

Embolx Sniper Quick Manual
Quick Guide
IMPORTANT! Always refer to the Sniper Balloon Occlusion Microcatheter Instructions For Use for detailed instructions.
Contents
0
0
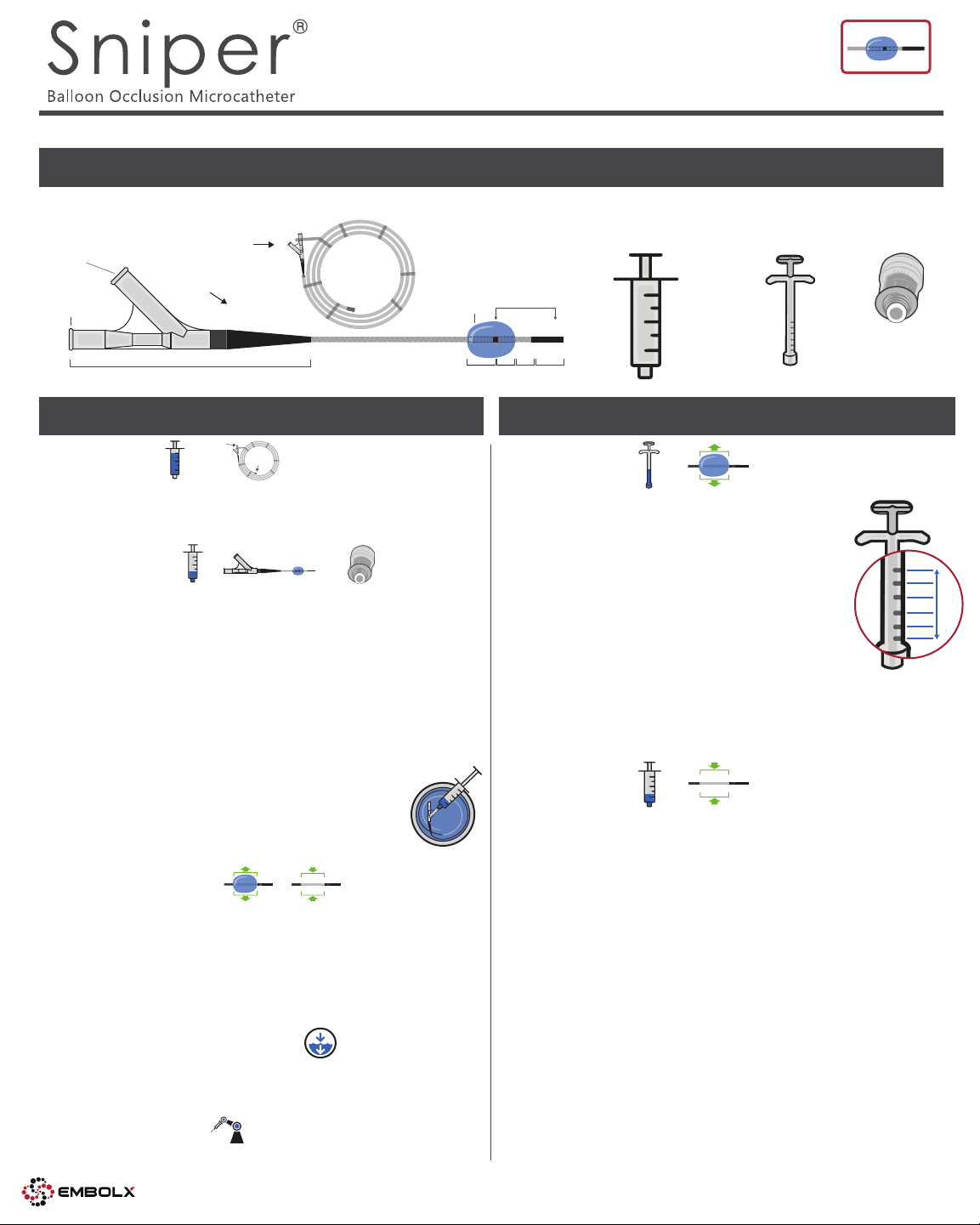
Sniper Balloon Occlusion Microcatheter (QTY 1)
Packaging Hoop
Balloon Port
Guidewire/
Injection Port
with Sniper
Sniper
Hub
Set-up
Flush
injection
port
Flush
Saline Flush
A
+
10 ml
► Flush inside end of hoop with 10 ml syringe filled with saline.
► Flush injection port with 10 ml syringe filled with saline.
► Remove Sniper from packaging hoop.
B
Prime Balloon
10 ml
► Submerge distal tip in saline bath. Place wet gauze on top to keep
distal balloon tip submerged.
► Fill 10 ml syringe with 2 ml of 50% contrast.
► Connect 10 ml syringe to the balloon port. Pull syringe plunger to
top lock position. Tap hub with finger until no bubbles are seen
rising in contrast. Release the plunger slowly down onto contrast.
► Remove syringe from balloon port. Exhaust air from syringe so
only contrast remains.
► Connect valve to the balloon port.
► Connect 10 ml syringe filled with 2 ml of 50% contrast to the valve
on balloon port.
► Pull syringe plunger to top lock position and place with
Sniper in saline bath. Let sit for at least 5 minutes.
► Move plunger slowly down onto contrast.
► Remove 10 ml syringe from valve.
C
Test Balloon Prime
► Follow the steps under “Use” to inflate and deflate balloon.
► To inflate balloon, use the .025 ml syringe to inject two units
(0.1 ml) and confirm balloon is completely filled with contrast.
► To deflate balloon, use the 10 ml syringe and confirm all
contrast has been removed.
► Save syringes filled with contrast for future use.
hoop
+
+
Ø6 mm
Saline Bath
Marker Bands (2)
4
3
mm3mm
mm
10 ml Flush, priming
and deflation syringe
(QTY 1)
10 ml
4
mm
0.25 ml
Inflation syringe
(QTY 1)
0.25 ml
Use
Inflate Balloon
► Use 0.25 ml syringe filled with 0.25 ml (5 units)
of 50% contrast.
► Connect syringe to the valve on balloon port.
► To inflate balloon:
◦ Inject one unit (0.05 ml)
◦ Under fluoroscopy, watch for balloon inflation
IMPORTANT! There will be a delay between injection and inflation
◦ Incrementally add additional units until the
balloon is visualized as contouring the vessel wall
IMPORTANT! If unable to visualize balloon, refer to troubleshooting
◦ Remove syringe from valve
◦ Save syringe filled with contrast
(subsequent inflation)
Deflate Balloon
► Use 10 ml syringe filled with 2 ml of 50% contrast.
► Connect syringe to the valve on the balloon port.
► To deflate and prime balloon for next use:
◦ Pull plunger to syringe top until balloon is completely deflated
IMPORTANT! May take up to 40 seconds for balloon to completely deflate
◦ Hold syringe vertical
◦ Move plunger slowly down onto contrast
◦ Remove syringe from valve
◦ Save syringe filled with contrast for future use
(subsequent deflation)
0.25 ml
10 ml
+
+
Valve
(QTY 1)
1 UNIT
1 UNIT
1 UNIT
1 UNIT
0.25 ml
1 UNIT
5 UNIT TOTAL
BALLOON CAPACITY
D
Maintain Catheter Hydration
► Keep Sniper’s hydrophilic coating activated.
► Return Sniper to saline bath when not in use.
E
Set Power Injector
► Limit input to no greater than 900 psi and 2 ml/second.
Best Practices
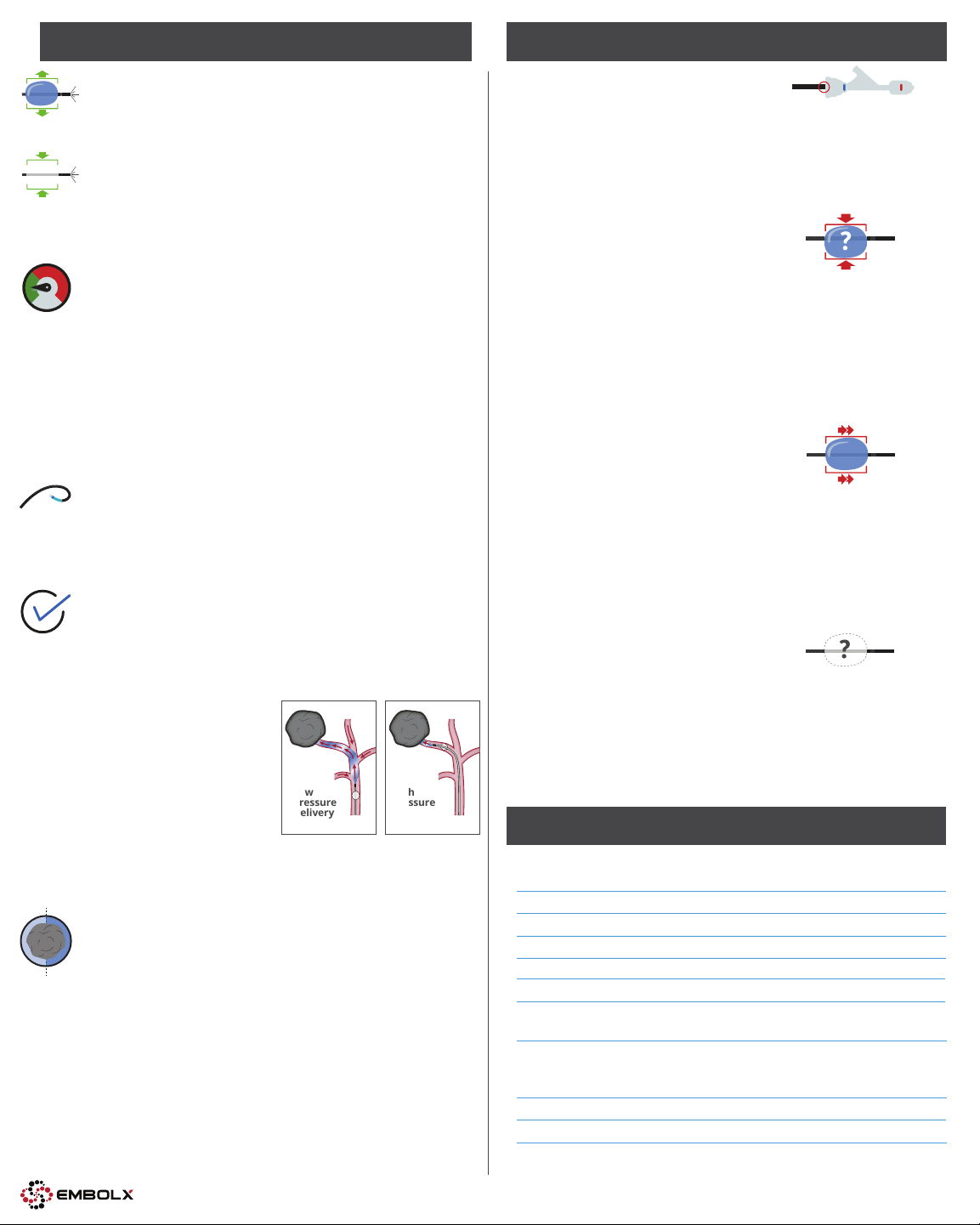
Troubleshooting
Imaging Before Embolization to Confirm
Flow Redistribution
► When the catheter tip is at the desired location, complete
an angiogram with the balloon down and with the
+
balloon up.
► IMPORTANT! When the balloon is up, blood flow is
slow and contrast will take longer to reach the tumor or
prostate. Therefore, fluoroscopy timing will be longer for
contrast visualization as compared to the balloon
down configuration.
Slow Injection of Contrast and Embolic Agent
► Flow redistribution in favor of the tumor or prostate
requires that a low pressure is maintained distal to
the balloon.
► Slow injection is required to maintain low pressure.
► Rapid injection will overwhelm the protective
pressure gradient.
► Contrast injection rate should be between 0.5 to
1.0 ml/second.
► Embolic injection rate should be about 1.0 ml/minute with
intermittent pause between injections.
Recommended Diagnostic Catheter Length with
110 cm Sniper
The use of a 65 cm diagnostic catheter is recommended for
use with the Sniper 110 cm length as it maximizes the distal
reach inside the patient.
Reaching Embolization Endpoint
With balloon occlusion there is slow moving, forward flow
Kink Prevention
Cause:
► An important part of Sniper’s exceptional tracking ability is its stiff
proximal catheter. The catheter can kink if the operator is not aware.
► There is a kink point at the RHV. The catheter cannot be bent sharply
in this area.
Solution:
► Advance the catheter forward by holding and pushing the catheter
no more than 3 cm from the RHV.
Unexpected Balloon Deflation
Cause:
► The valve is either not connected or not sufficiently tightened to
the balloon port or
► Excess vacuum in balloon lumen.
Solution:
► When inflating balloon, connect syringe to the valve on
balloon port.
► Remove and reconnect the valve on the balloon port which
equilibrates the pressure.
► Re-inflate the balloon until it is seen contouring to the vessel wall
under fluoroscopy.
Balloon Migration
Cause:
► A distal shift of the balloon is normal and expected and should
be corrected.
Solution:
► Remove 25% of the balloon inflation volume.
► Retract the Sniper catheter, with the balloon 75% inflated, until the
balloon is in the desired position.
► While holding the Sniper and diagnostic catheter in place, re-inflate
the balloon until it is seen contouring to the vessel wall under
fluoroscopy.
around the catheter tip due to reversal of collateral arteries,
capillaries and interstitial fluid. Depending on Sniper tip
placement during embolization, the treatment endpoint can
be visualized under fluoroscopy as follows:
Sniper tip is subselective
(Low Pressure Delivery)
► Observation of contrast
stasis in distal arteries.
Sniper tip is superselective
(High Pressure Delivery)
► Observation of:
Low
Pressure
Delivery
(Subselective)
High
Pressure
Delivery
(Superselective)
Unable to Visualize Inflated Balloon
Cause:
► Insufficient amount of contrast in balloon.
Solution:
► Take a high resolution spot image or
► Disconnect 0.25 ml syringe and connect 10 ml syringe filled with
2 ml of 50% contrast. Pull syringe plunger to top lock position for
2 minutes. Move plunger slowly down onto contrast. Then
reconnect 0.25 ml syringe to reinflate balloon.
Specifications and Compatibilities
◦ Contrast in portal vein or
◦ Embolic reflux around the Sniper balloon or
◦ Sniper balloon “pushing back” in the vessel.
Watershed Tumor Treatment
► Use high pressure delivery where the Sniper tip is placed
superselectively or segmentally.
► Not Recommended: Low pressure delivery where the Sniper
tip has a subselective or Lobar placement. In tumors that are
between segments and have multiple feeders, a low pressure
is maintained only in the segment with the balloon occlusion.
Therefore, pressure from the feeders originating in the other
segment with normal pressure can flow through the tumor
and into the low pressure created by the occlusion.
*
See Sniper Chemical Compatibility Statement Letter MK-0351 at http://embolx.com/products/. Embolx does not
make any claims; for informational purpose only.
**
Consult your sales representative for local market clearance and availability.
‡Boston Scientific Embozene™ 900 µm, 19020-S1. Merit Medical® Emboshere® 700-900 µm, S810GH. Data on file.
©Copyright 2018. Sniper is a registered trademark of Embolx. Visit embolx.com/patents for patent information. All
trademarks and registered trademarks are the property of their respective owners.
Specifications
Balloon Diameter
Catheter Functional Length
Tip Shape
**
Up to 6 mm
**
Catheter Outer Diameter (proximal)
Catheter Outer Diameter (distal)
Catheter Inner Diameter (Infusion Lumen)
Dead Space Volume
(hub + catheter)
Injection Pressure
Compatibilities
Guidewire
Embolic Beads‡
*
Coils
Embolic Agents
*
Embolx, Inc. | 530 Lakeside Dr. #200, Sunnyvale, CA 94085 | +1-408-990-2949 | customercare@embolx.com
(which occludes up to 5.5 mm vessels)
110 cm 130 cm 150 cm
Straight tip
2.9F (0.038")
2.2F (0.029")
0.020" (0.51 mm)
0.32 ml (110 cm)
0.36 ml (130 cm)
0.41 ml (150 cm)
Up to 900 psi
0.014" or 0.016"
Up to 900 µm
Up to 0.018"
®
Lipiodol
, EtOH, DMSO, Y-90,
Gelfoam, Glue (n-bCA)
MK-0314-01 revF1
 Loading...
Loading...