-11
Figure 4.4 mechanisms for
Radiofrequency heating
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-12
It is this radiofrequency motion which causes the ions to rub against the surrounding fluid
medium, causing friction which results in the tissue heating. The temperature at any point is
controlled by the frictionally induced power dissipation at that point, mediated by thermal
diffusion and thermal convection. The thermal diffusion and convection are typically caused by
blood circulation.
The temperature distribution around the electrode tip can be calculated by making certain
simplifying assumptions. One of the assumptions is that the medium is homogeneous and
that the factors of thermal diffusion and circulation are also uniform. Under these
circumstances one can calculate the isotherms (surfaces of constant temperature)
surrounding the electrode tip for a given impressed radiofrequency voltage. These
isothermal surfaces are critical to determining the lesion size. As it is known that living
tissue will be permanently destroyed for sustained temperatures of approximately 45 C, the
45 degree isotherm can be considered to be the outer border of the lesion since tissue
within this volume will be thermally destroyed and tissue outside of this volume will
experience lower temperatures than are necessary for cellular destruction. Isothermal
surfaces are indicated by the -- lines in figure 4.4
It is important to understand that the radiofrequency field, and thus power dissipation in the
tissue actually heats the tissue as opposed to the electrode itself. The heated tissue in turn
raises the temperature of the electrode tip and thus heats the tip. Therefore, it is not the
electrode tip which heats the tissue, but rather the tissue which heats the electrode tip. If
the electrode is properly designed so as not to sink away too much of the thermal energy,
the electrode will give an accurate representation of the tissue temperature at its surface. It
is for this reason that thermal monitoring of the radiofrequency tip is a good indication of the
hottest portion of the lesion volumes, namely the isotherm that lies closest to the surface of
the electrode. With the simplifying assumptions of a homogeneous medium, the lesion size
represented by the 45 degree isotherm increases with increasing tip temperature and also
increases with increasing tip dimension particularly the radius of the electrode tip.
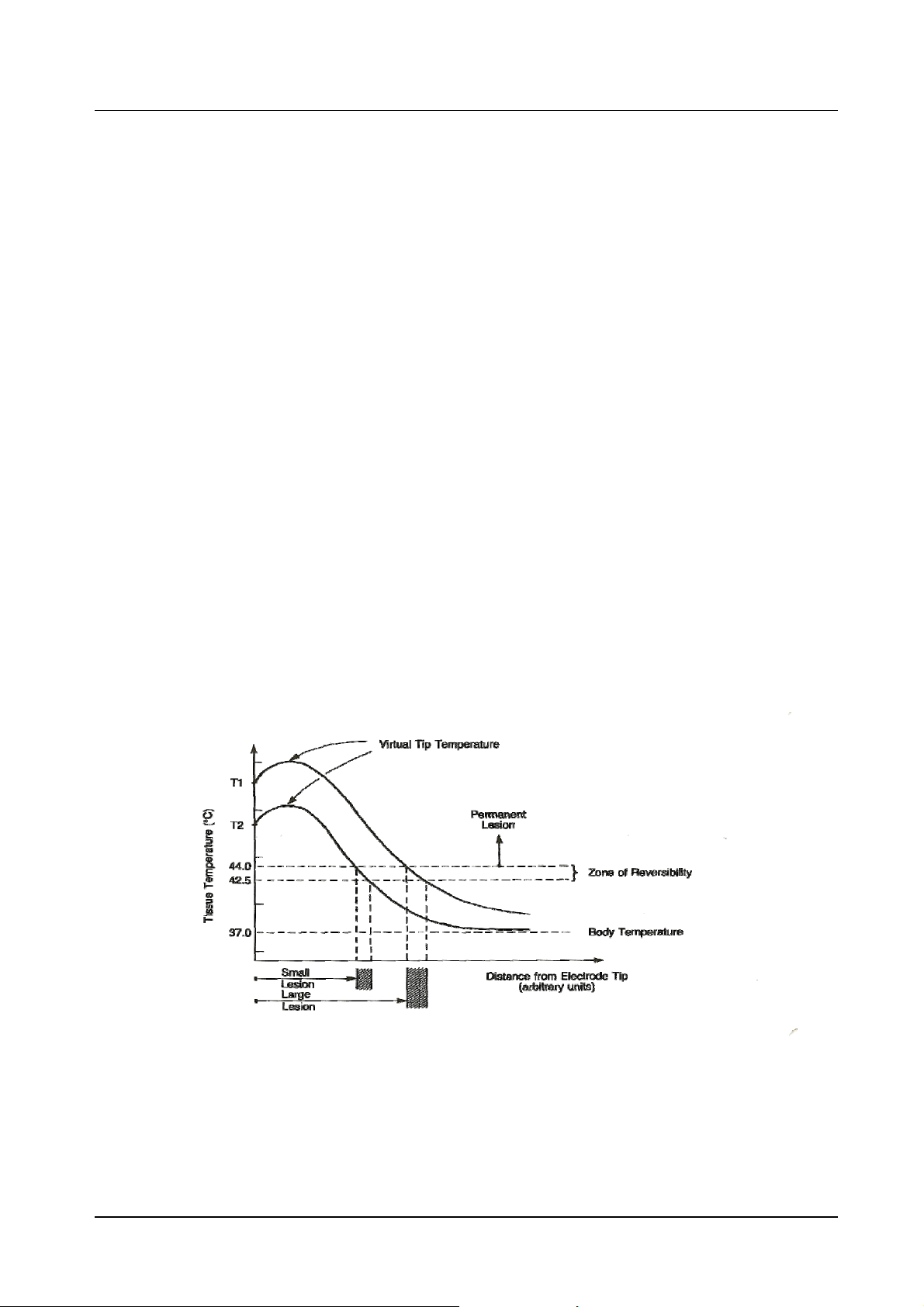
Figure 4.5 Schematic of Tissue Temperature v Distance for Electrode Tip.
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-13
Figure 4.5 shows a schematic diagram of the temperature of the tissue as a function of
distance from the electrode tip. It should be noted that the temperature is not isotropic for
a non-spherical electrode, and thus these curves may differ at different orientations on a
non-spherical electrode tip. The temperature at the surface of the electrode, such as T2,
measures very nearly the hottest tissue nearby, and the tissue at greater distances falls
off until it asymptotically approaches body temperature at large distances from the
electrode tip. By raising the radiofrequency voltage, one will increase the temperature to
T1 near the electrode tip, and thus the distances to the 45 C isotherm will increase
accordingly. With knowledge of these characteristics and the temperature vs.distance
curve, one can therefore judge the size of the lesion volumes by choosing the appropriate
tip temperature for a given tip geometry. This is the reason temperature measurement
has been historically essential to produce consistent and quantified lesion volumes.
Measurement of the tip temperature has another very important benefit. By avoiding tip
temperatures near 100 C (the temperature at which water boils), one avoids the undesired
effects of charring, sticking or the formation of a hemorrhage or explosive gas which may
be also be accompanied by sparking. In the early days of neurosurgical lesions, before
reliable tip temperature measurement was possible, neurosurgeons would establish the
end point of their lesion making by listening for the “popping” lesion. The popping was
caused by the tip temperature exceeding 100 C and the subsequent gas formation at the
tip to the electrode. This obviously was not a controlled lesion technique and led to
unpredictable and dangerous destructive conditions.
In pain management there are now well-established prescriptions for appropriate
electrode size and tip temperature to achieve desired lesion volumes. It has been
historically clear that prescriptions which involve power and current did not have lasting
value, but rather prescriptions that involve temperature, electrode size and accounting for
the heat washout caused by blood flow. The importance of temperature control was not
always recognized. For instance, in the early days of percutaneous cervical cordotomy,
elaborate prescriptions of current, power and time for making RF lesions were
established. The subsequent clinical results were not consistent in the early days of
cordotomies, and it was only when temperature was measured at the tip of the cordotomy
electrode that consistency and reproducibility was finally achieved.
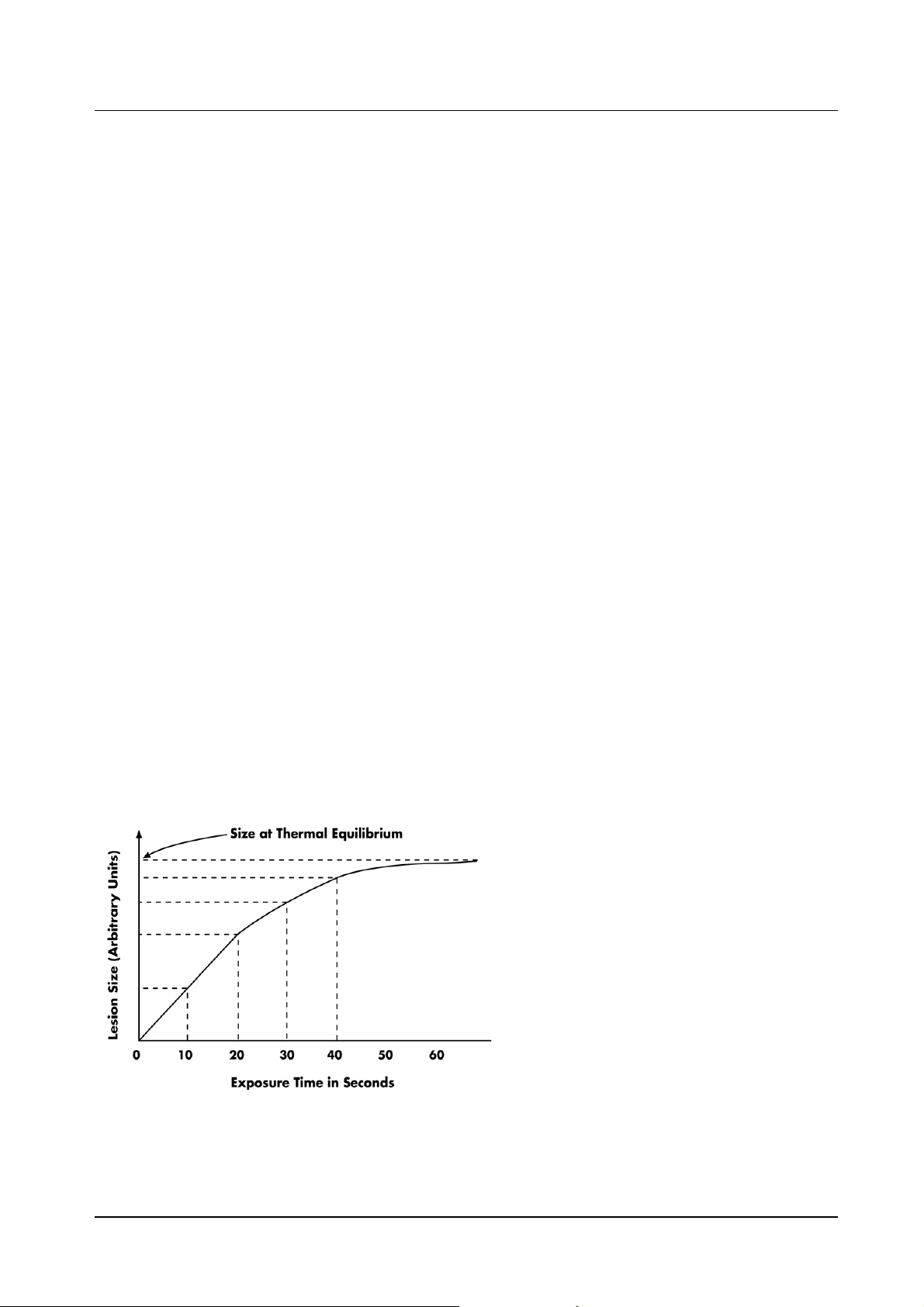
Another important aspect of controlled
radiofrequency lesion making is illustrated
in Figure 4.6. This shows experimental
data of the increase in lesion size for a
fixed electrode geometry and a fixed tip
Figure 4.6 Increase in Lesion Size v Time
temperature. The lesion size in this
situation is defined as the width of the
prolate ellipsoidal width of the prolate
ellipsoidal lesion volume. The graph
clearly shows that for constant tip
temperature the lesion size grows and
asymptotically reaches a maximum value
in a time between 30 and 60 seconds.
The 45C isothermal surface can then be
referred to as the equilibrium lesion size.
Leaving the radiofrequency power turned
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-14
on indefinitely beyond 60 seconds will not increase the equilibrium lesion size. In the past,
so-called time-dependent lesions were made in which a certain power was held by the
radiofrequency generator for 10-20 seconds. This too led to inconsistent results, and
resulted in the acknowledgment of the equilibrium lesion size as being the optimum
methodology.
It is noteworthy that impedance monitoring has a great value in assessing the progress of
a heat lesion. The impedance seen by the electrode tip depends on tissue interfaces and
this property has been used very effectively to distinguish between the interface of
electrolytic fluids and tissue. For example this has been used with percutaneous
cordotomy electrodes to clearly tell when the electrode has traversed from the cerebral
spinal fluid to a position of contact with the spinal cord. Impedance monitoring has also
been used to identify when an advancing electrode has progressed from the annulus of
the disk into the nucleus pulposus. The change of impedance during the heating process
is dramatic. It has been shown that as the tissue or medium heats up, the impedance will
drop. This is very much related to the phenomena that the engine oil in an automobile will
become less viscous as the temperature of the engine increases. There is a point,
however, as the temperature at the lesion tip approaches 100 C, when the impedance will
cease to decrease and, in fact, will rise precipitously as the temperature approaches the
boiling point. The reason for this is that the protein coagulation has a rapid onset in this
temperature range causing a decrease in Ionic mobility. Near the boiling point, gas
suddenly forms around the electrode tip, acting as an electrically insulating barrier thus
sending the impedance to very high levels. At the onset of boiling, the impedance rises
very rapidly. In summary, it is clear that the monitoring of temperature and impedance are
both of great significance.
4.2.2 Pulsed radiofrequency
Historically, radiofrequency was neuroablation. This was true for percutaneous
cordotomy, the treatment of trigeminal neuralgia, and the destruction of the medial branch
nerve for facet pain. Mysteries remained however. It was not understood why RF lesions
were so often followed by long periods of discomfort before any beneficial clinical effect
appeared. In the 1990s, additional unanswered questions were added. The mode of
action of RF lesions of the lumbar sympathetic change (other than for vascular disease)
was not understood since there were acceptable success rates, though the results did not
correlate with the degree of sympathetic block.
This led to the hypothesis by Sluijter that heat might not be the element causing the
clinical effect of an RF lesion. The next obvious steps were to define a method to apply
radiofrequency at high intensity without allowing the tip temperature to rise to
neurodestructive levels. The method that was chosen by Sluijter was placing the output
setting of the RF generator in the same range as was customary for making heat lesions
but interrupting the output, thus allowing for sufficient time for the generated heat to be
washed away by thermoconductivity and circulation.
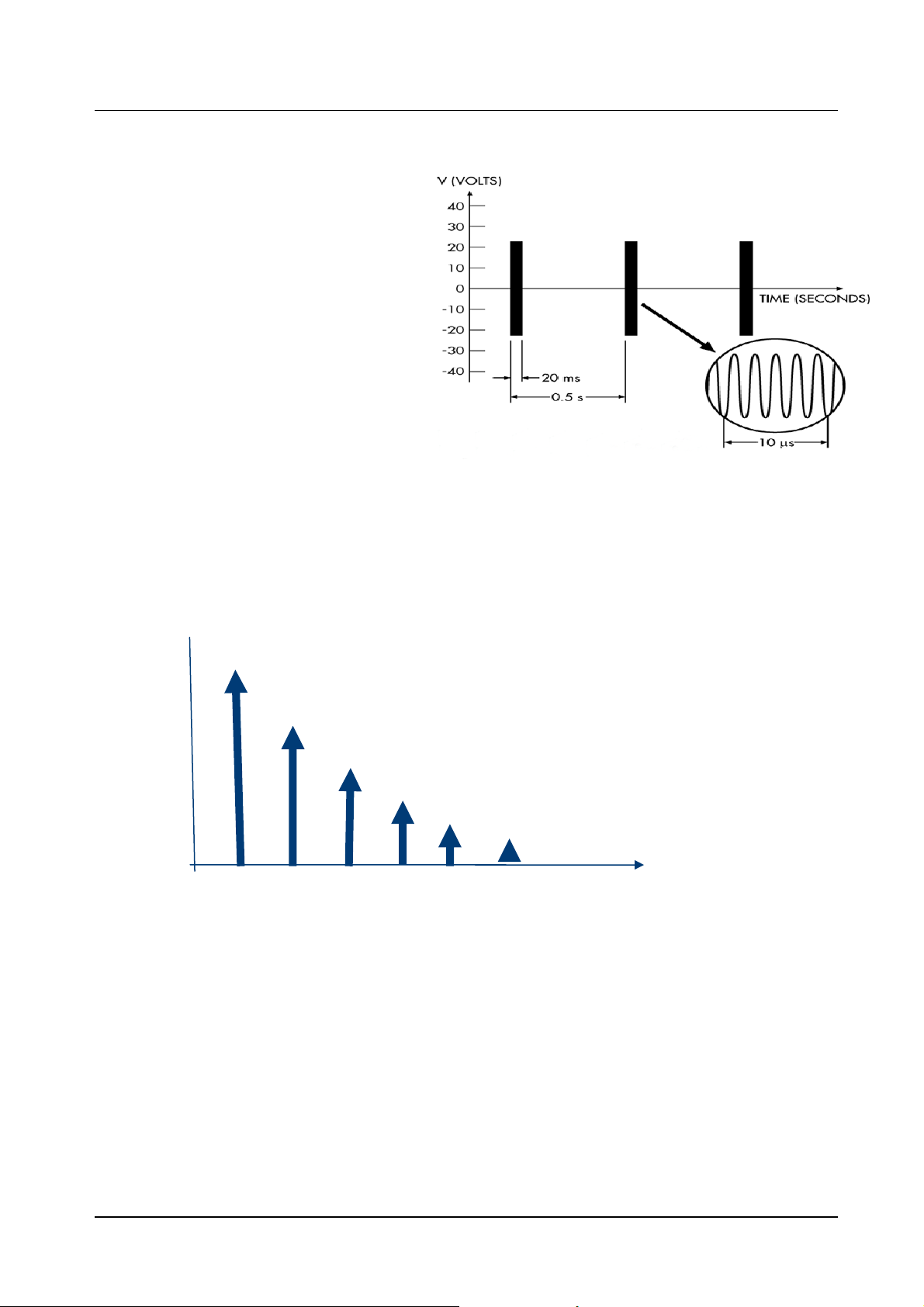
This method has been commonly referred to as pulsed radiofrequency (PRF). Pulsed
radiofrequency is a relatively new technique that applies short pulses of radiofrequency
(20 ms) at a high voltage of 45 to 60 volts to neural tissue. Figure 4.7 shows the currently
accepted paradigm of 20 milliseconds of RF followed by 480 milliseconds of off time. In
this way high intensity radiofrequency is delivered but with a short enough on time so as
not to
cause heating above 42 C.
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-15
It is a natural reaction to think of pulsed radiofrequency as being analogous to the neural
modulation effects achieved using spinal cord stimulators or TENS units. However, these two
modalities are very different. In neural modulation the therapeutic effect is achieved by applying
low frequency (< 1000Hz) rectangular pulses.
Figure 4.7 Typical Pulsed RF Signal
Strength
2 4 6 8 10 12 Frequency Hz
Figure 4.8 Frequency Spectrum of a 2Hz Rectangular Pulse.
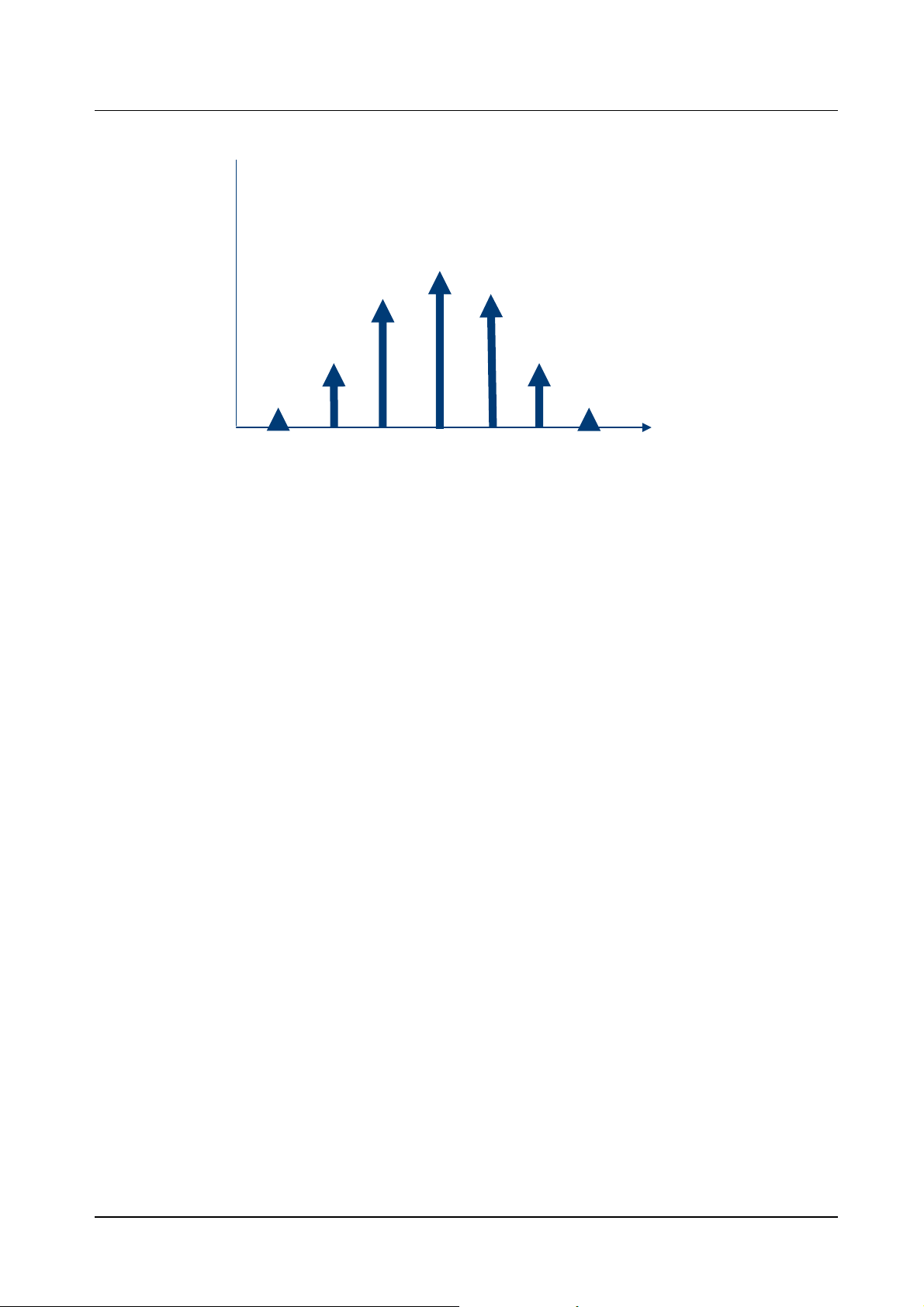
Figure 4.8 shows the frequency spectrum of a two Hz rectangular pulse. As can be seen from
the figure, the major frequency component is at two Hz and falls off as the frequency increases.
At frequencies above 1000 Hz, the amplitude of the frequency component is getting very small.
There is a very different situation with pulsed radiofrequency. In this case, the rectangular pulses
have radiofrequency inside of them. This changes the frequency spectrum entirely. As can be
seen from figure 4.9, the major frequency component is now 500 kHz and decreases at higher
and lower frequencies. At frequencies below 1000 Hz, the contribution can be shown to be
negligible. In conclusion, the frequency spectrums of pulsed radiofrequency are entirely different
than the frequency spectrums of low frequency stimulators.
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-16
Strength
500 kHz frequency Hz
Figure 4.9 Frequency Spectrum of a 500KHZ Signal.
There is very little conclusive research to date on the mode of action of PRF. A few
preliminary studies have shown that a modification of CFOS and DNA expression has
been observed in cells of rat DRG after exposure to PRF. However, additional basic
research needs to be done to come to any good scientific conclusion as to the mechanism
of action of PRF.
In this era of evidence based medicine, pulsed radiofrequency has not yet been validated.
Several retrospective studies and audits have been conducted and the initial results are
positive. Because of a lack of uniform treatment guidelines, the anecdotal results for
pulsed have ranged from magnificent to abysmal. It is this author's belief that
standardization of many of the PRF parameters will at worst result in uniform treatment for
all patients and at best significantly improve the clinical outcomes. In any case, controlled
clinical studies are long overdue for this potentially promising modality.
When the study of PRF began, the parameters were arbitrary. For the voltage, a value is
taken that was within the range of the voltage during the initial heating phase of an RF
heat lesion. The values of 20 milliseconds on time and 480 milliseconds off time were
chosen because they were thought to provide good conditions for preventing heating
above 42 degrees Centigrade. The initial choice of 120 second duration of the procedure
was completely arbitrary, and it was just taken as a starting point. With no scientific basis,
these parameters have been arbitrarily modified by clinicians and thus there is no
consensus as to what the optimum parameters are.
One of the major variables in pulsed radiofrequency treatment is the voltage level when
the pulses are “on”. This arises from the desire to keep the temperature below 42
degrees C. If 42 degrees C. is reached, it is necessary to either manually or automatically
reduce the pulsed amplitude or the pulsed duration in order to ensure the temperature
does not exceed 42 degrees. Using the pulsed dose method, every pulsed is ensured to
be of the same amplitude and duration. This method is explained in detail in the following
paragraph.
Morgan Automation Ltd June 2006

Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-17
4.2.3 The Pulse Dose Concept.
Whenever Pulsed RF is used, if the selected temperature limit is reached, the pulse must
be modified in some way to prevent the selected temperature limit from being exceeded;
this can be done by either.
1. Modifying the pulse amplitude of the pulses- i.e. if a 45 volt amplitude was set, and if
the temperature limit was set to 42 degrees and was reached, the next pulses will be
reduced in voltage to prevent the temperature from increasing above the 42 C
temperature limit.
2. Modifying the pulse width whenever the temperature limit was reached, thus insuring
that each pulse delivered was the full set voltage amplitude.
In Pulse dose the two conditions shown above are avoided. A FULL pulse is always
given, i.e. if the setting is 45 volts amplitude for 20 milliseconds, you will always deliver
this pulse amplitude and duration. If the set temperature limit is reached, the generator
will wait until the temperature drops below the set temperature limit, and then again will
give a FULL amplitude and duration pulse.
Because the generator is only delivering full pulses, in this mode initially one sets the
“number of pulses” that is desired for the procedure as opposed to procedure time, since
procedure time can vary depending on whether the set temperature limit was reached.
The following diagrams depict the different modes-
Morgan Automation Ltd June 2006
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
Figure 4.10 Shows Historical Pulsed RF amplitude control
Figure 10.8
Figure 4.10 Pulse RF Amplitude Control
The beginning pulses are the desired pulses of 45 volts amplitude and 20 ms duration.
Note that the moment the set temperature limit is reached the voltage is changed
(reduced) in order to keep the temperature below this limit. (Note that this implies that
every patient gets unpredictable and variable pulse amplitude which is undesirable).
4-18
Morgan Automation Ltd June 2006
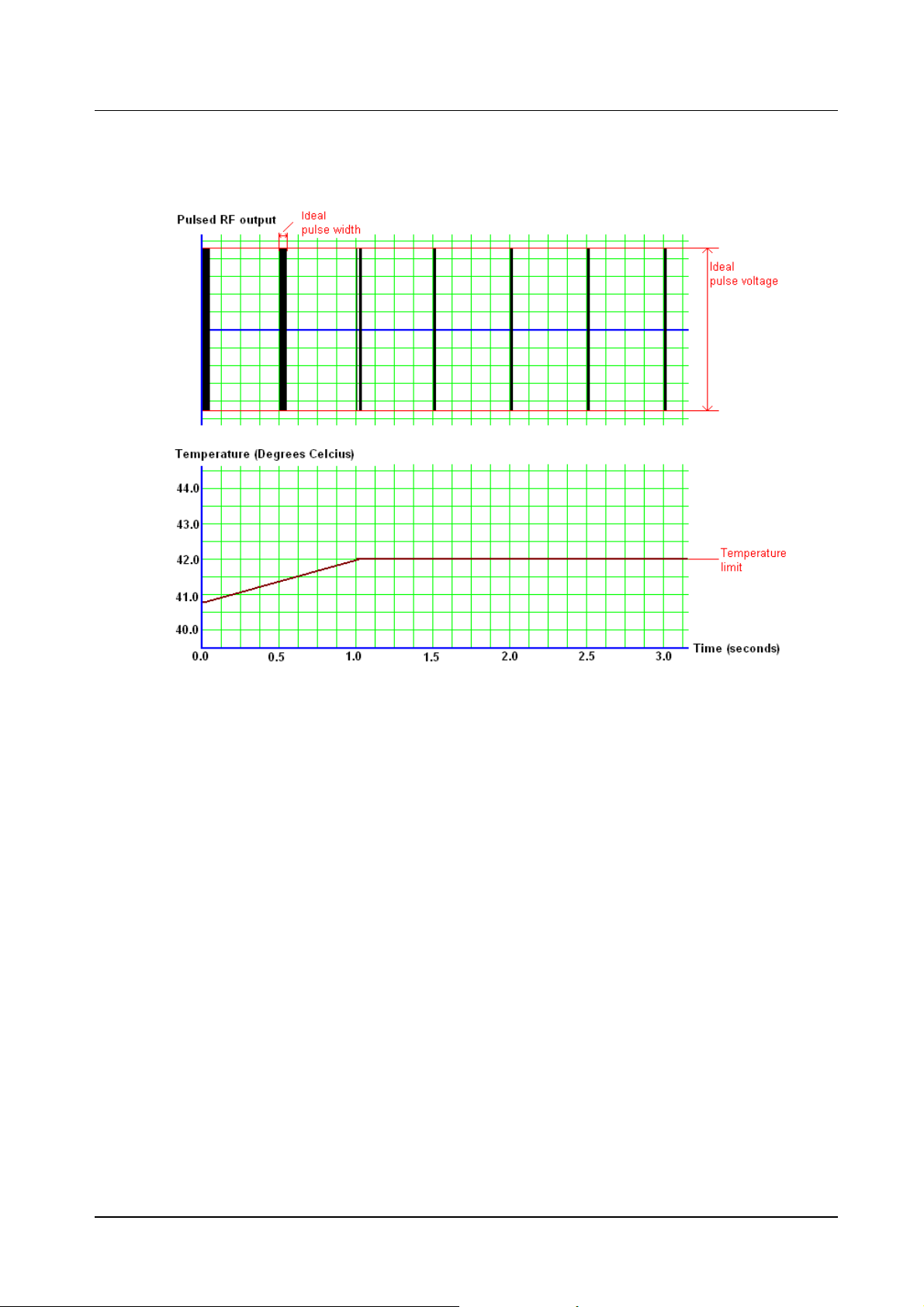
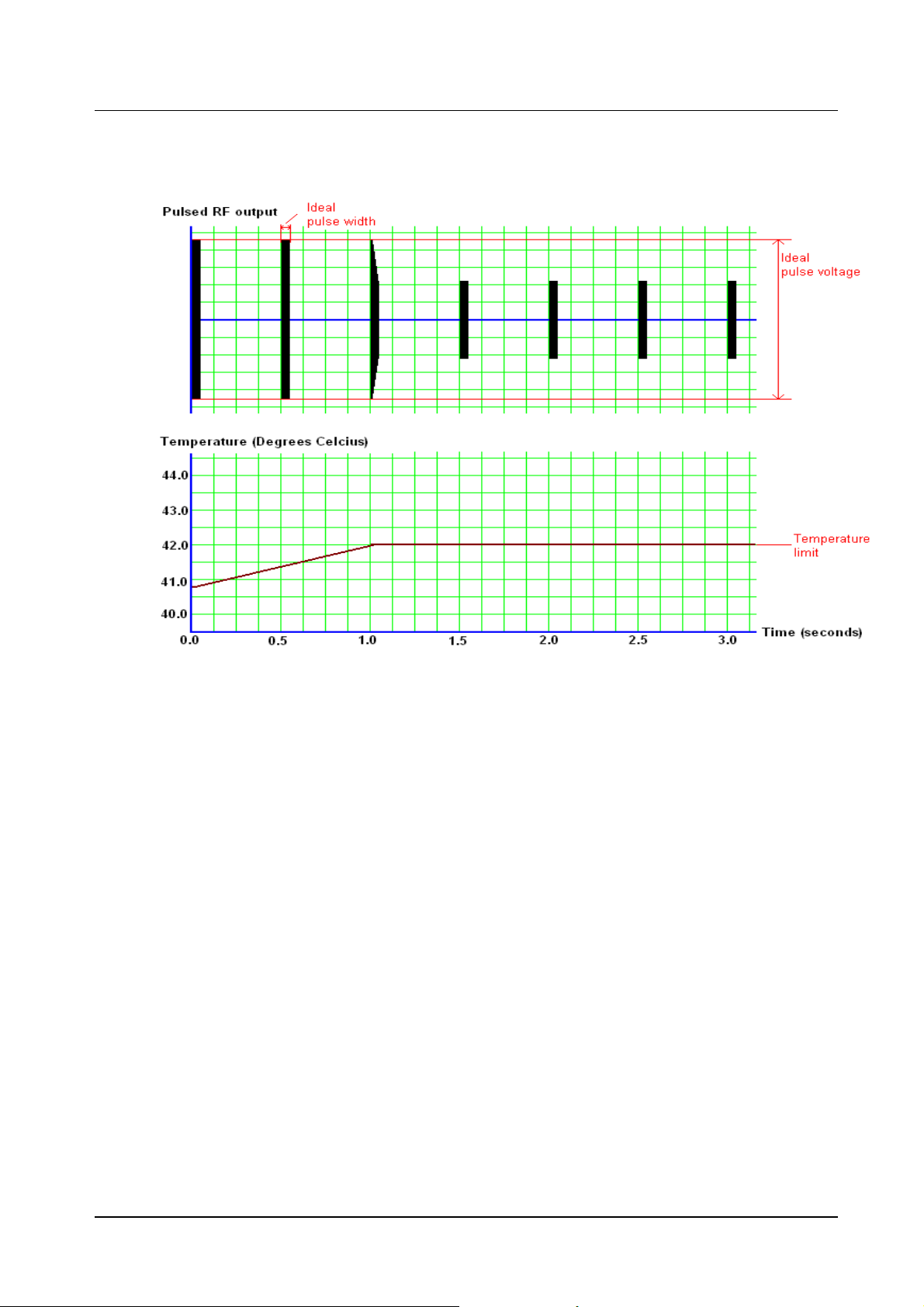
Figure 4.11 Shows Historical Pulsed RF – pulse width control
When the temperature limit is reached the pulse width is changed as opposed to the
pulse amplitude. Note that the pulse width is changed the moment the temperature limit
is reached, the width is varied to keep the temperature limit. Though this is better than
amplitude control, it still implies that treatments will not be consistent and uniform
between patients.
Neurotherm Radio Frequency Lesion Generator Service Manual
Model NT1100
4-19
Morgan Automation Ltd June 2006
 Loading...
Loading...