

Page 1

HANCOCK
®
Apical Left Ventricle Connector
Embout apical pour ventricule gauche
Apikaler linksventrikulärer Konnektor
Conector apical para el ventrículo izquierdo
Apicale connector voor het linkerventrikel
Connettore apicale per ventricolo sinistro
Apikal kobling for venstre ventrikkel
Apikaalinen vasemman kammion liitin
Apikal vänsterkammarkonnektor
Διακορυφαίος σύνδεσμος αριστερής κοιλίας
Apikale venstre ventrikel-konnektor
Conector apical ventricular esquerdo
Instructions for Use
Instrucciones de uso
Bruksanvisning
Brugsanvisning
■
Mode d'emploi ■ Gebrauchsanweisung ■
■
Gebruiksaanwijzing ■ Istruzioni per l’uso ■
■
Käyttöohjeet ■ Bruksanvisning ■ Οδηγίες χρήσης ■
■
Instruções de utilização
Caution: Federal law (USA) restricts this
device to sale by or on the order of a physician.
Page 2

Page 3

Explanation of symbols on package labeling / Explication des symboles des étiquettes sur
l'emballage / Erläuterung der Symbole auf dem Verpackungsetikett / Explicación de los símbolos
que aparecen en el etiquetado del envase / Verklaring van de symbolen op de verpakkingslabels /
Spiegazione dei simboli sulle etichette della confezione / Forklaring av symboler på produktet og
pakningen / Pakkauksen merkintöjen selitykset / Förklaring av symboler på
förpackningsetiketten / Επεξήγηση των συμβόλων στη σήμανση της συσκευασίας / Forklaring på
symboler på emballagens mærkater / Explicação dos símbolos nas etiquetas da embalagem
Conformité Européenne (European Conformity). This symbol means that the
device fully complies with European Council Directive 93/42/EEC. / Conformité
Européenne. Ce symbole signifie que le dispositif est entièrement conforme à la
Directive européenne 93/42/CEE. / Conformité Européenne (Europäische
Konformität). Dieses Symbol besagt, dass das Gerät allen Vorschriften der
europäischen Direktive (93/42/EWG) entspricht. / Conformité Européenne
(Conformidad Europea). Este símbolo indica que el dispositivo cumple
totalmente la Directiva Europea 93/42/CEE relativa a los productos sanitarios. /
Conformité Européenne (Europese Conformiteit). Dit symbool betekent dat het
apparaat volledig voldoet aan de Europese Richtlijn 93/42/EEG. / Conformité
Européenne (Conformità europea). Questo simbolo indica che il dispositivo è
conforme alla Direttiva del Consiglio europeo 93/42/CEE. / Conformité
Européenne (samsvar med europeisk standard). Dette symbolet betyr at
enheten er fullstendig i samsvar med EU-direktiv 93/42/EØF. / Conformité
Européenne (eurooppalainen vaatimustenmukaisuus). Tämä symboli tarkoittaa,
että laite on kaikilta osin Euroopan unionin neuvoston direktiivin 93/42/ETY
mukainen. / Conformité Européenne (EU-standard). Denna symbol betyder att
enheten helt följer rådets direktiv 93/42/EEG. / Conformité Européenne
(Eυρωπαϊκή Συμμόρφωση). Το σύμβολο αυτό σημαίνει ότι το προϊόν
συμμορφώνεται πλήρως με την Oδηγία του Ευρωπαϊκού Συμβουλίου 93/42/
ΕΟΚ. / Conformité Européenne (Europæisk Standard). Dette symbol betyder, at
enheden fuldt ud overholder det Europæiske Råds Direktiv 93/42/EØF. /
Conformité Européenne (Conformidade Europeia). Este símbolo significa
que o dispositivo está em total conformidade com a Directiva do Conselho
Europeu 93/42/CEE.
Do Not Reuse / Ne pas réutiliser / Nicht wiederverwenden / No reutilizar / Voor
eenmalig gebruik / Non riutilizzare / Skal ikke brukes flere ganger /
Kertakäyttöinen / Endast för engångsbruk / Μην επαναχρησιμοποιείτε / Må ikke
genbruges / Não reutilizar
Keep Away From Heat / Tenir éloigné des sources de chaleur / Hitzeeinwirkung
vermeiden / Mantener alejado del calor / Uit de buurt van warmtebronnen
houden / Tenere lontanto da fonti di calore / Skal holdes borte fra varme /
Suojaa kuumuudelta / Får inte utsättas för värme / Διατηρήστε το μακριά από τη
θερμότητα / Holdes væk fra varme / Manter afastado de fontes de calor
Keep Dry / À conserver au sec / Trocken aufbewahren / Mantener seco / Droog
houden / Conservare in un luogo asciutto / Skal holdes tørr / Säilytä kuivassa /
Förvaras torrt / Διατηρήστε το στεγνό / Holdes tørt / Manter seco
Quantity / Quantité / Menge / Cantidad / Aantal / Quantità / Antall / Määrä /
Antal / Ποσότητα / Antal / Quantidade
Sterilized Using Steam / Stérilisation par vapeur / Sterilisiert mittels Dampf /
Esterilizado mediante vapor / Gesteriliseerd met stoom / Sterilizzato mediante
vapore / Sterilisert med damp / Steriloitu höyryttämällä / Steriliserad med ånga /
Αποστειρωμένο με ατμό / Dampsteriliseret / Esterilizado por vapor
Do Not Use if Package is Damaged / Ne pas utiliser si l'emballage est
endommagé / Nicht verwenden, wenn die Verpackung beschädigt ist / No
utilizar si el envase está dañado / Niet gebruiken als de verpakking beschadigd
is / Non utilizzare se la confezione appare danneggiata / Skal ikke brukes hvis
pakningen er skadet / Älä käytä, jos pakkaus on vahingoittunut / Använd inte
produkten om förpackningen är skadad / Μην το χρησιμοποιείτε αν η
συσκευασία έχει υποστεί ζημιά / Må ikke anvendes, hvis emballagen er
beskadiget / Não utilizar se a embalagem estiver danificada
For US Audiences Only / Ne s'applique qu'aux États-Unis / Gilt nur für Leser in
den USA / Sólo aplicable en los Estados Unidos / Alleen van toepassing voor de
VS / Esclusivamente per il mercato statunitense / Gjelder bare USA / Koskee
vain Yhdysvaltoja / Gäller endast i USA / Μόνο για πελάτες εντός ΗΠΑ / Gælder
kun i USA / Apenas aplicável aos EUA
Caution: See Instructions for Use / Attention : voir le mode d'emploi / Achtung:
Siehe Bedienungsanleitung / Precaución: Consultar las instrucciones de uso /
Let op: Zie gebruiksaanwijzing / Attenzione: vedere le istruzioni per l'uso /
Forsiktig! Les bruksanvisningen / Varoitus: katso käyttöohjeet / OBS! Se
bruksanvisningen / Προσοχή: Bλ. οδηγίες χρήσης / Forsigtig: Se
brugsanvisningen / Atenção: Ver as instruções de utilização
1
Page 4

Do Not Resterilize / Ne pas restériliser / Nicht resterilisieren / No reesterilizar /
Niet hersteriliseren / Non risterilizzare / Skal ikke resteriliseres / Ei saa
uudelleensteriloida / Får inte omsteriliseras / Μην επαναποστειρώνετε / Må ikke
re-steriliseres / Não reesterilizar
Nonpyrogenic / Apyrogène / Pyrogenfrei / Apirógeno / Niet-pyrogeen / Non
pirogeno / Pyrogenfri / Pyrogeeniton / Icke-pyrogen / Μη πυρετογόνο / Nonpyrogen / Não pirogénico
MR Safe / RM sans risque / MR-tauglich / Seguro para RM / MR Safe (MRveilig) / Dispositivo sicuro per la risonanza magnetica (RM) / MR-sikker /
Turvallinen magneettikuvauksessa / MR-säker / Ασφαλές για MR / MRscanningssikker / RM seguro
Reorder Number / Numéro de commande / Bestellnummer / Número de
pedido / Bestelnummer / Numero d'ordine / Bestillingsnummer /
Uusintatilausnumero / Beställningsnummer / Αριθμός νέας παραγγελίας /
Genbestillingsnummer / Número de encomenda
Size / Taille / Abmessungen / Tamaño / Maat / Dimensioni / Størrelse / Koko /
Storlek / Μέγεθος / Størrelse / Tamanho
Use By / À utiliser jusqu'au / Zu verwenden bis einschließlich / No utilizar
después de / Te gebruiken tot en met / Data di scadenza / Siste forbruksdag /
Käytettävä viimeistään / Får användas till och med / Χρήση έως / Kan anvendes
til og med / Não utilizar depois de
Serial Number / Numéro de série / Seriennummer / Número de serie /
Serienummer / Numero di serie / Serienummer / Sarjanumero / Serienummer /
Αριθμός σειράς / Serienummer / Número de série
Manufacturer / Fabricant / Hersteller / Fabricante / Fabrikant / Produttore /
Produsent / Valmistaja / Tillverkare / Κατασκευαστής / Fabrikant / Fabricante
Authorized Representative in the European Community / Représentant agréé
dans la Communauté européenne / Autorisierte Vertretung für die Europäische
Gemeinschaft / Representante autorizado en la Comunidad Europea /
Geautoriseerde vertegenwoordiger in de Europese Gemeenschap /
Rappresentante autorizzato nella Comunità europea / Autorisert representant i
Det europeiske fellesskap / Valtuutettu edustaja Euroopan yhteisön alueella /
Auktoriserad representant inom EU / Εξουσιοδοτημένος αντιπρόσωπος στην
Ευρωπαϊκή Κοινότητα / Autoriseret repræsentant i EF / Representante
Autorizado na Comunidade Europeia
2
Page 5

Hancock® is a registered trademark of Medtronic, Inc.
Hancock
Hancock
Hancock
Hancock
Hancock
Hancock
Hancock
Hancock
Το Hancock
Hancock
Hancock
®
est une marque déposée de Medtronic, Inc.
®
ist eine eingetragene Marke von Medtronic, Inc.
®
es una marca comercial registrada de Medtronic, Inc.
®
is een geregistreerd handelsmerk van Medtronic, Inc.
®
è un marchio registrato della Medtronic, Inc.
®
er et registrert varemerke for Medtronic, Inc.
®
on Medtronic, Inc:n rekisteröity tavaramerkki.
®
är ett registrerat varumärke som tillhör Medtronic, Inc.
®
αποτελεί σήμα κατατεθέν της Medtronic, Inc.
®
er et registreret varemærke tilhørende Medtronic, Inc.
®
é uma marca comercial registada de Medtronic, Inc.
3
Page 6

Page 7

1 DEVICE DESCRIPTION
Hancock Apical Left Ventricle Connector Model 174A consists of a flexible polypropylene frame designed
in accordance with the same principles that led to the development of the stent for the Hancock Stabilized
Glutaraldehyde Process (SGP) aortic and atrioventricular heart valve bioprosthesis. The blood contact
surface of the connector is lined with low-porosity woven polyester material, which extends beyond the
supporting stent for anastomosis to a Hancock Valved Conduit made from the same material.
A compliant sewing ring allows suturing of the connector to the apex of the left ventricle. An additional
sewing ring is provided to control the depth of penetration of the connector into the left ventricle.
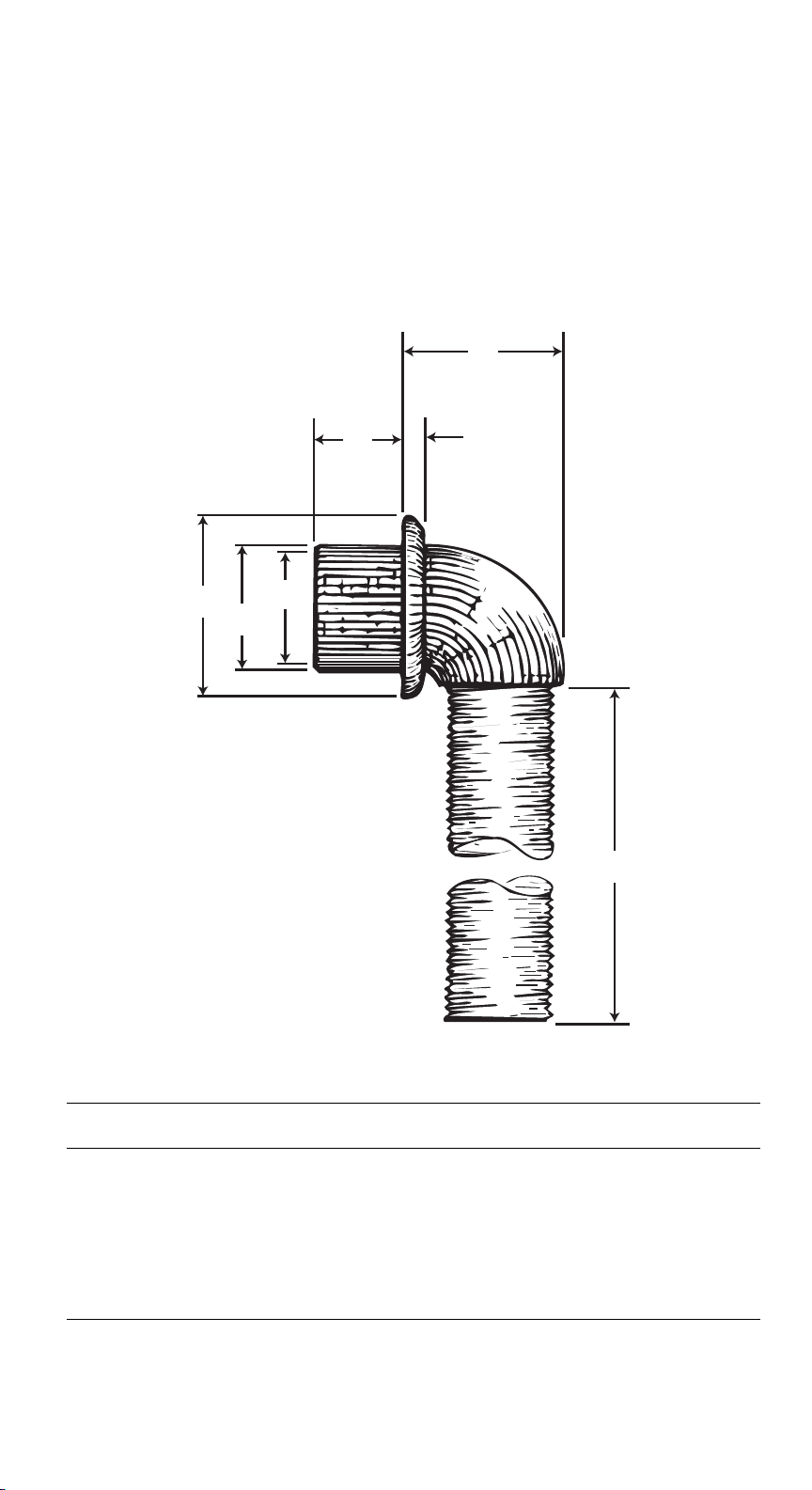
The Hancock Apical Left Ventricle Connector is available in the sizes and dimensions shown in Table 1.
Table 1. Available Sizes and Dimensions
F
D
C
A
B
E
G
CURVED CONNECTOR MODEL 174A
(mm)
SIZE A B C D E F
(minimum)
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Instructions for Use English 5
G
Page 8

2 INDICATIONS
The Hancock Apical Left Ventricle Connector, used in conjunction with Hancock Model 105 Valved Conduit
(low porosity), provides an alternate method for relief of left ventricular hypertension in patients with severe
left ventricular outflow tract obstruction, due to hypoplasia of the aortic root, hypoplasia of the aortic
annulus, or acquired problems secondary to aortic valve replacement, which cannot be relieved through
conventional techniques.
3 CONTRAINDICATIONS
The Hancock Apical Left Ventricle Connector is contraindicated for patients presenting with any of the
following conditions:
■
left ventricular aneurysm
■
thrombosis
■
severe aortic valve reflux
4 WARNINGS
This device was designed for single patient use only. Do not reuse, reprocess, or resterilize this product.
Reuse, reprocessing, or resterilization may compromise the structural integrity of the device and/or create
a risk of contamination of the device which could result in patient injury, illness, or death.
Do not use the connector if:
■
it has been dropped, damaged, or mishandled in any way
■
the use by date has elapsed
Although clinically proven materials for arterial reconstruction were selected for use in the Hancock Apical
Left Ventricle Connector, a potential for interstitial blood loss still exists, particularly in patients with
hemodilution or clotting factor deficiencies.
SERIOUS BLEEDING COMPLICATIONS HAVE BEEN REPORTED IN SUCH PATIENTS WHERE THE
CONNECTOR AND/OR VALVED CONDUIT WERE NOT PRECLOTTED. THIS POTENTIAL HAZARD
CAN BE MINIMIZED BY PRECLOTTING THE CONNECTOR AND VALVED CONDUIT.
When cross-clamping the valved conduit, do not clamp the conduit within 8 cm of the metal ring.
Select the appropriate Hancock Trocar blade and tip to perform the apical left ventriculotomy. For example,
use a size 14 mm Hancock Trocar blade and tip for insertion of a size 14 mm Hancock Apical Left Ventricle
Connector.
Examine the trocar before use to verify correct assembly and secure attachment of all components.
5 PRECAUTIONS
It is recommended that all patients undergoing this procedure have both pre-operative and intra-operative
echocardiography.
Caution: Do not use if severe coronary insufficiency, severe or symptomatic carotid occlusive disease, or
thoracic aortic aneurysmal diseases are present.
6 POTENTIAL ADVERSE EVENTS
Thromboembolism, while infrequent, has been reported. The potential for this complication should be
weighed when selecting the optimum surgical procedure for each patient.
BLEEDING AROUND THE ANASTOMOSIS OF THE CONNECTOR TO THE APEX CAN BE MINIMIZED
BY APPROPRIATE SURGICAL TECHNIQUE AND BY PRECLOTTING THE CONNECTOR AND
VALVED CONDUIT.
Significant reduction in coronary and cerebrovascular circulation may occur when intrinsic disease is
present in these systems.
7 PATIENT COUNSELING INFORMATION
Patients may require anticoagulation and/or antiplatelet therapy for an indefinite period based on each
patient's condition.
8 HOW SUPPLIED
8.1 Packaging
The Hancock Apical Left Ventricle Connector is available in the following sizes: 12, 14, 16, 18, 20, 22, and
26 mm. The package contains a single Hancock Apical Left Ventricle Connector packaged in sterile,
double-aseptic transfer pouches. The packaging system is designed to ease placement of the device in
the sterile field. The connector is sterile if the pouches are undamaged and unopened. The outer surfaces
of the outer pouch are NONSTERILE and must not be placed in the sterile field.
6 English Instructions for Use
Page 9

8.2 Storage
Store the product in its original packaging, including the outer shelf carton, in a clean, cool, dry area to
protect the product and minimize the potential for contamination. The sterility and nonpyrogenicity of the
conduit is validated to remain unaffected until the Use By date identified on the shelf carton, provided the
pouches are not opened or damaged.
Appropriate inventory control should be maintained so that connectors with earlier use by dates are
preferentially implanted and expiration is avoided.
9 INSTRUCTIONS FOR USE
9.1 Preparation
Because of the complexity and variation in surgical procedures for apico-aortic bypass, the choice
of surgical approach and suturing techniques is left to the discretion of the individual surgeon.
The following are techniques reported to Medtronic by surgeon implanters and can be used to
facilitate implant.
The insertion of the apical left ventricle connector is often performed under cardiopulmonary bypass.
Anastomosis to the descending thoracic aorta is frequently carried out through a left lateral thoracotomy
incision in the fifth intercostal space.
There are no sizers available for the connector. Sizing is determined by the capacity of the patient's
thoracic cavity instead of by traditional standards. The largest size connector that will fit into the thoracic
cavity and still allow closure of the incision without causing excessive pressure on the device should be
used.
The anastomosis of the connector and valved conduit may be performed prior to cardiopulmonary bypass.
It is strongly recommended that preclotting of the connector and valved conduit be completed in advance
of these anastomoses to avoid blood loss. An alternative is to anastomose the valved conduit to the aorta
and the connector to the apex of the ventricle separately, and then anastomose the 2 conduits together.
9.2 Device Implantation
With the pericardium split, the apex of the ventricle is elevated. A purse string suture is made at the apex.
Interrupted polyester sutures are passed through the myocardium at equidistant points around the
ventriculotomy site defined by the purse string suture and the sewing ring of the connector. A small stab
wound is made at the apex, and a myocardial plug is removed (Figures 1 and 3). Use Hancock Trocar
Blade and Tip Model 1701A with Hancock Trocar Handle Model 1701A1, hereafter referred to as Hancock
Trocar Assembly, for creation of a uniform circular ventricular opening and removal of the myocardial plug
(Figures 2a, 2b, and 2c). Care should be taken not to damage the interventricular septum, chordae
tendineae, or coronary flow. With the conduit extension clamped distal to the valve, the connector is
inserted in the left ventricle and sutured in place (Figure 4). Cardiopulmonary bypass may be discontinued
at this point at the discretion of the operator.
After trimming the distal end of the connector-valved conduit prosthesis to the correct length, end-to-side
aortic anastomosis is accomplished by using a partial occlusion clamp (Figure 4). Care should be taken
when trimming the valved conduit to remove excess length which may result in fabric wear due to friction
contact with the chest wall.
The aortic anastomosis may be located at the level of the sixth and seventh intercostal arteries (Figure 5).
The inferior pulmonary ligament is divided to permit exposure to the descending thoracic aorta.
With a vascular clamp partially occluding the aorta, a longitudinal incision is made with a right angle
scissors. The distal end of the valved conduit is anastomosed with a continuous polyester suture
(Figure 5). Air is evacuated from the left ventricle and the valved conduit with a 20-gauge needle, and the
aortic clamp is then removed.
9.3 Accessories
The Hancock Trocar Assembly, which consists of the Hancock Trocar Blade, Model 1701A and the
Hancock Trocar Handle, Model 1701A1 has been designed to facilitate apical ventriculotomy. Use only the
Hancock Trocar Assembly to create a clean, uniform opening in the left ventricular apex and to minimize
the possibility of damage to the chordae tendineae. The Hancock Trocar Assembly is available as a
reusable handle assembly employing disposable cylindrical stainless steel blades and matching tips in
sizes 12, 14, 16, 18, 20, 22, and 26 mm which correspond to the outer diameter (OD) of the connectors.
Select the size of blade and tip which match the left ventricle connector to be employed. Examine the
Hancock Trocar Assembly before use to verify correct assembly and secure attachment of all components.
Do not reuse the cutting blade.
Assembly Instructions
The Hancock Trocar Assembly consists of the tip (a), rod (b), blade (c), blade holder (d), handle (e), and
end cap (f) (Figures 6a through 6e).
1. Attach the end cap to the handle by turning the end cap clockwise (Figure 6a).
2. Attach the blade to the holder by turning the blade clockwise.
Caution: Do not hold the blade near the cutting edge (Figure 6b).
Instructions for Use English 7
Page 10

3. Slide the blade holder onto the shaft of the handle until the blade holder is fully seated inside the handle
(Figure 6c).
4. Attach the tip to the threaded shaft of the handle by turning the tip clockwise until tight (Figure 6d).
5. The completed Hancock Trocar Assembly (Figure 6e).
Refer to the Hancock Trocar Instructions for Use for detailed information on use and sterilization.
Warning: Do not use other trocar or surgical tools. Use of other tools may not create a left ventricular
opening that matches the size and geometry of the Hancock Apical Left Ventricle Connector. Their use
could result in serious bleeding around the sewing ring.
9.4 Sterilization
The Hancock Apical Left Ventricle Connector is provided STERILE (steam) and must not be resterilized.
Connectors that have been damaged or contaminated from patient contact should not be used.
10 POSTOPERATIVE INFORMATION
This device contains no metals and, therefore, poses no known hazards in all MR environments.
11 PATIENT INFORMATION
Note: Patient registration does not apply in countries where patient privacy laws conflict with providing
patient information, including countries from the EU.
A Patient Registration Form is included in each device package. After implantation, please complete all
requested information. The serial number may be found on the package and on the identification tag
attached to the retainer. Return the original form to the Medtronic address indicated on the form and
provide the temporary identification card to the patient prior to discharge.
An Implanted Device Identification Card is provided to the patient. The card contains the name and
telephone number of the patient's physician, as well as information that medical personnel would require
in the event of an emergency.
8 English Instructions for Use
Page 11

12 DISCLAIMER OF WARRANTIES
THE FOLLOWING DISCLAIMER OF WARRANTY APPLIES TO UNITED STATES CUSTOMERS ONLY:
DISCLAIMER OF WARRANTY
ALTHOUGH THE HANCOCK APICAL LEFT VENTRICLE CONNECTOR (MODEL 174A), HEREAFTER
REFERRED TO AS “PRODUCT,” HAS BEEN MANUFACTURED UNDER CAREFULLY CONTROLLED
CONDITIONS, MEDTRONIC HAS NO CONTROL OVER THE CONDITIONS UNDER WHICH THIS
PRODUCT IS USED. MEDTRONIC, THEREFORE, DISCLAIMS ALL WARRANTIES, BOTH EXPRESS
AND IMPLIED, WITH RESPECT TO THE PRODUCT, INCLUDING, BUT NOT LIMITED TO, ANY
IMPLIED WARRANTY OF MERCHANTABILITY OR FITNESS FOR A PARTICULAR PURPOSE.
MEDTRONIC SHALL NOT BE LIABLE TO ANY PERSON OR ENTITY FOR ANY MEDICAL
EXPENSES OR ANY DIRECT, INCIDENTAL, OR CONSEQUENTIAL DAMAGES CAUSED BY ANY
USE, DEFECT, FAILURE, OR MALFUNCTION OF THE PRODUCT, WHETHER A CLAIM FOR SUCH
DAMAGES IS BASED UPON WARRANTY, CONTRACT, TORT, OR OTHERWISE. NO PERSON HAS
ANY AUTHORITY TO BIND MEDTRONIC TO ANY REPRESENTATION OR WARRANTY WITH
RESPECT TO THE PRODUCT.
The exclusions and limitations set out above are not intended to, and should not be construed so as to,
contravene mandatory provisions of applicable law. If any part or term of this DISCLAIMER OF
WARRANTY is held by any court of competent jurisdiction to be illegal, unenforceable, or in conflict with
applicable law, the validity of the remaining portions of this DISCLAIMER OF WARRANTY shall not be
affected, and all rights and obligations shall be construed and enforced as if this DISCLAIMER OF
WARRANTY did not contain the particular part or term held to be invalid.
THE FOLLOWING DISCLAIMER OF WARRANTY APPLIES TO CUSTOMERS OUTSIDE THE UNITED
STATES:
DISCLAIMER OF WARRANTY
ALTHOUGH THE HANCOCK APICAL LEFT VENTRICLE CONNECTOR (MODEL 174A), HEREAFTER
REFERRED TO AS “PRODUCT,” HAS BEEN CAREFULLY DESIGNED, MANUFACTURED, AND
TESTED PRIOR TO SALE, THE PRODUCT MAY FAIL TO PERFORM ITS INTENDED FUNCTION
SATISFACTORILY FOR A VARIETY OF REASONS. THE WARNINGS CONTAINED IN THE PRODUCT
LABELING PROVIDE MORE DETAILED INFORMATION AND ARE CONSIDERED AN INTEGRAL
PART OF THIS DISCLAIMER OF WARRANTY. MEDTRONIC, THEREFORE, DISCLAIMS ALL
WARRANTIES, BOTH EXPRESS AND IMPLIED, WITH RESPECT TO THE PRODUCT. MEDTRONIC
SHALL NOT BE LIABLE FOR ANY INCIDENTAL OR CONSEQUENTIAL DAMAGES CAUSED BY
ANY USE, DEFECT, OR FAILURE OF THE PRODUCT, WHETHER THE CLAIM IS BASED ON
WARRANTY, CONTRACT, TORT, OR OTHERWISE.
The exclusions and limitations set out above are not intended to, and should not be construed so as to,
contravene mandatory provisions of applicable law. If any part or term of this DISCLAIMER OF
WARRANTY is held to be illegal, unenforceable, or in conflict with applicable law by a court of competent
jurisdiction, the validity of the remaining portions of this DISCLAIMER OF WARRANTY shall not be
affected, and all rights and obligations shall be construed and enforced as if this DISCLAIMER OF
WARRANTY did not contain the particular part or term held to be invalid.
Instructions for Use English 9
Page 12

Page 13
1 DESCRIPTION DU DISPOSITIF
L'embout apical pour ventricule gauche Hancock, Modèle 174A, se compose d'une structure souple en
polypropylène conçue selon le principe de l'armature de la valve cardiaque Hancock, bioprothèse
atrioventriculaire et aortique “SGP” (glutaraldéhyde stabilisé). La surface de l'embout en contact avec le
sang est revêtue d'un polyester tissé à faible porosité, dépassant l'armature pour permettre l'anastomose
avec un conduit valvé Hancock, fabriqué à partir du même matériau.
Un anneau de suture maniable permet de suturer l'embout sur l'apex du ventricule gauche. Un deuxième
anneau de suture permet de contrôler la profondeur de pénétration de l'embout dans le ventricule gauche.
L'embout apical pour ventricule gauche Hancock est disponible dans les tailles indiquées dans le
Tableau 1.
Tableau 1. Tailles et diamètres disponibles
F
D
C
A
B
E
G
EMBOUT RECOURBÉ MODÈLE 174A
(mm)
TAI LLE A B C D E F
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Mode d'emploi Français 11
G
(minimum)
Page 14

2 INDICATIONS
L'utilisation de l'embout apical pour ventricule gauche Hancock et du conduit valvé Hancock Modèle 105
(faible porosité) constitue une nouvelle méthode de traitement de l'hypertension ventriculaire gauche chez
les patients présentant une obstruction sévère de la chambre de chasse du ventricule gauche, due à une
hypoplasie de la racine aortique, une hypoplasie de l'anneau aortique ou des problèmes faisant suite au
remplacement d'une valve aortique ne pouvant pas être résolus par les méthodes conventionnelles.
3 CONTRE-INDICATIONS
L'embout apical pour ventricule gauche Hancock est contre-indiqué chez les patients atteints de l'une des
pathologies suivantes :
■
anévrysme ventriculaire gauche,
■
thrombose,
■
reflux aortique sévère.
4 AVERTISSEMENTS
Cet appareil est destiné à un patient unique. Ne pas réutiliser, retraiter ni restériliser ce produit. La
réutilisation, le retraitement ou la restérilisation risque de compromettre l'intégrité de l'appareil et/ou de
contaminer l'appareil, ce qui pourrait entraîner des blessures, une maladie ou le décès du patient.
Ne pas utiliser l'embout :
■
s'il est tombé, endommagé ou utilisé de manière incorrecte.
■
si la date de péremption est dépassée.
Bien que l'embout apical pour ventricule gauche Hancock se compose de matériaux testés cliniquement
pour la reconstruction artérielle, un risque de perte de sang interstitielle demeure, notamment chez les
patients présentant des insuffisances d'hémodilution ou de facteurs de coagulation.
DES COMPLICATIONS HÉMORRAGIQUES GRAVES ONT ÉTÉ SIGNALÉES LORSQUE L'EMBOUT
ET/OU LE CONDUIT VALVÉ N'ÉTAIENT PAS PRÉCOAGULÉS. POUR RÉDUIRE CE RISQUE,
L'EMBOUT ET LE CONDUIT VALVÉ DOIVENT ÊTRE PRÉCOAGULÉS.
Le clampage du conduit valvé doit être effectué à plus de 8 cm de l'anneau métallique.
Choisir une lame et extrémité de trocart Hancock appropriées pour pratiquer la ventriculotomie gauche
apicale. Par exemple, pour la pose d'un embout apical pour ventricule gauche Hancock de 14 mm, utiliser
une lame et extrémité de trocart Hancock de 14 mm.
Avant utilisation, vérifier que le trocart est solidement assemblé.
5 PRÉCAUTIONS
Il est recommandé de pratiquer une échocardiographie peropératoire et post-opératoire chez tous les
patients qui subissent cette procédure.
Attention : Ne pas utiliser en cas d'insuffisance coronarienne sévère, d'occlusion sévère ou
symptomatique de la carotide ou d'anévrysme de l'aorte thoracique.
6 EFFETS INDÉSIRABLES POTENTIELS
Des cas de thromboembolie, bien que rares, ont été signalés. L'éventualité de ces complications doit être
prise en compte lors du choix de la procédure chirurgicale la plus appropriée à chaque patient.
LE RISQUE HÉMORRAGIQUE AUTOUR DE L'ANASTOMOSE DE L'EMBOUT SUR L'APEX PEUT
ÊTRE LIMITÉ PAR UNE TECHNIQUE CHIRURGICALE APPROPRIÉE ET LA PRÉCOAGULATION DE
L'EMBOUT ET DU CONDUIT VALVÉ.
Une réduction significative de la circulation coronarienne et cérébrovasculaire peut se produire en cas de
pathologie intrinsèque affectant ces systèmes.
7 INFORMATIONS DESTINÉES AUX PATIENTS
Il se peut qu'un traitement aux anticoagulants et/ou aux inhibiteurs antiplaquettaires doive être prescrit aux
patients pour une durée indéterminée, selon leur état.
8 PRÉSENTATION
8.1 Conditionnement
L'embout apical pour ventricule gauche Hancock est disponible dans les tailles suivantes : 12, 14, 16, 18,
20, 22 et 26 mm. L'emballage contient un seul embout apical pour ventricule gauche Hancock, emballé
dans des doubles poches de transfert stériles et aseptisées. Ce conditionnement est conçu pour simplifier
le placement du dispositif dans le champ stérile. L'embout reste stérile si les poches ne sont ni ouvertes
ni endommagées. Les surfaces extérieures de la poche externe NE SONT PAS STÉRILES et ne doivent
pas être placées dans le champ stérile.
12 Français Mode d'emploi
Page 15

8.2 Conservation
Ranger le produit dans son emballage d'origine, y compris le carton externe, dans un local propre, frais
et sec afin de protéger le produit et de réduire au minimum les risques de contamination. La stérilité et
l'absence de pyrogénicité du conduit demeurent inaltérées jusqu'à la date de péremption indiquée sur la
boîte, sous réserve que les poches ne soient ni ouvertes ni endommagées.
Le contrôle des stocks doit avoir lieu de manière à ce que les embouts arrivant à expiration en premier
soient implantés en priorité afin d'éviter le dépassement de la date de péremption.
9 MODE D'EMPLOI
9.1 Préparation
En raison de la complexité et la variation des procédures chirurgicales de la dérivation apicoaortique, le choix de l'approche chirurgicale et les techniques de sutures sont laissés à la
discrétion du chirurgien. Les techniques suivantes ont été communiquées à Medtronic par des
chirurgiens ayant effectué une implantation et peuvent être utilisées pour faciliter l'implantation.
La pose de l'embout apical pour ventricule gauche est souvent réalisée sous circulation extracorporelle.
L'anastomose sur l'aorte thoracique descendante est fréquemment effectuée par une thoracotomie
latérale gauche, dans le cinquième espace intercostal.
Il n'y a pas de calibreurs disponibles pour l'embout. Le dimensionnement est défini par la capacité de la
cavité thoracique du patient et non par les normes traditionnelles. Utiliser l'embout le plus grand qui
entrera dans la cavité thoracique et qui permet de fermer l'incision sans produire une pression excessive
sur le dispositif.
L'anastomose de l'embout et du conduit valvé peut être effectuée avant la circulation extracorporelle. Il
est vivement conseillé de précoaguler l'embout et le conduit valvé avant ces anastomoses pour éviter
l'effusion de sang. Il est également possible de pratiquer séparément l'anastomose du conduit valvé sur
l'aorte, et l'anastomose de l'embout sur l'apex du ventricule, puis l'anastomose des deux conduits.
9.2 Implantation du dispositif
Avec la fente du péricarde, l'apex du ventricule est surélevé. Effectuer une suture en bourse sur l'apex.
Des sutures interrompues en polyester traversent le myocarde, à équidistance du site de ventriculotomie
défini par la suture en bourse et l'anneau de suture de l'embout. Une petite incision est pratiquée à l'apex
et un bouchon de myocarde est retiré (Figures 1 et 3). Utiliser une lame et extrémité de trocart Hancock,
Modèle 1701A, avec une poignée de trocart Hancock, Modèle 1701A1, ci-après appelé le jeu de trocart
Hancock, pour créer une ouverture uniforme circulaire sur le ventricule et retirer le bouchon de myocarde
(Figures 2a, 2b et 2c). Prendre soin de ne pas endommager le septum interventriculaire, les cordages
tendineux ou le débit coronarien. Clamper l'extension du conduit en distal de la valve, insérer l'embout
dans le ventricule gauche et le suturer en place (Figure 4). La circulation extracorporelle peut être
interrompue à ce stade, à la discrétion du perfusionniste.
Après raccourcissement de l'extrémité distale de la prothèse embout-conduit valvé à la longueur correcte,
l'anastomose latérale sur l'aorte est effectuée avec clampage partiel (Figure 4). Prendre soin de retirer la
longueur excédentaire lors du raccourcissement du conduit valvé, afin d'éviter l'usure du tissu par friction
avec la paroi thoracique.
L'anastomose aortique peut être effectuée au niveau des sixième et septième artères intercostales
(Figure 5). Le ligament pulmonaire inférieur est divisé pour avoir accès à l'aorte thoracique descendante.
Une pince vasculaire obturant partiellement l'aorte, pratiquer une incision longitudinale avec des ciseaux
à angle droit. L'extrémité distale du conduit valvé est anastomosée avec une suture continue en polyester
(Figure 5). Évacuer l'air du ventricule gauche et du conduit valvé avec une aiguille à 20 gauges et retirer
la pince aortique.
9.3 Accessoires
Le jeu de trocart Hancock, composé de la lame de trocart Hancock, Modèle 1701A, et de la poignée de
trocart Hancock, Modèle 1701A1, a été conçu pour faciliter la ventriculotomie apicale. Utiliser
systématiquement le jeu de trocart Hancock pour réaliser une ouverture nette et uniforme dans l'apex du
ventricule gauche et pour réduire le risque de dommage des cordages tendineux. Le jeu de trocart
Hancock se compose d'une poignée réutilisable, de lames cylindriques jetables en acier inoxydable et
d'extrémités de 12, 14, 16, 18, 20, 22 et 26 mm correspondant au diamètre externe des embouts. Choisir
une lame et une extrémité correspondant à l'embout pour ventricule gauche à poser. Avant utilisation,
vérifier que le jeu de trocart Hancock est solidement assemblé. Ne pas réutiliser la lame.
Instructions d'assemblage
Le jeu de trocart Hancock se compose de l'extrémité (a), de la tige (b), de la lame (c), du porte-lame (d),
de la poignée (e) et du capuchon (f) (Figures 6a à 6e).
1. Fixer le capuchon sur la poignée en le faisant tourner dans le sens des aiguilles d'une montre
(Figure 6a).
2. Fixer la lame sur le porte-lame en la faisant tourner dans le sens des aiguilles d'une montre.
Attention : Poser les doigts à distance du bord tranchant de la lame (Figure 6b).
Mode d'emploi Français 13
Page 16

3. Faire glisser le porte-lame sur la tige de la poignée jusqu'à ce que le porte-lame se trouve à fond dans
la poignée (Figure 6c).
4. Fixer l'extrémité sur la partie filetée de la tige de la poignée en la faisant tourner dans le sens des
aiguilles d'une montre (Figure 6d).
5. Jeu de trocart Hancock entièrement assemblé (Figure 6e).
Se reporter au mode d'emploi du trocart Hancock pour plus de détails sur les recommandations
d'utilisation et de stérilisation.
Avertissement : Ne pas utiliser d'autres trocarts ou instruments chirurgicaux. L'utilisation d'autres
instruments risque de résulter en une ouverture dont la taille et la forme ne sont pas adaptées à l'embout
apical pour ventricule gauche Hancock. Ceci risque de provoquer des hémorragies graves autour de
l'anneau de suture.
9.4 Stérilisation
L'embout apical pour ventricule gauche Hancock est fourni STÉRILE (stérilisation à la vapeur) et ne
doivent pas être restérilisés. Les embouts ayant été endommagées ou contaminées au contact d'un
patient ne doivent pas être utilisées.
10 INFORMATIONS POST-OPÉRATOIRES
Ce dispositif ne contient aucune partie métallique et ne présente donc aucun risque connu dans tous les
environnements à résonance magnétique.
11 INFORMATIONS SUR LE PATIENT
Remarque : L'enregistrement de données patient ne s'applique pas dans les pays (y compris certains
pays de l'UE) pour lesquels la divulgation d'informations patient est illégale au regard des lois en vigueur
relatives à la vie privée du patient.
L'emballage de chaque dispositif contient une fiche d'enregistrement du patient. Après l'implantation,
fournir toutes les informations demandées. Le numéro de série se trouve sur l'emballage et sur la
plaquette d'identification attachée au récipient. Renvoyer le document original à Medtronic à l'adresse
mentionnée sur le document et donner au patient sa carte d'identification temporaire avant sa sortie de
l'hôpital.
Une carte d'identification du dispositif implanté est fournie au patient. Cette carte contient le nom et le
numéro de téléphone du médecin traitant, ainsi que des informations utiles au personnel médical en cas
d'urgence.
14 Français Mode d'emploi
Page 17

12 DÉNI DE GARANTIE
SEULS LES CLIENTS EN DEHORS DES ÉTATS-UNIS PEUVENT AVOIR RECOURS AU PRÉSENT
DÉNI DE GARANTIE :
DÉNI DE GARANTIE
BIEN QUE L'EMBOUT APICAL POUR VENTRICULE GAUCHE HANCOCK (MODÈLE 174A), CI-
APRÈS LE "PRODUIT", AIT ÉTÉ SOIGNEUSEMENT CONÇU, FABRIQUÉ ET TESTÉ AVANT SA MISE
EN VENTE, LE PRODUIT PEUT, POUR DES RAISONS DIVERSES, CONNAÎTRE DES
DÉFAILLANCES. LES AVERTISSEMENTS PRÉSENTS DANS LA DOCUMENTATION DU PRODUIT
CONTIENNENT DES INFORMATIONS DÉTAILLÉES ET DOIVENT ÊTRE CONSIDÉRÉS COMME
FAISANT PARTIE INTÉGRANTE DU PRÉSENT DÉNI DE GARANTIE. EN CONSÉQUENCE,
MEDTRONIC DÉCLINE TOUTE RESPONSABILITÉ, EXPLICITE OU IMPLICITE, RELATIVE AU
PRODUIT. MEDTRONIC NE SERA PAS TENU RESPONSABLE DE TOUS DOMMAGES FORTUITS
OU INDIRECTS QUI SERAIENT PROVOQUÉS PAR TOUS USAGES, DÉFECTUOSITÉS OU
DÉFAILLANCES DU PRODUIT, ET CE QUE LA PLAINTE SOIT FONDÉE SUR UNE GARANTIE, UNE
RESPONSABILITÉ CONTRACTUELLE, DÉLICTUEUSE OU QUASI-DÉLICTUEUSE.
Les exclusions et les limitations de garantie mentionnées ci-dessus ne sont pas, et ne doivent pas être
interprétées comme contraires aux dispositions obligatoires des lois applicables. Si une partie ou une
disposition du présent DÉNI DE GARANTIE devait être considérée comme illégale, non applicable ou
contraire à la loi en vigueur par un tribunal compétent, la validité des autres dispositions du présent DÉNI
DE GARANTIE n'en sera pas affectée. Dans ce cas, tous les autres droits et obligations seront interprétés
et appliqués, sans tenir compte de la partie ou la disposition considérée comme illégale.
Mode d'emploi Français 15
Page 18

Page 19

1 PRODUKTBESCHREIBUNG
Der apikale linksventrikuläre Konnektor Modell Hancock 174A besteht aus einem flexiblen
Polypropylenrahmen, der nach denselben Prinzipien wie der Stent für die Hancock Stabilized
Glutaraldehyde Process (SGP) Aorten- und AV-Klappen-Bioprothese konzipiert wurde. Die
Blutkontaktfläche des Konnektors ist mit Polyestergewebe mit geringer Porösität bedeckt, das über
den Stützstent hinausreicht, sodass die Anastomose mit einem aus dem gleichen Material gefertigten
Hancock klappentragenden Conduit erfolgen kann.
Ein nachgiebiger Nahtring ermöglicht das Annähen des Konnektors an den Apex des linken Ventrikels.
Zur Steuerung der Einführtiefe des Konnektors in den linken Ventrikel wird ein zusätzlicher Nährring
bereitgestellt.
Der Hancock apikale linksventrikuläre Konnektor ist in den in Tabelle 1 aufgeführten Größen und
Abmessungen verfügbar.
Tab ell e 1 . Lieferbare Größen und Abmessungen
F
D
C
A
B
E
G
GEKRÜMMTER KONNEKTOR MODELL 174A
(mm)
GRÖSSE A B C D E F
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Gebrauchsanweisung Deutsch 17
G
(Minimum)
Page 20

2 INDIKATIONEN
Der Hancock apikale linksventrikuläre Konnektor, der in Verbindung mit dem klappentragenden Conduit
Modell Hancock 105 (geringe Porösität) verwendet wird, stellt eine alternative Methode zur Beseitigung
der linksventrikulären Hypertonie bei Patienten mit schwerer Obstruktion des linksventrikulären
Ausflusstrakts dar, wie etwa bei Hypoplasie der Aortenwurzel, Hypoplasie des Aortenanulus oder bei
sekundären Beschwerden nach Aortenklappenersatz, die mit herkömmlichen Methoden nicht beseitigt
werden können.
3 KONTRAINDIKATIONEN
Der Hancock apikale linksventrikuläre Konnektor ist beim Vorliegen der folgenden medizinischen
Gegebenheiten kontraindiziert:
■
linksventrikuläres Aneurysma
■
Thrombose
■
schwerer Aortenklappen-Reflux
4 WARNHINWEISE
Das Gerät ist zur Verwendung an nur einem Patienten bestimmt. Das Produkt darf nicht wiederverwendet,
aufbereitet oder resterilisiert werden. Wiederverwendung, Aufbereitung oder Resterilisierung können die
strukturelle Integrität des Geräts beeinträchtigen und/oder unter Umständen eine Kontamination des
Geräts bewirken, die wiederum zu Verletzung, Erkrankung oder zum Tod des Patienten führen kann.
Den Konnektor in den folgenden Situationen nicht verwenden:
■
Wenn das Gerät heruntergefallen ist, beschädigt oder in irgendeiner Weise falsch behandelt wurde.
■
Wenn das Verwendbarkeitsdatum überschritten ist.
Zwar wurden für den Hancock apikalen linksventrikulären Konnektor nur Materialen verwendet, deren
Einsatz in der Arterienrekonstruktion klinisch geprüft wurde, es besteht jedoch dennoch die Gefahr des
interstitiellen Blutverlusts, insbesondere bei Patienten mit Hämodilution oder Gerinnungsstörungen.
SCHWERE BLUTUNGEN WURDEN BEI SOLCHEN PATIENTEN BEOBACHTET, BEI DENEN FÜR
DEN KONNEKTOR UND/ODER DAS KLAPPENTRAGENDE CONDUIT KEINE VORGERINNUNG
DURCHGEFÜHRT WURDE. DIESES RISIKO KANN DURCH VORGERINNUNG DES KONNEKTORS
UND DES KLAPPENTRAGENDEN CONDUITS MINIMIERT WERDEN.
Beim Crossclamping des klappentragenden Conduits darf das Conduit nicht innerhalb der ersten 8 cm
vom Metallring abgeklemmt werden.
Wählen Sie für die apikale linksseitige Ventrikulotomie die geeignete Hancock Trokarklinge und -spitze
aus. Beispielsweise ist zum Einsetzen eines Hancock apikalen linksventrikulären Konnektors der Größe
14 mm eine Hancock Trokarklinge und -spitze der Größe 14 mm zu verwenden.
Überprüfen Sie den Trokar vor der Verwendung auf korrekten Zusammenbau und sichere Befestigung
aller Komponenten.
5 VORSICHTSMASSNAHMEN
Es empfiehlt sich, dass alle Patienten, an denen dieser Eingriff vorgenommen werden soll, sowohl vor als
auch während der Operation echokardiografisch überwacht werden.
Achtung: Nicht verwenden, wenn schwere Koronarinsuffizienz, schwere oder symptomatische
Karotisinsuffizienz oder aneurysmatische Erkrankungen der Brustaorta vorliegen.
6 MÖGLICHE KOMPLIKATIONEN
In seltenen Fällen kann es zu Thromboembolie kommen. Die Möglichkeit dieser Komplikation muss bei
der Auswahl des für den jeweiligen Patienten am besten geeigneten chirurgischen Verfahrens
berücksichtigt werden.
BLUTUNGEN UM DIE ANASTOMOSE DES KONNEKTORS ZUR HERZSPITZE KÖNNEN DURCH EINE
GEEIGNETE CHIRURGISCHE METHODE SOWIE DURCH VORGERINNUNG DES KONNEKTORS
UND DES KLAPPENTRAGENDEN CONDUITS MINIMIERT WERDEN.
Bei Vorliegen einer intrinsischen Erkrankung dieser Systeme kann es zu einem signifikanten Abfall der
koronaren und zerebrovaskulären Durchblutung kommen.
7 INFORMATIONEN ZUR PATIENTENBERATUNG
Je nach Zustand des Patienten kann eine Antikoagulations- oder Thrombozyten-AggregationshemmerTherapie angeraten sein.
18 Deutsch Gebrauchsanweisung
Page 21

8 LIEFERUMFANG
8.1 Verpackung
Der Hancock apikale linksventrikuläre Konnektor ist in den folgenden Größen verfügbar: 12, 14, 16, 18,
20, 22 und 26 mm. Die Packung enthält einen einzelnen Hancock apikalen linksventrikulären Konnektor
in sterilen, doppelt aseptischen Transportbeuteln. Das Verpackungssystem ist so konzipiert, dass das
Produkt problemlos in das sterile Feld überführt werden kann. Der Konnektor ist steril, wenn die Beutel
nicht beschädigt oder geöffnet wurden. Die Außenflächen des externen Beutels sind NICHT STERIL und
dürfen nicht im Sterilbereich abgelegt werden.
8.2 Lagerung
Lagern Sie das Produkt in seiner Originalverpackung einschließlich des Umkartons an einem kühlen und
trockenen Ort, um das Produkt zu schützen und Kontaminationen nach Möglichkeit auszuschließen.
Sofern die Beutel nicht geöffnet oder beschädigt werden, ist sichergestellt, dass das Conduit bis zu
dem auf dem Umkarton angegebenen Verwendbarkeitsdatum steril und nichtpyrogen ist.
Stellen Sie durch geeignete Lagerverwaltung sicher, dass vorzugsweise immer die Konnektoren mit
jüngerem Verfallsdatum implantiert werden und damit das Erreichen eines Verfallsdatums vermieden
wird.
9 GEBRAUCHSANWEISUNG
9.1 Vorbereitung
Aufgrund der Komplexität und Unterschiede zwischen den chirurgischen Verfahren zur
Durchführung eines apicoaortalen Bypass obliegt die Auswahl des chirurgischen Ansatzes und
der Nähmethoden dem jeweiligen Chirurgen. Folgende Methoden, die Medtronic von Implanteuren
mitgeteilt wurden, können für die Implantation verwendet werden.
Die Implantation eines apikalen linksventrikulären Konnektors wird zumeist bei kardiopulmonalem Bypass
durchgeführt. Die Anastomose mit der deszendierenden thorakalen Aorta erfolgt häufig durch eine
linkslaterale Thorakotomie im fünften Interkostalraum.
Für den Konnektor sind keine Größenmesser verfügbar. Die Auswahl der Größe wird nicht mithilfe
herkömmlicher Standards, sondern durch die Kapazität der Thoraxhöhle des Patienten bestimmt.
Es sollte der größte Konnektor verwendet werden, der in die Thoraxhöhle passt und gleichzeitig die
Schließung des Einschnitts erlaubt, ohne dass dadurch übermäßiger Druck auf das Gerät ausgeübt wird.
Die Anastomose des Konnektors und des klappentragenden Conduits kann durchgeführt werden, bevor
der kardiopulmonale Bypass gelegt wird. Zur Vermeidung von Blutverlust wird unbedingt empfohlen,
vor den Anastomosen eine Vorgerinnung des Konnektors und des klappentragenden Conduits
durchzuführen. Alternativ können das klappentragende Conduit und der Konnektor separat mit der Aorta
bzw. der Ventrikelspitze anastomosiert werden. In diesem Fall werden anschließend die beiden Conduits
miteinander anastomosiert.
9.2 Implantation
Bei eröffnetem Pericardium wird die Ventrikelspitze angehoben. An der Spitze wird eine Raffnaht
angebracht. Unterbrochene Polyesternähte werden entsprechend der Raffnaht und dem Nahtring des
Konnektors in gleichmäßigen Abständen um die Ventrikulotomie durch das Myocardium angebracht.
An der Ventrikelspitze wird ein kleiner Ausstich vorgenommen und der Pfropf aus dem Myocardium
entfernt (Abbildung 1 und 3). Verwenden Sie die Trokarklinge und -spitze Modell Hancock 1701A mit
dem Trokargriff Modell Hancock 1701A1 (im Folgenden als Hancock Trokarset bezeichnet), um eine
gleichmäßige kreisförmige Öffnung im Ventrikel anzubringen und den myocardialen Pfropf zu entfernen
(Abbildung 2a, 2b und 2c). Dabei ist darauf zu achten, dass das Interventrikularseptum, die Chordae
tendineae und der koronare Fluss nicht in Mitleidenschaft gezogen werden. Der Konnektor, dessen
Conduitverlängerung distal an die Klappe geklemmt ist, wird in den linken Ventrikel eingeführt und
festgenäht (Abbildung 4). Es liegt im Ermessen des Chirurgen, ob der kardiopulmonale Bypass jetzt
eingestellt werden kann.
Nachdem das distale Ende der Konnektor/klappentragenden Conduit-Prothese auf die erforderliche
Länge gekürzt wurde, wird mithilfe einer Klemme für teilweise Okklusion eine End-to-sideAortenanastomose erzielt (Abbildung 4). Gehen Sie beim Kürzen des klappentragenden Conduits äußerst
sorgfältig vor, um Materialabrieb zu verhindern, der durch Reibung mit der Thoraxwand entstehen kann.
Die Aortenanastomose kann auf der Höhe der sechsten und siebenten Interkostalarterie erfolgen
(Abbildung 5). Das Ligamentum pulmonale inferior wird geteilt, um die absteigende thorakale Aorta
freizulegen.
Während die Aorta mit einer Gefäßklemme teilweise abgeklemmt ist, wird mit einer Winkelschere ein
Längsschnitt vorgenommen. Das distale Ende des klappentragenden Conduits wird mit einer
ununterbrochenen Polyesternaht anastomosiert. (Abbildung 5). Aus dem linken Ventrikel und dem
klappentragenden Conduit wird mit einer Nadel der Größe 20 Gauge die Luft abgesaugt. Anschließend
wird die Aortenklemme entfernt.
Gebrauchsanweisung Deutsch 19
Page 22

9.3 Zubehörteile
Das Hancock Trokarset, bestehend aus Trokarklinge Modell Hancock 1701A und dem Trokargriff Modell
Hancock 1701A1 ist für die Verwendung in der apikalen Ventrikulotomie konzipiert. Verwenden Sie nur
das Hancock Trokarset, um eine saubere, gleichmäßige Öffnung in die linke Ventrikelspitze einzubringen
und das Risiko einer Beschädigung der Chordae tendineae so gering wie möglich zu halten. Das Hancock
Trokarset besteht aus einem wiederverwendbaren Griff, zylindrischen Einweg-Stahlklingen und
passenden Spitzen der Größen 12, 14, 16, 18, 20, 22 und 26 mm, die dem Außendurchmesser der
verschiedenen Konnektoren ensprechen. Wählen Sie die Klinge und Spitze in der Größe aus, die dem
zu verwendenden linksventrikulären Konnektor entspricht. Überprüfen Sie das Hancock Trokarset
vor der Verwendung auf korrekten Zusammenbau und sichere Befestigung aller Komponenten.
Die Schneidklinge nicht mehrmals verwenden.
Anleitung zum Zusammenbau
Das Hancock Trokarset besteht aus Spitze (a), Stift (b), Klinge (c), Klingenhalter (d), Griff (e), und
Endkappe (f) (Abbildungen 6a bis 6e).
1. Befestigen Sie die Endkappe durch Drehen der Endkappe im Uhrzeigersinn am Griff (Abbildung 6a).
2. Befestigen Sie den Griff durch Drehen der Klinge im Uhrzeigersinn am Klingenhalter.
Achtung: Die Klinge nicht nahe der Schnittfläche greifen (Figure 6b).
3. Schieben Sie den Klingenhalter auf den Schaft des Griffs, bis der Klingenhalter vollständig im Griff sitzt
(Abbildung 6c).
4. Befestigen Sie die Spitze des Gewindeschafts durch Drehen der Spitze im Uhrzeigersinn, bis diese fest
sitzt (Abbildung 6d).
5. Das zusammengesetzte Hancock Trokarset (Abbildung 6e).
Detaillierte Informationen zur Verwendung und Sterilisation sind der Gebrauchsanweisung für den
Hancock Trokar zu entnehmen.
Warnhinweis: Verwenden Sie keinen anderen Trokar oder andere chirurgische Instrumente. Die
Verwendung eines anderen Geräts kann zu einer Öffnung im linken Ventrikel führen, die nicht der Größe
oder Geometrie des Hancock apikalen linksventrikulären Konnektors entspricht. Dadurch kann es zu
schweren Blutungen um den Nahtring kommen.
9.4 Sterilisierung
Der Hancock apikale linksventrikuläre Konnektor wird STERIL (Dampf) geliefert und darf nicht erneut
sterilisiert werden. Beschädigte oder durch den Kontakt mit dem Patienten kontaminierte Konnektoren
dürfen nicht verwendet werden.
10 NACH DEM EINGRIFF
Das Produkt enthält keine Metalle und kann daher nach aktuellem Wissensstand ohne Bedenken MRTSystemen aller Art ausgesetzt werden.
11 PATIENTENINFORMATIONEN
Hinweis: Die Patientenregistrierung erfolgt nicht in Ländern, deren Datenschutzbestimmungen die
Weitergabe von Patienteninformationen untersagen. Hierzu gehören insbesondere die Länder der
Europäischen Union.
Der Verpackung des Produkts liegt ein Formular zur Registrierung des Patienten bei. Bitte tragen Sie nach
der Implantation alle benötigten Angaben ein. Die Seriennummer befindet sich auf der Verpackung und
auf dem Identifikationsetikett an dem Behälter. Senden Sie das Originalformular an die auf dem Formular
angegebene Anschrift von Medtronic und händigen Sie dem Patienten vor der Entlassung die vorläufige
Kennkarte aus.
Dem Patienten wird eine Implantat-Identifikationskarte ausgehändigt. Diese Karte enthält den Namen und
die Telefonnummer des behandelnden Arztes sowie alle Daten, die das medizinische Personal in einem
Notfall benötigen könnte.
20 Deutsch Gebrauchsanweisung
Page 23

12 HAFTUNGSAUSSCHLUSS
FOLGENDER HAFTUNGSAUSSCHLUSS GILT NUR FÜR KUNDEN AUSSERHALB DER USA:
HAFTUNGSAUSSCHLUSS
TROTZ SORGFÄLTIGER KONSTRUKTION, HERSTELLUNG UND VOR VERKAUF DURCHGEFÜHRTEN
TESTDURCHLÄUFE IST ES MÖGLICH, DASS DER APIKALE LINKSVENTRIKULÄRE KONNEKTOR
(MODELL HANCOCK 174A) – IM NACHFOLGENDEN ALS „PRODUKT“ BEZEICHNET – AUS
VERSCHIEDENSTEN GRÜNDEN NICHT ZUFRIEDENSTELLEND FUNKTIONIERT. DIE HINWEISE
IN DER PRODUKTINFORMATION ENTHALTEN WEITERE DETAILLIERTE INFORMATIONEN UND
SIND ALS TEIL DES HAFTUNGSAUSSCHLUSSES ANZUSEHEN. MEDTRONIC SCHLIESST JEDE
AUSDRÜCKLICHE ODER STILLSCHWEIGENDE GARANTIE IN BEZUG AUF DAS PRODUKT AUS.
MEDTRONIC HAFTET WEDER FÜR UNMITTELBARE NOCH MITTELBARE FOLGESCHÄDEN, DIE
DURCH DEN GEBRAUCH, DURCH STÖRUNGEN ODER FEHLFUNKTIONEN DES PRODUKTES
ENTSTEHEN, UNABHÄNGIG DAVON, OB SICH DER ANSPRUCH AUF SCHADENSERSATZ AUF
EINE GARANTIE, EINEN VERTRAG, EINE UNERLAUBTE HANDLUNG ODER EINE ANDERE
ANSPRUCHSGRUNDLAGE STÜTZT.
Die hier aufgeführten Haftungsausschlüsse und -beschränkungen sollen nicht gegen zwingende
gesetzliche Bestimmungen verstoßen und sind nicht dahingehend auszulegen. Sollte ein zuständiges
Gericht feststellen, dass dieser HAFTUNGSAUSSCHLUSS ganz oder teilweise unwirksam, nicht
durchsetzbar oder im Widerspruch zu zwingendem Recht ist, berührt dies die Gültigkeit der restlichen
Klauseln nicht und alle Rechte und Pflichten aus diesem HAFTUNGSAUSSCHLUSS sind so auszulegen
und durchzusetzen, als sei der für ungültig erklärte Teil oder die ungültige Vorschrift in diesem
HAFTUNGSAUSSCHLUSS nicht enthalten.
Gebrauchsanweisung Deutsch 21
Page 24

Page 25

1 DESCRIPCIÓN DEL DISPOSITIVO
El conector apical para el ventrículo izquierdo Hancock Modelo 174A consta de un armazón de
polipropileno flexible diseñado conforme a los mismos principios que condujeron al desarrollo de la
endoprótesis para las bioprótesis valvulares cardíacas aórticas y auriculoventriculares Hancock SGP
(proceso con glutaraldehído estabilizado, por su nombre en inglés). La superficie del conector que entra
en contacto con la sangre del conector está revestida con un material de poliéster tejido de baja porosidad
que se extiende más allá de la endoprótesis de soporte para su anastomosis a un conducto valvulado
Hancock fabricado con el mismo material.
Un anillo de sutura distensible permite suturar el conector al vértice del ventrículo izquierdo. Se
proporciona un anillo de sutura adicional para controlar la profundidad de penetración del conector en el
ventrículo izquierdo.
El conector apical para el ventrículo izquierdo Hancock se encuentra disponible en los tamaños y
dimensiones que se muestran en la Tabla 1.
Tab la 1 . Tamaños y dimensiones disponibles
F
D
C
A
B
E
G
CONECTOR CURVO MODELO 174A
(mm)
TAMAÑO A B C D E F
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Instrucciones de uso Español 23
G
(mínimo)
Page 26

2 INDICACIONES
El conector apical para el ventrículo izquierdo Hancock, utilizado junto con el conducto valvulado Hancock
Modelo 105 (de baja porosidad), proporciona un método alternativo de alivio de la hipertensión del
ventrículo izquierdo en pacientes que presentan una obstrucción marcada del tracto de salida del
ventrículo izquierdo, debida a una hipoplasia de la raíz aórtica o del anillo aórtico o a problemas
adquiridos secundarios a la sustitución de la válvula aórtica, que no puede aliviarse con las técnicas
convencionales.
3 CONTRAINDICACIONES
El conector apical para el ventrículo izquierdo Hancock está contraindicado en pacientes que presenten
cualquiera de los siguientes trastornos:
■
aneurisma del ventrículo izquierdo
■
trombosis
■
reflujo intenso en la válvula aórtica
4ADVERTENCIAS
Este dispositivo está diseñado para su uso en un solo paciente. No reutilice, reprocese ni reesterilice este
producto. La reutilización, el reprocesamiento o la reesterilización del dispositivo pueden poner en peligro
su integridad estructural o generar riesgos de contaminación del mismo que podrían provocar al paciente
lesiones, enfermedades e incluso la muerte.
No utilice el conector en las situaciones siguientes:
■
se ha caído, dañado o manipulado indebidamente de alguna forma
■
ha expirado la fecha de caducidad
Aunque se eligieron materiales clínicamente probados para la reconstrucción arterial con el fin de
utilizarlos en el conector apical para el ventrículo izquierdo Hancock, existe la posibilidad de que se
produzca una pérdida intersticial de sangre, especialmente en pacientes con hemodilución o déficits de
factores de la coagulación.
SE HAN OBSERVADO COMPLICACIONES HEMORRÁGICAS GRAVES EN PACIENTES EN LOS QUE
NO SE HA REALIZADO UNA PRECOAGULACIÓN DEL CONECTOR O DEL CONDUCTO VALVULADO.
ESTE RIESGO POTENCIAL PUEDE MINIMIZARSE MEDIANTE LA PRECOAGULACIÓN DEL
CONECTOR Y DEL CONDUCTO VALVULADO.
Al clampar el conducto valvulado, hágalo a una distancia de al menos 8 cm del anillo metálico.
Seleccione la cuchilla y punta de trocar Hancock apropiada para realizar la ventriculotomía apical
izquierda. Por ejemplo, utilice una cuchilla y punta de trocar Hancock de 14 mm para introducir un
conector apical para el ventrículo izquierdo Hancock de 14 mm.
Examine el trocar antes de usarlo para comprobar que está montado correctamente y que todos los
componentes están fijados de forma segura.
5 MEDIDAS PREVENTIVAS
Se recomienda realizar una ecocardiografía preoperatoria e intraoperatoria a todos los pacientes que se
sometan a este procedimiento.
Precaución: No utilice este producto si el paciente presenta insuficiencia coronaria intensa, enfermedad
oclusiva carotídea intensa o sintomática o enfermedades aneurismáticas de la aorta torácica.
6 POSIBLES EFECTOS ADVERSOS
Se han registrado casos de tromboembolia, aunque infrecuentes. Debe tenerse en cuenta esta posible
complicación al elegir la intervención quirúrgica óptima para cada paciente.
LA HEMORRAGIA ALREDEDOR DE LA ANASTOMOSIS DEL CONECTOR CON EL VÉRTICE PUEDE
MINIMIZARSE MEDIANTE UNA TÉCNICA QUIRÚRGICA APROPIADA Y MEDIANTE LA
PRECOAGULACIÓN DEL CONECTOR Y DEL CONDUCTO VALVULADO.
Puede producirse una reducción significativa de la circulación coronaria y cerebrovascular si existe una
enfermedad intrínseca en estos sistemas.
7 INFORMACIÓN DE ASESORAMIENTO PARA EL PACIENTE
Los pacientes pueden requerir tratamiento anticoagulante, tratamiento antiagregante plaquetario o
ambos durante un período no definido según su estado.
24 Español Instrucciones de uso
Page 27

8 PRESENTACIÓN
8.1 Envasado
El conector apical para el ventrículo izquierdo Hancock se encuentra disponible en los tamaños
siguientes: 12, 14, 16, 18, 20, 22 y 26 mm. El envase contiene un único conector apical para el ventrículo
izquierdo Hancock envasado en bolsas de transferencia estériles de doble asepsia. El sistema de
envasado está diseñado para facilitar la colocación del dispositivo en el campo estéril. El conector se
mantendrá estéril mientras no se abran ni se dañen las bolsas. Las superficies exteriores de la bolsa
externa NO SON ESTÉRILES y, por tanto, no deben colocarse en el campo estéril.
8.2 Almacenamiento
Guarde el producto en su envase original, dentro de la caja de cartón externa, en un lugar limpio, fresco
y seco para protegerlo y reducir al mínimo el riesgo de contaminación. La condición estéril y apirógena
del conducto está validada para permanecer inalterable hasta la fecha "No utilizar después de" indicada
en la caja de cartón, siempre que las bolsas no hayan sido abiertas ni estén dañadas.
Debe llevarse un control adecuado del inventario, de modo que se implanten preferentemente los
conectores cuya fecha de caducidad esté más próxima con objeto de evitar la caducidad de los mismos.
9 INSTRUCCIONES DE USO
9.1 Preparación
Debido a la complejidad y a la variación de los procedimientos quirúrgicos para el bypass
apicoaórtico, la elección del abordaje quirúrgico y de las técnicas de sutura corresponderá al
cirujano. A continuación, se describen técnicas que pueden utilizarse para facilitar la implantación
que han sido comunicadas a Medtronic por cirujanos implantadores.
La inserción del conector apical para el ventrículo izquierdo a menudo se realiza bajo un bypass
cardiopulmonar. La anastomosis a la aorta torácica descendente se realiza a menudo a través de una
toracotomía lateral izquierda en el quinto espacio intercostal.
No existen medidores para el conector. El tamaño apropiado se determina por la capacidad de la cavidad
torácica del paciente en lugar de por métodos tradicionales. Debe utilizarse el conector de mayor tamaño
que encaje en la cavidad torácica y que permita el cierre de la incisión sin causar una presión excesiva
sobre el dispositivo.
La anastomosis del conector y del conducto valvulado puede realizarse antes del bypass cardiopulmonar.
Se recomienda encarecidamente realizar la precoagulación del conector y del conducto valvulado antes
de llevar a cabo estas anastomosis para evitar la pérdida de sangre. Una alternativa es unir el conducto
valvulado a la aorta y el conector al vértice del ventrículo por separado y, a continuación, unir los dos
conductos.
9.2 Implantación del dispositivo
Con el pericardio abierto, se eleva el vértice del ventrículo. Se realiza una sutura en bolsa de tabaco en
el vértice. Se hacen pasar hilos de sutura de poliéster discontinuos a través del miocardio en puntos
equidistantes alrededor del lugar de ventriculotomía definido por la sutura en bolsa de tabaco y el anillo
de sutura del conector. Se practica una pequeña incisión en el vértice y se extrae el tapón miocárdico
(Figuras 1 y 3). Utilice una cuchilla y punta de trocar Hancock Modelo 1701A con un mango de trocar
Hancock Modelo 1701A1, denominados en adelante conjunto de trocar Hancock, para crear una abertura
circular uniforme en el ventrículo y para extraer el tapón miocárdico (Figuras 2a, 2b y 2c). Debe tenerse
cuidado de no dañar el tabique interventricular ni las cuerdas tendinosas ni alterar el flujo coronario. Con
la extensión del conducto clampada en posición distal a la válvula, se introduce el conector en el
ventrículo izquierdo y se sutura en su posición (Figura 4). En este momento puede interrumpirse el
bypass cardiopulmonar bajo el criterio del cirujano.
Después de recortar el extremo distal de la prótesis del conector-conducto valvulado a la longitud
correcta, se realiza una anastomosis terminolateral utilizando un clamp de oclusión parcial (Figura 4). Al
recortar el conducto valvulado debe procurarse eliminar la longitud sobrante que podría causar un
desgaste del tejido por fricción con la pared torácica.
La anastomosis aórtica puede situarse a la altura de la sexta y la séptima arterias intercostales (Figura 5).
Se divide el ligamento pulmonar inferior para permitir la exposición de la aorta torácica descendente.
Con un clamp vascular ocluyendo parcialmente la aorta, se practica una incisión longitudinal con unas
tijeras de ángulo recto. Se anastomosa el extremo distal del conducto valvulado con una sutura de
poliéster continua (Figura 5). Se elimina el aire del ventrículo izquierdo y del conducto valvulado con una
aguja de 20 gauges y, a continuación, se retira el clamp aórtico.
9.3 Accesorios
El conjunto de trocar Hancock, formado por la cuchilla de trocar Hancock Modelo 1701A y por el mango
de trocar Hancock Modelo 1701A1, está diseñado para facilitar la ventriculotomía apical. Utilice
únicamente el conjunto de trocar Hancock para crear una abertura uniforme y limpia en el vértice del
ventrículo izquierdo y para reducir al mínimo la posibilidad de lesión de las cuerdas tendinosas. El
conjunto de trocar Hancock está disponible como conjunto de mango reutilizable que utiliza cuchillas
Instrucciones de uso Español 25
Page 28

cilíndricas de acero inoxidable desechables y las puntas correspondientes en tamaños de 12, 14, 16, 18,
20, 22 y 26 mm, que corresponden al diámetro externo de los conectores. Seleccione el tamaño de
cuchilla y punta que concuerde con el conector para el ventrículo izquierdo utilizado. Examine el conjunto
de trocar Hancock antes de usarlo para comprobar que está montado correctamente y que todos los
componentes están fijados de forma segura. No reutilice la cuchilla de corte.
Instrucciones de montaje
El conjunto de trocar Hancock consta de la punta (a), el eje (b), la cuchilla (c), el soporte de la cuchilla (d),
el mango (e) y el protector terminal (f) (Figuras 6a a 6e).
1. Acople el protector terminal al mango girando el protector en el sentido de las agujas del reloj
(Figura 6a).
2. Acople la cuchilla al soporte girando la cuchilla en el sentido de las agujas del reloj.
Precaución: No sujete la cuchilla cerca del borde de corte (Figura 6b).
3. Deslice el soporte de la cuchilla sobre el eje del mango hasta que el soporte quede completamente
asentado en el interior del mango (Figura 6c).
4. Acople la punta al eje roscado del mango girando la punta en el sentido de las agujas del reloj hasta
que quede bien apretada (Figura 6d).
5. Conjunto de trocar Hancock completo (Figura 6e).
Consulte las instrucciones de uso del trocar Hancock para obtener información detallada sobre su
utilización y esterilización.
Advertencia: No utilice otros trocares ni instrumentos quirúrgicos. La utilización de otros instrumentos
podría no crear una abertura en el ventrículo izquierdo que coincida con el tamaño y la geometría del
conector apical para el ventrículo izquierdo Hancock. Su uso podría causar una hemorragia grave
alrededor del anillo de sutura.
9.4 Esterilización
El conector apical para el ventrículo izquierdo Hancock se suministra ESTÉRIL (por vapor) y no debe
reesterilizarse. No deben utilizarse conectores que estén dañados o que se hayan contaminado por
contacto con el paciente.
10 INFORMACIÓN RELATIVA AL PERÍODO POSOPERATORIO
Este dispositivo no contiene metales y, por tanto, no plantea riesgos conocidos en ningún entorno de
resonancia magnética.
11 INFORMACIÓN SOBRE EL PACIENTE
Nota: El registro de pacientes no es aplicable en países en los que las leyes de privacidad del paciente
entran en conflicto con la provisión de información sobre el paciente, incluidos los países de la
Unión Europea.
Los envases de todos los dispositivos incluyen un formulario de registro del paciente. Después de la
implantación, rellene los datos solicitados. Encontrará el número de serie en el envase y en la etiqueta de
identificación adherida al recipiente de retención. Devuelva el formulario original a la dirección de
Medtronic que consta en en formulario y entregue al paciente la tarjeta de identificación temporal antes
de darle el alta.
Se proporciona al paciente una tarjeta identificativa del dispositivo implantado. La tarjeta contiene el
nombre y el número de teléfono del médico del paciente, así como aquella información que el personal
médico requeriría en caso de urgencia.
26 Español Instrucciones de uso
Page 29

12 RENUNCIA DE RESPONSABILIDAD
LA SIGUIENTE RENUNCIA DE RESPONSABILIDAD SE APLICA SÓLO A LOS CLIENTES DE FUERA
DE LOS ESTADOS UNIDOS:
RENUNCIA DE RESPONSABILIDAD
AUNQUE EL CONECTOR APICAL PARA EL VENTRÍCULO IZQUIERDO HANCOCK
(MODELO 174A), AL QUE NOS REFERIREMOS DE AHORA EN ADELANTE COMO “PRODUCTO”,
HA SIDO DISEÑADO, FABRICADO Y PROBADO CUIDADOSAMENTE ANTES DE PONERLO A LA
VENTA, EL PRODUCTO PUEDE NO CUMPLIR SUS FUNCIONES SATISFACTORIAMENTE POR
DIVERSAS RAZONES. LAS ADVERTENCIAS QUE CONTIENE LA DOCUMENTACIÓN DEL
PRODUCTO PROPORCIONAN INFORMACIÓN MÁS DETALLADA Y SE CONSIDERAN COMO
PARTE INTEGRANTE DE ESTA RENUNCIA DE RESPONSABILIDAD. POR TANTO, MEDTRONIC
RENUNCIA A CUALQUIER RESPONSABILIDAD, TANTO EXPRESA COMO IMPLÍCITA, CON
RESPECTO AL PRODUCTO. MEDTRONIC NO SERÁ RESPONSABLE DE LOS DAÑOS CAUSADOS
O DERIVADOS DE CUALQUIER USO, DEFECTO, FALLO O MAL FUNCIONAMIENTO DEL
PRODUCTO, AUN CUANDO LA RECLAMACIÓN SE BASE EN UNA GARANTÍA, CONTRATO,
RESPONSABILIDAD EXTRACONTRACTUAL U OTROS FUNDAMENTOS LEGALES.
Las exclusiones y limitaciones anteriormente expresadas no pretenden contravenir las disposiciones
obligatorias establecidas por la legislación vigente, ni deben interpretarse de dicha forma. En el supuesto
de que cualquier parte o término de la presente RENUNCIA DE RESPONSABILIDAD sea declarado por
cualquier tribunal competente como ilegal, inaplicable o contrario a la ley, ello no afectará a la validez del
resto de la RENUNCIA DE RESPONSABILIDAD, interpretándose y aplicándose cuantos derechos y
obligaciones se incluyen en ella como si la presente RENUNCIA DE RESPONSABILIDAD no contuviera
la parte o término considerado no válido.
Instrucciones de uso Español 27
Page 30

Page 31

1 PRODUCTBESCHRIJVING
De apicale Hancock-connector voor het linkerventrikel Model 174A bestaat uit een flexibel polypropyleen
frame dat is ontworpen volgens dezelfde principes als die voor de ontwikkeling van de stent voor de
atrioventriculaire en aorta-hartklepbioprothese in het Hancock-proces voor gestabiliseerde
glutaaraldehyde. Het oppervlak van de connector dat met bloed in aanraking komt, is voorzien van
geweven polyester met een lage poreusheid dat doorloopt voorbij de ondersteunende stent voor
anastomose tot een Hancock-conduit met klep die uit hetzelfde materiaal bestaat.
Door een compliant naairing kan de connector op de apex van het linkerventrikel worden vastgehecht. Er
wordt een extra naairing meegeleverd voor de bepaling van de penetratiediepte van de connector in het
linkerventrikel.
De apicale Hancock-connector voor het linkerventrikel is verkrijgbaar in de maten en afmetingen zoals
getoond in Tabel 1.
Tab el 1 . Verkrijgbare maten en afmetingen
F
D
C
A
B
E
G
GEBOGEN CONNECTOR MODEL 174A
(mm)
MAAT A B C D E F
(minimum)
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Gebruiksaanwijzing Nederlands 29
G
Page 32

2 INDICATIES
De apicale Hancock-connector voor het linkerventrikel, voor gebruik in combinatie met de Hancockconduit met klep Model 105 (lage poreusheid), vormt een alternatieve methode voor de verlichting van
hypertensie in het linkerventrikel voor patiënten met ernstige obstructie van de linkerventrikel-outflow,
vanwege hypoplasie van de aortawortel of hypoplasie van de annulus van de aorta, of voor problemen die
zijn ontstaan na vervanging van de aortaklep en waarbij geen verlichting kan worden geboden door middel
van conventionele technieken.
3 CONTRA-INDICATIES
De apicale Hancock-connector voor het linkerventrikel is gecontra-indiceerd voor patiënten met één of
meer van onderstaande aandoeningen:
■
Linkerventrikel-aneurysma
■
Trombose
■
Ernstige aortaklep-reflux
4 WAARSCHUWINGEN
Dit product is uitsluitend bedoeld voor eenmalig gebruik. Niet opnieuw gebruiken of hersteriliseren. Door
het opnieuw gebruiken of hersteriliseren kan het product worden besmet en/of de structuur van het
product worden aangetast, wat kan resulteren in letsel, ziekte of overlijden van de patiënt.
Gebruik de connector niet als:
■
Deze gevallen, beschadigd of op andere wijze verkeerd gebruikt is.
■
De uiterste gebruiksdatum verstreken is.
Hoewel voor de apicale Hancock-connector voor het linkerventrikel klinisch bewezen materialen voor
arteriële reconstructie zijn gebruikt, bestaat er toch een kans op interstitiële bloedingen, met name bij
patiënten met hemodilutie of stollingsfactordeficiënties.
ER ZIJN ERNSTIGE BLOEDINGSCOMPLICATIES GEMELD BIJ DERGELIJKE PATIËNTEN WAARBIJ
DE CONNECTOR EN/OF CONDUIT MET KLEP NIET VOORAF BEHANDELD WAREN MET
ANTISTOLLING. DIT POTENTIËLE GEVAAR KAN WORDEN VERKLEIND DOOR DE CONNECTOR EN
DE CONDUIT MET KLEP VOORAF TE BEHANDELEN MET ANTISTOLLING.
Klem de conduit met klep niet af binnen 8 cm van de metalen ring.
Selecteer het juiste Hancock-trocartmes en -tip voor het uitvoeren van de apicale linker ventriculotomie.
Gebruik bijvoorbeeld een Hancock-trocartmes en -tip van 14 mm voor het inbrengen van een apicale
Hancock-connector van 14 mm.
Controleer vóór gebruik of de trocart juist gemonteerd is en of alle onderdelen stevig bevestigd zijn.
5 VOORZORGSMAATREGELEN
Aanbevolen wordt van alle patiënten die deze procedure ondergaan, een preoperatief en peroperatief
echocardiogram te maken.
Let op: Niet gebruiken bij patiënten met ernstige coronaire insufficiëntie, ernstige of symptomatisch
geoccludeerde carotis, of thoracale aorta-aneurysma.
6 MOGELIJKE COMPLICATIES
Hoewel dit niet frequent voorkomt, is trombo-embolie gemeld. Bij het kiezen van de optimale chirurgische
procedure voor de patiënt moet het risico van deze complicatie worden afgewogen.
BLOEDINGEN ROND DE ANASTOMOSE VAN DE CONNECTOR MET DE APEX KUNNEN WORDEN
GEMINIMALISEERD DOOR HET GEBRUIK VAN EEN GESCHIKTE CHIRURGISCHE TECHNIEK EN
DE CONNECTOR EN DE CONDUIT MET KLEP VOORAF TE BEHANDELEN MET ANTISTOLLING.
Er kan aanzienlijke vermindering van de coronaire en cerebrovasculaire circulatie optreden bij patiënten
met een intrinsieke aandoening.
7 INFORMATIE VOOR PATIËNTBEGELEIDING
De patiënt kan voor onbepaalde tijd antistollingstherapie en/of trombocytenaggregatieremmers nodig
hebben, afhankelijk van de conditie van de patiënt.
8 LEVERING
8.1 Verpakking
De apicale Hancock-connector voor het linkerventrikel is verkrijgbaar in de volgende maten: 12, 14, 16,
18, 20, 22 en 26 mm. De verpakking bevat één apicale Hancock-connector voor het linkerventrikel die in
steriele, dubbelwandige zakken is verpakt. Het verpakkingssysteem is zo ontworpen dat het product
gemakkelijk in het steriele veld kan worden geplaatst. Als de zakken niet beschadigd en niet geopend zijn,
is de connector steriel. De buitenkant van de buitenzak is NIET STERIEL en mag niet in het steriele veld
worden geplaatst.
30 Nederlands Gebruiksaanwijzing
Page 33

8.2 Opslag
Bewaar het product in de originele buitenste kartonnen verpakking op een schone, koele en droge plaats,
om het product te beschermen en de kans op besmetting te beperken. De conduit is steriel en nietpyrogeen tot aan de op de kartonnen verpakking aangegeven uiterste gebruiksdatum, mits de zakken niet
geopend en niet beschadigd zijn.
Er dient goed voorraadbeheer te worden toegepast zodat connectoren met een eerdere vervaldatum als
eerste worden geïmplanteerd en overschrijding van de vervaldatum wordt voorkomen.
9 GEBRUIKSINSTRUCTIES
9.1 Voorbereiden
Vanwege de complexiteit en variatie in chirurgische procedures voor apicoaortabypassprocedures wordt de keuze voor chirurgische benadering en hechttechnieken
overgelaten aan de chirurg. Hieronder staan technieken die chirurgen aan Medtronic gemeld
hebben en die gebruikt kunnen worden bij de implantatie.
Het inbrengen van de apicale connector voor het linkerventrikel wordt vaak uitgevoerd met behulp van
cardiopulmonale bypass. De anastomose met de thoracale aorta descendens wordt vaak uitgevoerd via
een linker laterale thoracotomie-incisie in de vijfde intercostale ruimte.
Er zijn geen sizers beschikbaar voor de connector. De maat wordt bepaald aan de hand van de capaciteit
van de borstholte van de patiënt, niet aan de hand van traditionele standaarden. Gebruik de grootste
connector die in de borstholte past en waarbij de incisie gesloten kan worden zonder overmatige druk op
het product uit te oefenen.
De anastomose van de connector en conduit met klep kan voorafgaand aan de cardiopulmonale bypass
worden uitgevoerd. Om bloedverlies te voorkomen, wordt ten zeerste aanbevolen de connector en conduit
met klep vóór de anatomose te behandelen met antistolling. Het is ook mogelijk eerst de conduit met klep
op de aorta en de connector op de apex van het ventrikel te bevestigen en vervolgens de twee conduits
te verbinden.
9.2 Implantatie
Open het pericard en breng de apex van het ventrikel omhoog. Breng een tabakzaknaad aan bij de apex.
Rond de locatie van de ventriculotomie, die wordt gedefinieerd door de tabakzaknaad en de naairing van
de connector, brengt u op equidistante punten individuele polyester knoophechtingen in het myocard aan.
Maak een kleine steekincisie in de apex en verwijder vervolgens een losgesneden weefselkern uit het
myocard (Afbeelding 1 en 3). Gebruik een Hancock-trocartmes en -tip Model 1701A met Hancocktrocarthandgreep Model 1701A1, hierna Hancock-trocart genoemd, om een uniforme ronde ventriculaire
opening te maken en de losgesneden weefselkern uit het myocard te verwijderen (Afbeelding 2a, 2b en
2c). Voorkom dat het interventriculaire septum of de chordae tendineae beschadigd raken of dat de
bloedstroom in de kransslagaderen belemmerd wordt. Klem de conduitverlenging distaal van de klep af,
breng de connector in het linkerventrikel in en hecht deze op de juiste plaats vast (Afbeelding 4). Naar
inzicht van de chirurg kan de cardiopulmonale bypass nu worden beëindigd.
Snijd het distale uiteinde van de connector/conduit-prothese op de juiste lengte af en maak een end-toside anastomose van de aorta met behulp van een klem waarmee de aorta gedeeltelijk wordt afgeklemd
(Afbeelding 4). Ga voorzichtig te werk bij het afsnijden van de conduit met klep voor het verwijderen van
de overtollige lengte waarvan het materiaal kan verslijten door de wrijving met de borstwand.
De anastomose van de aorta kan aangebracht worden ter hoogte van de zesde en zevende intercostale
slagaderen (Afbeelding 5). Open het inferieure ligamentum pulmonale zodat de thoracale aorta
descendens wordt blootgelegd.
Klem de aorta gedeeltelijk af met een vaatklem en gebruik een schaar met rechte hoek voor het maken
van een longitudinale incisie. Maak met een doorlopende polyester hechting een anastomose aan het
distale uiteinde van de conduit met klep (Afbeelding 5). Verwijder de lucht met een naald van 20 gauge uit
het linkerventrikel en de conduit met klep, en verwijder vervolgens de aortaklem.
9.3 Toebehoren
De Hancock-trocart, die bestaat uit het Hancock-trocartmes Model 1701A en de Hancocktrocarthandgreep Model 1701A1, is ontworpen als hulpmiddel bij een apicale ventriculotomie. Gebruik
uitsluitend de Hancock-trocart om een nette, gelijkmatige opening in het apex van het linkerventrikel te
creëren en de kans op beschadiging van de chordae tendineae te minimaliseren. De Hancock-trocart is
verkrijgbaar als herbruikbare handgreep voor cilindrische roestvrijstalen messen voor eenmalig gebruik
en bijbehorende tips van 12, 14, 16, 18, 20, 22 en 26 mm die overeenkomen met de buitendiameter van
de connectoren. Selecteer voor het mes en de tip de afmeting die overeenkomt met de te gebruiken
connector voor het linkerventrikel. Controleer vóór gebruik of de Hancock-trocart juist gemonteerd is en
of alle onderdelen stevig bevestigd zijn. Gebruik het mes niet opnieuw.
Assemblage-instructies
De Hancock-trocart bestaat uit de tip (a), pen (b), mes (c), meshouder (d), handgreep (e) en dop (f)
(Afbeelding 6a tot en met 6e)
1. Bevestig de dop aan de handgreep door de dop met de klok mee te draaien (Afbeelding 6a).
Gebruiksaanwijzing Nederlands 31
Page 34

2. Bevestig het mes aan de houder door het mes met de klok mee te draaien.
Let op: Houd het mes niet te dicht bij het snijvlak vast (Afbeelding 6b).
3. Schuif de meshouder over de schacht van de handgreep totdat de meshouder volledig in de
handgreep vastzit (Afbeelding 6c)
4. Bevestig de tip op het schroefdraad van de handgreep door de tip met de klok mee te draaien tot deze
vastzit (Afbeelding 6d).
5. De complete Hancock-trocart (Afbeelding 6e).
Raadpleeg de gebruiksaanwijzing bij de Hancock-trocart voor instructies over gebruik en sterilisatie.
Waarschuwing: Gebruik geen andere trocart of chirurgische instrumenten. Door het gebruik van andere
instrumenten kan er een opening in het linkerventrikel gecreëerd worden die niet overeenkomt met de
afmeting en geometrie van de apicale Hancock-connector voor het linkerventrikel. Het gebruik ervan kan
leiden tot ernstige bloedingen rond de naairing.
9.4 Sterilisatie
De apicale Hancock-connector voor het linkerventrikel wordt STERIEL (stoom) geleverd en mag niet
opnieuw worden gesteriliseerd. Connectoren die beschadigd of besmet zijn door contact met de patiënt,
mogen niet worden gebruikt.
10 POSTOPERATIEVE INFORMATIE
Dit product bevat geen metalen en vormt dus geen bekende risico's in alle MR-omgevingen.
11 PATIËNTENINFORMATIE
Opmerking: Patiëntenregistratie is niet van toepassing in landen waar de wetten met betrekking tot
privacy van patiënten in conflict zijn met het verstrekken van patiëntinformatie, inclusief landen binnen
de EU.
In elke verpakking is een patiëntenregistratieformulier ingesloten. Gelieve na implantatie alle gevraagde
informatie in te vullen. Het serienummer vindt u op de verpakking en op het aan de koker bevestigde
identificatielabel. Retourneer het originele formulier naar het adres van Medtronic op het formulier en geef
de tijdelijke identificatiekaart aan de patiënt voordat deze het ziekenhuis verlaat.
De patiënt ontvangt een identificatiekaart voor het geïmplanteerde product. Op de kaart staan de naam
en het telefoonnummer van de arts alsmede andere informatie die medisch personeel bij noodgevallen
nodig kan hebben.
32 Nederlands Gebruiksaanwijzing
Page 35

12 UITSLUITING VAN GARANTIE
DE HIERNAVOLGENDE UITSLUITING VAN GARANTIE GELDT ALLEEN VOOR KLANTEN BUITEN
DE VERENIGDE STATEN:
UITSLUITING VAN GARANTIE
HOEWEL DE APICALE HANCOCK-CONNECTOR VOOR HET LINKERVENTRIKEL (MODEL 174A),
HIERNA HET "PRODUCT" GENOEMD, MET VEEL ZORG IS ONTWORPEN, VERVAARDIGD EN
VÓÓR DE VERKOOP GETEST, KUNNEN ER VERSCHILLENDE REDENEN ZIJN WAAROM HET
PRODUCT NIET VOLGENS DE SPECIFICATIES WERKT. DE WAARSCHUWINGEN IN DE
DOCUMENTATIE BIEDEN MEER GEDETAILLEERDE INFORMATIE EN MOETEN WORDEN
BESCHOUWD ALS EEN WEZENLIJK ONDERDEEL VAN DEZE UITSLUITING VAN GARANTIE.
MEDTRONIC VERLEENT DAAROM GEEN ENKELE GARANTIE, NOCH EXPLICIET NOCH
IMPLICIET, MET BETREKKING TOT HET PRODUCT. MEDTRONIC IS NIET AANSPRAKELIJK VOOR
ENIGE INCIDENTELE OF GEVOLGSCHADE, VEROORZAAKT DOOR OM HET EVEN WELK
GEBRUIK, DEFECT OF FALEN VAN HET PRODUCT, ONGEACHT OF DE VORDERING IS
GEBASEERD OP EEN GARANTIE, CONTRACT, ONRECHTMATIGE DAAD OF ANDERSZINS.
De uitsluitingen en beperkingen die hierboven uiteengezet zijn, zijn niet bedoeld, en moeten niet
geïnterpreteerd worden als een inbreuk op dwingende bepalingen van de van toepassing zijnde wet.
Indien enig onderdeel of enige bepaling van deze UITSLUITING VAN GARANTIE door een daartoe
bevoegde rechtbank als onrechtmatig, onuitvoerbaar of in strijd met de van toepassing zijnde wet
beschouwd wordt, zal dit de geldigheid van het overige deel van deze UITSLUITING VAN GARANTIE niet
aantasten en zullen alle rechten en plichten worden uitgelegd en ten uitvoer worden gebracht alsof deze
UITSLUITING VAN GARANTIE het desbetreffende ongeldig verklaarde gedeelte niet bevatte.
Gebruiksaanwijzing Nederlands 33
Page 36

Page 37

1 DESCRIZIONE DEL DISPOSITIVO
Il connettore apicale per ventricolo sinistro Hancock modello 174A è formato da una struttura flessibile
in polipropilene progettata secondo gli stessi principi che hanno condotto allo sviluppo dello stent per
le bioprotesi valvolari atrioventricolari e aortiche Hancock realizzate tramite procedura di fissazione con
glutaraldeide. La superficie del connettore a contatto con il sangue è rivestita con materiale in poliestere
intrecciato a bassa porosità che si estende oltre lo stent di supporto per l'anastomosi fino a raggiungere
il condotto valvolato Hancock realizzato nello stesso materiale.
Un anello di sutura adattabile permette di suturare il connettore all'apice del ventricolo sinistro. Viene
inoltre fornito un anello di sutura aggiuntivo per controllare la profondità di penetrazione del connettore nel
ventricolo sinistro.
Il connettore apicale per ventricolo sinistro Hancock è disponibile nelle dimensioni e nei diametri riportati
nella Tabella 1.
Tab ell a 1 . Dimensioni e diametri disponibili
F
D
C
A
B
E
G
CONNETTORE RICURVO MODELLO 174A
(mm)
DIMENSIONI A B C D E F
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Istruzioni per l’uso Italiano 35
G
(minimo)
Page 38

2 INDICAZIONI
Il connettore apicale per ventricolo sinistro Hancock, usato insieme alla conduttura con valvola Hancock
Modello 105 (bassa porosità), fornisce un metodo alternativo per la decompressione dell'ipertensione
ventricolare sinistra nei pazienti affetti da grave ostruzione del tratto di uscita del ventricolo sinistro, dovuta
a ipoplasia della radice aortica, ipoplasia dell'anello aortico o a problemi acquisiti in conseguenza della
sostituzione della valvola aortica, che non può essere ottenuta con le tecniche convenzionali.
3 CONTROINDICAZIONI
Il connettore apicale per ventricolo sinistro Hancock è controindicato nei pazienti con i seguenti problemi:
■
aneurisma del ventricolo sinistro
■
trombosi
■
grave reflusso della valvola aortica
4 AVVERTENZE
Il dispositivo è destinato all'utilizzo su un singolo paziente. Non riutilizzare, ritrattare o risterilizzare
il prodotto poiché ciò potrebbe comprometterne l'integrità strutturale e/o comportare un'eventuale
contaminazione dello stesso, con potenziale rischio di lesioni, insorgenza di malattie o decesso
del paziente.
Non utilizzare il connettore se:
■
è caduto, danneggiato o maneggiato male
■
la data di scadenza è stata superata
Sebbene per l'utilizzo con il connettore apicale Hancock per ventricolo sinistro siano stati selezionati
materiali clinicamente testati per la ricostruzione arteriosa, sussiste in ogni caso il rischio potenziale di
perdita di sangue interstiziale, particolarmente nei pazienti con emodiluizione o carenza dei fattori della
coagulazione.
NEI PAZIENTI IN CUI IL CONNETTORE E/O IL CONDOTTO VALVOLATO NON ERANO STATI
PRECOAGULATI SONO STATE RIPORTATE GRAVI COMPLICAZIONI EMORRAGICHE. È POSSIBILE
MINIMIZZARE TALE RISCHIO MEDIANTE LA PRECOAGULAZIONE DEL CONNETTORE E DEL
CONDOTTO VALVOLATO.
Durante la chiusura con clamp incrociato, clampare il condotto valvolato ad almeno 8 cm di distanza
dall'anello metallico.
Selezionare la lama e la punta per trocar Hancock appropriate per eseguire la ventricolotomia apicale
sinistra. Ad esempio, per l'inserimento di un connettore apicale per ventricolo sinistro Hancock da 14 mm,
utilizzare la lama e la punta per trocar Hancock da 14 mm.
Ispezionare il trocar prima dell'uso per verificare il corretto montaggio e fissaggio di tutti i componenti.
5 PRECAUZIONI
Si consiglia che in tutti i pazienti sottoposti a questa procedura venga eseguita un'ecocardiografia pree intraoperatoria.
Attenzione: non usare se sono presenti insufficienza coronarica grave, patologia occlusiva della carotide
sintomatica o grave oppure patologie da aneurismi dell'aorta toracica.
6 POSSIBILI EFFETTI INDESIDERATI
Anche se poco frequentemente, è stato riportata la comparsa di tromboembolismo. È consigliabile tenere
presente la potenzialità di tale complicazione nella scelta della procedura chirurgica ottimale per ciascun
paziente.
L'EMORRAGIA ATTORNO ALL'ANASTOMOSI PRESENTE TRA IL CONNETTORE E L'APICE PUÒ
ESSERE RIDOTTA AL MINIMO UTILIZZANDO LA TECNICA CHIRURGICA APPROPRIATA E LA
PRECOAGULAZIONE DEL CONNETTORE E DEL CONDOTTO VALVOLATO.
In questi sistemi quando è presente una patologia intrinseca è possibile che si verifichi una riduzione
significativa nella circolazione coronaria e cerebrovascolare.
7 RACCOMANDAZIONI PER IL PAZIENTE
In base alle specifiche condizioni di ciascun paziente, potrebbe essere necessario ricorrere ad una terapia
anticoagulante e/o antipiastrinica per una durata indeterminata.
8 FORNITURA
8.1 Confezione
Il connettore apicale per ventricolo sinistro Hancock è disponibile nelle seguenti misure: 12, 14, 16, 18,
20, 22 e 26 mm. La confezione contiene un singolo connettore apicale per ventricolo sinistro Hancock
preparato con una doppia confezione asettica composta da tasche sterili. Il sistema di confezionamento
è ideato per facilitare il posizionamento del dispositivo in campo sterile. Il connettore è sterile a condizione
che le tasche non siano danneggiate e siano chiuse. Le superfici esterne della tasca esterna NON SONO
STERILI e non devono essere collocate nel campo sterile.
36 Italiano Istruzioni per l’uso
Page 39

8.2 Conservazione
Conservare il prodotto con la scatola esterna nella confezione originale in un luogo pulito, fresco e asciutto
per proteggerlo e ridurre al minimo il rischio di contaminazione. Si garantisce che la sterilità e la non
pirogenicità del condotto restano inalterate fino alla data di scadenza stampata sulla confezione esterna,
a condizione che le tasche non vengano aperte o danneggiate.
È necessario eseguire un controllo adeguato dell'inventario in modo da utilizzare prima i connettori con
una data di scadenza più imminente ed evitare quindi che vengano utilizzati quelli già scaduti.
9 ISTRUZIONI PER L'USO
9.1 Preparazione
A causa della complessità e della variabilità delle procedure chirurgiche per l'inserimento del
condotto apico-aortico, la scelta dell'approccio chirurgico e delle tecniche di sutura viene lasciata
a discrezione del singolo chirurgo. Le tecniche qui di seguito riportate sono state indicate alla
Medtronic da chirurghi impiantatori e possono essere utilizzate per facilitare l'impianto del
dispositivo.
L'inserimento del connettore apicale del ventricolo sinistro viene spesso eseguito durante bypass
cardiopolmonare. L'anastomosi sull'aorta toracica discendente viene frequentemente effettuata mediante
un'incisione con toracotomia laterale sinistra a livello del quinto spazio intercostale.
Non sono disponibili misuratori per il connettore. La dimensione viene determinata in base alla capacità
della cavità toracica del paziente e non in base agli standard tradizionali. È necessario utilizzare il
connettore di dimensione maggiore che sia possibile inserire nella cavità toracica ma che comunque
permetta la chiusura dell'incisione senza causare una pressione eccessiva sul dispositivo.
L'anastomosi del connettore e del condotto valvolato può essere eseguita prima del bypass
cardiopolmonare. Per evitare perdite di sangue, si raccomanda vivamente di completare la
precoagulazione del connettore e del condotto valvolato prima di eseguire queste anastomosi. In
alternativa, è possibile anastomizzare separatamente il condotto valvolato all'aorta e il connettore all'apice
del ventricolo e quindi anastomizzare insieme i due condotti.
9.2 Impianto del dispositivo
Una volta inciso il pericardio, viene sollevato l'apice del ventricolo. Sull'apice viene eseguita una sutura
a borsa di tabacco. Vengono apposte suture interrotte in poliestere attraverso il miocardio in punti
equidistanti tra di loro ed intorno la sede della ventricolotomia definita dalla sutura a borsa di tabacco
e dall'anello di sutura del connettore. Sull'apice viene eseguita una piccola incisione e viene asportato un
piccolo tappo di tessuto miocardico (Figure 1 e 3). Utilizzare la lama e la punta per trocar Hancock modello
1701A con il manico per trocar Hancock modello 1701A1, d'ora in avanti chiamati unità trocar Hancock,
per la creazione di un'apertura circolare uniforme nel ventricolo e per l'asportazione del tappo di tessuto
miocardico (Figure 2a, 2b e 2c). Prestare attenzione a non danneggiare il setto interventricolare, le corde
tendinee o il flusso coronarico. Con l'estensione del condotto clampata in posizione distale rispetto alla
valvola, inserire il connettore nel ventricolo sinistro e suturarlo in sede (Figura 4). A discrezione
dell'operatore, a questo punto è possibile interrompere il bypass cardiopolmonare.
Dopo avere accorciato l'estremità distale della protesi formata dal connettore e dal condotto valvolato
secondo la lunghezza desiderata, l'anastomosi termino-laterale viene eseguita dopo avere eseguito
il clampaggio parziale (Figura 4). Durante il taglio del condotto valvolato, prestare attenzione a non
rimuovere una lunghezza eccessiva per evitare di causare l'usura del tessuto dovuto all'attrito causato
dal contatto con la parete toracica.
L'anastomosi aortica può essere identificata a livello della sesta e della settima arteria intercostale
(Figura 5). Il legamento polmonare inferiore viene diviso per consentire l'esposizione dell'aorta toracica
discendente.
Dopo il clampaggio parziale dell'aorta, viene eseguita un'incisione longitudinale con delle forbici ad
angolo retto. L'estremità distale del condotto valvolato viene anastomizzata mediante suture continue
in poliestere (Figura 5). Dal ventricolo sinistro e dal condotto valvolato viene fatta spurgare l'aria mediante
un ago calibro 20 e viene rimosso il clamp vascolare dall'aorta.
9.3 Accessori
L'unità trocar Hancock, che è formato dalla lama per trocar Hancock, Modello 1701A e dall'impugnatura
per trocar Hancock, Modello 1701A1 è stata progettata per facilitare la ventriculotomia apicale. Utilizzare
esclusivamente l'unità trocar Hancock per creare un'apertura uniforma e netta nell'apice del ventricolo
sinistro e per ridurre al minimo la possibilità di danneggiare le corde tendinee. L'unità trocar Hancock
è disponibile come manico riutilizzabile con lame cilindriche monouso in acciaio inossidabile e punte
abbinate da 12, 14, 16, 18, 20, 22 e 26 mm corrispondenti al diametro esterno dei connettori. Selezionare
la lama e la punta della dimensione corrispondente del connettore del ventricolo sinistro da utilizzare.
Esaminare l'unità trocar Hancock prima dell'uso per verificare che sia montata in modo corretto e che
tutti i componenti siano saldamante attaccati. Non riutilizzare la lama.
Istruzioni per l’uso Italiano 37
Page 40

Istruzioni per il montaggio
L'unità trocar Hancock è formata da punta (a), asta (b), lama (c), portalama (d), impugnatura (e) e un
tappo (f) (Figure da 6a a 6e).
1. Attaccare il tappo all'impugnatura girandolo in senso orario (Figura 6a).
2. Attaccare la lama al portalame girandola in senso orario.
Attenzione: non reggere la lama vicino al bordo tagliente (Figura 6b).
3. Fare scorrere il portalama sull'asta dell'impugnatura fino a quando il portalama non è completamente
inserito nell'impugnatura (Figura 6c).
4. Attaccare la punta all'asta filettata sull'impugnatura girandola in senso orario fino a quando non
è serrata (Figura 6d).
5. L'unità trocar Hancock completa (Figura 6e).
Per informazioni dettagliate sull'uso e sulla sterilizzazione, fare riferimento alle istruzioni per l'uso del
trocar Hancock.
Avvertenza: non utilizzare altri trocar o strumenti chirurgici. L'uso di altri strumenti può portare alla
creazione di un'apertura nel ventricolo sinistro non corrispondente alle dimensioni e alla geometria del
connettore apicale Hancock per ventricolo sinistro. L'uso di questi strumenti può provocare una grave
emorragia intorno all'anello di sutura.
9.4 Sterilizzazione
Il connettore apicale per ventricolo sinistro Hancock viene fornito STERILE (sterilizzazione a vapore)
e non può essere risterilizzato. I connettori che presentano danni o sono stati contaminati per essere stati
a contatto con il paziente non devono essere utilizzati.
10 INFORMAZIONI POSTOPERATORIE
Questo dispositivo non contiene metalli, pertanto non è noto alcun pericolo relativo alla sua introduzione
in tutti gli ambienti per la risonanza magnetica (RM).
11 INFORMAZIONI SUL PAZIENTE
Nota: la registrazione dei pazienti non è richiesta nei Paesi in cui la legge sulla privacy è in conflitto con
l'acquisizione dei dati personali dei pazienti, compresi i Paesi dell'Unione europea.
Nella confezione di ogni dispositivo è contenuto un modulo di registrazione del paziente. Dopo l'impianto,
inserire tutte le informazioni richieste. Il numero di serie si trova sulla confezione e sull'etichetta di
identificazione attaccata al dispositivo di ritenuta. Spedire il modulo originale all'indirizzo della Medtronic
riportato sul modulo stesso e consegnare la tessera di identificazione temporanea al paziente prima di
dimetterlo.
Al paziente viene infine consegnata una tessera di identificazione del dispositivo impiantato. La tessera
contiene il nome ed il numero di telefono del medico del paziente e le informazioni utili per il personale
medico in caso di emergenza.
38 Italiano Istruzioni per l’uso
Page 41
12 ESCLUSIONE DALLA GARANZIA
LA SEGUENTE ESCLUSIONE DALLA GARANZIA È VALIDA SOLO PER I CLIENTI AL DI FUORI
DEGLI STATI UNITI:
ESCLUSIONE DALLA GARANZIA
SEBBENE IL CONNETTORE APICALE PER VENTRICOLO SINISTRO HANCOCK MODELLO 174A
DELLA MEDTRONIC, QUI DI SEGUITO INDICATO COME “PRODOTTO”, SIA STATO
ACCURATAMENTE PROGETTATO, REALIZZATO E TESTATO PRIMA DI ESSERE STATO
COMMERCIALIZZATO, IL PRODOTTO POTREBBE NON FUNZIONARE IN MODO SODDISFACENTE
PER DIVERSE RAGIONI. LE AVVERTENZE INDICATE NELLA DOCUMENTAZIONE DEL
PRODOTTO FORNISCONO INFORMAZIONI PIÙ DETTAGLIATE A TALE RIGUARDO E SONO
DA CONSIDERARSI COME PARTE INTEGRANTE DELLA PRESENTE ESCLUSIONE DALLA
GARANZIA. DI CONSEGUENZA, LA MEDTRONIC NON RILASCIA ALCUNA GARANZIA, NÉ
ESPRESSA NÉ TACITA, IN MERITO AL PRODOTTO. LA MEDTRONIC NON PUÒ IN ALCUN
CASO ESSERE RITENUTA RESPONSABILE, NÉ IN VIA CONTRATTUALE NÉ IN VIA
EXTRACONTRATTUALE, PER DANNI DIRETTI OD INDIRETTI CAUSATI DALL'USO, DA DIFETTI
O DA MANCANZE DEL PRODOTTO, INDIPENDENTEMENTE DAL FATTO CHE LA RICHIESTA DI
RISARCIMENTO DI TALI DANNI SIA BASATA SU GARANZIA, CONTRATTO, FATTO ILLECITO
OD ALTRO.
Le esclusioni e le restrizioni di cui sopra non sono intese, né devono essere interpretate in quanto tali,
come contravvenenti alle norme inderogabili della legislazione vigente. Nel caso in cui una parte od un
termine della presente ESCLUSIONE DALLA GARANZIA venga giudicato illegale, inefficace od in
conflitto con il diritto applicabile da un organo giudiziario competente, la validità delle rimanenti parti della
presente ESCLUSIONE DALLA GARANZIA non verrà compromessa e tutti i diritti e gli obblighi verranno
interpretati ed applicati come se la presente ESCLUSIONE DALLA GARANZIA non contenesse la parte
od i termini ritenuti non validi.
Istruzioni per l’uso Italiano 39
Page 42

Page 43

1 BESKRIVELSE
Hancock apikal kobling for venstre ventrikkel, modell 174A, er en bøyelig polypropylenkonstruksjon laget
i samsvar med de samme prinsippene som førte til utviklingen av stenten for Hancock-aortaklaffbioprotese
og Hancock atrioventrikulær hjerteklaffbioprotese med stabilisert glutaraldehydprosess (SGP). Overflaten
på koblingen som kommer i kontakt med blod, er dekket med et vevd polyestermateriale med lav porøsitet,
som fortsetter ut fra stenten for å kunne anastomoseres til et Hancock-ventilavløp laget av samme
materiale.
En elastisk sy-ring gjør det mulig å suturere koblingen til apeks i den venstre ventrikkelen. Det følger med
en ekstra sy-ring som kan brukes til å kontrollere hvor dypt koblingen settes inn i den venstre ventrikkelen.
Hancock apikal kobling for venstre ventrikkel er tilgjengelig i størrelsene og dimensjonene som står
i Tabell 1.
Tab ell 1. Tilgjengelige størrelser og dimensjoner
F
D
C
A
B
E
G
BUET KOBLING, MODELL 174A
(mm)
STØRRELSE A B C D E F
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Bruksanvisning Norsk 41
G
(minimum)
Page 44

2 INDIKASJONER
Hancock apikal kobling for venstre ventrikkel brukt sammen med Hancock-klaffavløp (med lav porøsitet),
modell 105, er en alternativ metode som kan brukes til å behandle hypertensjon i venstre ventrikkel
hos pasienter med kraftig obstruksjon av utløpsgangen i venstre ventrikkel forårsaket av hypoplasi
i aortaroten, hypoplasi i aortaannulus eller ervervede problemer som kan oppstå etter at hjerteklaffen
er skiftet ut, og som ikke kan behandles med konvensjonelle teknikker.
3 KONTRAINDIKASJONER
Hancock apikal kobling for venstre ventrikkel er kontraindisert til pasienter med følgende lidelser:
■
aneurisme i venstre ventrikkel
■
trombose
■
kraftig hjerteklaffrefluks
4 ADVARSLER
Denne enheten er kun beregnet på engangsbruk. Produktet skal ikke brukes, bearbeides eller steriliseres
flere ganger. Hvis produktet brukes, bearbeides eller steriliseres flere ganger, kan dette påvirke produktets
strukturelle integritet og/eller skape en risiko for kontaminering av produktet, noe som kan føre til
pasientskade, sykdom eller død.
Bruk ikke koblingen hvis:
■
den har falt i gulvet, er skadet eller har blitt håndtert feil
■
siste forbruksdag har passert
Selv om det er brukt klinisk dokumenterte materialer for arterierekonstruksjon i Hancock apikal kobling for
venstre ventrikkel, kan det likevel oppstå interstitielt blodtap, spesielt hos pasienter med hemodilusjon
eller koaguleringsforstyrrelser.
DET ER RAPPORTERT OM ALVORLIGE BLØDNINGSKOMPLIKASJONER HOS SLIKE PASIENTER
DER KOBLINGEN OG/ELLER KLAFFAVLØPET IKKE BLE FORHÅNDSKOAGULERT. DENNE
POTENSIELLE FAREN KAN REDUSERES VED Å FORHÅNDSKOAGULERE KOBLINGEN OG
KLAFFAVLØPET.
Når det settes en ekstra klemme på klaffavløpet, må klemmen ikke settes nærmere metallringen enn 8 cm.
Velg egnet Hancock-trokarblad og -tupp til å utføre apikal ventrikulotomi i venstre ventrikkel. Bruk for
eksempel et 14 mm Hancock-trokarblad og -tupp til å sette inn en 14 mm Hancock apikal kobling for
venstre ventrikkel.
Undersøk trokaren før bruk for å sikre at den er riktig montert, og at alle deler er godt festet.
5 FORHOLDSREGLER
Det anbefales både preoperativ og intraoperativ ekkokardiografi for alle pasienter som skal gjennomgå
denne prosedyren.
Forsiktig! Må ikke brukes hvis pasienten har alvorlig koronar insuffisiens, alvorlig eller symptomatisk
karotid okkluderende sykdom eller torakal aortaaneurisme.
6 MULIGE BIVIRKNINGER
Det er rapportert om sjeldne tilfeller av tromboemboli. Muligheten for denne komplikasjonen bør vurderes
når det velges kirurgisk fremgangsmåte for den enkelte pasienten.
BLØDNINGER RUNDT ANASTOMOSEN DER KOBLINGEN GÅR INN I APEKS, KAN REDUSERES
VED EGNET KIRURGISK TEKNIKK OG VED Å FORHÅNDSKOAGULERE KOBLINGEN OG
KLAFFAVLØPET.
Det kan forekomme betydelig reduksjon av koronar og cerebrovaskulær sirkulasjon hvis det er intrinsisk
sykdom i disse systemene.
7 PASIENTRÅDGIVNING
Det kan være nødvendig å behandle pasienten med antikoagulantia og/eller blodplatehemmere i en viss
periode basert på den aktuelle pasientens tilstand.
8 LEVERINGSFORM
8.1 Pakking
Hancock apikal kobling for venstre ventrikkel er tilgjengelig i følgende størrelser: 12, 14, 16, 18, 20, 22 og
26 mm. Pakningen inneholder én Hancock apikal kobling for venstre ventrikkel som er sterilt pakket i doble
aseptiske poser. Pakningen er konstruert slik at det er enkelt å plassere enheten i det sterile feltet.
Koblingen er steril så lenge posene ikke er skadet eller åpnet. Utsiden på ytterposen er USTERIL
og må ikke plasseres i det sterile feltet.
42 Norsk Bruksanvisning
Page 45

8.2 Oppbevaring
Oppbevar produktet i originalemballasjen i ytterkartongen på et rent, kjølig og tørt sted for å beskytte det
og redusere muligheten for kontaminasjon. Avløpet er validert for å holde seg sterilt og pyrogenfritt frem
til siste forbruksdato som er trykt på ytterkartongen, såfremt posene ikke åpnes eller skades.
Roter lagerbeholdningen slik at koblingene med den tidligste forbruksdatoen brukes først. Dermed unngår
du at produktene går ut på dato.
9 INSTRUKSJONER FOR BRUK
9.1 Klargjøring
På grunn av kompleksiteten og variasjonene knyttet til kirurgiske prosedyrer ved apiko-aortabypass
må hver enkelt kirurg selv bestemme kirurgisk fremgangsmåte og sutureringsteknikker. Teknikkene
nedenfor er rapportert til Medtronic av kirurger som har implantert protesen, og kan brukes for at
implantasjonen skal gå lettere.
Den apikale koblingen for venstre ventrikkel settes ofte inn under kardiopulmonal bypass. Anastomose til
aorta descendens i toraks utføres ofte gjennom en venstrelateral torakotomiincisjon i det femte
interkostalrommet.
Det finnes ingen måleinstrumenter for koblingen. Riktig størrelse fastslås ved hjelp av kapasiteten til
pasientens torakshule istedenfor vanlige måter. Bruk den største koblingen som får plass i torakshulen,
samtidig som incisjonen skal kunne lukkes uten at det legges overdrevent trykk på enheten.
Anastomosen til koblingen og klaffavløpet kan utføres før kardiopulmonal bypass. Det anbefales sterkt at
koblingen og klaffavløpet forhåndskoaguleres før disse anastomosene for å unngå blodtap. Et alternativ
er å anastomosere klaffavløpet til aorta og koblingen til apeks i ventrikkelen hver for seg, og deretter
anastomosere de 2 avløpene sammen.
9.2 Implantasjon av enheten
Når perikardet er delt, er apeks i ventrikkelen forhøyet. Lag en sirkulær sutur i apeks. Lag avbrutte
polyestersuturer gjennom myokardet med lik avstand rundt ventrikulotomistedet som definert av den
sirkulære suturen og koblingens sy-ring. Lag et lite stikksår i apeks, og fjern myokardpluggen (Figur 1
og 3). Bruk Hancock-trokarblad og -tupp, modell 1701A, med Hancock-trokarhåndtak, modell 1701A1,
heretter kalt Hancock-trokarsett, til å lage en enhetlig, rund ventrikulær åpning og til å fjerne
myokardpluggen (Figur 2a, 2b og 2c). Pass på at det ikke oppstår skade på skilleveggen mellom
ventriklene, chordae tendineae eller koronarflow. Når avløpsforlengelsen er klemt av distalt for klaffen,
settes koblingen inn i venstre ventrikkel og sutureres på plass (Figur 4). Kirurgen kan velge å avbryte
kardiopulmonal bypass på dette tidspunktet.
Etter å ha klipt av den distale enden på protesen med koblingen og klaffavløpet slik at den får riktig lengde,
opprettes aortaanastomose ende-til-side ved hjelp av en klemme til delvis okklusjon (Figur 4). Vær nøye
når du klipper av klaffavløpet, slik at overflødig materiale fjernes. Hvis avløpet er for langt, kan det føre til
stoffslitasje på grunn av friksjonskontakt med brystveggen.
Aortaanastomosen kan være på nivå med sjette og sjuende interkostalarterier (Figur 5). Del det nedre
pulmonale ligamentet for å eksponere aorta descendens i toraks.
Bruk en karklemme til delvis å okkludere aorta, og lag en langsgående incisjon med en høyrevinklet saks.
Den distale enden på klaffavløpet anastomoseres med en kontinuerlig polyestersutur (Figur 5). Bruk en
20 G kanyle til å fjerne luft fra venstre ventrikkel og klaffavløpet. Fjern deretter klemmen på aorta.
9.3 Tilbehør
Hancock-trokarsettet, som består av Hancock-trokarbladet, modell 1701A, og Hancock-trokarhåndtaket,
modell 1701A1, er utformet for å gjøre det enklere å utføre apikal ventrikulotomi. Bruk kun Hancocktrokarsettet til å lage en tydelig, enhetlig åpning i venstre ventrikkelapeks og for å redusere faren for skade
på chordae tendineae. Hancock-trokarsettet er tilgjengelig som et gjenbrukbart håndtakssett med
sylindriske engangsblader av rustfritt stål og matchende tupper i størrelsene 12, 14, 16, 18, 20, 22 og
26 mm, som tilsvarer koblingenes ytre diameter. Velg bladstørrelsen og tuppen som passer til koblingen
som skal benyttes. Undersøk Hancock-trokarsettet før bruk for å sikre at det er riktig montert, og at alle
deler er godt festet. Bruk ikke skjærebladet flere ganger.
Monteringsinstruksjoner
Hancock-trokarsettet består av tupp (a), stang (b), blad (c), bladholder (d), håndtak (e) og endehette (f)
(Figur 6a–6e).
1. Fest endehetten til håndtaket ved å skru endehetten med klokken (Figur 6a).
2. Fest bladet til holderen ved å skru bladet med klokken.
Forsiktig! Hold ikke bladet i nærheten av skjærekanten (Figur 6b).
3. Skyv bladholderen inn på skaftet på håndtaket til bladholderen er fullstendig på plass inne i håndtaket
(Figur 6c).
4. Fest tuppen til det gjengede skaftet på håndtaket ved å skru tuppen med klokken til den er festet (Figur 6d).
5. Det ferdigmonterte Hancock-trokarsettet (Figur 6e).
Bruksanvisning Norsk 43
Page 46

Du finner mer informasjon om bruk og sterilisering i bruksanvisningen for Hancock-trokaren.
Advarsel! Bruk ikke andre trokarer eller kirurgiske instrumenter. Hvis det benyttes andre instrumenter,
kan det hende at åpningen som lages i venstre ventrikkel, ikke passer til størrelsen og geometrien til
Hancock apikal kobling for venstre ventrikkel. Slik bruk kan føre til kraftig blødning rundt sy-ringen.
9.4 Sterilisering
Hancock apikal kobling for venstre ventrikkel leveres STERIL (damp) og må ikke resteriliseres. Koblinger
som er skadet eller kontaminert på grunn av pasientkontakt, skal ikke brukes.
10 POSTOPERATIV INFORMASJON
Dette produktet inneholder ingen metaller og utgjør derfor ingen kjent risiko i MR-miljøer.
11 PASIENTINFORMASJON
Merk! Pasientregistrering gjelder ikke i land der registrering av personinformasjon strider mot
personvernlover, inkludert land i EU.
Det følger et pasientregistreringsskjema med i hver pakning. Fyll ut samtlige opplysninger etter
implantasjonen. Serienummeret står på pakningen og på identifikasjonsmerket på den indre beholderen.
Returner originalskjemaet til Medtronic på den adressen som er oppgitt på skjemaet, og gi det foreløpige
identifikasjonskortet til pasienten før utskrivingen.
Pasienten får et ID-kort for den implanterte enheten. Kortet inneholder navnet og telefonnummeret til
pasientens lege samt annen informasjon som helsepersonell kan trenge i en akuttsituasjon.
44 Norsk Bruksanvisning
Page 47

12 ANSVARSFRASKRIVELSE
FØLGENDE ANSVARSFRASKRIVELSE GJELDER KUNDER UTENFOR USA:
ANSVARSFRASKRIVELSE
SELV OM HANCOCK APIKAL KOBLING FOR VENSTRE VENTRIKKEL (MODELL 174A), HERETTER
KALT “PRODUKTET”, ER BLITT OMHYGGELIG KONSTRUERT, FREMSTILT OG TESTET FØR
SALG, KAN DET AV EN REKKE GRUNNER LIKEVEL SKJE AT PRODUKTET IKKE OPPFYLLER SIN
TILTENKTE FUNKSJON. ADVARSLENE SOM FINNES I PRODUKTMERKINGEN, INNEHOLDER MER
DETALJERT INFORMASJON OG SKAL BETRAKTES SOM EN UATSKILLELIG DEL AV DENNE
ANSVARSFRASKRIVELSEN. MEDTRONIC FRASIER SEG DERFOR ALT GARANTIANSVAR, BÅDE
DIREKTE OG INDIREKTE, FOR DETTE PRODUKTET. MEDTRONIC PÅTAR SEG IKKE ANSVAR FOR
INDIREKTE SKADER ELLER FØLGESKADER FORÅRSAKET AV BRUK ELLER DEFEKT ELLER
FEIL PÅ PRODUKTET, ENTEN KRAVET ER BASERT PÅ GARANTI, KONTRAKT,
ERSTATNINGSKRAV UTENFOR KONTRAKTSFORHOLD ELLER ANNET.
Unntakene og begrensningene som er angitt ovenfor, er ikke ment å omgå obligatoriske bestemmelser
i gjeldende lov og skal heller ikke tolkes slik. Hvis en ansvarlig rettsinstans finner at en del eller betingelse
i denne ANSVARSFRASKRIVELSEN er ulovlig, ugjennomførlig eller i konflikt med gjeldende lov, skal
gyldigheten til de øvrige delene av ANSVARSFRASKRIVELSEN ikke berøres, og alle retter og plikter skal
tolkes og håndheves som om denne ANSVARSFRASKRIVELSEN ikke inneholdt den bestemte delen
eller betingelsen som ble funnet å være ugyldig.
Bruksanvisning Norsk 45
Page 48

Page 49

1 LAITTEEN KUVAUS
Apikaalinen vasemman kammion Hancock-liitinmalli 174A koostuu joustavasta polypropeenirungosta ja
se on suunniteltu samojen periaatteiden mukaan, jotka johtivat stentin kehittämiseen Hancock SGP
(Stabilized Glutaraldehyde Process) -menetelmää käyttämällä valmistettuja aortan ja atrioventrikulaarisen
sydänläpän bioproteeseja varten. Liittimen veren kanssa kosketuksiin joutuva pinta on päällystetty
vähähuokoisella kudotulla polyesterimateriaalilla, joka ulottuu anastomoosia tukevan stentin yli samasta
materiaalista tehtyyn läpälliseen Hancock-putkeen.
Taipuisa ompelurengas mahdollistaa liittimen ompelemisen vasemman kammion kärkeen kiinni.
Lisäompelurenkaalla voidaan hallita liittimen työntymissyvyyttä vasempaan kammioon.
Apikaalisen vasemman kammion Hancock-liittimen koot ja mitat on esitetty alla (Taulukko 1).
Taulukko 1. Saatavilla olevat koot ja mitat
F
D
C
A
B
E
G
KÄYRÄ LIITINMALLI 174A
(mm)
KOKO A B C D E F
(vähintään)
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Käyttöohjeet Suomi 47
G
Page 50

2 KÄYTTÖAIHEET
Apikaalista vasemman kammion Hancock-liitintä käytetään läpällisen (vähähuokoisen) Hancockputkimallin 105 kanssa vasemman kammion hypertension vaihtoehtoisena hoitomenetelmänä. Sitä
käytetään potilailla, joilla on vaikea vasemman kammion ulosvirtauskanavan tukkeuma, kun tukkeuma
johtuu aortan tyven hypoplasiasta, aortan aukon hypoplasiasta tai aorttaläpän korvaamisesta
seuranneista hankinnaisista ongelmista, joita ei voida helpottaa perinteisillä tekniikoilla.
3 VASTA-AIHEET
Apikaalinen vasemman kammion Hancock-liitin on vasta-aiheinen potilailla, joilla on jokin seuraavista
tiloista:
■
vasemman kammion aneurysma
■
tromboosi
■
vakava aorttaläpän käänteisvirtaus.
4 VAARAT
Laite on kertakäyttöinen. Älä käytä, käsittele tai steriloi tuotetta uudelleen. Uudelleenkäyttö, -käsittely tai
-sterilointi voi heikentää laitteen rakennetta ja/tai kontaminoida laitteen, mikä voi johtaa potilaan vammaan,
sairauteen tai kuolemaan.
Älä käytä liitintä seuraavissa tapauksissa:
■
Se on pudonnut tai vahingoittunut, tai sitä on käsitelty jollain tavalla väärin.
■
Viimeinen käyttöpäivämäärä on ylittynyt.
Vaikka apikaaliseen vasemman kammion Hancock-liittimeen valittiin kliinisesti valtimorekonstruktioon
sopivia materiaaleja, on silti olemassa interstitiaalisen verenvuodon mahdollisuus, erityisesti potilailla,
joilla veri on laimentunut tai joilla on hyytymistekijän puutos.
VAKAVIA VERENVUOTOKOMPLIKAATIOITA ON RAPORTOITU POTILAILLA TAPAUKSISSA, JOISSA
LIITINTÄ JA/TAI LÄPÄLLISTÄ PUTKEA EI OLE PREKOAGULOITU. TÄMÄ MAHDOLLINEN VAARA
VOIDAAN MINIMOIDA PREKOAGULOIMALLA LIITIN JA LÄPÄLLINEN PUTKI.
Kun läpällinen putki ristiinsuljetaan puristimella, älä sulje putkea 8 cm:n etäisyydellä metallirenkaasta.
Valitse sopiva Hancock-troakaariterä ja -kärki vasemman kammion kärjen avaukseen. Käytä esimerkiksi
14 mm:n Hancock-troakaariterää ja -kärkeä 14 mm:n apikaalisen vasemman kammion Hancock-liittimen
sisäänvientiin.
Tutki troakaari ennen käyttöä varmistaaksesi, että kokoonpano on oikea ja että kaikki osat ovat hyvin kiinni.
5 VAROTOIMET
On suositeltavaa, että kaikille potilaille, joille tämä toimenpide tehdään, suoritetaan sydämen kaikukuvaus
ennen leikkausta ja leikkauksen aikana.
Varoitus: Älä käytä tuotetta potilailla, joilla on vaikea sepelvaltimoiden vajaatoiminta, vaikea tai
symptomaattinen kaulavaltimotauti tai rinta-aortan aneurysmatauti.
6 MAHDOLLISET HAITTAVAIKUTUKSET
Joitakin tromboemboliatapauksia on raportoitu. Tämän komplikaation mahdollisuus on otettava huomioon
valittaessa leikkausmenetelmää, joka takaa kullekin potilaalle parhaimman tuloksen.
VERENVUOTO LIITTIMEN ANASTOMOOSIN YMPÄRILLÄ KÄRKEEN VOIDAAN MINIMOIDA
ASIANMUKAISELLA LEIKKAUSTEKNIIKALLA SEKÄ PREKOAGULOIMALLA LIITIN JA LÄPÄLLINEN
PUTKI.
Sepelvaltimo- ja aivoverenkierto voi heikentyä huomattavasti potilailla, joilla on sisäsyntyinen sairaus
sepelvaltimoissa tai aivoverisuonissa.
7 POTILAIDEN HOITOON LIITTYVIÄ TIETOJA
Potilaat saattavat tarvita antikoagulaatiohoitoa ja/tai antitromboottista hoitoa määrittelemättömän ajan
kunkin potilaan tilan mukaan.
8TOIMITUS
8.1 Pakkaus
Apikaalinen vasemman kammion Hancock-liitin on saatavana seuraavina kokoina: 12, 14, 16, 18, 20,
22 ja 26 mm. Pakkaus sisältää yhden apikaalisen vasemman kammion Hancock-liittimen, joka on pakattu
steriiliin, kaksoisaseptiseen siirtopussiin. Kaksinkertainen pakkaus helpottaa laitteen siirtämistä steriilille
alueelle. Liitin on steriili, jos pussit eivät ole vahingoittuneet tai auki. Ulkopussin ulkopuoli EI OLE STERIILI
eikä sitä saa asettaa steriilille alueelle.
48 Suomi Käyttöohjeet
Page 51

8.2 Säilytys
Säilytä tuote alkuperäisessä pakkauksessa (myös päällimmäisessä pahvipakkauksessa) puhtaassa,
viileässä ja kuivassa paikassa. Näin suojaat tuotteen ja vähennät sen kontaminaatioriskiä. Putki pysyy
validoidusti steriilinä ja pyrogeenittomana pahvipakkaukseen merkittyyn viimeiseen käyttöpäivään saakka
sillä ehdolla, että pusseja ei ole avattu eivätkä ne ole vaurioituneet.
Varastoa on hoidettava huolellisesti siten, että ensin käytetään aina aikaisemmin vanhentuvat liittimet.
Näin vältetään viimeisen käyttöpäivän ylittyminen.
9 KÄYTTÖOHJEET
9.1 Valmistelu
Apikaalisen aortan ohituksen monimutkaisuuden ja leikkaustekniikoiden vaihtelun takia
leikkaustavan ja ompelutekniikan valinta on yksittäisen kirurgin harkinnan varassa. Implantoivat
kirurgit ovat raportoineet seuraavia tekniikoita Medtronicille ja niitä voidaan käyttää
implantoinnissa.
Apikaalisen vasemman kammion liittimen sisäänvienti suoritetaan usein potilaan ollessa kytkettynä
sydän-keuhkokoneeseen. Yhdysaukko laskevaan torakaaliseen aorttaan tehdään usein vasemman
lateraalisen torakotomiaviillon avulla viidenteen kylkiluuväliin.
Liittimen koon määrittämiseen ei ole saatavilla apuvälineitä. Koko määräytyy potilaan rintaontelon
perusteella eikä perinteisillä standardeilla. On käytettävä suurinta liitintä, joka mahtuu rintaonteloon
ja mahdollistaa silti insision sulkemisen aiheuttamatta liiallista painetta laitteeseen.
Liittimen ja läpällisen putken yhdysaukko voidaan tehdä ennen potilaan kytkemistä sydänkeuhkokoneeseen. On erittäin suositeltavaa, että liitin ja läpällinen putki prekoaguloidaan ennen
yhdysaukkojen tekemistä verenhukan välttämiseksi. Vaihtoehtoisesti läpällinen putki voidaan yhdistää
aorttaan ja liitin kammion kärkeen erikseen ja sitten yhdistää nämä kaksi putkea toisiinsa.
9.2 Laitteen implantointi
Kun sydänpussi on jaettu, kohota kammion kärkeä. Tee tupakkapussiommel kärkeen. Käytä
polyesteriompeleita ja vie ne katko-ompeleina tasavälein sydänlihaksen läpi ventrikulotomiakohdan
ympärille, jonka tupakkapussiommel ja liittimen ompelurengas määrittävät. Tee pieni viilto kärkeen ja
poista sydänlihaksen tulppa (kuvat 1 ja 3). Käytä Hancock-troakaariterää ja kärkimallia 1701A Hancocktroakaarikahvamallin 1701A1 kanssa (jäljempänä Hancock-troakaarikokoonpano) tasaisen
ympyränmuotoisen kammioaukon luomista ja sydänlihaksen tulpan poistamista varten (kuvat 2a, 2b ja 2c).
Ole huolellinen, ettet vahingoita kammioiden välistä seinämää, jännerihmoja tai sepelvaltimon virtausta. Kun
putken jatko-osa on suljettu puristimella venttiiliin distaalipuolella, vie liitin vasempaan kammioon ja ompele
se paikoilleen (kuva 4). Potilas voidaan tässä vaiheessa irrottaa sydän-keuhkokoneesta harkinnan mukaan.
Kun olet leikannut liitinproteesin / läpällisen putkiproteesin distaalipään oikeanpituiseksi, aortan
anastomoosi päästä sivulle saadaan aikaan käyttämällä osittaista okkluusiopuristinta (kuva 4). Varmista
leikatessasi läpällistä putkea, että poistat ylimääräisen pituuden, joka voi aiheuttaa materiaalin kulumista
rintakehän kosketuksen aiheuttaman kitkan takia.
Aortan anastomoosi voi olla kuudennen ja seitsemännen kylkiluuvälin valtimon tasolla (kuva 5). Jaa
inferiorinen keuhkoligamentti, jotta laskeva torakaalinen aortta paljastuu.
Kun verisuonipuristin tukkii aortan osittain, tee pitkittäinen viilto saksilla, joissa on kulma oikealle.
Läpällisen putken distaalipää yhdistetään jatkuvalla polyesteriompeleella (kuva 5). Poista ilma
vasemmasta kammiosta ja läpällisestä putkesta 20 G:n neulalla ja irrota sitten aortan puristin.
9.3 Lisävarusteet
Hancock-troakaarikokoonpano, joka koostuu Hancock-troakaariterämallista 1701A ja Hancocktroakaarikahvamallista 1701A1, on suunniteltu helpottamaan apikaalista ventrikulotomiaa. Käytä vain
Hancock-troakaarikokoonpanoa siistin, tasaisen aukon tekemiseksi vasemman kammion kärkeen ja
läppäjänteiden vahingoittumisen mahdollisuuden minimoimiseksi. Hancock-troakaarikokoonpano
on saatavilla kestokäyttöisenä kahvakokoonpanona, jossa käytetään kertakäyttöistä lieriömäistä
ruostumattomasta teräksestä valmistettua terää ja vastaavia kärkiä, joiden koot ovat 12, 14, 16, 18, 20,
22 ja 26 mm. Kärkien koot vastaavat liittimien ulkoläpimittaa (OD). Valitse terän ja kärjen koko, joka
vastaa käytettävää vasemman kammion liitintä. Tutki Hancock-troakaarikokoonpano ennen käyttöä
varmistaaksesi, että se on koottu oikein ja että kaikki osat ovat hyvin kiinni. Älä käytä leikkausterää
uudelleen.
Kokoamisohjeet
Hancock-troakaarikokoonpanoon kuuluu kärki (a), varsi (b), terä (c), terän pidike (d), kahva (e) ja
päätytulppa (f) (kuvat 6a–6e).
1. Kiinnitä päätytulppa kahvaan kiertämällä päätytulppaa myötäpäivään (kuva 6a).
2. Kiinnitä terä pidikkeeseen kiertämällä terää myötäpäivään.
Varoitus: Pidä sormet pois leikkaavasta reunasta, kun pitelet terää (kuva 6b).
3. Liu'uta terän pidike kahvan varteen niin, että se asettuu täysin paikalleen kahvan sisään (kuva 6c).
Käyttöohjeet Suomi 49
Page 52

4. Kiinnitä kärki kahvan kierteitettyyn varteen kiertämällä kärkeä myötäpäivään, kunnes se on tiukasti
kiinni (kuva 6d).
5. Valmis Hancock-troakaarikokoonpano (kuva 6e).
Katso lisätiedot käytöstä ja steriloinnista Hancock-troakaarin käyttöohjeista.
Vaara: Älä käytä muita troakaareja tai leikkausvälineitä. Muita työvälineitä käytettäessä vasemman
kammion aukko ei ehkä vastaa apikaalisen vasemman kammion Hancock-liittimen kokoa ja geometriaa.
Niiden käyttö voi johtaa vakavaan verenvuotoon ompelurenkaan ympärillä.
9.4 Sterilointi
Apikaalinen vasemman kammion Hancock-liitin toimitetaan STERIILINÄ (höyrysteriloituna) ja sitä ei saa
steriloida uudelleen. Jos liitin vaurioituu tai kontaminoituu koskettaessaan potilasta, sitä ei saa käyttää.
10 LEIKKAUKSEN JÄLKEISTÄ HOITOA KOSKEVIA TIETOJA
Laite ei sisällä metalleja, joten sillä ei ole tunnettuja riskejä magneettikuvausympäristöissä.
11 POTILASTIEDOT
Huomautus: Potilastietojen rekisteröinti ei koske maita, joissa potilaan yksityisyyttä koskevat lait estävät
potilastietojen antamisen, mukaan lukien EU-maat.
Jokaisen laitteen pakkauksessa on potilasrekisteröintilomake. Täytä kaikki lomakkeen tiedot
implantoinnin jälkeen. Sarjanumero on pakkauksessa ja läppäkoteloon kiinnitetyssä tunnistelapussa.
Palauta alkuperäinen lomake siinä mainittuun Medtronicin osoitteeseen ja anna potilaalle väliaikainen
tunnistekortti ennen kotiuttamista.
Potilaalle toimitetaan implantoidun bioproteesin tunnistekortti. Korttiin on merkitty potilasta hoitavan
lääkärin nimi ja puhelinnumero sekä hätätilanteissa hoitohenkilökunnan tarvitsemia tietoja.
50 Suomi Käyttöohjeet
Page 53

12 TAKUUTA KOSKEVA VASTUUVAPAUSLAUSEKE
SEURAAVA TAKUUTA KOSKEVA VASTUUVAPAUSLAUSEKE KOSKEE YHDYSVALTOJEN
ULKOPUOLISIA ASIAKKAITA:
TAKUUTA KOSKEVA VASTUUVAPAUSLAUSEKE
VAIKKA APIKAALINEN VASEMMAN KAMMION HANCOCK-LIITIN (MALLI 174A), JÄLJEMPÄNÄ ”TUOTE”,
ON SUUNNITELTU, VALMISTETTU JA TESTATTU HUOLELLISESTI ENNEN MYYNTIÄ, USEISTA ERI
SYISTÄ SAATTAA JOHTUA, ETTÄ TUOTE EI TOIMI TARKOITETULLA TAVALLA. TUOTEPAKKAUKSESSA
OLEVAT VAROITUKSET SISÄLTÄVÄT TARKEMPIA LISÄTIETOJA JA KUULUVAT OLENNAISENA OSANA
TÄHÄN TAKUUTA KOSKEVAAN VASTUUVAPAUSLAUSEKKEESEEN. MEDTRONIC EI SITEN VASTAA
MISTÄÄN SUORASTI TAI EPÄSUORASTI ILMAISTUISTA TAKUISTA, JOTKA LIITTYVÄT TUOTTEESEEN.
MEDTRONIC EI OLE VASTUUSSA MISTÄÄN SATUNNAISESTA TAI VÄLILLISESTÄ VAHINGOSTA, JOKA
ON AIHEUTUNUT TUOTTEEN KÄYTÖSTÄ, TUOTTEESSA OLEVASTA VIASTA TAI TUOTTEEN
VIRHEELLISESTÄ TOIMINNASTA, RIIPPUMATTA SIITÄ, PERUSTUUKO VAADE TAKUUSEEN,
SOPIMUKSEEN, OIKEUDENLOUKKAUKSEEN TAI MUUHUN SEIKKAAN.
Yllä mainittuja rajoituksia ei ole tarkoitettu voimassa olevan pakottavan lainsäädännön vastaisiksi, eikä niitä
pidä tällä tavoin tulkita. Mikäli toimivaltainen tuomioistuin katsoo, että jokin tämän TAKUUTA KOSKEVAN
VASTUUVAPAUSLAUSEKKEEN osa tai ehto on laiton, täytäntöönpanokelvoton tai ristiriidassa tapaukseen
sovellettavan lainsäädännön kanssa, TAKUUTA KOSKEVA VASTUUVAPAUSLAUSEKE säilyy kuitenkin
muilta osin voimassa, ja kaikkia oikeuksia ja velvollisuuksia on tulkittava ja pantava täytäntöön ikään kuin tämä
TAKUUTA KOSKEVA VASTUUVAPAUSLAUSEKE ei sisältäisi sitä erityistä osaa tai ehtoa, joka katsotaan
pätemättömäksi.
Käyttöohjeet Suomi 51
Page 54

Page 55

1 BESKRIVNING AV ENHETEN
Hancock apikal vänsterkammarkonnektor, modell 174A, består av en böjlig polypropenram som är
utformad i enlighet med samma principer som ledde till utvecklingen av stentet för Hancock stabiliserad
glutaraldehydprocess (SGP), aorta- och AV-biologisk hjärtklaff. Konnektorns blodkontaktyta är av vävt
polyestermaterial med låg porositet, vilket förlängs bortom det stödjande stentet för anastomosering till
en Hancock-conduit med klaff gjort av samma material.
En eftergivlig suturring tillåter suturering av konnektorn till apex i vänsterkammaren. En ytterligare
suturring tillhandahålls för att kontrollera konnektorns djup vid penetreringen in i vänsterkammaren.
Hancock apikal vänsterkammarkonnektor finns i de storlekar och dimensioner som visas i Tabell 1.
Tab ell 1. Tillgängliga storlekar och dimensioner
F
D
C
A
B
E
G
BÖJD KONNEKTOR, MODELL 174A
(mm)
STORLEK A B C D E F
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Bruksanvisning Svenska 53
G
(minimum)
Page 56

2 INDIKATIONER
Hancock apikal vänsterkammarkonnektor, använd tillsammans med Hancock-conduit med klaff (låg porositet)
modell 105, ger en alternativ metod för lindring av hypertoni i vänster kammare hos patienter med allvarlig
obstruktion av utflödet i vänster kammare p.g.a. hypoplasi av aortaroten, hypoplasi av aortaanulus eller
uppkomna problem sekundära till aortaklaffsutbyte, vilka inte kan lindras med traditionella tekniker.
3 KONTRAINDIKATIONER
Hancock apikal vänsterkammarkonnektor är kontraindicerad hos patienter med något av följande tillstånd:
■
vänsterkammaraneurysm
■
trombos
■
allvarlig aortaklaffinsufficiens
4 VARNINGAR
Den här enheten är endast avsedd för användning på en patient. Denna produkt får ej återanvändas,
omarbetas eller omsteriliseras. Återanvändning, omarbetning eller omsterilisering kan försämra den
strukturella integriteten hos enheten och/eller skapa en risk för kontaminering av enheten, vilket kan
resultera i patientskada, sjukdom eller dödsfall.
Använd inte konnektorn om:
■
den har tappats, skadats eller använts felaktigt på något sätt
■
utgångsdatumet har passerats
Även om kliniskt bevisat material för artärrekonstruktion vore utvalt för användning i Hancock apikal
vänsterkammarkonnektor, finns det fortfarande en risk för interstitiell blodförlust, framförallt hos patienter
med hemodilution eller brister i koagulationsfaktorer.
KOMPLIKATIONER MED ALLVARLIGA BLÖDNINGAR HAR RAPPORTERATS HOS PATIENTER DÄR
KONNEKTOR OCH/ELLER CONDUIT MED KLAFF INTE VAR FÖRKOAGULERADE. DENNA MÖJLIGA
RISK KAN MINIMERAS GENOM FÖRKOAGULERING AV KONNEKTOR OCH CONDUIT MED KLAFF.
Stäng ej conduiten med klämma närmare än 8 cm från metallringen när conduiten med klaff försluts.
Välj lämpligt Hancock troakarblad och -spets för att utföra den apikala vänstra ventrikulotomin. Använd t.ex. ett
Hancock troakarblad och -spets på 14 mm för införing av en Hancock apikal vänsterkammarkonnektor på 14 mm.
Undersök troakaren före användning för att säkerställa korrekt montering och att alla komponenter är
säkert fästa.
5 FÖRSIKTIGHETSÅTGÄRDER
Det rekommenderas att alla patienter som genomgår detta ingrepp får ekokardiografi både före och under
operation.
OBS! Använd inte vid allvarlig kranskärlsinsufficiens, allvarlig eller symptomatisk karotisförträngning eller
aortaaneurysm i thorax.
6 POTENTIELLA BIVERKNINGAR
Tromboemboli har rapporterats vid några få tillfällen. Risken för denna komplikation måste övervägas när
det för patienten optimala kirurgiska ingreppet väljs.
BLÖDNING RUNT ANASTOMOSEN PÅ KONNEKTORN TILL APEX KAN MINIMERAS GENOM
LÄMPLIG KIRURGISK TEKNIK OCH FÖRKOAGULERING AV KONNEKTORN SAMT CONDUITEN
MED KLAFF.
Kranskärls- och cerebrovaskulär cirkulation kan minska avsevärt om det finns inneboende sjukdomar
i dessa system.
7 RÅDGIVANDE INFORMATION
Patienten kan behöva behandling med antikoagulantia och/eller trombocytaggregationshämmande
läkemedel under obestämd tid beroende på respektive patients tillstånd.
8 VID LEVERANS
8.1 Förpackning
Hancock apikal vänsterkammarkonnektor finns tillgänglig i följande storlekar: 12, 14, 16, 18, 20, 22 och 26 mm.
Förpackningen innehåller en enda Hancock apikal vänsterkammarkonnektor, som ligger i en steril, dubbel
aseptisk transportpåse. Förpackningssystemet är utformat för att underlätta placering av enheten i det
sterila området. Konnektorn är steril om påsarna är oskadade och inte har öppnats. Ytterpåsens utsidor
är INTE STERILA och får inte placeras i det sterila området.
8.2 Förvaring
Förvara produkten i originalförpackningen i ytterkartongen på en ren, sval och torr plats så att produkten
skyddas och risken för kontaminering minimeras. Conduitens sterilitet och pyrogenfrihet förblir oförändrade
till och med det Används före-datum som anges på ytterförpackningen, såvida påsarna inte har öppnats
eller skadats.
54 Svenska Bruksanvisning
Page 57

En lämplig inventariekontroll bör upprätthållas, så att konnektorer med tidigare används före-datum
implanteras före klaffar med senare används före-datum.
9 BRUKSANVISNING
9.1 Förberedelse
På grund av komplexiteten och variationen i kirurgiska ingrepp för apiko-aortal bypass, väljer
kirurgen själv kirurgiska metoder och sutureringstekniker. Följande tekniker har rapporterats till
Medtronic av implantationskirurger och kan användas för att underlätta implantation.
Införingen av den apikala vänsterkammarkonnektorn utförs ofta under kardiopulmonell bypass.
Anastomos till den nedåtgående delen av bröstaorta utförs regelbundet genom ett vänster-lateralt
thorakotomisnitt i det femte interkostala utrymmet.
Det finns inga sizers tillgängliga för konnektorn. Storleksval bestäms utifrån kapaciteten av patientens
brösthåla istället för att man utgår ifrån traditionella standarder. Den största konnektorn som passar
i brösthålan och som fortfarande tillåter tillslutning av snittet utan att förorsaka kraftigt tryck på enheten
ska användas.
Anastomosen på konnektor och conduiten med klaff kan utföras före kardiopulmonell bypass. Det
rekommenderas starkt att förkoagulering av konnektor och conduit med klaff avslutas innan dessa
anastomoser görs för att undvika blodförlust. Ett alternativ är att anastomosera conduiten med klaff till
aorta och konnektorn till kammarapex separat, och sedan anastomosera de två conduiterna tillsammans.
9.2 Implantation av enheten
I och med att perikardiet delas blir kammarapex förhöjt. En tobakspungssutur görs vid apex. Avbrutna
polyestersuturer förs igenom myokardiet vid ekvidistanta avståndspunkter runt ventrikulotomiområdet
som definieras av konnektorns tobakspungssutur och suturring. Ett litet sticksnitt görs vid apex och en
myokardipropp tas bort (Figur 1 och 3). Använd Hancock troakarblad och -spets modell 1701A med
Hancock troakarhandtag modell 1701A1, hädanefter kallad Hancock troakaranordning, för att skapa en
uniform cirkulär kammaröppning och ta bort myokardiproppen (Figur 2a, 2b och 2c). Var försiktig så att
inte interventrikulärt septum, chordae tendineae eller koronarflödet skadas. Med conduitförlängningen
stängd med klämma distalt om klaffen, förs konnektorn in i den vänstra kammaren och sutureras på plats
(Figur 4). Kardiopulmonell bypass kan avbrytas vid denna punkt, vilket beslutas av kirurgen.
Efter avkortning till rätt längd av den distala änden på proteskonnektorns conduit med klaff, utförs ände-till-sida
aortaanastomos genom att använda en partiell ocklusionsklämma (Figur 4). Var försiktig vid avkortning
av conduiten med klaff när överbliven längd avlägsnas, eftersom det kan resultera i tygslitage genom
friktionskontakt med bröstväggen.
Aortaanastomosen kan lokaliseras i höjd med de sjätte och sjunde interkostala artärerna (Figur 5). Det
inferiora pulmonella ligamentet är delat för att tillåta exponering av den nedåtgående delen av bröstaorta.
Med en kärlklämma som delvis ockluderar aorta, görs ett längsgående snitt med en högervinklad sax. Den
distala änden av conduiten med klaff är anastomoserad med en kontinuerlig polyestersutur (Figur 5). Luft
avlägsnas från vänster kammare och conduiten med klaff med hjälp av en nål på 20 gauge, och därefter
avlägsnas aortaklämman.
9.3 Tillbehör
Hancock troakaranordningen, som består av Hancock troakarbladet, modell 1701A, och Hancock
troakarhandtaget, modell 1701A1, har utformats för att underlätta apikal ventrikulotomi. Använd endast
Hancock troakaranordningen för att skapa en ren, uniform öppning i vänster kammarapex och för
att minimera risken att skada chordae tendineae. Hancock troakaranordning finns tillgänglig som en
återanvändbar handtagsanordning med cylindriska engångsblad i rostfritt stål och matchande spetsar
i storlekarna 12, 14, 16, 18, 20, 22 och 26 mm, vilka motsvarar ytterdiametern (OD) hos konnektorerna.
Välj storlek på blad och spets som matchar den vänsterkammarkonnektor som ska användas. Undersök
Hancock troakaranordningen före användning för att säkerställa korrekt montering och att alla
komponenter är säkert fästa. Återanvänd inte skärbladet.
Monteringsanvisningar
Hancock troakaranordningen består av spets (a), stång (b), blad (c), bladhållare (d), handtag (e) och
ändskydd (f) (Figur 6a till 6e).
1. Montera ändskyddet på handtaget genom att vrida det medurs (Figur 6a).
2. Montera bladet i hållaren genom att vrida det medurs.
OBS! Håll inte bladet nära eggen (Figur 6b).
3. Skjut bladhållaren på handtagets skaft tills bladhållaren sitter på plats inuti handtaget (Figur 6c).
4. Montera spetsen på handtagets gängade skaft genom att vrida spetsen medurs tills den sitter tätt
(Figur 6d).
5. Färdigmonterad Hancock troakaranordning (Figur 6e).
Ytterligare information om användning och sterilisering finns i bruksanvisningen till Hancock-troakaren.
Bruksanvisning Svenska 55
Page 58

Varning! Använd ej andra troakarer eller kirurgiska verktyg. Det är inte säkert att det går att skapa en
vänsterkammaröppning som matchar storleken och geometrin hos Hancock apikala vänsterkammarkonnektor
vid användning av andra verktyg. Användning av andra verktyg kan resultera i allvarlig blödning runt suturringen.
9.4 Sterilisering
Hancock apikala vänsterkammarkonnektor tillhandahålls STERIL (ånga) och får inte steriliseras om.
Konnektorer som skadats eller kontaminerats genom patientkontakt får inte användas.
10 POSTOPERATIV INFORMATION
Denna enhet innehåller inga metaller och därför finns inga kända risker vid MR-undersökning.
11 PATIENTINFORMATION
Observera: Patientregistrering gäller inte i länder där patientens privaträtt kommer i konflikt med givandet
av patientinformation, inklusive länder inom EU.
Ett formulär för patientregistrering medföljer varje enhet. Fyll i samtliga uppgifter efter implantationen.
Serienumret återfinns på förpackningen och på identifikationsetiketten som sitter på behållaren. Returnera
originalformuläret till Medtronic på den adress som anges på formuläret och ge patienten det tillfälliga
ID-kortet före utskrivning.
Patienten får ett ID-kort till den implanterade enheten. Kortet ger information om läkarens namn och
telefonnummer samt annan information som kan vara nödvändig i en akutsituation.
56 Svenska Bruksanvisning
Page 59

12 FRISKRIVNING FRÅN ANSVAR
FÖLJANDE FRISKRIVNING FRÅN ANSVAR GÄLLER KUNDER UTANFÖR USA:
FRISKRIVNING FRÅN ANSVAR
TROTS ATT HANCOCK APIKAL VÄNSTERKAMMARKONNEKTOR (MODELL 174A), HÄDANEFTER
KALLAD ”PRODUKTEN”, HAR BLIVIT NOGGRANT KONSTRUERAD, TILLVERKAD OCH
KONTROLLERAD FÖRE FÖRSÄLJNING, KAN DET AV OLIKA SKÄL INTRÄFFA ATT PRODUKTEN
ÄR BEHÄFTAD MED FEL ELLER INTE FUNGERAR TILLFREDSSTÄLLANDE. VARNINGSTEXT
PÅ PRODUKTETIKETTEN INNEHÅLLER MERA DETALJERADE UPPLYSNINGAR OCH UTGÖR
EN INTEGRERAD DEL AV DENNA FRISKRIVNING FRÅN ANSVAR. MEDTRONIC FRISKRIVER
SIG DÄRFÖR HELT FRÅN ANSVAR FÖR ALLA FEL I PRODUKTEN. INGA GARANTIER LÄMNAS,
VARE SIG UTTRYCKLIGEN ELLER UNDERFÖRSTÅTT. MEDTRONIC SKALL DÄRFÖR INTE
VARA SKYLDIGT ATT ERSÄTTA NÅGON SKADA, VARE SIG DIREKT ELLER INDIREKT, SOM
UPPKOMMER MED ANLEDNING AV PRODUKTENS UTFORMNING ELLER DESS ANVÄNDNING,
OAVSETT OM KRAVET GRUNDAR SIG PÅ PÅSTÅENDE OM GARANTI, AVTALSBROTT,
SKADEGÖRANDE HANDLING ELLER ANNAT.
Ovan angiven ansvarsbegränsning är inte avsedd att stå i strid med tvingande regler i tillämplig lag, och
den skall inte heller tolkas så. Skulle FRISKRIVNING FRÅN ANSVAR till någon del av behörig domstol
anses ogiltig, verkningslös eller stridande mot tillämplig lag, skall FRISKRIVNING FRÅN ANSVAR gälla
i övrigt, varvid alla rättigheter och skyldigheter skall bestå, som om avtalet inte innehöll den del av garantin
eller FRISKRIVNING FRÅN ANSVAR som underkänts.
Bruksanvisning Svenska 57
Page 60

Page 61

1 ΠΕΡΙΓΡΑΦΗ ΠΡΟΪΟΝΤΟΣ
Ο Διακορυφαίος σύνδεσμος αριστερής κοιλίας Hancock, μοντέλο 174A, αποτελείται από ένα εύκαμπτο
πλαίσιο πολυπροπυλενίου, σχεδιασμένο σύμφωνα με τις ίδιες αρχές που οδήγησαν στη δημιουργία του
stent για τη Διαδικασία σταθεροποιημένης με γλουταραλδεΰδη (SGP: Stabilized Glutaraldehyde Process)
βιοπρόσθεση αορτικής και κολποκοιλιακής καρδιακής βαλβίδας Hancock. Η επιφάνεια του συνδέσμου
που έρχεται σε επαφή με το αίμα είναι επικαλυμμένη με πλεγμένο
διαπερατότητας, το οποίο επεκτείνεται πέρα από το stent στήριξης για αναστόμωση σε βαλβιδοφόρο
μόσχευμα Hancock, κατασκευασμένο από το ίδιο υλικό.
Ένας συμβατός δακτύλιος συρραφής επιτρέπει τη συρραφή του συνδέσμου στην κορυφή της αριστερής
κοιλίας. Ένας πρόσθετος δακτύλιος συρραφής χρησιμοποιείται για τον έλεγχο του βάθους της διείσδυσης
του συνδέσμου στην αριστερή
κοιλία.
Ο διακορυφαίος σύνδεσμος αριστερής κοιλίας Hancock διατίθεται στα μεγέθη και στις διαμέτρους που
απεικονίζονται στον Πίν.1.
Πίνακας 1. Διαθέσιμα μεγέθη και διαστάσεις
πολυεστερικό υλικό χαμηλής
F
D
C
Α
B
Ε
G
ΚΑΜΠΥΛΩΜΕΝΟΣ ΣΥΝΔΕΣΜΟΣ, ΜΟΝΤΕΛΟ 174A
(mm)
ΜΕΓΕΘΟΣ Α BCDΕ F
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Οδηγίες χρήσης Ελληνικά 59
G
(ελάχιστο)
Page 62

2 ΕΝΔΕΙΞΕΙΣ
Ο διακορυφαίος σύνδεσμος αριστερής κοιλίας Hancock, που χρησιμοποιείται σε συνδυασμό με το
βαλβιδοφόρο μόσχευμα Hancock Μοντέλο 105 (χαμηλής διαπερατότητας), αποτελεί μια εναλλακτική
μέθοδο για την ανακούφιση της υψηλής αρτηριακής πίεσης της αριστερής κοιλίας σε ασθενείς με σοβαρή
απόφραξη της οδού εκροής της αριστερής κοιλίας, λόγω υποπλασίας της αορτικής ρίζας, υποπλασίας του
αορτικού δακτύλιου ή
επίκτητα προβλήματα, δευτερογενή ακολούθως της αντικατάστασης αορτικής
βαλβίδας, τα οποία δεν μπορούν να αποκατασταθούν με συμβατικές τεχνικές.
3 ΑΝΤΕΝΔΕΙΞΕΙΣ
Ο διακορυφαίος σύνδεσμος αριστερής κοιλίας Hancock αντενδείκνυνται για ασθενείς οι οποίοι πάσχουν
από οποιαδήποτε από τις ακόλουθες παθήσεις:
■
ανεύρυσμα αριστερής κοιλίας
■
θρόμβωση
■
σοβαρή παλινδρόμηση αορτικής βαλβίδας
4 ΠΡΟΕΙΔΟΠΟΙΗΣΕΙΣ
Το παρόν προϊόν έχει σχεδιαστεί για μία μόνο χρήση σε έναν ασθενή. Μην επαναχρησιμοποιείτε, μην
επανεπεξεργάζεστε και μην επαναποστειρώνετε το παρόν προϊόν. Η επαναχρησιμοποίηση,
επανεπεξεργασία ή επαναποστείρωση ενδέχεται να θέσει σε κίνδυνο τη δομική ακεραιότητα του
προϊόντος ή/και να προκαλέσει κίνδυνο μόλυνσης του προϊόντος, γεγονός που θα μπορούσε να οδηγήσει
σε τραυματισμό, ασθένεια ή θάνατο του ασθενούς.
Μη χρησιμοποιείτε το σύνδεσμο αν:
■
έχει πέσει κάτω, έχει υποστεί ζημιά ή έχει υποβληθεί σε κακό χειρισμό με οποιονδήποτε τρόπο
■
η ημερομηνία «Χρήση έως» έχει παρέλθει
Παρότι τα υλικά που επιλέχθηκαν για χρήση στο διακορυφαίο σύνδεσμο αριστερής κοιλίας Hancock είναι
κλινικώς ελεγμένα για αρτηριακή ανάπλαση, το ενδεχόμενο απώλειας αίματος στον ενδιάμεσο ιστό
εξακολουθεί να υπάρχει, ιδιαίτερα σε ασθενείς με αιμοαραίωση ή με ανεπάρκειες των παραγόντων πήξης
του αίματος.
ΕΧΟΥΝ ΑΝΑΦΕΡΘΕΙ ΣΟΒΑΡΕΣ ΑΙΜΟΡΡΑΓΙΚΕΣ
Ή/ΚΑΙ ΤΟ ΒΑΛΒΙΔΟΦΟΡΟ ΜΟΣΧΕΥΜΑ ΔΕΝ ΥΠΟΒΛΗΘΗΚΕ(-ΑΝ) ΣΕ ΔΙΑΔΙΚΑΣΙΑ ΠΡΟΠΗΞΗΣ.
ΑΥΤΟ Σ Ο ΕΝΔΕΧΟΜΕΝΟΣ ΚΙΝΔΥΝΟΣ ΜΠΟΡΕΙ ΝΑ ΕΛΑΧΙΣΤΟΠΟΙΗΘΕΙ ΜΕ ΠΡΟΠΗΞΗ ΤΟΥ
ΣΥΝΔΕΣΜΟΥ ΚΑΙ ΤΟΥ ΒΑΛΒΙΔΟΦΟΡΟΥ ΜΟΣΧΕΥΜΑΤΟΣ.
Κατά τη διαδικασία σύγκλεισης του βαλβιδοφόρου μοσχεύματος, μην τοποθετείτε σφιγκτήρα στο
μόσχευμα σε απόσταση κάτω των 8cm από το μεταλλικό
Επιλέξτε τον κατάλληλο τύπο λεπίδας και άκρου τροκάρ Hancock για να πραγματοποιήσετε διακορυφαία
αριστερή κοιλιοτομή. Χρησιμοποιήστε, για παράδειγμα, λεπίδα και άκρο τροκάρ Hancock μεγέθους
14 mm για την εισαγωγή ενός διακορυφαίου συνδέσμου αριστερής κοιλίας Hancock 14 mm.
Ελέγξτε το τροκάρ πριν από τη χρήση, για να βεβαιωθείτε για τη σωστή του συναρμολόγηση και την
ασφαλή προσάρτηση
όλων των εξαρτημάτων.
ΕΠΙΠΛΟΚΕΣ ΣΕ ΑΣΘΕΝΕΙΣ ΟΠΟΥ Ο ΣΥΝΔΕΣΜΟΣ
δακτύλιο.
5 ΠΡΟΦΥΛΑΞΕΙΣ
Όλοι οι ασθενείς που θα υποβληθούν σε αυτή τη διαδικασία συνιστάται να υποβληθούν και σε
προεγχειρητικό και διεγχειρητικό ηχοκαρδιογράφημα.
Προσοχή: Μη χρησιμοποιείτε σε περίπτωση σοβαρής στεφανιαίας ανεπάρκειας, σοβαρής ή
συμπτωματικής αποφρακτικής νόσου της καρωτίδας ή όταν υπάρχει ανευρυσματική νόσος θωρακικής
αορτής.
6 ΕΝΔΕΧΟΜΕΝΕΣ ΑΝΕΠΙΘΥΜΗΤΕΣ ΕΝΕΡΓΕΙΕΣ
Έχουν αναφερθεί σπάνιες περιπτώσεις θρομβοεμβολής. Κατά την επιλογή της βέλτιστης χειρουργικής
διαδικασίας για κάθε ασθενή, θα πρέπει να αξιολογείται η πιθανότητα εμφάνισης αυτής της επιπλοκής.
Η ΑΙΜΟΡΡΑΓΙΑ ΓΥΡΩ ΑΠΟ ΤΗΝ ΑΝΑΣΤΟΜΩΣΗ ΤΟΥ ΣΥΝΔΕΣΜΟΥ ΜΕ ΤΗΝ ΚΟΡΥΦΗ ΜΠΟΡΕΙ ΝΑ
ΕΛΑΧΙΣΤΟΠΟΙΗΘΕΙ ΜΕ ΚΑΤΑΛΛΗΛΗ ΧΕΙΡΟΥΡΓΙΚΗ ΤΕΧΝΙΚΗ ΚΑΙ ΜΕ ΠΡΟΠΗΞΗ ΤΟΥ ΣΥΝΔΕΣΜΟΥ
ΚΑΙ ΤΟΥ ΒΑΛΒΙΔΟΦΟΡΟΥ
ΜΟΣΧΕΥΜΑΤΟΣ.
Ενδέχεται να εμφανιστεί σημαντική μείωση στη στεφανιαία και εγκεφαλοαγγειακή κυκλοφορία όταν
υπάρχει ενδογενής νόσος σε αυτά τα συστήματα.
7 ΠΛΗΡΟΦΟΡΙΕΣ ΣΥΜΒΟΥΛΕΥΤΙΚΗΣ ΑΣΘΕΝΩΝ
Οι ασθενείς ενδέχεται να χρειάζονται αντιπηκτική ή/και αντιαιμοπεταλιακή θεραπεία για απροσδιόριστη
χρονική περίοδο, ανάλογα με την πάθηση κάθε ασθενούς.
60 Ελληνικά Οδηγίες χρήσης
Page 63

8 ΤΡΟΠΟΣ ΔΙΑΘΕΣΗΣ
8.1 Συσκευασία
Ο διακορυφαίος σύνδεσμος αριστερής κοιλίας Hancock διατίθεται στα ακόλουθα μεγέθη: 12, 14, 16, 18,
20, 22 και 26 mm. Η συσκευασία περιέχει ένα διακορυφαίο σύνδεσμο αριστερής κοιλίας Hancock,
συσκευασμένο σε στείρους, διπλά άσηπτους σάκους μεταφοράς. Το σύστημα συσκευασίας είναι
σχεδιασμένο να διευκολύνει την τοποθέτηση του προϊόντος στο στείρο πεδίο. Ο σύνδεσμος είναι
αποστειρωμένος αν οι σάκοι είναι άθικτοι και
σάκου ΔΕΝ ΕΙΝΑΙ ΑΠΟΣΤΕΙΡΩΜΕΝΕΣ και δεν πρέπει να τοποθετούνται μέσα στο στείρο πεδίο.
8.2 Αποθήκευση
Αποθηκεύστε το προϊόν στην αρχική συσκευασία του, περιλαμβανομένου και του εξωτερικού χάρτινου
κουτιού, σε καθαρό, δροσερό, ξηρό μέρος για να το προστατεύσετε και για να ελαχιστοποιήσετε τις
πιθανότητες μόλυνσης
πυρετογόνο μέχρι την ημερομηνία «Χρήση έως» που αναγράφεται στο χάρτινο κουτί, υπό την
προϋπόθεση ότι οι σάκοι δεν θα ανοιχτούν και δεν θα αλλοιωθούν.
Θα πρέπει να πραγματοποιείται κατάλληλος έλεγχος του αποθέματος, ώστε να επιλέγονται κατά
προτίμηση προς εμφύτευση οι
παρέλευση της ημερομηνίας λήξης.
. Έχει διασφαλιστεί ότι το μόσχευμα θα παραμείνει αποστειρωμένο και μη
σύνδεσμοι με προγενέστερη ημερομηνία λήξης και να αποφεύγεται η
δεν έχουν ανοιχτεί. Οι εξωτερικές επιφάνειες του εξωτερικού
9 ΟΔΗΓΙΕΣ ΧΡΗΣΗΣ
9.1 Προετοιμασία
Λόγω της πολυπλοκότητας και της πολυμορφίας των χειρουργικών διαδικασιών για διακορυφαία
αορτική παράκαμψη, η επιλογή της χειρουργικής προσπέλασης και των τεχνικών συρραφής
επαφίεται στην κρίση του εκάστοτε χειρουργού. Οι παρακάτω τεχνικές έχουν αναφερθεί στη
Medtronic από χειρουργούς εμφύτευσης και μπορούν να χρησιμοποιηθούν για να διευκολύνουν
την εμφύτευση.
Η εισαγωγή του
καρδιοπνευμονικής παράκαμψης. Η αναστόμωση της κατιούσας θωρακικής αορτής συχνά διεξάγεται
μέσω μιας αριστερής πλευρικής θωρακοτομής στο πέμπτο μεσοπλεύριο διάστημα.
Δεν υπάρχουν μετρητές μεγέθους διαθέσιμοι για το σύνδεσμο. Το μέγεθος καθορίζεται βάσει της
χωρητικότητας της θωρακικής κοιλότητας του ασθενούς και όχι βάσει των συμβατικών
πρέπει να χρησιμοποιείται το μεγαλύτερο μέγεθος συνδέσμου που προσαρμόζεται στη θωρακική
κοιλότητα και παράλληλα επιτρέπει το κλείσιμο της τομής χωρίς να ασκείται υπερβολική πίεση στο προϊόν.
Η αναστόμωση του συνδέσμου και του βαλβιδοφόρου μοσχεύματος μπορεί να πραγματοποιηθεί πριν την
καρδιοπνευμονική παράκαμψη. Για την αποφυγή απώλειας αίματος, συνιστάται θερμά
συνδέσμου και του βαλβιδοφόρου μοσχεύματος πριν από τις αναστομώσεις. Εναλλακτικά, μπορεί να
πραγματοποιηθεί χωριστά αναστόμωση του βαλβιδοφόρου μοσχεύματος με την αορτή και του συνδέσμου
με την κορυφή της κοιλίας και έπειτα να πραγματοποιηθεί αναστόμωση μεταξύ των δύο μοσχευμάτων.
διακορυφαίου συνδέσμου αριστερής κοιλίας πραγματοποιείται συχνά στο πλαίσιο
προτύπων. Θα
η πρόπηξη του
9.2 Εμφύτευση προϊόντος
Με διαχωρισμό του περικαρδίου η κορυφή της κοιλίας
περιρραφής. Διακεκομμένα ράμματα από πολυεστέρα περνούν από το μυοκάρδιο σε σημεία ίσης
απόστασης γύρω από το σημείο κοιλιοτομής, το οποίο ορίζεται από το ράμμα περιρραφής και το δακτύλιο
συρραφής του συνδέσμου. Στην κορυφή δημιουργείται ένα μικρό τραύμα, όπως από αιχμηρό όργανο, και
το μυοκαρδιακό βύσμα
Hancock, μοντέλο 1701A, με τη λαβή τροκάρ Hancock, μοντέλο 1701A1, στο εξής αναφερόμενα ως
«διάταξη τροκάρ Hancock», για τη δημιουργία ενός ομοιόμορφου κυκλικού κοιλιακού ανοίγματος και για
την αφαίρεση του μυοκαρδιακού βύσματος (Εικόνες 2a, 2b και 2c). Πρέπει να είστε ιδιαίτερα προσεκτικοί,
ώστε να μην προκαλέσετε βλάβη στο
ροή. Με την προέκταση του μοσχεύματος περισφιγμένη περιφερικά της βαλβίδας, ο σύνδεσμος εισέρχεται
στην αριστερή κοιλία και συρράβεται στη θέση του (Εικόνα 4). Η καρδιοπνευμονική παράκαμψη μπορεί
να διακοπεί σε αυτό το σημείο, κατά την κρίση του χειριστή.
Αφού κόψετε το άπω άκρο
πραγματοποιήστε αορτική αναστόμωση από άκρο σε πλευρά, χρησιμοποιώντας ένα σφιγκτήρα μερικής
απόφραξης (Εικόνα 4). Θα πρέπει να είστε προσεκτικοί κατά το κόψιμο του βαλβιδοφόρου μοσχεύματος
για την αφαίρεση του περιττού μήκους, καθώς μπορεί να προκληθεί φθορά του υφάσματος λόγω της
τριβής με το θωρακικό
Η αορτική αναστόμωση μπορεί να βρίσκεται στο επίπεδο έκτης και έβδομης μεσοπλεύριας αρτηρίας
(Εικόνα 5). Ο κατώτερος πνευμονικός σύνδεσμος διαχωρίζεται για να επιτρέψει την έκθεση στην κατιούσα
θωρακική αορτή.
Με έναν αγγειακό σφιγκτήρα που αποφράσσει μερικώς την αορτή πραγματοποιείται επιμήκης τομή με ένα
ψαλίδι ορθής γωνίας. Το άπω άκρο του
πολυεστερικό ράμμα (Εικόνα 5). Ο αέρας αφαιρείται από την αριστερή κοιλία και το βαλβιδοφόρο
μόσχευμα με μια βελόνα 20 gauge και έπειτα ο αορτικός σφιγκτήρας αφαιρείται.
αφαιρείται (Εικόνες 1 και 3). Χρησιμοποιήστε τη λεπίδα και το άκρο τροκάρ
μεσοκοιλιακό διάφραγμα, στις τενόντιες χορδ ές ή στη στεφανιαία
της πρόσθεσης συνδέσμου-βαλβιδοφόρου μοσχεύματος στο σωστό μήκος,
τοίχωμα.
βαλβιδοφόρου μοσχεύματος αναστομώνεται με ένα συνεχόμενο
ανυψώνεται. Στην κορυφή πραγματοποιείται ράμμα
Οδηγίες χρήσης Ελληνικά 61
Page 64

9.3 Παρελκόμενα
Η διάταξη τροκάρ Hancock, η οποία αποτελείται από τη λεπίδα τροκάρ Hancock, Μοντέλο 1701A και τη
λαβή τροκάρ Hancock, Μοντέλο 1701A1, έχει σχεδιαστεί για να διευκολύνει τη διακορυφαία κοιλιοτομή.
Χρησιμοποιήστε μόνο τη διάταξη τροκάρ Hancock για να δημιουργήσετε ένα καθαρό, ομοιόμορφο
άνοιγμα στην κορυφή της αριστερής κοιλίας και να ελαχιστοποιήσετε το ενδεχόμενο βλάβης στις τενόντιες
χορδές
. Η διάταξη τροκάρ Hancock είναι διαθέσιμη ως επαναχρησιμοποιούμενο συναρμολόγημα
χειρισμού, που περιλαμβάνει κυλινδρικές ατσάλινες λεπίδες μίας χρήσης και αντίστοιχα άκρα σε μεγέθη
12, 14, 16, 18, 20, 22 και 26 mm, που αντιστοιχούν στην εξωτερική διάμετρο (Ε.Δ.) των συνδέσμων.
Επιλέξτε το μέγεθος λεπίδας και άκρου που ταιριάζει με το σύνδεσμο αριστερής κοιλίας που θα
χρησιμοποιηθεί. Ελέγξτε τη διάταξη
της συναρμολόγηση και την ασφαλή προσάρτηση όλων των εξαρτημάτων. Μην επαναχρησιμοποιείτε τη
λεπίδα τομής.
Οδηγίες συναρμολόγησης
Η διάταξη τροκάρ Hancock αποτελείται από το άκρο (a), τη ράβδο (b), τη λεπίδα (c), το στήριγμα
λεπίδας (d), τη λαβή (e) και το τελικό πώμα (f) (Εικόνες 6a έως 6e).
1. Προσαρτήστε
2. Προσαρτήστε τη λεπίδα στο στήριγμα περιστρέφοντας τη λεπίδα δεξιόστροφα.
Προσοχή: Μην κρατάτε τη λαβή κοντά στο αιχμηρό άκρο (Εικόνα 6b).
3. Σύρετε το στήριγμα λαβίδας επάνω στον άξονα της λαβής μέχρι το στήριγμα λαβής να εδράσει πλήρως
εντός της λαβής (Εικόνα
4. Προσαρτήστε το άκρο στον κοχλιωτό άξονα της λαβής περιστρέφοντας το άκρο δεξιόστροφα μέχρι να
σφίξει (Εικόνα 6d).
5. Η ολοκληρωμένη διάταξη τροκάρ Hancock (Εικόνα 6e).
Ανατρέξτε στις οδηγίες χρήσης του τροκάρ Hancock για λεπτομερείς πληροφορίες σχετικά με τη χρήση
και την αποστείρωση.
Προειδοποίηση: Μην χρησιμοποιείτε άλλο τροκάρ ή άλλα χειρουργικά εργαλεία. Η χρήση άλλων
εργαλείων μπορεί να μην δημιουργήσει άνοιγμα στην αριστερή κοιλία το οποίο να ταιριάζει στο μέγεθος
και στη γεωμετρία του διακορυφαίου συνδέσμου αριστερής κοιλίας Hancock. Η χρήση τους μπορεί να
προκαλέσει σοβαρή αιμορραγία γύρω από το δακτύλιο συρραφής.
το τελικό πώμα στη λαβή περιστρέφοντας το τελικό πώμα δεξιόστροφα (Εικόνα 6a).
τροκάρ Hancock πριν από τη χρήση για να βεβαιωθείτε για τη σωστή
6c).
9.4 Αποστείρωση
Ο διακορυφαίος σύνδεσμος αριστερής κοιλίας Hancock διατίθεται ΑΠΟΣΤΕΙΡΩΜΕΝΟΣ (με χρήση ατμού)
και δεν επιτρέπεται να
την επαφή με τον ασθενή δεν πρέπει να χρησιμοποιούνται.
επαναποστειρώνεται. Σύνδεσμοι που έχουν υποστεί βλάβη ή έχουν μολυνθεί από
10 ΜΕΤΕΓΧΕΙΡΗΤΙΚΕΣ ΠΛΗΡΟΦΟΡΙΕΣ
Το παρόν προϊόν δεν περιέχει μέταλλα και συνεπώς δεν θέτει κάποιο γνωστό κίνδυνο σε όλα τα
περιβάλλοντα MR.
11 ΠΛΗΡΟΦΟΡΙΕΣ ΓΙΑ ΤΟΝ ΑΣΘΕΝΗ
Σημείωση: Η εγγραφή ασθενούς δεν ισχύει για χώρες όπου οι νόμοι περί απορρήτου του ασθενούς
έρχονται σε διένεξη με την παροχή πληροφοριών για τον ασθενή, συμπεριλαμβανομένων των χωρών της
ΕΕ.
Σε κάθε συσκευασία του προϊόντος υπάρχει ένα έντυπο εγγραφής ασθενούς. Μετά την εμφύτευση,
παρακαλούμε συμπληρώστε όλες τις απαιτούμενες πληροφορίες. Ο αριθμός
συσκευασία και στην αναγνωριστική ετικέτα που είναι προσαρτημένη στον κύλινδρο συγκράτησης.
Επιστρέψτε το πρωτότυπο έντυπο στη Medtronic, στη διεύθυνση που αναγράφεται στο έντυπο και δώστε
την προσωρινή κάρτα αναγνώρισης στον ασθενή πριν λάβει εξιτήριο.
Στον ασθενή δίνεται μια κάρτα αναγνώρισης του εμφυτευμένου προϊόντος. Στην κάρτα αυτή αναγράφονται
το
όνομα και ο αριθμός τηλεφώνου του ιατρού του ασθενούς, καθώς και πληροφορίες που θα είναι
χρήσιμες στο ιατρικό προσωπικό σε περίπτωση ανάγκης.
σειράς αναφέρεται στη
62 Ελληνικά Οδηγίες χρήσης
Page 65

12 ΑΠΟΠΟΙΗΤΙΚΗ ΔΗΛΩΣΗ ΤΗΣ ΕΓΓΥΗΣΗΣ
Η ΑΚΟΛΟΥΘΗ ΑΠΟΠΟΙΗΤΙΚΗ ΔΗΛΩΣΗ ΤΗΣ ΕΓΓΥΗΣΗΣ ΙΣΧΥΕΙ ΜΟΝΟ ΓΙΑ ΠΕΛΑΤΕΣ ΕΚΤΟΣ ΤΩΝ
ΗΝΩΜΕΝΩΝ ΠΟΛΙΤΕΙΩΝ:
ΑΠΟΠΟΙΗΤΙΚΗ ΔΗΛΩΣΗ ΕΓΓΥΗΣΗΣ
ΠΑΡΟΤΙ Ο ΔΙΑΚΟΡΥΦΑΙΟΣ ΣΥΝΔΕΣΜΟΣ ΑΡΙΣΤΕΡΗΣ ΚΟΙΛΙΑΣ HANCOCK (ΜΟΝΤΕΛΟ 174Α),
ΕΦΕΞΗΣ ΑΝΑΦΕΡΟΜΕΝΟΣ ΩΣ «ΠΡΟΪΟΝ», ΕΧΕΙ ΣΧΕΔΙΑΣΤΕΙ, ΚΑΤΑΣΚΕΥΑΣΤΕΙ ΚΑΙ ΔΟΚΙΜΑΣΤΕΙ
ΠΡΟΣΕΚΤΙΚΑ ΠΡΙΝ ΤΗΝ ΠΩΛΗΣΗ ΤΟΥ, ΤΟ ΠΡΟΪΟΝ ΜΠΟΡΕΙ ΝΑ ΑΠΟΤΥΧΕΙ ΣΤΗΝ ΕΚΤΕΛΕΣΗ ΤΗΣ
ΛΕΙΤΟΥΡΓΙΑΣ ΓΙΑ ΤΗΝ ΟΠΟΙΑ ΠΡΟΟΡΙΖΕΤΑΙ ΛΟΓΩ ΔΙΑΦΟΡΩΝ ΑΙΤΙΩΝ. ΟΙ ΠΡΟΕΙΔΟΠΟΙΗΣΕΙΣ
ΠΟΥ ΠΕΡΙΕΧΟΝΤΑΙ ΣΤΗ ΣΗΜΑΝΣΗ ΤΟΥ ΠΡΟΪΟΝΤΟΣ ΠΑΡΕΧΟΥΝ ΠΕΡΙΣΣΟΤΕΡΟ
ΠΛΗΡΟΦΟΡΙΕΣ ΚΑΙ ΘΕΩΡΟΥΝΤΑΙ ΑΚΕΡΑΙΟ ΤΜΗΜΑ ΤΗΣ ΠΑΡΟΥΣΑΣ ΑΠΟΠΟΙΗΤΙΚΗΣ ΔΗΛΩΣΗΣ
ΤΗΣ ΕΓΓΥΗΣΗΣ. ΣΥΝΕΠΩΣ, Η MEDTRONIC, ΑΠΟΠΟΙΕΙΤΑΙ ΟΛΕΣ ΤΙΣ ΕΓΓΥΗΣΕΙΣ, ΡΗΤΕΣ ΚΑΙ
ΣΙΩΠΗΡΕΣ, ΟΣΟΝ ΑΦΟΡΑ ΣΤΟ ΠΡΟΪΟΝ. H MEDTRONIC ΔΕΝ ΘΑ ΕIΝΑΙ ΥΠΕYΘΥΝΗ ΓΙΑ
ΟΠΟΙΕΣΔHΠΟΤΕ ΘΕΤΙΚΕΣ ΚΑΙ ΑΠΟΘΕΤΙΚΕΣ ΖΗΜΙΕΣ ΠΡΟΚΑΛΟΥΜΕΝΕΣ ΑΠΟ ΚΑΘΕ ΧΡΗΣΗ,
ΕΛΑΤΤΩΜΑ Ή ΑΠΟΤΥΧΙΑ ΤΟΥ ΠΡΟΪΟΝΤΟΣ, ΑΝΕΞΑΡΤΗΤΩΣ ΤΟΥ ΑΝ Η
ΕΓΓΥΗΣΗ, ΣΥΜΒΟΛΑΙΟ, ΑΔΙΚΟΠΡΑΞΙΑ Ή ΟΤΙΔΗΠΟΤΕ ΑΛΛΟ.
Οι εξαιρέσεις και οι περιορισμοί που ορίζονται ανωτέρω δεν έχουν σκοπό και δεν θα πρέπει να
ερμηνεύονται κατά τέτοιο τρόπο, ώστε να αντίκεινται στις υποχρεωτικές διατάξεις της ισχύουσας
νομοθεσίας. Εάν οποιοδήποτε μέρος ή όρος της παρούσας ΑΠΟΠΟΙΗΤΙΚΗΣ ΔΗΛΩΣΗΣ ΤΗΣ ΕΓΓΥΗΣΗΣ
κριθεί παράνομο(ς), μη εφαρμόσιμο
αρμόδιας δικαιοδοσίας, η ισχύς των υπολείπων τμημάτων της παρούσας ΑΠΟΠΟΙΗΤΙΚΗΣ ΔΗΛΩΣΗΣ
ΤΗΣ ΕΓΓΥΗΣΗΣ δεν θα επηρεάζεται και όλα τα δικαιώματα και οι υποχρεώσεις θα ερμηνεύονται και θα
εφαρμόζονται όπως εάν η παρούσα ΑΠΟΠΟΙΗΤΙΚΗ ΔΗΛΩΣΗ ΤΗΣ ΕΓΓΥΗΣΗΣ δεν περιείχε το
συγκεκριμένο
μέρος ή όρο που κρίθηκε άκυρο(ς).
(ς) ή αντίθετο(ς) προς την ισχύουσα νομοθεσία από δικαστήριο
ΑΠΑΙΤΗΣΗ ΒΑΣΙΖΕΤΑΙ ΣΕ
ΛΕΠΤΟΜΕΡΕΙΣ
Οδηγίες χρήσης Ελληνικά 63
Page 66

Page 67

1 BESKRIVELSE
Hancock apikale venstre ventrikel-konnektor model 174A består af et fleksibelt polypropylenydre, der er
konstrueret i overensstemmelse med de samme principper som dem, der førte til udviklingen af stenten
til Hancock SGP (Stabilized Glutaraldehyde Process) aorta- og atrioventrikulære hjerteklap-bioprotese.
Den del af konnektorens flade, der kommer i kontakt med blod, er beklædt med et vævet polyestermateriale med lav porøsitet, som strækker sig ud over den støttende stent til anastomose til en Hancockconduit m. klap, der er fremstillet af samme materiale.
En smidig syring muliggør suturering af konnektoren til apex på venstre ventrikel. Der medfølger også en
syring til kontrol af dybden af konnektorens penetrering i venstre ventrikel.
Hancock apikale venstre ventrikel-konnektor kan leveres i de størrelser og mål, der er vist i Tabel 1.
Tab el 1. Tilgængelige størrelser og mål
F
D
C
A
B
E
G
BUET KONNEKTOR MODEL 174A
(mm)
STR A B C D E F
(minimum)
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Brugsanvisning Dansk 65
G
Page 68

2 INDIKATIONER
Hancock apikale venstre ventrikel-konnektor, anvendt i kombination med Hancock conduit m. klap (lav
porøsitet) model 105, udgør en alternativ metode til aflastning af venstre ventrikel hypertension hos
patienter med alvorlig venstresidig ventrikulær obstruktion i udløbsdelen på grund af hypoplasi af
aortaroden, hypoplasi af aorta-annulus eller opståede problemer i forbindelse med udskiftning af
aortaklap, som ikke kan aflastes ved konventionel teknik.
3 KONTRAINDIKATIONER
Hancock apikale venstre ventrikel-konnektor er kontraindiceret for patienter med en eller flere af følgende
tilstande:
■
aneurisme i venstre ventrikel
■
trombose
■
alvorlig tilbageløb for aortaklap
4 ADVARSLER
Enheden må kun anvendes på én patient. Dette produkt må ikke bruges flere gange, genbehandles eller
resteriliseres. Brug flere gange, genbehandling eller resterilisering kan forringe enhedens strukturelle
integritet og/eller medføre risiko for tilsmudsning af enheden, hvilket kan føre til personskade, sygdom
eller død for patienten.
Konnektoren må ikke bruges, hvis:
■
den er blevet tabt, beskadiget eller på anden måde håndteret forkert
■
udløbsdatoen er overskredet
Selvom der blev valgt materialer, som er klinisk godkendt til arteriel rekonstruktion, til brug i Hancock
apikale venstre ventrikel-konnektor, er der stadig risiko for interstitielt blodtab, især hos hæmodilaterede
patienter eller patienter med koagulationsdefekter.
DER ER RAPPORTERET ALVORLIGE BLØDNINGSKOMPLIKATIONER HOS DISSE PATIENTER,
HVOR KONNEKTOREN OG/ELLER CONDUIT M. KLAP IKKE BLEV PRÆKLOTTET. DENNE
POTENTIELLE RISIKO KAN MINIMERES VED AT PRÆKLOTTE KONNEKTOREN OG CONDUIT M.
KLAP.
Ved tværafklemning af conduit m. klap må conduit ikke afklemmes inden for 8 cm fra metalringen.
Vælg den korrekte Hancock-trokarkniv og -spids til at udføre apikal venstresidig ventrikulotomi. Brug f.eks.
en str. 14 mm Hancock-trokarkniv og -spids til indføring af str. 14 mm Hancock apikale venstre ventrikelkonnektor.
Kontrollér trokaren inden brug for at bekræfte korrekt samling, og at alle komponenter er fæstnet sikkert.
5 FORHOLDSREGLER
Det anbefales, at patienter, der får foretaget denne procedure, gennemgår både præoperativ og
intraoperativ ekkokardiografi.
Forsigtig: Må ikke bruges, hvis der er alvorlig koronar insufficiens, alvorlige eller symptomatiske carotisokklusive sygdomme eller torakale aorta-aneurismale sygdomme.
6 MULIGE KOMPLIKATIONER
Der er, skønt det er sjældent, rapporteret tromboembolisme. Risikoen for denne komplikation skal afvejes
for hver enkelt patient, når det optimale kirurgiske indgreb skal udvælges.
BLØDNING OMKRING ANASTOMOSEN MELLEM KONNEKTOREN OG APEX KAN MINIMERES VED
KORREKT KIRURGISK TEKNIK OG VED AT PRÆKLOTTE KONNEKTOREN OG CONDUIT M. KLAP.
Signifikant nedsættelse af den koronare og cerebrovaskulære cirkulation kan forekomme, når der er en
spontan lidelse i disse systemer.
7 PATIENTRÅDGIVNING
Patienter skal eventuelt have antikoagulationsbehandling og/eller trombocytfunktionshæmmende
behandling i en ubestemt periode baseret på den enkelte patients tilstand.
8 LEVERING
8.1 Emballage
Hancock apikale venstre ventrikel-konnektor kan leveres i følgende størrelser: 12, 14, 16, 18, 20, 22 og
26 mm. Emballagen indeholder en enkelt Hancock apikale venstre ventrikel-konnektor, der er pakket i
sterile, dobbelt-aseptiske overførselsposer. Emballagesystemet er konstrueret til at lette placering af
enheden i det sterile område. Konnektoren er steril, hvis poserne er ubeskadigede og uåbnede.
Yderposens udvendige overflader er IKKE-STERILE og må ikke komme ind i det sterile område.
66 Dansk Brugsanvisning
Page 69

8.2 Opbevaring
Opbevar produktet i den originale emballage - inklusive den udvendige opbevaringsæske - på et rent,
køligt og tørt sted, så produktet beskyttes, og risikoen for forurening minimeres. Steriliteten og de ikkepyrogene egenskaber af conduit er valideret til at forblive upåvirkede, indtil udløbsdatoen, som står på
opbevaringsæsken, under forudsætning af at poserne ikke er åbnede eller beskadigede.
Der bør føres passende lagerkontrol for at sikre, at konnektorer med tidligere udløbsdatoer foretrækkes
ved implantering, så overskridelse af udløbsdatoen undgås.
9 BRUGSANVISNING
9.1 Forberedelse
På grund af kompleksiteten og variationen i de kirurgiske procedurer ved apico-aorta bypass
overlades valget af kirurgisk fremgangsmåde og sutureringsteknik til den enkelte kirurg. De
følgende teknikker er rapporteret til Medtronic af kirurger og kan bruges til at lette implanteringen.
Indføringen af den apikale venstre ventrikel-konnektor foretages ofte under kardiopulmonale bypassoperationer. Anastomose til thorakal aorta descendens foretages ofte ved hjælp af venstresidig
thorakotomi-incision i femte interkostale rum.
Der findes ikke størrelsesmålere til konnektoren. Størrelsen bestemmes ud fra patientens thorakale
kapacitet og ikke traditionelle standarder. Der skal anvendes den størst mulige konnektor, der kan passes
ind i thoraxhulen og stadig muliggør lukning af incisionen, uden at dette medfører overdrevent tryk på
enheden.
Anastomosen mellem konnektoren og conduit m. klap kan foretages inden den kardiopulmonale bypass.
Det anbefales på det kraftigste at præklotte konnektoren og conduit m. klap før anastomosering for at
undgå blodtab. Et alternativ er at anastomosere conduit m. klap med aorta og konnektoren med apex af
ventriklen separat og derefter anastomosere de 2 conduit'er.
9.2 Implantering af enheden
Ved åbning af perikardiet eleveres apex af ventriklen. Der laves en tobaksposesutur ved apex. Afbrudte
polyestersuturer føres gennem myokardiet ved punkter med lige stor afstand omkring ventrikulotomistedet, der er defineret af tobaksposesuturen og konnektorens syring. Der laves et lille indstik ved apex,
og udtages en prop fra myokardiet (Figur 1 og 3). Brug Hancock-trokarkniv og -spids model 1701A med
Hancock-trokarhåndtag model 1701A1, i det følgende kaldet Hancock-trokarinstrumentet, for at skabe en
ensartet cirkulær ventrikelåbning og udtage myokardieproppen (Figur 2a, 2b og 2c). Der skal udvises
forsigtighed for at undgå at beskadige det interventrikulære septum, chordae tendineae eller det koronare
flow. Med conduit-forlængelsen afklemt distalt for klappen indføres konnektoren i venstre ventrikel og
sutureres (Figur 4). Den kardiopulmonale bypass kan ophøre på dette tidspunkt efter operatørens skøn.
Efter afskæring af den distale ende af konnektor-conduit m. klap-protesen til den korrekte længde
færdiggøres end-to-side aorta-anastomosen ved brug af en partiel okklusionsklemme (Figur 4). Der skal
udvises forsigtighed ved tilpasning af conduit m. klap for at fjerne overskydende længde, som kan
resultere i slitage på grund af friktion mod thoraxvæggen.
Aorta-anastomosen kan placeres i niveau med sjette og syvende interkostale arterier (Figur 5). Det
inferiore pulmonale ligament deles for at tillade eksponering af den thorakale aorta descendens.
Der udføres - med en karklemme, der delvist okkluderer aorta - en længdegående incision med en
højrevinklet saks. Den distale ende af conduit m. klap anastomoseres med en kontinuerlig polyestersutur.
(Figur 5). Der udtømmes luft fra venstre ventrikel og conduit m. klap med en 20-gauge (Ga) nål, og
aortaklemmen kan så fjernes.
9.3 Tilbehør
Hancock-trokarinstrumentet, som består af Hancock-trokarkniv model 1701A og Hancock-trokarhåndtag
model 1701A1, er fremstillet med henblik på at lette apikal ventrikulotomi. Anvend kun Hancocktrokarinstrumentet til at skabe en ren, ensartet åbning i venstre ventrikulære apex og til at minimere
muligheden for beskadigelse af chordae tendineae. Hancock-trokarinstrumentet kan leveres som et
genanvendeligt håndtagssæt, der bruger cylinderformede engangsknive af rustfrit stål og tilsvarende
spidser i str. 12, 14, 16, 18, 20, 22 og 26 mm, som svarer til konnektorernes udvendige diameter (OD,
Outer Diameter). Vælg den størrelse kniv og spids, som svarer til den venstre ventrikel-konnektor, der skal
anvendes. Kontrollér Hancock-trokarinstrumentet inden brug for at bekræfte korrekt samling, og at alle
komponenter er fæstnet sikkert. Knivsblade må ikke bruges flere gange.
Monteringsvejledning
Hancock-trokarinstrumentet består af spidsen (a), stangen (b), kniven (c), knivholderen (d), håndtaget (e)
og endehætten (f) (Figur 6a til 6e).
1. Fastgør endehætten på håndtaget ved at dreje endehætten højre om (med uret) (Figur 6a).
2. Fastgør kniven til holderen ved at dreje kniven højre om (med uret).
Forsigtig: Undgå at holde på kniven i nærheden af æggen (Figur 6b).
3. Skub knivholderen på håndtagets skaft, indtil den sidder helt fast inde i håndtaget (Figur 6c).
Brugsanvisning Dansk 67
Page 70

4. Fastgør spidsen af håndtagets gevindskaft ved at dreje spidsen højre om (med uret), indtil den sidder
fast (Figur 6d).
5. Den fuldførte montering af Hancock-trokarinstrumentet (Figur 6e).
Se brugsanvisningen til Hancock-trokarinstrumentet for yderligere oplysninger om anvendelse og
sterilisering.
Advarsel: Der må ikke anvendes andre trokarer eller kirurgiske instrumenter. Brug af andre instrumenter
vil muligvis ikke skabe en venstresidig ventrikulær åbning, der svarer til størrelsen og geometrien på
Hancock apikale venstre ventrikel-konnektor. Brug af disse kan resultere i alvorlig blødning omkring
syringen.
9.4 Sterilisering
Hancock apikale venstre ventrikel-konnektor leveres STERIL (damp) og må ikke resteriliseres.
Konnektorer, der er blevet beskadiget eller kontamineret pga. patientkontakt, må ikke anvendes.
10 POSTOPERATIVE INFORMATIONER
Denne enhed indeholder ingen metaller og udgør derfor ikke nogen umiddelbar risiko i MR-miljøer.
11 PATIENTOPLYSNINGER
Bemærk: Registrering af patienter er ikke påkrævet i lande, hvor lovgivningen om databeskyttelse ikke
tillader, at der indhentes oplysninger om patienter, herunder også lande i EU.
Der medleveres en patientregistreringsblanket i hver pakke. Udfyld alle de påkrævede oplysninger efter
implanteringen. Serienummeret kan findes på emballagen og på identifikationsmærket, der er fastgjort til
den indvendige holder. Send den originale blanket til den Medtronic-adresse, der er angivet på blanketten,
og giv det midlertidige identifikationskort til patienten, før patienten udskrives.
Patienten vil få udleveret et identifikationskort for implanteret udstyr. Kortet indeholder navn og
telefonnummer på patientens læge samt andre oplysninger, som sundhedspersonalet kan have brug for i
en nødsituation.
68 Dansk Brugsanvisning
Page 71

12 ANSVARSFRASKRIVELSE
FØLGENDE ANSVARSFRASKRIVELSE GÆLDER FOR KUNDER UDEN FOR USA:
ANSVARSFRASKRIVELSE
SELVOM HANCOCK APIKALE VENSTRE VENTRIKEL-KONNEKTOR (MODEL 174A), I DET
FØLGENDE KALDET "PRODUKTET", ER OMHYGGELIGT DESIGNET, FREMSTILLET OG
AFPRØVET FØR SALG, KAN DER AF MANGE GRUNDE VÆRE EN RISIKO FOR, AT PRODUKTET
IKKE FUNGERER TILFREDSSTILLENDE EFTER HENSIGTEN. ADVARSLERNE, SOM FREMGÅR AF
PRODUKTETS MÆRKATER, GIVER MERE DETALJEREDE OPLYSNINGER OG BETRAGTES SOM
EN INTEGRERET DEL AF DENNE ANSVARSFRASKRIVELSE. MEDTRONIC FRASIGER SIG
DERFOR ALLE GARANTIER, UDTRYKKELIGE SÅVEL SOM STILTIENDE, MED HENSYN TIL
PRODUKTET. MEDTRONIC KAN IKKE HOLDES ANSVARLIG FOR TILFÆLDIGE SKADER ELLER
FØLGESKADER SOM FØLGE AF BRUG AF PRODUKTET ELLER DETS DEFEKT ELLER
FEJLFUNKTION, UANSET OM KRAVET BASERES PÅ GARANTI, KONTRAKT, ERSTATNING UDEN
FOR KONTRAKT, ELLER ANDET.
Ovennævnte undtagelser og begrænsninger har ikke til hensigt at være, og må ikke fortolkes som
værende, i modstrid med ufravigelige bestemmelser i gældende lovgivning. Hvis nogen del af eller vilkår
i denne ANSVARSFRASKRIVELSE af en kompetent ret anses for ulovlig, uden retskraft eller i konflikt
med den relevante lovgivning, berøres den resterende del af denne ANSVARSFRASKRIVELSE ikke, og
alle rettigheder og forpligtelser skal tolkes og håndhæves, som om denne ANSVARSFRASKRIVELSE
ikke indeholdt det pågældende afsnit eller vilkår, der anses for ugyldigt.
Brugsanvisning Dansk 69
Page 72

Page 73

1 DESCRIÇÃO DO DISPOSITIVO
O conector apical ventricular esquerdo Hancock, modelo 174A é composto por uma estrutura flexível em
polipropileno, concebida de acordo com os mesmos princípios que levaram ao desenvolvimento do stent
para as biopróteses de válvulas cardíacas aórticas e auriculoventriculares Hancock, preparadas pelo
“Stabilized Glutaraldehyde Process” (SGP). A superfície de contacto com o sangue do conector
é revestida com um tecido de poliéster de baixa porosidade, que se estende para lá do stent de
sustentação para anastomose a um conduto valvulado Hancock, fabricado no mesmo material.
Um anel de sutura compatível permite suturar o conector ao ápex do ventrículo esquerdo. É fornecido um
anel de sutura adicional para controlar a profundidade de penetração do conector no ventrículo esquerdo.
O conector apical ventricular esquerdo Hancock está disponível nos tamanhos e dimensões indicados
na Tabela 1.
Tab ela 1. Tamanhos e dimensões disponíveis
F
D
C
A
B
E
G
CONECTOR CURVO, MODELO 174A
(mm)
TAMANHO A B C D E F
12 12 17 26 21 3 26 90
14 14 19 28 21 4 24 90
16 16 21 30 21 4 26 90
18 18 23 33 25 4 33 90
20 20 25 37 25 4 37 90
22 22 27 41 25 4 41 90
26 26 32 43 25 4 41 90
Instruções de utilização Português 71
G
(mínimo)
Page 74

2 INDICAÇÕES
O conector apical ventricular esquerdo Hancock, utilizado em conjunto com o conduto valvulado (de baixa
porosidade) Hancock, modelo 105, proporciona um método alternativo para o alívio da hipertensão
ventricular esquerda em doentes com obstrução grave do tracto de saída do ventrículo esquerdo, devido
a hipoplasia da raiz da aorta, hipoplasia do anel aórtico ou problemas resultantes de substituição da
válvula aórtica, que não pode ser aliviada através de técnicas convencionais.
3 CONTRA-INDICAÇÕES
O conector apical ventricular esquerdo Hancock está contra-indicado para doentes com alguma das
seguintes patologias:
■
aneurisma do ventrículo esquerdo
■
trombose
■
refluxo grave da válvula aórtica
4 AVISOS
Este dispositivo foi concebido apenas para utilização num único doente. Não reutilize, reprocesse nem
reesterilize este produto. Estes processos poderão comprometer a integridade estrutural do dispositivo e/ou
originar um risco de contaminação do dispositivo, o que poderia causar lesões, doença ou mesmo a morte
do doente.
Não use o conector se:
■
tiver caído, estiver danificado ou tiver sido alvo de manuseamento inadequado;
■
a data “Não utilizar depois de” tiver expirado.
Embora tenham sido seleccionados materiais validados clinicamente para a reconstrução arterial para
serem utilizados com o conector apical ventricular esquerdo Hancock, continua a existir um risco potencial
de perda sanguínea intersticial, em especial nos doentes com hemodiluição ou deficiências dos factores
de coagulação.
FORAM RELATADAS GRAVES COMPLICAÇÕES HEMORRÁGICAS EM DOENTES DESTE GÉNERO
E PARA OS QUAIS O CONECTOR E/OU O CONDUTO VALVULADO NÃO FORAM PRÉ-COAGULADOS.
ESTE PERIGO POTENCIAL PODE SER MINIMIZADO PRÉ-COAGULANDO O CONECTOR E O CONDUTO
VALVU LADO.
Durante a clampagem do conduto valvulado, não clampe o conduto a menos de 8 cm do anel metálico.
Seleccione a lâmina e ponta de trocarte Hancock adequadas para efectuar a ventriculostomia apical
esquerda. Por exemplo, utilize uma lâmina e ponta de trocarte Hancock de 14 mm para a inserção de um
conector apical ventricular esquerdo Hancock de 14 mm.
Examine o trocarte antes de o utilizar para verificar a correcta montagem e a ligação segura de todos os
componentes.
5 PRECAUÇÕES
Recomenda-se que todos os doentes submetidos a este procedimento façam uma ecocardiografia nos
períodos pré- e intra-operatórios.
Atenção: não utilizar se se verificar insuficiência coronária grave, doença oclusiva sintomática ou grave
da carótida ou doenças aneurismáticas da aorta torácica.
6 POSSÍVEIS EFEITOS ADVERSOS
Foram relatados casos de tromboembolia, embora raros. A possibilidade de ocorrência desta
complicação deve ser ponderada ao seleccionar o procedimento cirúrgico ideal para cada doente.
A HEMORRAGIA EM REDOR DA ANASTOMOSE DO CONECTOR AO ÁPEX PODE SER MINIMIZADA
ATRAVÉS DE UMA TÉCNICA CIRÚRGICA APROPRIADA E DA PRÉ-COAGULAÇÃO DO CONECTOR
E DO CONDUTO VALVULADO.
Pode ocorrer redução significativa na circulação coronária e vascular cerebral quando se verifica
a presença de doenças intrínsecas nestes sistemas.
7 INFORMAÇÕES DE ACONSELHAMENTO AO DOENTE
Poderá ser necessário medicar os doentes por um período de tempo indefinido com terapêutica
anticoagulante e/ou antiplaquetária, com base na sua situação individual.
8 APRESENTAÇÃO
8.1 Embalagem
O conector apical ventricular esquerdo Hancock está disponível nos seguintes tamanhos: 12, 14, 16, 18,
20, 22 e 26 mm. A embalagem contém um único conector apical ventricular esquerdo Hancock embalado
em bolsas de transferência assépticas duplas e esterilizadas. O sistema de embalagem foi concebido
para facilitar o posicionamento do dispositivo no campo estéril. O conector encontra-se esterilizado se as
bolsas não estiverem danificadas nem tiverem sido abertas. As superfícies externas da bolsa externa
NÃO estão ESTERILIZADAS e não devem ser colocadas no campo estéril.
72 Português Instruções de utilização
Page 75

8.2 Armazenamento
Armazene o produto na sua embalagem original, incluindo a caixa de cartão externa, num local limpo,
fresco e seco para proteger o produto e minimizar a possibilidade de contaminação. A esterilidade e não
pirogenicidade do conduto estão validadas e não serão afectadas até à a data “Não utilizar depois de”
indicada na caixa de cartão, desde que as bolsas não tenham sido abertas nem se encontrem danificadas.
Deve manter-se um controlo adequado do inventário de forma a que os conectores com prazos de validade
mais curtos sejam implantados preferencialmente e se possa evitar a expiração do prazo de validade.
9 INSTRUÇÕES DE UTILIZAÇÃO
9.1 Preparação
Devido à complexidade e variação dos procedimentos cirúrgicos para bypass ápico-aórtico, a escolha
da abordagem cirúrgica e das técnicas de sutura é deixada ao critério de cada cirurgião. As seguintes
são técnicas comunicadas à Medtronic por cirurgiões especializados em implantes e podem ser
utilizadas para facilitar a implantação.
A inserção do conector apical ventricular esquerdo é frequentemente efectuada sob bypass cardiopulmonar.
A anastomose à aorta torácica descendente é frequentemente efectuada através de uma incisão de
toracotomia lateral esquerda no quinto espaço intercostal.
Não existem calibradores disponíveis para o conector. A determinação do tamanho é definida pela
capacidade da cavidade torácica do doente em vez de o ser por padrões tradicionais. O conector de
maior tamanho que caiba na cavidade torácica e mesmo assim permita o fecho da incisão sem causar
pressão excessiva no dispositivo é o que deve ser utilizado.
A anastomose do conector e do conduto valvulado poderá ser efectuada antes do bypass cardiopulmonar.
Recomenda-se vivamente que a pré-coagulação do conector e do conduto valvulado seja efectuada antes
destas anastomoses de modo a evitar a perda de sangue. Uma alternativa é efectuar a anastomose do
conduto valvulado à aorta e a anastomose do conector ao ápex do ventrículo separadamente e só depois
fazer a anastomose entre os dois condutos.
9.2 Implante do dispositivo
Com o pericárdio dividido, o ápex do ventrículo fica elevado. É efectuada uma sutura em bolsa de tabaco
no ápex. São passadas suturas interrompidas simples de poliéster através do miocárdio em pontos
equidistantes em redor do local da ventriculostomia, definido pela sutura em bolsa de tabaco e pelo anel
de sutura do conector. É efectuada uma pequena incisão no ápex e é removido um pedaço de tecido
miocárdico (Figuras 1 e 3). Utilize uma lâmina e ponta de trocarte Hancock, modelo 1701A com o manípulo
de trocarte Hancock, modelo 1701A1, doravante referidos como o conjunto de trocarte Hancock, para criar
uma abertura ventricular circular e uniforme e para a remoção do pedaço de tecido miocárdico (Figuras 2a,
2b e 2c). Deverá proceder-se com cuidado para não danificar o septo interventricular, as cordas tendinosas
ou o fluxo coronário. Com a extensão do conduto pinçada distalmente na válvula, o conector é inserido no
ventrículo esquerdo e suturado no devido lugar (Figura 4). O bypass cardiopulmonar poderá ser interrompido
neste momento, ao critério do cirurgião.
Após aparar a extremidade distal da prótese conector-conduto valvulado para ficar com o tamanho correcto,
a anastomose aórtica término-lateral é efectuada usando uma pinça de oclusão parcial (Figura 4). Deverá
proceder-se com cuidado ao aparar o conduto valvulado para retirar o comprimento em excesso pois este
pode causar desgaste do tecido devido a fricção com a parede torácica.
A anastomose aórtica poderá ficar localizada ao nível da sexta e sétima artérias intercostais (Figura 5).
O ligamento pulmonar inferior é dividido para permitir a exposição da aorta torácica descendente.
Com uma pinça vascular a ocluir parcialmente a aorta, é efectuada uma incisão longitudinal com uma
tesoura de ângulo recto. A extremidade distal do conduto valvulado é anastomosada com fios de sutura
de poliéster contínua (Figura 5). O ar é retirado do ventrículo esquerdo e do conduto valvulado com uma
agulha de calibre 20 e a pinça aórtica é então removida.
9.3 Acessórios
O conjunto de trocarte Hancock, constituído pela lâmina de trocarte Hancock, modelo 1701A e pelo manípulo
de trocarte Hancock, modelo 1701A1, foi concebido para facilitar a ventriculostomia apical. Para criar uma
abertura perfeita e uniforme no ápex no ventrículo esquerdo e para minimizar a possibilidade de lesionar as
cordas tendinosas utilize exclusivamente o conjunto de trocarte Hancock. O conjunto de trocarte Hancock
está disponível sob a forma de um conjunto de manípulo reutilizável que emprega lâminas cilíndricas de aço
inoxidável descartáveis e pontas correspondentes nos tamanhos de 12, 14, 16, 18, 20, 22 e 26 mm, que
correspondem ao diâmetro externo (DE) dos conectores. Seleccione o tamanho de lâmina e de ponta que
corresponde ao conector do ventrículo esquerdo que vai ser utilizado. Examine o conjunto de trocarte
Hancock antes de o utilizar para verificar a correcta montagem e a ligação segura de todos os componentes.
Não reutilize a lâmina de corte.
Instruções de utilização Português 73
Page 76

Instruções de montagem
O conjunto de trocarte Hancock é constituído pela ponta (a), haste (b), lâmina (c), suporte da lâmina (d),
manípulo (e) e tampa da extremidade (f) (Figuras 6a a 6e).
1. Prenda a tampa da extremidade ao manípulo, rodando-a para a direita (Figura 6a).
2. Prenda a lâmina ao suporte, rodando-a para a direita.
Atenção: não segure a lâmina pela extremidade de corte (Figura 6b).
3. Faça deslizar o suporte da lâmina pelo eixo do manípulo até que o suporte da lâmina fique
completamente inserido dentro do manípulo (Figura 6c).
4. Prenda a ponta ao eixo roscado do manípulo, rodando a ponta para a direita, até ficar apertada
(Figura 6d).
5. O conjunto de trocarte Hancock completo (Figura 6e).
Consulte as instruções de utilização do trocarte Hancock para obter informações pormenorizadas sobre
a utilização e esterilização.
Aviso: não utilize outros trocartes ou ferramentas cirúrgicas. A utilização de outras ferramentas poderá
não criar uma abertura no ventrículo esquerdo que corresponda ao tamanho e à geometria do conector
apical ventricular esquerdo Hancock. A sua utilização pode causar uma hemorragia grave em redor do
anel de sutura.
9.4 Esterilização
O conector apical ventricular esquerdo Hancock é fornecido ESTERILIZADO (por vapor) e não deve ser
reesterilizado. Os conectores que tenham sido danificados ou contaminados por contacto com o doente
não devem ser utilizados.
10 INFORMAÇÕES PÓS-OPERATÓRIAS
Este dispositivo não contém metais, logo não representa qualquer perigo em todos os ambientes de RM.
11 INFORMAÇÕES DO DOENTE
Nota: o registo do doente não se aplica nos países onde o fornecimento de dados sobre o doente
contrarie a legislação relativa à privacidade do doente, inclusive em países da UE.
Cada embalagem do dispositivo inclui um formulário de registo do doente. Após o implante, forneça todas
as informações que lhe são pedidas nesse formulário. O número de série encontra-se na embalagem
e na etiqueta de identificação presa ao retentor. Devolva o formulário original para o endereço da Medtronic
indicado no formulário e forneça o cartão de identificação temporário ao doente antes de lhe dar alta.
É fornecido ao doente um cartão de identificação do dispositivo implantado. O cartão contém o nome
e o número de telefone do médico do doente, bem como informações de que o pessoal médico venha
a necessitar em caso de emergência.
74 Português Instruções de utilização
Page 77

12 RENÚNCIA DE GARANTIA
A SEGUINTE RENÚNCIA DE GARANTIA APLICA-SE A CLIENTES FORA DOS EUA:
RENÚNCIA DE GARANTIA
EMBORA O CONECTOR APICAL VENTRICULAR ESQUERDO HANCOCK (MODELO 174A),
A PARTIR DAQUI REFERIDO COMO “PRODUTO”, TENHA SIDO CUIDADOSAMENTE DESENHADO,
FABRICADO E TESTADO ANTES DA COMERCIALIZAÇÃO, O PRODUTO PODE NÃO DESEMPENHAR
SATISFATORIAMENTE A SUA FUNÇÃO DEVIDO A UMA VARIEDADE DE MOTIVOS. OS AVISOS
CONTIDOS NAS ETIQUETAS DOS PRODUTOS FORNECEM INFORMAÇÕES MAIS DETALHADAS
E SÃO CONSIDERADOS COMO PARTE INTEGRANTE DESTA RENÚNCIA. POR CONSEGUINTE,
A MEDTRONIC RENUNCIA A TODAS AS GARANTIAS, EXPRESSAS OU IMPLÍCITAS, RELATIVAS AO
PRODUTO. A MEDTRONIC NÃO SERÁ RESPONSÁVEL POR QUAISQUER DANOS ACIDENTAIS OU
CONSEQUENCIAIS CAUSADOS POR QUALQUER UTILIZAÇÃO, DEFEITO OU FALHA DO PRODUTO,
QUER A QUEIXA SE BASEIE NA GARANTIA, CONTRATO, DANO OU OUTROS.
As exclusões e limitações acima definidas não se destinam a infringir estipulações obrigatórias da lei
aplicável e não devem ser interpretadas como tal. Se alguma parte ou termo desta RENÚNCIA DE
GARANTIA for considerado ilegal, não executável ou em conflito com a lei aplicável por parte de um
tribunal da jurisdição competente, a validade das partes restantes da RENÚNCIA DE GARANTIA não
deverá ser afectada e todos os direitos e obrigações devem ser interpretados e executados como se esta
RENÚNCIA DE GARANTIA não contivesse a parte ou termo particular considerado inválido.
Instruções de utilização Português 75
Page 78

Page 79

Figure 1. Use the Hancock Trocar Assembly to create a uniform ventricular opening and to
remove the resulting circular tissue plug. / Figure 1. Pratiquer une ouverture uniforme sur
le ventricule à l'aide du jeu de trocart Hancock et retirer le bouchon circulaire de tissu
obtenu. / Abbildung 1. Verwenden Sie das Hancock Trokarset, um eine gleichmäßige
Öffnung in den Ventrikel einzubringen und den dadurch entstehenden zylindrischen Pfropf zu
entfernen. / Figura 1. Utilice el conjunto de trocar Hancock para crear una abertura uniforme
en el ventrículo y extraer el tapón circular de tejido resultante. / Afbeelding 1. Gebruik de
Hancock-trocart voor het creëren van een gelijkmatige opening in het ventrikel en het
verwijderen van de resulterende ronde weefselkern. / Figura 1. Utilizzare l'unità trocar
Hancock per creare un'apertura ventricolare uniforme e per asportare il tappo circolare di
tessuto da essa risultante. / Figur 1. Bruk Hancock-trokarsettet til å lage en enhetlig
ventrikulær åpning og til å fjerne den runde vevspluggen som dannes. / Kuva 1. Käytä
Hancock-troakaarikokoonpanoa tasaisen kammioaukon luomiseen ja syntyneen
ympyränmallisen kudostulpan poistamiseen. / Figur 1. Använd Hancock
troakaranordningen för att skapa en uniform kammaröppning och för att ta bort den cirkulära
vävnadsproppen. / Εικόνα 1. Χρησιμοποιήστε τη διάταξη τροκάρ Hancock για να
δημιουργήσετε ένα ομοιόμορφο άνοιγμα στην κοιλία και να αφαιρέσετε το προκύπτον
κυκλικό βύσμα ιστού./ Figur 1. Brug Hancock-trokarinstrumentet til at skabe en ensartet
ventrikulær åbning og fjerne den resulterende runde prop af væv. / Figura 1. Utilize
o conjunto de trocarte Hancock para criar uma abertura ventricular uniforme e para retirar
o pedaço circular de tecido resultante.
77
Page 80

Figure 2a. Gentle pressure and rotation of the trocar tip assists passage through the
incision. During this maneuver, the trocar blade should be in the closed position. /
Figure 2a. Une pression et une rotation modérées de l'extrémité du trocart facilitent le
passage dans l'incision. Pendant cette opération, la lame du trocart doit être en position
fermée. / Abbildung 2a. Die Trokarspitze wird durch Drehen bei leichtem Druck durch den
Einschnitt geführt. Während dieses Vorgangs sollte sich die Trokarklinge in der
geschlossenen Position befinden. / Figura 2a. Una presión suave y la rotación de la punta
del trocar facilitan el paso a través de la incisión. Durante esta maniobra, la cuchilla del
trocar debe estar en la posición cerrada. / Afbeelding 2a. Oefen enige druk uit op de
trocarttip en draai de tip een beetje om hem via de incisie in te brengen. Hierbij moet het
trocartmes in de gesloten positie staan. / Figura 2a. Per facilitare il passaggio del trocar
attraverso l'incisione, esercitare una lieve pressione e rotazione sulla punta del trocar.
Durante questa operazione, mantenere la lama del trocar in posizione chiusa. /
Figur 2a. Legg forsiktig press på trokartuppen og drei på den for at den lettere skal føres
gjennom incisjonen. Trokarbladet skal være i lukket posisjon når du gjør dette. /
Kuva 2a. Troakaarin kärjen painaminen ja kiertäminen varovasti auttaa kulkua insision läpi.
Tämän toimenpiteen aikana troakaarin terän pitäisi olla suljetussa asennossa. /
Figur 2a. Försiktigt tryck och rotering av troakarspetsen underlättar passagen genom
snittet. Vid denna manöver ska troakarbladet vara i stängt läge. / Εικόνα 2a. Η ήπια πίεση
και περιστροφή του άκρου του τροκάρ διευκολύνει τη διέλευση μέσω της τομής. Κατά τη
διάρκεια αυτού του χειρισμού η λεπίδα του τροκάρ θα πρέπει να είναι κλειστή./
Figur 2a. Forsigtigt tryk på og drejning af trokarspidsen letter passage gennem incisionen.
Trokarkniven skal under denne manøvre være lukket. /
Figura 2a. Uma pressão suave
e a rotação da ponta do trocarte ajudam a passar através da incisão. Durante esta
manobra, a lâmina do trocarte deve estar na posição fechada.
78
Page 81

Figure 2b. Retract the trocar blade after the tip has penetrated the incision. After the blade
has been retracted, ensure that the tip is firmly seated against the inner ventricular wall. /
Figure 2b. Rétracter la lame du trocart lorsque l'extrémité est dans la cavité. Une fois la
lame rétractée, vérifier que l'extrémité est fermement appuyée contre la paroi interne du
ventricule. / Abbildung 2b. Ziehen Sie die Trokarklinge zurück, nachdem die Spitze den
Einschnitt durchstochen hat. Stellen Sie sicher, dass die Spitze nach dem Zurückziehen der
Klinge fest an der inneren Ventrikelwand anliegt. / Figura 2b. Haga retroceder la cuchilla
del trocar una vez que la punta haya penetrado la incisión. Una vez retraída la cuchilla,
asegúrese de que la punta está firmemente asentada contra la pared interna del
ventrículo. / Afbeelding 2b. Trek het trocartmes terug nadat de tip in de incisie is
doorgedrongen. Controleer na het terugtrekken van het mes of de tip stevig tegen de
binnenste ventrikelwand zit. / Figura 2b. Ritirare la lama del trocar dopo che la punta è
penetrata nell'incisione. Una volta ritirata la lama, verificare che la punta sia saldamente
posizionata a contatto con la parete ventricolare interna. / Figur 2b. Trekk trokarbladet
tilbake etter at tuppen er satt inn gjennom incisjonen. Etter at bladet er trukket tilbake, må du
sikre at tuppen er plassert godt inntil den indre ventrikkelveggen. / Kuva 2b. Vedä troakaarin
terä taakse, kun kärki on työntynyt insisioon. Kun terä on vedetty taakse, varmista, että kärki
on tukevasti kammion sisäseinämää vasten. / Figur 2b. Dra tillbaka troakarbladet efter att
spetsen har trängt igenom snittet. Se till att spetsen sitter fast ordentligt mot den inre
kammarväggen efter att bladet har dragits tillbaka. / Εικόνα 2b. Αποσύρετε τη λεπίδα του
τροκάρ αφού το άκρο διεισδύσει στην τομή. Μετά την απόσυρση της λεπίδας, βεβαιωθείτε
ότι το άκρο έχει επικαθίσει σταθερά έναντι του εσωτερικού κοιλιακού τοιχώματος./
Figur 2b. Træk trokarkniven tilbage, når spidsen har penetreret incisionen. Når knivsbladet
er trukket tilbage, skal det sikres, at spidsen er fast placeret mod den indre ventrikulære
væg. / Figura 2b. Retraia a lâmina do trocarte após a ponta ter penetrado na incisão. Após
a retracção da lâmina, certifique-se de que a ponta está firmemente assente contra
a parede ventricular interna.
79
Page 82

Figure 2c. Perform the ventriculotomy by gently advancing the blade with continuous
rotation. The handle should remain stationary with the tip against the inner ventricular
wall when advancing the blade. / Figure 2c. Effectuer la ventriculotomie en faisant avancer
doucement la lame avec une rotation continue. La poignée doit rester fixe, extrémité contre
la paroi interne du ventricule, pendant que la lame avance. / Abbildung 2c. Führen Sie die
Ventriculotomie durch, indem Sie die Klinge bei ständigem Drehen vorsichtig vorwärts
schieben. Der Griff sollte dabei unbeweglich bleiben, wobei die Spitze an der inneren
Ventrikelwand anliegt. / Figura 2c. Realice la ventriculotomía haciendo avanzar
suavemente la cuchilla con una rotación continua. El mango debe mantenerse fijo con la
punta asentada contra la pared interna del ventrículo al hacer avanzar la cuchilla. /
Afbeelding 2c. Voer de ventriculotomie uit door het mes voorzichtig en voortdurend
draaiend op te voeren. De handgreep moet op de plaats worden gehouden met de tip tegen
de binnenste ventrikelwand terwijl het mes wordt opgevoerd. / Figura 2c. Eseguire la
ventricolotomia facendo avanzare delicatamente la lama con un movimento rotatorio
continuo. Durante l'avanzamento della lama, l'impugnatura deve rimanere ferma e la punta
deve rimanere a contatto della parete ventricolare interna. / Figur 2c. Utfør ventrikulotomi
ved å føre bladet forsiktig frem med en kontinuerlig, dreiende bevegelse. Håndtaket skal
være i samme posisjon med tuppen mot den indre ventrikkelveggen når bladet føres frem. /
Kuva 2c. Suorita ventrikulotomia työntämällä terää varovasti ja kiertämällä sitä
keskeytyksettä. Kahvan pitäisi pysyä paikallaan niin, että kärki on kammion sisäseinämää
vasten, kun terää työnnetään eteenpäin. / Figur 2c. Utför ventrikulotomi genom att försiktigt
föra fram bladet med kontinuerlig rotering. Handtaget ska förbli stationärt med spetsen mot
den inre kammarväggen när bladet förs fram. / Εικόνα 2c. Πραγματοποιήστε την κοιλιοτομή
προωθώντας μαλακά τη λεπίδα με συνεχή περιστροφή. Κατά την προώθηση της λεπίδας,
η λαβή πρέπει να παραμένει σταθερή με το άκρο έναντι του εσωτερικού κοιλιακού
τοιχώματος./ Figur 2c. Udfør ventrikulotomi ved forsigtigt at fremføre knivsbladet under
kontinuerlig drejning. Håndtaget skal holdes stationært med spidsen op mod den indvendige
ventrikel- væg under fremføring af kniven. / Figura 2c. Efectue a ventriculostomia fazendo
a lâmina avançar suavemente com rotação contínua. O manípulo deve permanecer imóvel
com a ponta contra a parede ventricular interna enquanto faz avançar a lâmina.
80
Page 83

AA
PA
LA
LV
DA
Figure 3. After placement of the sutures through the sewing ring and removal of the
myocardial tissue plug, the connector is inserted into position. Note the conduit extension is
clamped distal to the valve. In patients without significant left ventricular hypertrophy,
projection of the connector into the ventricle may be reduced by use of the additional sewing
ring supplied with each connector. / Figure 3. Une fois les sutures pratiquées sur l'anneau
de suture et le bouchon de tissu myocardique retiré, insérer l'embout. Noter que l'extension
du conduit est clampée en distal de la valve. Chez les patients sans hypertrophie importante
du ventricule gauche, la projection de l'embout dans le ventricule peut être réduite par
l'utilisation du deuxième anneau de suture fourni avec chaque embout. /
Abbildung 3. Nachdem die Nähte durch den Nahtring gesetzt und der myocardiale
Gewebspfropf entfernt wurde, wird der Konnektor eingesetzt. Beachten Sie, dass die
Condiutverlängerung distal an die Klappe geklemmt wird. Bei Patienten ohne signifikante
linksventrikuläre Hypertrophie kann das Hervorstehen des Konnektors innerhalb des
Ventrikels durch Einsatz des mit dem Konnektor gelieferten zusätzlichen Nahtrings
verringert werden. / Figura 3. Una vez colocadas las suturas a través del anillo de sutura y
retirado el tapón de tejido miocárdico, se introduce el conector en su posición. Compruebe
que la extensión del conducto está clampada en posición distal a la válvula. En los
pacientes que no presentan una hipertrofia marcada del ventrículo izquierdo puede
conseguirse que el conector sobresalga menos dentro del ventrículo utilizando el anillo de
sutura adicional que se suministra con cada conector. / Afbeelding 3. Na het aanbrengen
van de hechtingen met behulp van de naairing en het verwijderen van de myocardiale
weefselkern, wordt de connector ingebracht. De conduitverlenging wordt distaal van de klep
afgeklemd. Bij patiënten zonder aanzienlijke hypertrofie in het linkerventrikel kan de
projectie van de connector in het ventrikel worden gereduceerd door het gebruik van de
extra naairing die bij elke connector wordt meegeleverd. / Figura 3. Dopo il posizionamento
delle suture attraverso l'anello di sutura e l'asportazione del tappo di tessuto miocardico, il
connettore viene inserito in sede. L'estensione del condotto viene clampata in posizione
distale rispetto alla valvola. Nei pazienti senza ipertrofia significativa del ventricolo sinistro,
la sporgenza del connettore nel ventricolo può essere ridotta utilizzando l'anello di sutura
aggiuntivo fornito con ogni connettore. / Figur 3. Sett koblingen på plass etter at du har
plassert suturene gjennom sy-ringen og fjernet myokardvevspluggen. Pass på at
avløpsforlengelsen er klemt av distalt for klaffen. Hos pasienter uten signifikant hypertrofi i
venstre ventrikkel kan du begrense hvor langt koblingen føres inn i ventrikkelen, ved å bruke
den ekstra sy-ringen som følger med hver kobling. / Kuva 3. Kun olet vienyt ompeleet
ompelurenkaan läpi ja poistanut sydänlihaksen kudostulpan, liitin on paikoillaan. Huomaa,
että putken jatko-osa on suljettu venttiilin distaalipuolella. Potilailla, joilla ei ole merkittävää
vasemman kammion liikakasvua, liittimen siirtymistä kammioon voidaan vähentää
käyttämällä kunkin liittimen mukana toimitettavaa lisäompelurengasta. / Figur 3. Efter
placering av suturerna genom suturringen och borttagande av myokardivävnadsproppen
sätts konnektorn på plats. Observera att conduitförlängningen är stängd med klämma distalt
om klaffen. Hos patienter utan signifikant vänster kammarhypertrofi kan projektionen av
konnektorn in i kammaren minskas genom användning av en extra suturring som levereras
med varje konnektor. /
81
Page 84

Εικόνα 3. Μετά την τοποθέτηση των ραμμάτων μέσω του δακτύλιου συρραφής και την
αφαίρεση του βύσματος μυοκαρδιακού ιστού, ο σύνδεσμος εισέρχεται στη θέση του.
Σημειώστε ότι η προέκταση του μοσχεύματος είναι περισφιγμένη περιφερικά της βαλβίδας.
Σε ασθενείς χωρίς σοβαρή υπερτροφία της αριστερής κοιλίας, η προέκταση του συνδέσμου
στην κοιλία μπορεί να ελαττωθεί
από τη χρήση του πρόσθετου δακτύλιου συρραφής που
παρέχεται με κάθε σύνδεσμο./ Figur 3. Når suturerne er anbragt gennem syringen, og
vævsproppen fra myokardiet er fjernet, anbringes konnektoren. Bemærk, at conduitforlængelsen er afklemt distalt for klappen. Hos patienter uden signifikant venstre
ventrikulær hypertrofi kan forskydning af konnektoren ind i ventriklen reduceres ved at bruge
den ekstra syring, der leveres sammen med hver konnektor. / Figura 3. Após a colocação
das suturas através do anel de sutura e da remoção do pedaço de tecido miocárdico,
o conector é inserido na devida posição. Tenha em atenção que a extensão do conduto
é pinçada distalmente à válvula. Em doentes sem hipertrofia ventricular esquerda
significativa, a projecção do conector para dentro do ventrículo poderá ser reduzida através
da utilizaão do anel de sutura adicional, fornecido com cada conector.
82
Page 85

AA
PA
LA
LV
DA
Figure 4. With a vascular clamp partially occluding the aorta, a longitudinal incision is made
with a right angle scissors. The distal end of the prosthesis is anastomosed with
polyester sutures. / Figure 4. Une pince vasculaire obturant partiellement l'aorte, pratiquer
une incision longitudinale avec des ciseaux à angle droit. L'extrémité distale de la prothèse
est anastomosée avec des sutures en polyester. / Abbildung 4. Während die Aorta mit
einer Gefäßklemme teilweise abgeklemmt ist, wird mit einer Winkelschere ein Längsschnitt
vorgenommen. Das distale Ende der Prothese wird mit Polyesterfaden anastomosiert. /
Figura 4. Con un clamp vascular ocluyendo parcialmente la aorta, se practica una incisión
longitudinal con unas tijeras de ángulo recto. Se anastomosa el extremo distal de la prótesis
con suturas de poliéster. / Afbeelding 4. Klem de aorta gedeeltelijk af met een vaatklem en
gebruik een schaar met rechte hoek voor het maken van een longitudinale incisie. Maak met
polyester hechtingen een anastomose aan het distale uiteinde van de prothese. /
Figura 4. Dopo il clampaggio parziale dell'aorta, viene eseguita un'incisione longitudinale
con delle forbici ad angolo retto. L'estremità distale della protesi viene anastomizzata
mediante suture in poliestere. / Figur 4. Bruk en karklemme til å delvis okkludere aorta, og
lag en langsgående incisjon med en høyrevinklet saks. Den distale proteseenden
anastomoseres med polyestersuturer. / Kuva 4. Kun verisuonipuristin tukkii aortan osittain,
tee pitkittäinen viilto saksilla, joissa on kulma oikealle. Proteesin distaalipää yhdistetään
polyesteriompeleilla. / Figur 4. Med en kärlklämma som delvis ockluderar aorta, görs ett
längsgående snitt med en högervinklad sax. Den distala änden av protesen är
anastomoserad med polyestersuturer. / Εικόνα 4. Με έναν αγγειακό σφιγκτήρα που
αποφράσσει μερικώς την αορτή πραγματοποιείται επιμήκης τομή με ένα ψαλίδι ορθής
γωνίας. Το άπω άκρο της πρόσθεσης αναστομώνεται με πολυεστερικά ράμματα./
Figur 4. Der udføres - med en karklemme, der delvist okkluderer aorta - en længdegående
incision med en højrevinklet saks. Protesens distale ende anastomoseres med
polyestersuturer. / Figura 4. Com uma pinça vascular a ocluir parcialmente a aorta,
é efectuada uma incisão longitudinal com uma tesoura de ângulo recto. A extremidade distal
da prótese é anastomosada com fios de sutura de poliéster.
83
Page 86

AA
PA
LA
DA
Figure 5. Hancock Apical Left Ventricle Connector with valved conduit in position. /
Figure 5. Embout apical pour ventricule gauche Hancock avec conduit valvé en place. /
Abbildung 5. Implantierter Hancock apikaler linksventrikulärer Konnektor mit
klappentragendem Conduit / Figura 5. Conector apical para el ventrículo izquierdo
Hancock con el conducto valvulado en posición. / Afbeelding 5. Geplaatste apicale
Hancock-connector voor het linkerventrikel met conduit met klep. / Figura 5. Connettore
apicale per ventricolo sinistro Hancock con il condotto valvolato in sede. / Figur 5. Ferdig
plassert Hancock apikal kobling for venstre ventrikkel med klaffavløp. / Kuva 5. Apikaalinen
vasemman kammion Hancock-liitin ja läpällinen putki paikallaan. / Figur 5. Hancock apikal
vänsterkammarkonnektor och conduit med klaff i position. / Εικόνα 5. Τοποθετημένος
διακορυφαίος σύνδεσμος αριστερής κοιλίας Hancock με βαλβιδοφόρο μόσχευμα./
Figur 5. Hancock apikale venstre ventrikel-konnektor med conduit m. klap placeret
korrekt. / Figura 5. Conector apical ventricular esquerdo Hancock com conduto valvulado
na posição devida.
84
Page 87

(f)
(e)
Figure 6a. / Figure 6a. / Abbildung 6a. / Figura 6a. / Afbeelding 6a. / Figura 6a. /
Figur 6a. / Kuva 6a. / Figur 6a. / Εικόνα 6a. / Figur 6a. / Figura 6a.
(c)
(d)
Figure 6b. / Figure 6b. / Abbildung 6b. / Figura 6b. / Afbeelding 6b. / Figura 6b. /
Figur 6b. / Kuva 6b. / Figur 6b. / Εικόνα 6b. / Figur 6b. / Figura 6b.
(e)
(d)
(c)
Figure 6c. / Figure 6c. / Abbildung 6c. / Figura 6c. / Afbeelding 6c. / Figura 6c. /
Figur 6c. / Kuva 6c. / Figur 6c. / Εικόνα 6c. / Figur 6c. / Figura 6c.
(a)
(b)
(e)
(d)
(c)
Figure 6d. / Figure 6d. / Abbildung 6d. / Figura 6d. / Afbeelding 6d. / Figura 6d. /
Figur 6d. / Kuva 6d. / Figur 6d. / Εικόνα 6d. / Figur 6d. / Figura 6d.
85
Page 88

(c)
(e)
(b)
(a)
(d)
(f)
Figure 6e. / Figure 6e. / Abbildung 6e. / Figura 6e. / Afbeelding 6e. / Figura 6e. /
Figur 6e. / Kuva 6e. / Figur 6e. / Εικόνα 6e. / Figur 6e. / Figura 6e.
86
Page 89

Page 90

Europe
Europe/Africa/Middle East Headquarters
Medtronic International Trading Sàrl
Route du Molliau 31
Case Postale 84
CH - 1131 Tolochenaz
Switzerland
Internet: www.medtronic.co.uk
Tel. 41-21-802-7000
Fax 41-21-802-7900
Authorized Representative in the
European Community
Medtronic B.V.
Earl Bakkenstraat 10
6422 PJ Heerlen
The Netherlands
Tel. 31-45-566-8000
Fax 31-45-566-8668
Asia-Pacific
Japan
Medtronic Japan
Comodio Shiodome 5F
2-14-1 Higashi-Shimbashi, Minato-ku
Tokyo 105-0021
Japan
Tel. 81-3-6430-2011
Fax 81-3-6430-7140
Australia
Medtronic Australasia Pty. Ltd.
Business Address:
97 Waterloo Road
North Ryde NSW 2113
Mailing Address:
PO Box 945
North Ryde NSW 1670
Tel. 61-2-9857-9000
Fax: 61-2-9878-5100
Asia
Medtronic International Ltd.
Suite 1602 16/F, Manulife Plaza
The Lee Gardens, 33 Hysan Avenue
Causeway Bay
Hong Kong
Tel. 852-2891-4068
Fax 852-2591-0313
Americas
Latin America
Medtronic Latin America
3750 NW 87th Avenue
Suite 700
Miami, FL 33178
USA
Tel. 1-305-500-9328
Fax 1-786-709-4244
Canada
Medtronic of Canada Ltd.
6733 Kitimat Road, Mississauga
Ontario L5N 1W3
Canada
Tel. 905-826-6020
Fax 905-826-6620
Toll-free in Canada:
1-800-268-5346
United States
Manufacturer:
Medtronic, Inc.
710 Medtronic Parkway
Minneapolis, MN 55432
USA
Internet: www.medtronic.com or
www.heartvalves.com
Tel. 1-763-526-7890
Fax 1-763-526-7888
Toll-free in the USA:
1-877-526-7890
(24-hour consultation service)
© 2000, 2009, 2010 Medtronic M939280A001 Rev. 1A
*M939281A001*
 Loading...
Loading...